
Abstract
Communication measures can raise protective behavior regarding climate change, natural hazards, and other health risks. For being effective in such communication, we designed a five-steps methodology and applied it to health-protective behavior during heat extremes in Austria. The five steps are as follows: (1) target group selection, a multicriteria assessment (MCA) to identify the most important target group(s)—this led to the identification of mobile health care nurses as our primary target group; (2) target group analysis by interviews to identify drivers of and barriers to protective behavior—for the mobile health care nurses, the drivers were their climate change perceptions, control beliefs, perceptions of role models, and extent of thinking about heat and health, and the barriers were fatalism and work stress; (3) development of target group specific communication formats addressing the identified drivers and barriers—for the nurses, we designed a workshop format, animated videos, and two print formats; (4) pretest of formats in focus groups—these revealed our formats were effective in increasing heat risk awareness, competence, and protective behavior among the nurses; (5) improvement of formats based on pretest results—for example, we modified the workshop format to become a venue for mutual learning. These five steps can be applied to other projects where awareness, competence, or behavior shall be increased by means of communication.
Background and Objectives
Due to climate change, changes in many extreme weather and climate events have been observed since about 1950 (Intergovernmental Panel Climate Change [IPCC], 2013). Particularly, excessive heat and heat waves are a growing threat to public health. The heat wave in the summer of 2003 in Europe resulted in more than 70,000 deaths, 1 in particular of the elderly (Robine et al., 2008). Morbidity and mortality of the elderly increase during and after heat periods, as has been shown for several locations in Europe (e.g., Fouillet et al., 2008) and the United States (e.g., Anderson & Bell, 2009). Climate change models project near-term increases in the duration, intensity, and spatial extent of heat waves and warm spells (IPCC, 2013).
Communication of climate change risks and adaptation options—including procedures for education and participation—can play an important role in increasing protective behavior and thereby decreasing vulnerabilities to climate change (Grothmann, 2014). Related to the risk of increasing heat waves, the most widely documented policy for reducing heat vulnerabilities to date is the adoption of heat warnings and air quality alert systems to trigger emergency responses (Harlan & Ruddell, 2011). Nevertheless, in their review study on the effectiveness of public health interventions in reducing morbidity and mortality during heat episodes, Bassil and Cole (2010) conclude that the evidence for a positive impact of communicative public health interventions during heat waves is limited and that the most vulnerable groups are not being adequately reached.
With this in mind, we aimed at developing communication formats, which have the potential to be more effective than previous communicative public health interventions during heat waves, in the project CcTalk! 2 We focused on the development of communication measures only, as other vulnerability reduction measures (e.g., urban greening to decrease air temperature in urban areas) have not been possible within the scope of this project.
In addition to developing communication formats that contribute to reducing vulnerabilities of the elderly during heat waves, we also wanted to address the following three gaps in previous scientific work and communication practice:
Publications in the heat and health domain mostly address either perceptions of health risks and options for protective behavior (e.g., Abrahamson et al., 2008; Akompab et al., 2013; Lane et al., 2013; Toloo, FitzGerald, Aitken, Verrall, & Tong, 2013) or communication interventions such as heat warnings to increase risk awareness and protective behavior (e.g., Bassil & Cole, 2010; Bouzid, Hooper, & Hunter, 2013; Lowe, Ebi, & Forsberg, 2011; White-Newsome et al. 2014). Publications that link knowledge about influential perceptions (e.g., those which act as drivers of or barriers to protective behavior in a particular group) with the development of communication interventions that are able to change these influential perceptions (e.g., by increasing perceptions that motivate protective behavior) are lacking. Making this link is an integral step in marketing approaches that develop their marketing instruments for specific target groups (e.g., television spots) from systematic analyses of these groups. It is surprising that such marketing approaches have been used in several projects to influence mitigation of climate change (primarily to reduce household energy use; see Maibach, Roser-Renouf, & Leiserowitz, 2008), but have rarely been used to influence adaptation to climate change such as protective behavior during heat extremes. Therefore, it was an objective of the CcTalk! project to systematically use the results of target group analyses on influential perceptions to develop effective communication formats that are able to change these influential perceptions.
Much of the development of communication formats, not only in the domain of adaptation to climate change but also the public health domain, lack a systematic understanding of the drivers of and barriers to protective behavior. Psychological research on perceptions and behavior regarding natural hazards and other health risks has identified a number of determinants (e.g., risk perceptions, self-efficacy beliefs, etc.) of protective behavior, including self-protective and altruistic behavior, and has systematized these determinants in theories such as Protection Motivation Theory (PMT; Rogers, 1983; Rogers & Prentice-Dunn, 1997), Health Belief Model (HBM; Champion & Skinner, 2008; Hochbaum, 1958), and Norm-Activation Theory (NAT; Schwartz, 1977). Furthermore, psychological intervention research has identified a number of effective interventions to change people’s risk awareness and behavior (e.g., Mosler & Gutscher, 1998). The CcTalk! project aimed to make use of this scientific knowledge to develop target group specific communication formats. It was not the aim of CcTalk! to test, compare, or improve psychological theories of protective behavior or effective interventions. Therefore, this article aims at presenting the use (not a test, comparison, or improvement) of psychological knowledge and theories (such as PMT, HBM, NAT) for the design of communication measures that have the potential to contribute to behavior change.
