
Abstract
Children in care of the state are amongst the most disadvantaged in society. They have often experienced adverse childhood experiences leading to their care entry including abuse and neglect. Longitudinal data suggests problems children in care of the state experience within adolescence persist into adulthood, showing “a continuing legacy of adversity.” Emerging literature shows that edge of care interventions can bring about benefits. These interventions support families to meet their child’s needs and prevent, or reduce, the likelihood of children going into care. However, it is not clear how or why these interventions work. It is important to develop this understanding to inform the development of effective, theory-informed practice to benefit this population. We reviewed and synthesised published literature to expose mechanisms by which interventions may promote and support family preservation for children at the edge of care. Our synthesis uses a realist approach to examine mechanisms by which interventions, in various contexts, can promote and support family preservation for children at the edge of care. Previous work by the team shaped the initial search strategy and in line with RAMESES realist review guidelines, no restrictions were placed on the types of study to be included in the synthesis. From 7,530 potentially relevant references identified, 61 papers were included in final extraction. Extracted data was themed, prior to developing narrative and formulating programme theories. Effective edge of care service operation seemed to be based on four core programme theories pertaining to the need for family skills training, home-based delivery, dedicated worker, and rapid response to need.
Introduction
Children in care of the state are amongst the most disadvantaged in society. Two thirds of children who enter care do so as a result of abuse and neglect, with family dysfunction and family acute stress also being commonly reported risk factors (Dept. for Education, 2021). Young people within the care system are more likely to have experienced multiple adverse childhood experiences than their peers not in care of the state, including through environmental risks such as parental conflict, mental illness and substance misuse (Hughes et al., 2017). They are five times more likely than their peers to have a mental health disorder (Meltzer et al., 2003), with 39% of children in care of the state in the England reporting a level of emotional and behavioural health that were a cause for concern (Dept of Education, 2021). Children in care of the state have lower levels of educational attainment; by the age of 16 years most falling well behind the average for their age (Sinclair et al., 2019). Longitudinal data suggest that many of the problems that children in care of the state experience within adolescence persist into adulthood, showing “a continuing legacy of adversity” for those who have been in care (Cameron et al., 2018). This can be further complicated by the promotion of children in care of the state maintaining contact with their birth families. Atwool (2013) suggests that children in care of the state face challenges in managing conflicting loyalties to adults caring for them meaning they are left to navigate complex relationships.
Statistics show that there are nearly 46,000 young people in the care system in Australia (Australian Institute of Health and Welfare [AIHW], 2021), and 407,493 in the US (Statista Research Department, 2022). In the past two decades there has been a year-on-year increase in the number of children who have entered care in England (Thomas, 2018). In 2021, there were 80,850 (67 per 10,000) children in the care of a local authority in England; a 1% rise on the previous year and an all-time high (DfE, 2021). As well as the considerable human cost to the families involved, the economic cost of a child being taken into care is substantial. Recent estimates in England suggest that it costs £53,000 per year for each child in care (Stanford & Lennon, 2019). Consequently, providing effective interventions to prevent care entry has become a priority of many child welfare systems internationally.
In an effort to address inequalities experienced by families at the edge of care (i.e., where the child(ren) are at immediate or potential risk of being removed from their families care and will become looked after by the state if there is no alternative intervention) and reduce costs, interventions are typically provided to families where a child or young person requires statutory intervention to protect them from the risk of significant harm (child protection) or where the child’s health and development is impacted if services are not provided (child in need). Edge of care services, also known as preservation services, aim to support families to safely reduce the “in care” population by working more effectively with families; at a time when care is “being actively considered to meet the young person’s needs” (Rees et al., 2017). There is emerging literature across the globe showing the potential benefits such interventions can have. However, it is not clear how or why these interventions might work or the circumstances when they do not work. This synthesis therefore seeks to develop an understanding of these complex interventions to inform the development of effective, theory-informed practice for practitioners, and policy makers in order to benefit this marginalized population.
Aim
This synthesis examined existing literature to identify what “works” to reduce children being removed from families and taken into statutory cared by a council or state authority. This was considered in terms of discrete community delivered interventions provided in response to referral(s) from statutory child welfare agencies, which address specific issue(s) to promote family preservation. The primary purpose was to explore the literature to identify practices which can inform the development of explanatory formulae (programme theories), pertaining to the impact, and effectiveness of such interventions.
Two main research questions guided the synthesis:
What does the existing literature suggest “works,” as demonstrated by children not being taken into local authority/state care and remaining in the care of their usual caregiver?
What community delivered interventions are provided in response to referral(s) from child welfare services and addressing specific issue(s) in promoting family preservation and/or permanency: for whom, how and in which circumstances?
Rationale for Using Realist Synthesis
Realist approaches are underpinned by the belief that observational evidence cannot alone establish causal uniformities. They therefore focus on providing explanation as to “why” relationships are established through the exploration of events happening within the system (mechanisms) to connect inputs and outputs (Dalkin et al., 2015).