Most of the current practices in communication of climate change adaptation have not been empirically evaluated regarding their effectiveness in creating awareness for climate change risks and stimulating adaptation action (Wirth, Prutsch, & Grothmann, 2014). “Although there are many guidelines for climate communication, there is little empirical evidence of their efficacy” (Pidgeon & Fischhoff, 2011, p. 35). The same situation seems to apply to interventions regarding health risks of heat waves. Eight years ago, the World Health Organization (WHO; 2009) stated, “There is a lack of targeted, systematic reviews to identify and assess the effectiveness of interventions to control key climate-sensitive health risks, for example, for the control of vector-borne diseases, or heat health action plans” (p. 9). Since then, some studies tried to evaluate the effectiveness of heat wave early warning systems (Bassil & Cole, 2010; Lowe et al., 2011), but it remains largely unclear which communication formats work for reducing vulnerabilities and which do not. Furthermore, evaluations have focused on heat wave early warning systems. Other methods of communication such as education tools to train professionals like mobile health care nurses for heat waves have not yet been evaluated. Hence, following the claim “it should be no more acceptable to release an untested communication than an untested drug” by Fischhoff (2007), a further objective of the CcTalk! project was to evaluate its communication formats prior to their broad dissemination (p. 190).
In sum, the overall aim of the project was to develop communication formats that have the potential to be more effective than previous communicative public health interventions during heat waves. The specific aims were to (a) systematically use results of target group analyses on perceptions that influence behavior to develop effective communication formats that are able to change these influential perceptions, (b) present the benefits of using scientific psychological knowledge for the design of communication formats, and (c) evaluate communication formats prior to their broad dissemination.
To address these objectives, we developed a five-steps methodology for designing communication formats that support the motivation of protective behavior in various risk domains (e.g., climate change, natural hazards) and applied it to health-protective behavior during heat extremes in Austria. The methodology strongly builds on psychological knowledge about determinants of protective behavior regarding health risks (e.g., Prentice-Dunn, McMath, & Cramer, 2009) and on psychological methods for designing behavior change interventions (e.g., Abrahamse & Matthies, 2012). The five steps can be applied to various risks domains and are therefore meant as a general approach for communication design—especially in the context of climate change adaptation and protective behavior regarding heat extremes, where such systematic methodologies are as yet very rare.
Paper Structure and Overview
The five-steps methodology includes the following:
target group selection by a MCA,
target group analysis by interviews based on psychological knowledge of determinants of protective behavior,
development of communication formats based on results of the target group analysis and on psychological knowledge of effective behavior change interventions,
pretest of communication formats by focus group workshops, and
improvement of formats based on pretest results.
In the following sections, these steps are presented in detail. Every section first describes the methods applied in the respective step and then presents our results related to the design of effective communication formats for reducing the vulnerability of the elderly during heat waves—the specific topic addressed in the CcTalk! project.
Step 1—Target Group Selection: Selecting the “Right” Target Group
Method
A systematic selection of the target group(s) is essential to reach the communication aims. In the project CcTalk!, we first compiled a list of potential target groups for communication aimed primarily at changing behavior to reduce vulnerabilities to heat waves. This list, specific to the health sector in Austria, included groups such as the elderly, public health authorities, pharmacies, health insurances, doctors, kindergarten teachers, and mobile health care services. 3 Second, we conducted a MCA to select our target groups. Each of the groups identified in the first step was assessed based on the following 10 criteria, which were developed in the CcTalk! project and appear generalizable to other projects aiming at increasing awareness, competence, and protective behavior regarding risks such as climate change, natural hazards, or other health risks.
Negative future impacts of the risk (in this case, heat waves) on the group
Options for protective behavior in the group
Low level of current protective behavior in the group
Low probability for future increase of protective behavior in the group without additional measures (like communication measures addressing the group)
Urgency of protective behavior by the group (because negative impacts have to be expected in the near future)
Relevance of the group to increase awareness of the risk beyond the group (role as “awareness multipliers,” opinion leaders)
Relevance of the group to increase awareness of options for protective behavior beyond the group (role as “behavior multipliers,” behavioral models)
Reachability of the group by communication measures
Existing contacts to the group
Willingness of group members to take part in focus group workshops for a pretest of communication formats
The first criterion applies to direct impacts (e.g., health impacts of heat waves for the group of the elderly) as well as indirect impacts (e.g., increasing workload for mobile health care nurses during heat waves). Its assessment should be based on current scientific knowledge.
Criteria 2 to 5 are closely linked to the aim of ensuring a high level of protective behavior within the group. Criteria 6 and 7 assess the potential of group members to act as multipliers and therefore address social network–level drivers of behavior (cf. Maibach et al., 2008).
The eighth criterion requires an assessment whether a group can be reached and influenced by communication formats. Some groups seem relatively insensitive to communication formats. For example, public health authorities appear to react mainly to laws and regulations, and less to communication measures such as flyers or brochures that are sent to them.
The ninth criterion was included due to economic reasons. A good and trustful contact to a group is often a necessary condition for the willingness of group members to take part in target group interviews (see Step 2) and in pretests of communication formats (see Step 4). Establishing such a contact to a new group often requires a lot of time and effort, but the CcTalk! project had a restricted budget. The tenth criterion is closely linked to the specific method used in the CcTalk! project for the pretest of the communication formats (see Step 4). A focus group workshop requires that members of the group are taking part, and for some groups, the willingness to attend such a workshop can be expected to be lower than for others.
The 10 criteria were assessed for all identified target groups in the heat risk domain by all 10 project team members individually (rating 0 = “criterion is probably not fulfilled” or 1 = “criterion is probably fulfilled”). In a subsequent discussion by the project team, those assessments were discussed for which there was a high level of disagreement. These were assessments for which about half of the team members had given a rating of 0, whereas the other half had chosen a 1. Individual assessments could be changed after the discussion. Finally, the ratings of all team members were added for all criteria and those target groups were selected that gained the highest rating sums.