The realist synthesis methodology is based on the philosophical assumptions of “scientific” realism proposed by Pawson and Tilley (1997) and seeks to identify “what works in which circumstances and for whom?,” rather than simply answering “does it work?” By taking this approach, mechanisms (definitions of terminology used within this synthesis are provided in Table 1) are identified which explain how outcomes are achieved, alongside the conditions which facilitate their interaction (context). Thereby providing explanation as to “how” an intervention works (Rycroft-Malone et al., 2012). The realist approach is theory-driven and seeks to explore ways in which interventions may have different effects for different people, through developing understanding pertaining to configurations of these identified contexts, mechanisms, and outcomes. This is presented within realist work as programme theories. Programme theories are explanatory formula which detail configurations of context, mechanism and outcome which are refined and tested through empirical data to provide a more nuanced account of how an intervention works (Dalkin et al., 2015).
Realist Terminology.
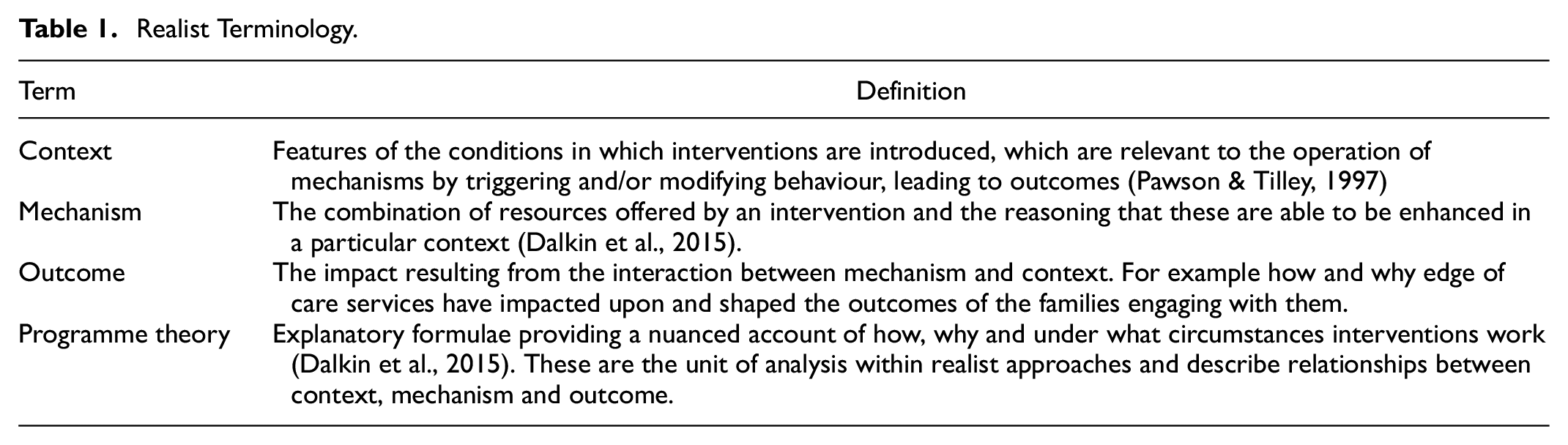
Explanations as to “why” relationships come about are identified and explored through this synthesis by detailing an understanding what is happening within the edge of care intervention (mechanisms) to connect inputs and outputs (Dalkin et al., 2015). Definitions of terminology used within this synthesis is provided in Table 1.
There has been a rise in the use of realist approaches for understanding the relative success or failure of innovation in health and social care contexts due to its ability to acknowledge the importance of the contextual environment within which interventions are being delivered, as well as the impact(s) this then has on outcomes for individuals (Dalkin et al., 2015). Using a realist synthesis approach to explore mechanisms which promote and support family preservation for children at the edge of care has several benefits. This approach accepts and provides techniques in which to understand complex interventions (Pawson, 2013). Edge of care interventions are inherently complex, they provide a range of different approaches, used in different contexts. Previous reviews and meta-analysis of edge of care services (e.g., Bezeczky et al., 2020; Schweitzeret al., 2015) have focused on impacts from such services, but have not gone into depth about how and why interventions work/do not work. Using a realist synthesis approach we look to identify and understand the contexts within which edge of care services operate and identify core mechanisms within these contexts which promote and support family preservation for children at the edge of care. In addition, using this approach allows for practice implications to be inferred from resultant concepts or theories, instead of being directly extracted from summed or aggregated data (Hannes & Lockwood, 2011).
Methods
The synthesis identified, characterised and systematically synthesized the literature, to expose the mechanisms by which interventions, in various contexts, can reduce the likelihood of children going into care. In using a realist approach, we were able to identify potential underlying causal mechanisms (i.e., the resources offered by an intervention), and the reasoning that these are able to enhance in a particular context(s), leading to measurable or observable outcomes (Dalkin et al., 2015). Through the synthesis, a framework depicting context, mechanism, outcome pattern configurations in the form of programme theories was developed. Although iterative in nature, the realist synthesis approach is not random and therefore a structured approach is required. This synthesis was based upon the four stages laid out by Rycroft-Malone et al. (2012). These include; scoping the review, searching and appraising the evidence, extracting and synthesising findings, and drawing conclusions, and making recommendations. Figure 1 provides an illustrative overview of the method.