Results and Discussion
Mobile health care nurses and kindergarten teachers got the highest rating sums and were therefore selected as the primary target groups. In this publication, only the results for the mobile health care nurses are presented. Mobile health care nurses visit people in need of care—most of them are older than 65—on a regular basis (once or twice a day).
One important reason for selecting mobile health care nurses and not the elderly themselves as a primary target group was that several publications (Abrahamson et al., 2008; Bassil & Cole, 2010; Lane et al., 2013) report a lack of self-perception as vulnerable among the elderly—obviously leading to a lack of self-protective behavior (Bassil & Cole, 2010). Although one study (Alberini et al., 2011) does not detect such a lack of self-perception as vulnerable, the majority of studies indicate that older people are probably difficult to reach by communication formats on heat-related health risks, which led to low ratings for the elderly regarding Criterion 8. As many of them, due to their lack of self-perception as vulnerable, do not see any need to read or listen to heat-related communication measures, these measures would have no or only a minor effect on their risk awareness or behavior (cf. WHO, 2011).
Furthermore, the following considerations were relevant for selecting mobile health care nurses as a primary target group. They can act as follows:
“Protectors”: They can directly reduce the vulnerability of the elderly (e.g., by giving them something to drink or by measures to cool down patients’ bodies) and thereby partly compensate for the lack of self-protective behavior among the elderly;
“Multipliers”: They have regular personal contact with the elderly and their relatives and know the medical conditions of the patients. Hence, they can act as awareness and behavior multipliers (see Criteria 6 and 7), who can tailor their communication to the specific medical conditions of the patients;
“Motivators”: Due to their regular personal contact to the elderly, they are also in a good position to motivate self-protective behavior of the elderly, as studies (e.g., Mosler & Gutscher, 1998) have shown that direct face-to-face forms of communication are better suited to change people’s behavior than nonpersonal forms of communication such as flyers or brochures, especially if the communicators are known and respected for their expertise regarding an issue. 4
While the health care nurses were selected as a primary target group in the CcTalk! project, the elderly and their relatives were planned to be addressed as secondary target groups—mainly via the health care nurses in their roles as multipliers and motivators. The self-protective behavior of the elderly was seen as essential to reduce their vulnerabilities. Hence, they had to be addressed by the communication formats as well. Furthermore, the social context of the elderly, primarily their relatives, was regarded as an important secondary target group because they can act as protectors, multipliers, and motivators like the nurses.
Step 2—Target Group Analysis
Method
A recent WHO (2011) publication states, “one must know what people think in order to design successful messages” (p. 28). Accordingly, the aim of a target group analysis is to find out as much as possible about the properties of the target group that are of relevance for the design of the communication formats.
Although the analysis of publications (scientific or media articles) that relate to the target group in question can be a useful method for gathering data on a target group, in most cases, a survey with members of the target group—by individual or group interviews or by questionnaires—is necessary. Most of the important questions about knowledge, attitudes, opinions, preferred communication channels, and so on in the target group can only be answered in this way. In the CcTalk! project, we conducted half-standardized telephone interviews with 30 female mobile health care nurses in the provinces of Lower Austria and Burgenland, which already had experienced heat waves in the past. The nurses were identified and contacted via the higher management levels of two major mobile health care providers in Austria (Red Cross Austria, Caritas). Hence, the interviewed nurses do not constitute a random sample. We interviewed the nurses during the working time of the mobile nurses. Interviews took on average 40 min. Answers of the interviewees were documented in note form by the interviewer during the interviews.
The interview guideline (see the appendix) included 22 questions, was pretested, and was slightly adjusted based on the pretest results. Similar to target group analyses in marketing research, we asked for information needs of the interviewees (Questions 17/18), perceived information needs of those affected (Question 22), preferred information channels (Question 19), and potential multipliers for heat and health information (Questions 20/21). Different from many target group analyses in marketing research, we tried to identify determinants of the current protection, multiplying, and motivation behavior of the nurses (cf. differentiation of three behavioral roles above: protectors, multipliers, and motivators). We developed the respective questions mostly from current scientific knowledge regarding potential drivers of and barriers to the three types of behavior. Primarily, three theories guided the questions included in the interview: PMT (Rogers, 1983; Rogers & Prentice-Dunn, 1997), HBM (Champion & Skinner, 2008; Hochbaum, 1958), and NAT (Schwartz, 1977). PMT has already been successfully applied to explain self-protective behavior regarding climate change and natural hazards (e.g., Grothmann & Patt, 2005). HBM is “one of the most widely used conceptual frameworks in health behavior research” (Champion & Skinner, 2008, p. 45) and has already been successfully used to explain self-protective behavior regarding heat extremes in Australia (Akompab et al., 2013). NAT has proven to be a very useful theory to explain helping behavior in various social settings so that we expected some explanatory power also for protective behavior of mobile health care nurses during heat extremes.
It was not the aim of the target group analysis to test specific theories of behavior or compare their explanatory power. Instead, the various theories and publications on protective behavior were used to generate a list of potential determinants of protection, multiplying, and motivation behavior to identify the statistically significant determinants, so that these could be addressed in the design of target group specific communication formats. Mainly from PMT, HBM, and NAT, we included 14 potential determinants—drivers and barriers of the three types of behavior. Every potential determinant was addressed by one specific question (see Questions 1-10, 12, 13, 15, and 16 in interview guideline in the appendix).