Illustrative overview of method.
Step 1: Define scope of Review
The review scope was informed by advisory group engagement and subject expertise within the research team. The advisory group included a parent who had previously been in receipt of an edge of care service, referring social workers, service and operational managers and edge of care provision practitioners.
The review team constructed candidate theories in consultation with the advisory group offering explanations of how edge of care services might work—what they do, who they are aimed at, and their causal relationship to outcomes. Potential generative mechanisms included the voluntary nature of the intervention (in contrast with statutory child protection intervention) prompted by an anticipated context of potential risk of a child being taken into care. This created a “window of opportunity” for a “teachable moment” for the family, whereby the family are more receptive to working with services to resolve their difficulties. The edge of care practitioner was thought to adopt a learner/teacher approach to practically supporting families in the acquisition of new skills, strategies, and coping mechanisms. Restorative practice was seen to facilitate the rebuilding of fragile family relationships. These improved family relationships have a “ripple effect” and resulted in further improved outcomes for the children, including reduced behavioural difficulties. Based on advisory group engagement and informal literature searches, the following inclusion criteria was agreed:
Families who are “at the edge of care” where a child/young person is being considered for care but have not entered into (out-of-home) state care or who are already in the care of the state, but permanence has not been identified and secured are the main focus of the synthesis.
Interventions must not be statutory.
They must be time-limited therapeutic and/or practical interventions which promote family unity & relationships in response to assessed need.
Include an outcome of reducing family crisis, improving family functioning and keep children safely living at home with their birth parents.
The synthesis was registered on PROSPERO, the international prospective register of systematic reviews (CRD42021231009).
Step 2: Search for and Appraise Evidence
Search Strategy
The search strategy for a realist synthesis needs to ensure that the strategy is able to operate at a level of abstraction which allows reviewers to be at a distance from the detail and variation in evidence presented; however, it must also be specific enough in order to meet the purpose of the review (Rycroft-Malone et al., 2012). The search strategy followed a purposive, iterative approach. Our initial search strategy was developed to identify broad international literature examining family preservation services, consisting of mesh terms, thesaurus headings, Boolean and proximity operators. This search strategy was administered (February 2021) without language or date restrictions in nine electronic databases: MEDLINE (OVID), PsycINFO (OVID), Applied Social Science Index and Abstract (ProQuest), International Bibliography of Social Science (ProQuest), ProQuest Social Science Journals (ProQuest), ProQuest Sociology (ProQuest), Social Service Abstracts (ProQuest), Sociological Abstracts (ProQuest), EBSCO. In line with RAMESES realist review guidelines (Wong et al., 2013), no restrictions were placed on the types of study to be included in the synthesis. Two reviewers independently screened all titles and abstracts using specified inclusion and exclusion criteria, retrieving articles for all potentially eligible studies and evaluating full text. Discrepancies at each stage were resolved by discussion or by consulting a third reviewer if consensus could not be reached.
Step 3: Extract and Synthesise Findings
The data synthesis utilised a piloted bespoke structured data extraction form to assist with the organisation of data, providing structure to the theming of evidence. Each paper was reviewed, with a data extraction form completed independently by two researchers. Data from these forms was collated and discussed by the research team.
The approach taken to synthesise extracted data was based on the principles of realist evaluation (Pawson & Tilley, 1997). It included the organisation of extracted data into evidence tables (context, mechanism, outcome, and formal theory); theming of data; linking of the chains of inference within and between themes; development of the narrative; programme theory formation.
In addition, to ensure our postulated theories from the data extraction were in accordance with current thinking and had practical consideration for implementation and impact, an advisory group was consulted throughout the review. The advisory group provided a platform to discuss, test and refine our thinking as the synthesis progressed, and was consulted at three key points of the data analysis (Figure 2). They provided feedback on initial core mechanisms identified as influencing edge of care service provision, initial programme theory development, and programme theory consolidation. At each point, perspectives were sought in relation to the following: (a) Does the mechanism/programme theory match their experience? (b) Which of the mechanisms/programme theories are most important and why? (c) What do the mechanisms/programme theories mean in a practical context? and (d) Does the mechanism/programme theory terminology resonate/make sense? Changes were then made in accordance with feedback received from the advisory group.

Advisory group consultation points.
Findings
We identified 7,530 potentially relevant records. We excluded 7,362 on the basis that the abstract and title did not meet the inclusion criteria. A further 107 papers were excluded during full text review, including for example, those identified as not linked to edge of care provision and papers where no intervention was stated. Sixty-two papers were included in the final data extraction phase. See Table 2 for an overview of the countries represented and study types in the included studies.
Country and Study Type of Included Studies.

The participants in receipt of the intervention(s) within the included studies predominately focused on the whole family (n = 42). However, a number focused only on the parents/caregivers (n = 7), child/young person (n = 6), mothers (n = 4) and a combination of parents/caregivers, and professionals (n = 2). Only one study targeted a specific participant ethnicity, looking to reduce disparities for American Indian/Alaska Native children.