Furthermore, the interviews included an open-ended question on the current behavior of the nurses (see Question 14 in interview guideline). By this question, we expected to capture information regarding all three types of behavior we were interested in. Unfortunately, the answers of most interviewees related almost exclusively to protection behavior regarding their patients, not to multiplying and motivation behavior. Hence, we could not calculate quantitative measures of multiplying and motivation behavior, and in the statistical analyses of the answers, we could only calculate correlations of one type of behavior, protection behavior, with the potential determinants (see “Results and Discussion” of “Target Group Analysis” section). 5
As the behavioral measure relied on self-reported information only, we were concerned about getting biased answers due to a potential tendency of the interviewees to give socially desirable answers (in this case: to report more protection behavior than actually conducted). Therefore, we included also a question measuring the tendency to give socially desirable answers (see Question 11 in interview guideline). As there was no correlation between the answers to this question and the self-reported behavior, we concluded that the behavioral measure was not biased by a social desirability tendency.
All answers to the open-ended questions were categorized according to qualitative content analysis (Mayring, 2000). We then quantified potential behavioral determinants (Questions 1, 4, 15, 16) and the behavioral measure (Question 14). For example, the behavioral measure was generated by counting the number of performed behavioral categories (e.g., shading the apartment, giving the patients something to drink).
Finally, we calculated Kendall correlations 6 between the quantitative levels of the behavioral measure (Question 14) and the quantitative levels of the potential behavioral determinants (Questions 1-10, 12, 13, 15, and 16) of the interviewed nurses. Multiple regressions could not be computed due to the small sample size (N = 30) and the high number of potential determinants.
Results and Discussion
The statistically significant correlations in Table 1 indicate that the current protective behavior of the nurses is probably driven by a perception of climate change, high control beliefs, perceived role models for protective behavior, and previous thinking about heat and health (positive significant correlations), whereas fatalism and perceived work stress obviously act as barriers to protective behavior (significant negative correlations). 7 We do not interpret these results as direct influences of the statistically significant drivers and barriers on the behavior. For example, the perception of climate change might have led to an increased thinking about heat and health, which then led to an increase in protection behavior.
Correlations (Kendall’s Tau) of Potential Behavioral Drivers and Barriers With Self-Reported Current Protection Behavior (N = 30).
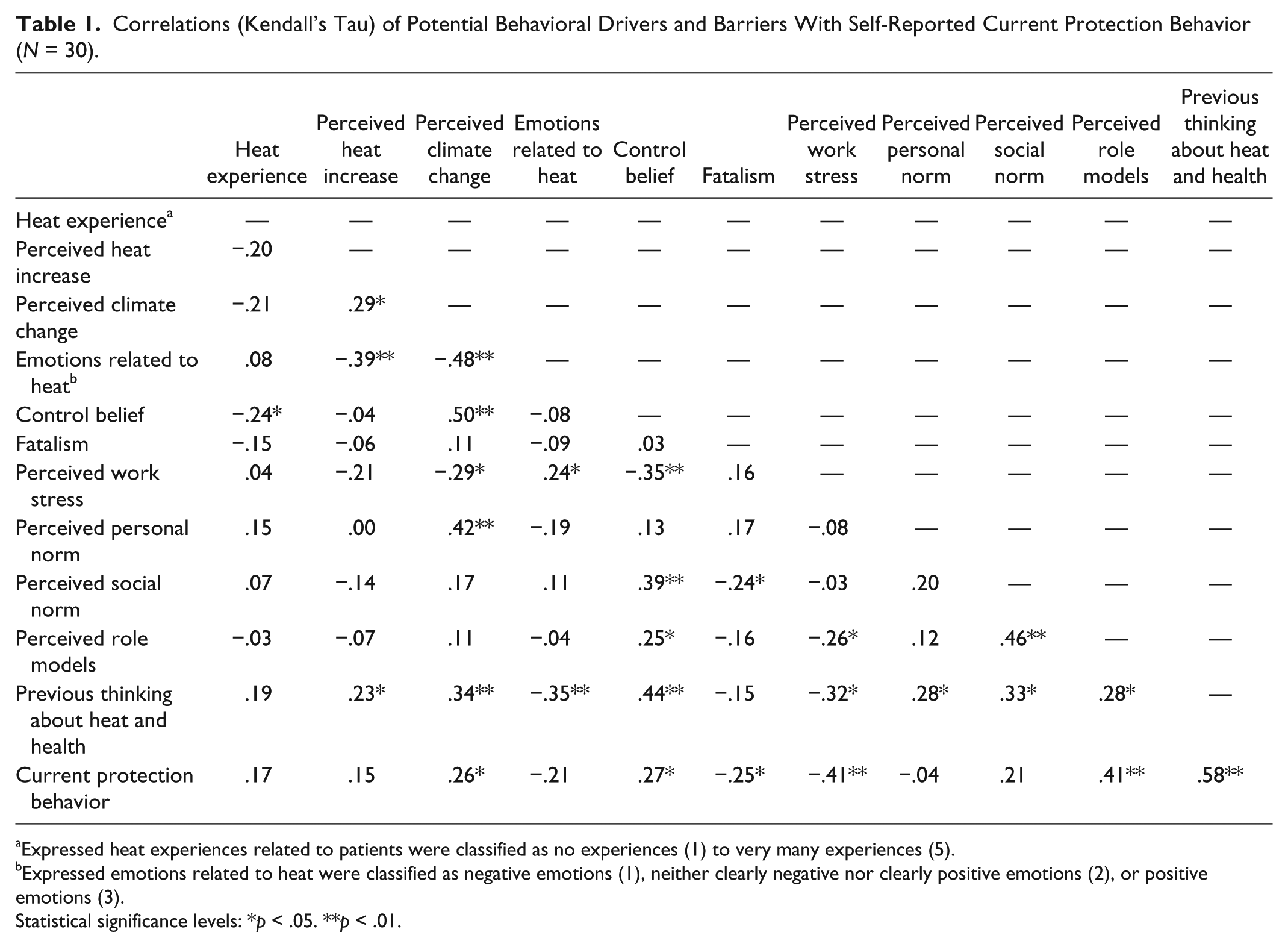
Expressed heat experiences related to patients were classified as no experiences (1) to very many experiences (5).