Associated Contexts
Whilst the aim of the synthesis was to develop an understanding of how specific contexts impact on identified mechanism(s) to produce outcomes, our review highlighted that such detailed explanations are rarely seen within the literature. Many of the interventions were delivered within a context of families experiencing multiple problem issues and included the delivery of a number of different mechanisms. Papers were not always explicit about the “type(s)” of issues families included in the research experienced. However, from those that did, we identified five contextual groupings which were seen to influence the effectiveness of edge of care interventions. These groups included; (a) Families having low(er) levels of social capital (i.e., the internal and external resources of support to draw upon). In particular, single parent families, younger parents or families with no extended social networks were identified as often having lower levels of support, and thus are thought to be under increased stress relating to managing family life. (b) Parental health needs. In families where the parent is experiencing significant health needs in relation to substance use and/or mental health needs, it is suggested that the parent must first have their health needs addressed prior to addressing the needs of the family. (c) Families experiencing abuse. Where abuse including physical or emotional for example, is occurring within the family this will often require intervention from additional statutory based services outside the edge of care intervention remit. (d) Families having a level of skill deficit. Although not often explicitly stated within the literature, references were often found to edge of care interventions providing training and support to improve skills within the family, therefore implying that the family had been operating in the context of a “skill deficit.” These skills were wide ranging and included practical (i.e., budgeting and providing a safe home environment) and more emotional (i.e., speaking and listening) skills. (e) Immediate threat of a child being placed in care. This context is seen within all families connected to edge of care service provision as it is a pre-requisite for accessing such provision. The threat of state care entry for a child is viewed to place the family under additional stress and may also compound other contextual conditions being experienced.
The number of these contextual conditions experienced by the families increases the complexity of the family context in which the intervention is delivered, and thus has the potential to limit the effectiveness of the intervention being delivered (Pfadenhauer et al., 2017). Overall however, contexts 1, 4, and 5 (Families having low(er) levels of social capital, Families having a level of skill deficit, and Immediate threat of a child being placed in care) were seen to support the successful implementation of edge of care services, as initiatives often targeted or at least acknowledged these family contexts. Context 2, Parental health needs, was often seen as a barrier for effective edge of care services, due to the individual needs of the parent having to be met by a specialist service, prior to being able to effectively engage with the edge of care provision. Context 3, Families experiencing abuse, varied in terms of its impact on the mechanisms within the edge of care provision. The potential for this context to support successful implementation of edge of care services is dependent on the severity of abuse and if other specialist services are required to assist.
Identified Outcomes
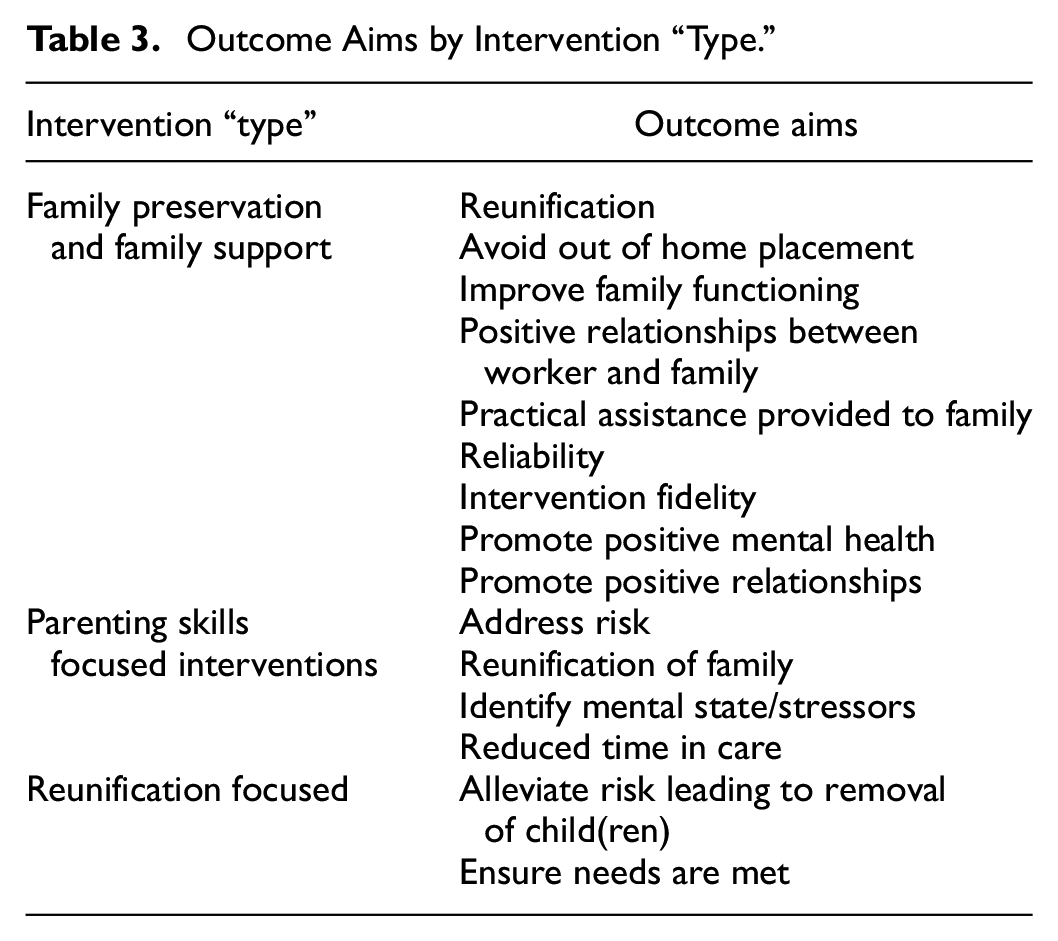
In terms of outcomes, what can be described to “work,” where children are not taken into local authority/state care, remaining instead in the care of their usual caregiver, is inherently connected to the context in which the intervention is delivered. As with contexts, we identified an overall lack of detailed explanations as to the outcomes observed within the literature. However, outcomes are inextricably linked to the context in which the intervention is being delivered and mechanisms included in the intervention. Key outcomes extracted from the review have therefore been grouped by intervention “type” as categorised by the research team relating to the key focus of the intervention (Table 3).
Outcome Aims by Intervention “Type.”
Core Mechanisms Influencing Edge of Care Service Provision and Development of Programme Theories
Based on the data, five initial programme theories were postulated around identified core mechanisms, taking into account additional context and outcome information. Core mechanisms were identified which held significant causal power and/or are critical for influencing how edge of care service provision works (See Supplemental Appendix A for full breakdown of mechanisms). These mechanisms were presented to the advisory group for confirmation, refinement, and refutation.
It emerged from the literature that identified mechanisms often interact in such a way that they are unable to be untangled from one another. In particular, “individual family need” was identified as a cross cutting theme throughout all the core mechanisms. It should be noted however that the contextual implications of the families were viewed to have, in some cases, significantly impacts on how interventions were received, and the outcomes achieved as a result. Mechanisms are viewed to therefore work, either to facilitate, or hinder interventions, depending on context.
Programme Theory 1: Structured Parent and Family Skills Training
Core Mechanism: Family Skills Training
A high proportion of the papers referred to family “training” (e.g., Akin et al., 2017; Akin et al., 2018; Al et al., 2012; Chaffin et al., 2001; Chambers et al., 2016; Forrester et al., 2008; Forsythe, 1992; Hayward & Cameron, 2002; Oxford et al., 2016; Roberts, 2016; Sen, 2016; Smith, 1995). What was meant by training and training approaches however, varied. Some training was viewed to follow well defined structured curriculum-based approaches (Akin et al., 2017; Akin et al., 2018; Chambers et al., 2016), whilst others were based on structured approaches, but adapted to reflect the family’s needs (Chaffin et al., 2001; Roberts, 2016; Rodrigo et al., 2006). Further, some based training on more general parenting competence approaches, aiming to meet immediate needs of the family (Al et al., 2012; Gillespie et al., 1995; Roberts, 2016; Smith, 1995). Although not often explicitly stated, training was seen to be delivered to families who have perceived skill deficit and/or low reflective functioning.
Training is viewed on a continuum, from training delivered within a highly structured curriculum-based approach, to individually tailored ad hoc training approaches. The reasoning behind delivery of many of the training approaches across the continuum, was a focus on the family, with the notion that fostering strength and skills within the parent and family is key. The family in this sense are perceived as the “agents” or “catalyst” for change (Akin et al., 2018; Al et al., 2012; Roberts, 2016; Rodrigo et al., 2006). In focusing on the family, there is a need to ensure that training is able to benefit the family and respond to their need(s).
In viewing the family within the context of having some level of skill deficit, through participation in training, the family could be introduced to skills and strategies to assist in promoting pro-social behaviours within the family and improved family functioning (Fox & Ashmore, 2015; Parra et al., 2016; Roberts, 2016). This is seen in approaches which included practical activities, such as maintaining a safe home environment for children and homemaking skills including budgeting, careful shopping, meal planning/preparation, and housekeeping (Parra et al., 2016; Smith, 1995). And also, more emotional/support-based parent management training including a focus on social and emotional regulation, listening and speaking skills, peer pressure resistance, sharing emotions, alcohol and drug education, and problem solving (Akin et al., 2017, 2018; Al et al., 2012; Gillespie et al., 1995; Roberts, 2016). For the training to be effective however, we theorise that the family must be in a position to actively engage. This is not always possible for families where parental health needs are yet to be met.