Expressed emotions related to heat were classified as negative emotions (1), neither clearly negative nor clearly positive emotions (2), or positive emotions (3).
Statistical significance levels: *p < .05. **p < .01.
Because almost all nurses (25 out of 30) answered with the highest possible rating (6 = totally agree) to the question measuring the perceived personal norm for protective behavior during heat, there was a lack of variance in this variable resulting in rather low correlations. Nevertheless, due to the very high reported levels of this personal norm, we expect that it also plays a role in causing protective behavior of the nurses. To the open question on barriers to protection behavior, six nurses named financial limitations of their patients, five named financial limitations of the mobile health care service, and three mentioned the apartments of their patients that are not adapted to heat.
The results also indicated that all interviewed nurses had experienced heat events in the past, that most of them perceive that their old patients suffer from heat, and that most of the nurses also suffer from heat. They feel exhausted and/or stressed during heat waves because they have to work hard (e.g., lifting heavy patients) and their company car is heating up strongly as they often have to park in the full sun and drive only short distances from patient to patient so that air-conditioning in the car has almost no effect or the company cars do not have air-conditioning yet.
It is likely that their experience of heat events in the past had contributed to their relatively high existing awareness of heat-related health risks and to the result that all of the interviewed nurses reported at least two types of protection behavior. Nevertheless, we detected strong interindividual differences: Some health care nurses seem to conduct much more protective behavior than others. Hence, we regarded the development of communication formats to further strengthen and increase the protective behavior of the nurses as useful, especially of those who as yet show only low levels of such behavior.
Step 3—Development of Target Group Specific Communication Formats
Method
The design of communication formats to further increase the protection, multiplying, and motivating behaviors of the mobile health care nurses strongly built on the results of the target group analyses and followed the logic to
fulfill the expressed information needs and to reduce identified gaps in knowledge and behavior,
use the preferred information channels and multipliers, and
address the identified drivers of and barriers to the behavior. Hence, the communication formats that are developed in Step 3 primarily target those perceptions and beliefs that proved influential as drivers of or barriers to behavior in Step 2.
Results and Discussion
About one third of the interviewed nurses expressed the information need for concrete recommendations on effective measures to prevent negative health effects during heat extremes. None of the interviewed nurses mentioned the regular measurement of the patients’ body temperature or medicine-related measures (heat-adapted dosing and stocking of medicine) as their current behavior to protect their patients from heat-related health effects. Therefore, we wanted to develop communication formats that could provide such detailed information (e.g., brochures and/or training workshops).
Only very few interview statements related to multiplying and motivating behavior. We concluded that, as yet, most nurses do not see themselves as multipliers (of knowledge on health risks and options for protective behavior) or motivators of protection behavior among the patients and the patients’ relatives. On the contrary, five interviewees mentioned the relatives of their patients and three interviewees named the patients as barriers to the implementation of health protection measures before and during heat extremes. Therefore, we identified the need to strongly support the nurses in their intended roles as multipliers and motivators. Based on these results, we intended to develop communication formats that motivate the nurses for taking the roles as multipliers and motivators (e.g., by stressing the high mortality among the elderly during heat waves in the past and by eliciting feelings of solidarity with the elderly). Furthermore, the communication formats should assist them in being effective in these roles (e.g., by training them in persuasive forms of communication and providing them with communication formats such as flyers, which they could use in their interactions with the patients and their relatives in motivating them to take protective actions).
To address mobile health care nurses as the primary target group and to also reach the secondary target groups, the elderly and their relatives, we selected and designed four communication formats: an expert workshop, a brochure, animated videos, and a flyer. All formats have the same heading/slogan (“Healthy Despite Heat”) and all visual formats (invitation letter for expert workshop, brochure, flyer, animated videos) have a similar graphical design to allow the use of the formats in an integrated communication campaign. The formats are presented in more detail in Table 2. The selection of these specific formats was guided by the following rules from communication practice:
create a combination of formats that is suited to reach the different target groups via established communication channels,
reach the target groups via various senses and activities (reading, listening, watching, speaking, etc.), and
appeal to people on both the emotional and intellectual level (emotions were mainly targeted by the animated videos whereas the other formats rather addressed knowledge aspects; cf. Slovic, Finucane, Peters, & MacGregor, 2007).
Developed Communication Formats for Addressing Mobile Health Care Nurses, the Elderly, and Their Relatives.