A common theme detailed throughout the training continuum, is the aim to increase a family’s skill base, their “resources,” in order to promote pro-social behaviours and assist the prevention of family breakdown. Programme theory 1 therefore postulated that;

Programme Theory 2: Home Based Response to Individual Need
Core Mechanism: Home Based Response
A theme running throughout the analysis was an importance of “tailoring” or “matching” services to a family’s needs (including emotional, financial, relational etc.), and an acknowledgement that in order to understand and meet these needs, services should be delivered within the home environment (Bath et al., 1993; Bezeczky et al., 2020; Chambers et al., 2016; Dagenais et al., 2009; Forrester et al., 2008; Fox & Ashmore, 2015; Forsythe, 1992; Fraser et al., 1997; Hayward & Cameron, 2002; Marcenko et al., 1996; Parra et al., 2016; Scannapieco, 1993; Smith, 1995). The mechanistic components and subsequent importance of the home environment was not always explicitly stated. Often papers portrayed an almost “taken for granted” assumption that services are best suited to delivery in the home if they are to address and subsequently improve family functioning with limited detail. However, in the context of parental health needs, these may not be appropriate, or possible to be addressed by the edge of care intervention and therefore referral to other providers may be required. Therefore, families with needs that can be addressed by the edge of care intervention within the home environment are likely to experience improved family functioning. Whilst families with needs that exceed this, may not.
Although little data was able to be extracted with regards to the underpinning assumptions as to why services are best delivered within the home, the frequency of its reference (services are delivered within the home) led to it being considered a core mechanism and thus programme theory 2 postulated that;
Programme Theory 3: Dedicated Worker Time
Core Mechanism: Dedicated Worker Working Intensively With Family
The approach and interpersonal skills of workers delivering services are often acknowledged to be a key element of the service experience. Underpinning this experience, dedication and intensity were identified as key mechanistic components (Berry, 1991; Chambers et al., 2016; Dagenais et al., 2009; Forsythe, 1992; Fraser et al., 1997; Hayward & Cameron, 2002; Marcenko et al., 1996; Mason, 2012; McWey, 2008; Roberts, 2016; Scannapieco, 1993; Sen, 2016; Smith, 1995). A key factor in achieving a dedicated approach was the continuity of care afforded by workers carrying small caseloads, in order that they could spend more time with a family (Al et al., 2012; Berry, 1991; Chambers et al., 2016; Forrester et al., 2008; Scannapieco, 1993).
Supporting a small number of families at a time, allow for workers to be more responsive in a crisis, which is crucial in building relationships and trust with the family wherein the worker can be relied upon to “be there” when the family needs them (Mason, 2012). In addition, approaches and the manner of interactions by workers with families was highlighted to be important in facilitating a feeling of respect, which led to open and honest conversations (Mason, 2012). This again, highlights the need for individually tailored family support which is threaded through each of the programme theories. It is through these relationships that workers are able to assist families with facilitating change through the establishment of trust (Roberts, 2016).
The intensive work (i.e., high frequency of communication and visits) seen between worker and family allows for practical assistance to be provided alongside “therapeutic” intervention(s) (Campbell, 1997; Mason, 2012), thus providing both practical and emotional benefits to the family. Practical benefits in this sense may include for example, assistance in filling out forms or accompanying the family to appointments. In addition, the intensity of an individual worker’s interactions is also required to match needs. Examples were given whereby visits may increase during times of crisis or periods of high stress (Al et al., 2012; Gillespie et al., 1995; Marcenko et al., 1996). Although the edge of care workers are viewed to be able to address or support a number of needs. There are some contexts which can be argued to be outside their influence, such as parental health issues such as severe mental health issues, abuse and substance misuse, whereby other services may need to be involved.
Programme theory 3 postulated that;

Programme Theory 4: Whole Family Approach
Core Mechanism: Whole Family Approach
Viewing the family as a whole system/unit rather than through its individual component parts (i.e., individual role of a parent/child etc.), behaviours and interactions can be understood in relation to how they influence the family or “system” balance (Al et al., 2012). Links to the interacting, systemic difficulties often seen can also be made. Behaviours are observed by workers as they are interacting with the family, and in doing so they are thought to be better placed to facilitate and encourage communication between family members residing in the house and facilitate activities which can be undertaken together (de Melo & Alarcao, 2012; Smith, 1995; Thomas et al., 2005). Central to the notion of a whole family approach is the acknowledgement of the requirement to understand the context of the family and to engage with/include all family members. This is so that individual family needs can be identified and addressed. This links to the previous concept of home-based response to individual need, and being able to observe family functioning, as it happens.
In taking a whole family approach, involving all members of the family, workers are seen as offering families respectful, empowering, and strength-based support based on their individual needs (de Melo & Alarcao, 2012). Building and promoting family resilience to better cope with needs is also prioritised through the development of a whole family approach to methods aimed at resolving conflicts and development of skills to improve interactions within the family (Mitchell, 2020; Smith, 1995; Thomas et al., 2005). Programme theory 4 therefore postulated;
Programme Theory 5: Rapid Response
Core Mechanism: Rapid Response
It was evident that edge of care related interventions needed to provide a rapid response, often immediate, to families in times of high stress/crisis (Dagenais et al., 2009; Forrester et al., 2008; Forsythe, 1992; Fraser et al., 1997; Hayward & Cameron, 2002; Mason, 2012, McWey, 2008; Parra et al., 2016; Scannapieco, 1993). Although the terms “high stress” and “crisis” were used in many of the papers, they were not defined. These terms were used within the literature to relate to any and all situations experienced which caused additional strain on the family. This time element often related to a requirement of quick engagement and was suggested to relate to assistance with resolving practical problems faced, as a precedent to promote further engagement with the worker (Parra et al., 2016). The reasoning often referenced with regards to the need for the service to be rapid was to assist families during times of high stress by providing the immediate capacity required to help families pass through crises without breaking down (Hayward & Cameron, 2002).
Programme theory 5 therefore postulated:
Step 4: Develop Narrative
Formal Theory
Within realist approaches there is a “to and fro” between the initial programme theory and more substantive (or formal) theory in order to enhance the explanatory potential of the programme theory (Dalkin et al., 2021). Throughout data extraction, formal theories explicitly stated within the literature (in terms of underpinning and providing explanation as to how the intervention created impact) were recorded. From the theories recorded, ecological systems theory, attachment theory, and crisis theory were identified to assist in the refinement of our own programme theories as they had the most explanatory potential. Table 4 below provides a brief summary for each of these theories and their application to family preservation services.
Theory Overview and Application to Family Preservation Services.

Advisory Group Consultation
Overall, advisory group members were supportive of the mechanisms/programme theories discussed and were able to suggest key points for refinement. At the initial core mechanism stage all mechanisms were agreed to be relevant and reflect core influential components of edge of care service provision. During the initial programme theory development consultation, a parent who had previously received support from edge of care services was able to provide valuable insight and examples as to how mechanisms interacted within their own context alongside examples given by staff connected to the edge of care service. Thus, providing practical based information as to how mechanisms link together and the potential outcomes they could produce. The final advisory group session consisted of four workers from an edge of care service. The refined programme theories were presented to the group, with a view to consolidate them.
Theory Refinement and Consolidation
Following the advisory group consultation (2 and 3—see Figure 2) and the incorporation of formal theory as described above the programme theories were refined and consolidated.
Programme Theory 1: Structured Parent and Family Skills Training
Initial programme theories were presented to the advisory group and discussions held in relation to their content, wording, and practical application. Through these discussions it was acknowledged that family skills training had to incorporate opportunities for families to reflect on their learning. That is, it must respond to real situations the family has found themselves in. The approach to training is also an important element in ensuring family engagement. Training was suggested to be counterproductive if it adopted a “teaching/instruction” approach as this would be perceived as “patronising” and “judgmental.” Training should be reflective and systematic as it promotes family confidence to manage and respond to situations, which they will find themselves in once the support has ended. An outcome from this approach, of the worker working with, rather than imposing on the family, is that the family is more willing to be open with the worker. In this situation it is acknowledged that it is okay to learn from mistakes and that skills training created hope and promoted the belief that things could get better for the family; that something was going to change.
It was highlighted how training can incorporate a number of different elements and whilst the content is often based on structured programmes, the training delivered to families is bespoke and delivered at times convenient to the family, reflecting the needs of the families, therefore the reference to “structured” was removed. Drawing on the premise of crisis theory, people in crisis often have reduced coping responses affecting their resilience and are more likely to be motivated to change, and open to learning new behaviours (Bezeczky et al., 2020; Fraser et al., 1997; Roberts, 2000). The interventions delivered by family preservation services therefore present opportunities for the families in crisis to reduce their skill deficit by learning new skills, identify mechanisms for coping and regain stability.
Programme Theory 2: Home Based Response to Individual Need
The importance of delivering services within a family’s home was echoed strongly by the advisory group. It was commented that in having services in the home, crisis points can be observed in real time with workers seeing what is “actually” happening rather than a recount of events, this assists in helping the family to feel understood and not judged by those working with them. It was also noted that families may present differently in public than at home so gives a real-life perspective for workers to better understand “triggers” to certain behaviours. However, it was felt important to stress that workers are not seen to be “phased” by behaviours witnessed and that it is very much observation and not surveillance within the home. It is also important to note contexts within which behaviours may not be appropriately addressed by the edge of care interventions, such as when power cannot be safely transferred to a family in the case of safeguarding incidents or abuse for example.
Drawing on both attachment and ecological theory, it can be suggested that many of the parents will it find it difficult to trust professionals and that workers may be perceived as threat, potentially as a result of pervious engagement with children’s services as a child. Therefore, having services delivered within the family’s home environment was suggested by the advisory group to remove barriers to engagement and shift the power dynamic. The worker is in the family’s home, and so power shifts away from the worker empowering the family. It was concluded that homework is really critical in being able to support families in “real” situations.

Programme Theory 3: Dedicated Worker Time
Having a dedicated worker was discussed to relate strongly to the need of having a flexible approach to the work. In addition, a dedicated worker allows for the high level of involvement (by the worker) required by crisis intervention approaches, in providing immediate relief and assistance. The advisory group commented that there is a need for the worker to work alongside and with the family, not to be “doing something to them” and for the family to “be ready” to accept assistance. Echoing findings from the literature, worker consistency, and reliability are said to be crucial in building trust with the family. This is also aligned with attachment theory.