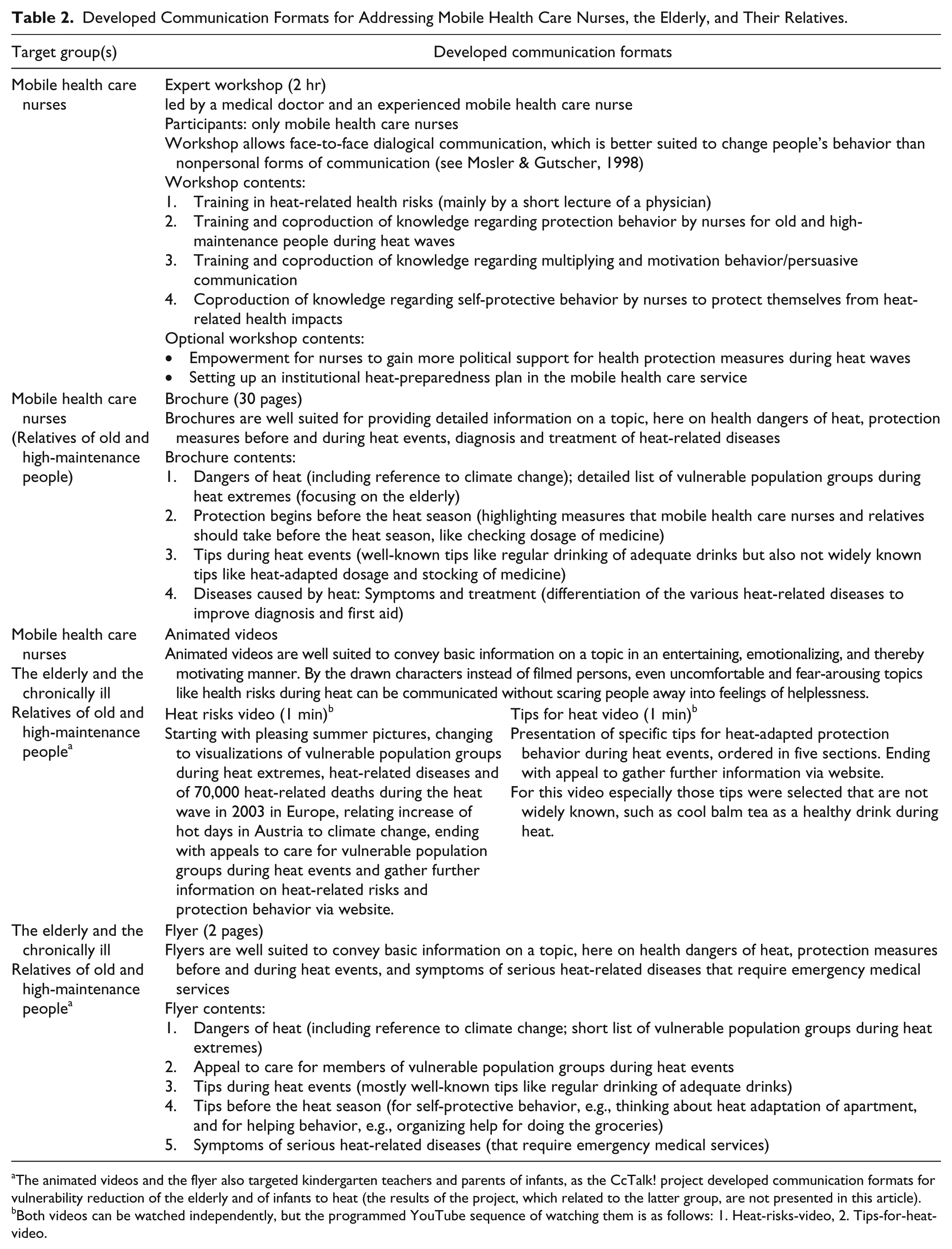
The animated videos and the flyer also targeted kindergarten teachers and parents of infants, as the CcTalk! project developed communication formats for vulnerability reduction of the elderly and of infants to heat (the results of the project, which related to the latter group, are not presented in this article).
Both videos can be watched independently, but the programmed YouTube sequence of watching them is as follows: 1. Heat-risks-video, 2. Tips-for-heat-video.
Furthermore, the selection of the four formats was determined by the available financial and time resources for their development.
To address the identified statistically significant drivers of and barriers to the protection behavior of the nurses (see Table 1), we included the following information in the communication formats: Climate change and its relation to the increase of heat extremes is mentioned in all four communication formats to increase perceptions of climate change, which was identified as a probable driver of protection behavior. To increase control beliefs and decrease fatalism, the longest sections of all four communication formats are devoted to presenting the many options for protection, multiplying, and motivating behavior. To increase the perception of role models for protective behavior, we included a mobile health care nurse, who is very experienced in dealing with heat-related health issues, as one of the leaders of the expert workshop. The animated videos were designed to present the risks and protective options regarding heat extremes in a visually appealing way and to provide links to further information, so that thinking about heat and health, another identified driver of protection behavior, is stimulated. To reduce the barrier of perceived work stress, which is probably partly related to the fact that the nurses themselves suffer from heat (see “Results and Discussion” of “Target Group Analysis” section), we included a section in the expert workshop devoted to the following question: How can mobile health care nurses protect themselves from heat-related health impacts and work stress during heat events? Nevertheless, the high negative correlation between perceived work stress and protective behavior also indicates that communication formats aiming at increasing nurses’ protective behavior will probably not suffice. In addition, interventions aiming at improving nurses’ working conditions and reducing work stress appear necessary (cf. McLeroy, Bibeau, Steckler, & Glanz, 1988)—interventions that could not be planned in the CcTalk! project, which focused on the development of communication formats.
To use the preferred information channels and multipliers mentioned by the nurses in the target group interviews, we focused on distribution channels via the work hierarchy of the nurses. Twenty-four of the 30 nurses mentioned their superiors as potential multipliers for heat and health information; 20 named these superiors as very influential in their work area. Hence, to reach the mobile health care nurses (the primary target group), we planned for communication formats to be sent to them by mail or email via superiors. To reach the secondary target groups—the elderly and their relatives—the mobile health care nurses are seen as important multipliers (see Step 1), for example, to distribute the flyer to their patients and relatives. Furthermore, the elderly can be reached by animated videos if these are shown on TV, depending on their health status. In the interviews, the nurses named TV as the information channel mostly used by their patients.
As a central portal providing access to all developed communication formats, an existing Austrian website for information related to climate change adaptation (www.klimawandelanpassung.at/kwa_hitzevideos) is used. Here, the animated videos (available only in German) can be watched via an embedded YouTube link; the flyer, brochure, and the concept for the expert workshop can be downloaded.
In the development of the four communication formats, a definition of specific objectives for each format has proven to be useful. Through the formulation of these format-specific objectives, the work on the formats could be carried out in a more focused manner than without such objectives. The definition of these objectives was also a crucial basis for the subsequent pretest of the communication formats, as this pretest evaluated to what extent the objectives were achieved. The objectives for the four communication formats are included in Table 3.
Objectives of Communication Formats and Questionnaire Results From Focus Groups.

Note. Objectives defined for the respective formats are marked by italics.
Due to the restricted time frame for the focus groups, the concept of the expert workshop could only be presented and discussed superficially. Hence, instead of assessing whether the workshop is reaching its objectives, the respective questionnaire assessed the willingness to take part in the workshop and the acceptance of the lead by a medical doctor together with an experienced health care nurse. Objectives of the workshop were (a) building further expertise and motivation for protection, multiplying, and motivating behavior; (b) discussing and giving answers to questions related to health protection during heat; and (c) exchange of experiences and good-practice examples related to health protection during heat.
Step 4 and 5—Pretest and Further Improvement of Communication Formats
Method
Not only for a target group analysis, but also for a pretest of the communication formats, a survey with members of the target group(s) is necessary in most cases. In the CcTalk! project, we chose to conduct focus group workshops (a form of group interview, which is often used in marketing research) as the concrete method for pretesting and gathering ideas for further improvement of our four communication formats from members of the target group. Only members of the primary target group (mobile health care nurses) were included in these focus group workshops. Due to resource restrictions, we could not conduct focus group workshops with members of the secondary target groups, the elderly and their relatives. Therefore, we did not only ask the mobile health care nurses in the focus group workshops how they evaluate the suitability of the four communication formats for themselves but also requested their opinions whether the formats are probably suited for the elderly and their relatives.
The advantage of focus group workshops is that their implementation is usually more cost-effective and less time-consuming than performing individual interviews. Furthermore, such workshops are well suited to developing new ideas for the improvement of communication formats. A disadvantage compared with individual interviews is that the group process is often characterized by evolving conversation from initial topics of discussion, often meaning other topics are not discussed. To minimize the influence of such group specific discussion processes on the pretest results, we conducted two focus group workshops with two groups of mobile health care nurses (one with seven participants from Red Cross Austria, and another with 11 participants from Caritas). Another disadvantage of focus group workshops is that the evaluations of persons, who are shy in a group situation, are generally underrepresented in results.
To utilize advantages and compensate for respective disadvantages, we used a combined individual and group survey method in the CcTalk! project: closed-ended questionnaires, which were completed individually by the participants of the focus group workshops (to gather the individual evaluations of the four communication formats), and open-ended discussions (to gather the collective evaluations and develop ideas for further improvement of the four communication formats). The 2-hr focus group workshops were divided into four format-specific blocks of discussion. At the beginning of each block, the format (e.g., the expert workshop) and respective target group(s) (e.g., mobile health care nurses) were presented. Each participant of the workshop was then asked to individually complete a format-specific questionnaire, which assessed the extent to which the objective of the respective format was fulfilled according to her or his opinion (for questionnaire items, see Table 3). Hence, the format specific objectives that were defined in Step 3 of the five-steps methodology to carry out the design of the communication formats in a focused manner were “reused” as evaluation criteria here in Step 4 of the methodology.
Finally, the professional moderator of the workshop led a discussion on the following questions:
What aspects (graphics, content, etc.) of the format do you like?
What aspects do you not like?
What suggestions do you have for the improvement of the format?
The discussions were tape-recorded and observed by two independent observers who focused particularly on emotional expressions (verbal and nonverbal) of the workshop participants, because emotions can indicate whether behavior is motivated—the primary aim of the CcTalk! communication formats. 8 The moderator visualized the main results of the discussion on a flip chart, which helped to organize the discussion and also served as a summary of the discussion results.
The quantitative results of the questionnaire were analyzed statistically (see Table 3). The two observer protocols and the flip chart protocol by the moderator were content-analyzed (Mayring, 2000). Only if contents of these three protocols were unclear or contradictory, the respective parts of the transcripts 9 of the tape-records were included in the content analysis.
Results and Discussion
The results of the pretest indicated that most of the objectives of the communication formats could be reached (including the motivation of protection behavior) but that some modifications to the formats would be useful to further improve their effectiveness and practical usability. Table 3 includes the individual questionnaire evaluations of the formats and indicates that most of the format objectives were largely fulfilled in the opinion of the mobile health care nurses that participated in the focus group workshops. Only the fulfillment of the brochure objective, to provide new information to the nurses, got an average rating of lower than 3 in one focus group—a result which can be explained by the fact that the participating nurses already showed a very broad knowledge regarding heat and health issues.
The results of the discussions indicated that the collective evaluations of the four formats were generally quite positive. Rather drastic animations of heat-related deaths in the heat-risks-video were received positively. Although the many dying animated characters were perceived as “brutal” or “threatening,” the nurses expressed that these drastic pictures caught their attention but did not discourage them from taking protection measures. Accordingly, the observer protocols indicated that, of all communication formats, the animated videos resulted in the highest number of expressed emotions. After showing signs of surprise and shock following the high number of 70,000 deaths caused by the 2003 heat wave in Europe, the nurses expressed joy and hope watching later parts of the heat-risks-video. They also mainly expressed joy and hope watching the tips-for-heat-video.
The workshop participants had several ideas for further improving the different formats. One idea was attractive to many participants. It related to including a graphical presentation of the sun as an intuitive symbol of heat in the brochure, the flyer, and the invitation letter for the expert workshop. Hence, in the revised versions of these formats, a sun symbol was included and acted as a further design element present in all formats, thereby contributing to the potential use of different formats in an integrated communication campaign.
An interesting and unexpected result of the discussions was that some nurses disapproved of the idea to include a physician in the expert workshop. They felt very well informed and competent regarding heat-related health risks and health-protective measures so that they seemed uninterested in listening to a physician in an expert workshop. Based on this result, we decided to stress in the invitation letter for the expert workshop that all participants of the workshop are seen as experts, and that the workshop is a venue for coproduction of knowledge and mutual learning processes regarding heat-related health risks and health-protective measures.
Overall Discussion
One of the aims of the CcTalk! project was to develop communication formats that have the potential to be more effective than previous communicative public health interventions during heat waves, which had only limited impacts and could not reach the most vulnerable groups (Bassil & Cole, 2010). The focus group pretest of our communication formats indicated that they were regarded as effective on various dimensions, including the motivation of protection behavior. We believe that this positive evaluation in the focus groups was very much based on our systematic five-steps methodology for developing communication materials, which build on a psychological understanding of determinants of protection behavior. Nevertheless, we could not test whether our communication formats were more effective than conventional public health interventions during heat waves, because the realization of a control group with conventional communication formats was not possible within the scope of this project.
Furthermore, we wanted to address three gaps in previous scientific work and communication practice:
To address the lack of publications that link knowledge about influential perceptions (e.g., influential as drivers of or barriers to protective behavior during heat extremes) in a particular group with the development of communication formats that are able to change these influential perceptions (e.g., increase those perceptions that motivate protective behavior), we have shown how the CcTalk! project—by building on existing marketing methodologies (e.g., Maibach et al., 2008)—systematically used the results of target group analyses on influential perceptions to develop effective communication formats that have the potential to change the influential perceptions.
Communication, not only in the domain of adaptation to climate change but also the public health domain, often lacks a systematic psychological understanding of the drivers of and barriers to human protective behavior. Furthermore, results of psychological intervention research are not adequately used. We have presented how the CcTalk! project made use of results and theories of psychological research on human perceptions and behavior regarding natural hazards and other health risks by including potential psychological behavioral determinants known from psychological literature in our interviews of the target group analysis. We then addressed the statically significant determinants in the design of our communication formats. Furthermore, we made use of results from psychological intervention research in the development of our communication formats (e.g., by including face-to-face forms of communication; cf. Mosler & Gutscher, 1998).
To address the lack of evaluations of communication formats in the domain of climate change adaptation and interventions regarding health risks of heat waves, we presented how we evaluated our communication formats in focus group workshops (by using a combined individual and group survey method).
Another aim of this publication was to portray a five-steps methodology to design communication formats that support the motivation of protective behavior in various risk domains (e.g., climate change, natural hazards). Our application of the methodology to design communication formats for stimulating health-protective behavior during heat extremes in Austria has shown that it proved useful for developing formats that are effective in raising awareness, building competence, and motivating protective behavior with regard to heat-related health risks.
One particularly interesting result of the target group analyses (Step 2) was that perceived work stress of the nurses obviously negatively influences their protective behavior. This indicates that communication formats aiming at increasing nurses’ protective behavior will probably not suffice. In addition, interventions aiming at improving nurses’ working conditions appear necessary (cf. McLeroy et al., 1988) so that they have the time to conduct heat protective behavior such as washing patients’ bodies with cool water.
Nevertheless, the five-steps methodology has some limitations. It does not provide exact rules, neither for the selection and development of communication formats based on the target group interview results nor for the improvement of the formats based on the focus group workshop results. Here, the CcTalk! project has shown that the development and improvement of the communication formats do not only rely on rational and scientific interpretations of the interview and workshop results but also very much on the experience and creativity of the designers of the formats.
A further limitation of the methodology, as it was applied in the CcTalk! project, considers the samples of the target groups. Neither the nurses in the target group interviews nor the nurses participating in the focus group workshops constituted representative random samples of all mobile health care nurses in Austria. Generally, interviewing a representative sample of a target group is possible (e.g., by representative telephone surveys like they were conducted in the project KommEx 10 in Germany), but is often relatively costly and was therefore not possible within the resources of the CcTalk! project.
A final limitation we want to note here is that the pretest of communication formats by focus group workshops does not constitute a valid effectiveness evaluation of communication formats. The evaluation of the formats in such a workshop is an artificial setting. In reality, formats such as flyers or brochures are not distributed and read in a workshop but people find these in their mail or they are handed to them by colleagues or friends. A more valid evaluation of communication formats is a communication campaign evaluation that assesses the level of awareness, competence, and/or behavior in a representative sample of the target group before and after a communication campaign and controls for other factors that might contribute to changes in awareness, competence, and/or behavior. Such a communication campaign evaluation is possible but is often not carried out due to its high costs.
Conclusion
Despite its limitations, the five-steps methodology presented here could and should be used by authorities when trying to affect people’s behavior in a positive way by means of communication—especially in the context of climate change adaptation or protective behavior regarding heat extremes, where such systematic methodologies are as yet very rare.
Second, the results also indicate that communication measures alone will not suffice. Work stress decreased the nurses’ protective behavior. Therefore, also interventions improving nurses’ working conditions appear necessary. This highlights that communication measures should be part of systemic intervention strategies directed at changing interpersonal, organizational, community, public policy factors (McLeroy et al., 1988), and infrastructures (e.g., urban greening to decrease air temperature in urban areas) to reduce vulnerabilities comprehensively.