However, it was stated that there is a need for workers to ensure they carry through with the actions they say they will do in developing trust and that they “always show up.” This is important in making the family feel like they matter, and their needs are important.
In addition to the dedication and intensive components of the workers approach to a family, discussions suggested that workers core beliefs in influencing their approach are also important. Workers must be seen to be genuine and able to focus on a family’s potential, promoting the belief that the family can be the drivers of their own change. Their need to convey understanding, care, compassion to the family, contribute to a non-judgemental approach. Support needs to be responsive, whether that it is in person or by phone. Ecological systems theory takes into consideration the dynamic and fluid nature of relationships within families (Hayes et al., 2017). This is central to edge of care services and the need for practitioners to adapt their approach to best engage with individual family members.

Programme Theory 4: Whole Family Approach
Ecological theory proposes that change cannot be made, or it would be very challenging to be achieved if the needs of the family are not addressed holistically. The concept of “whole family” prompted discussion within the advisory group and questions were asked on whether a true “whole family” approach can be taken. Examples were provided whereby often there is a focus on one member of the family, that is, a child and their disruptive behaviour—practitioners will focus on this and provide a whole family approach to resolving issues identified as the source of behavioural problems. Further, there may be a focus upon mothers as the primary caregiver, without recognition of the importance of intervening with the father for example to address the risk they present to the family (i.e., in cases of domestic violence) or as an important family resource to improve child outcomes. In addition, questions were asked as to what constitutes the family? It was commented that “family” is often wider than the “traditional” family with social and community networks having strong influences also.
Taking a whole family approach was viewed as an important concept which is threaded through all the other programme theories. It was therefore decided to remove PT 4 and ensure that reference to whole family approach is more explicit in the other theories.
PT 5: Rapid Response
The requirement for rapid response was echoed by the advisory group. Crisis theory states that interventions should be immediate, and action orientated, requiring a high level of involvement by the worker in the provision of immediate relief and assistance (Knox & Roberts, 2016). The notion of rapid response was discussed and suggested that it needed to include the family not waiting around whether this be the first visit or subsequent visits, the family not being given excuses, the worker needs to be there when they say they will be, and that it is essential that the family feels listened to and important. This can be achieved by simple acts such as being on the end of a phone when needed to provide re-assurance. This also links attachment theory in terms of understanding efforts required to build trusting relationships.

Discussion
The importance of providing effective edge of care interventions to prevent care entry for children and young people is not disputed. However, there is a need to further develop understanding of how these interventions work, and what is required for them to benefit the marginalised population they serve. This synthesis was undertaken to understand contextual factors and mechanisms pertaining to support for family preservation with children at the edge of care. Importantly, the programme theories developed and tested within this synthesis focused on explaining what it is within edge of care services that works, for whom and in what circumstances, in order to influence future edge of care service provision. In disaggregating context and mechanism components, alongside the associated outcomes they produce, generative mechanisms related to parent and family skills training, home based response to individual need, dedicated worker time, and rapid response are identified as central to effective edge of care service provision.
The provision of parent and family skills training delivered within edge of care was evident to some degree across all services. Parenting skill training has been found to improve the overall emotional and behavioural adjustment of younger (Barlow, 2016) and older (Zwi, 2011) children and parents (Barlow, 2012; Zwi, 2011), including families in contact with child welfare services (Gubbels, 2019). However, these reviews examine whether parent skills training “works.” Our synthesis builds upon this successive causal approach seeking to explain the generative mechanisms. We found that for parent and family skills training with families at the edge of care to be effective, it must be led by a professional with an understanding of the subtleties and dynamics already within the family to ensure that training delivered can directly reflect and be applied to day-to day family life and on-going family’s needs. In rooting the training in a detailed understanding of the family, training can be tailored in order that the family itself can be the driving force in its implementation, and thus fostering strengths and skills within the family, ultimately promoting empowerment.
Multiple studies have examined the effectiveness of “home-based interventions” for vulnerable families (Mullen, 2020; O’Farrelly 2021; van Assen et al., 2020), reporting benefits for vulnerable children and families, without examining the mechanisms which are activated by the context. In order for professionals to develop a contextual understanding of the family, they need to work closely and develop trust. In delivering edge of care services within the families’ own home, barriers to engagement from the family can be reduced. This approach also has the potential to help shift the power dynamic between the family and the worker, with more emphasis being placed on families taking the lead in their engagement with the edge of care service. Observations from the worker can also better reflect the family’s actual need as they are witnessing family dynamics within the home environment.
An important aspect of edge of care provision is aiding the development of trust. This is addressed through continuation of support from a single dedicated worker. In order to be effective, edge of care services need to work intensively with families, being there at times of need as well as more generally in order that the family feels supported. This intensity supports relational practice which has been suggested to be essential in achieving positive outcomes with vulnerable families (Ingram & Smith, 2018), allowing opportunities for the worker to deliver both practical and therapeutic assistance in direct response to the family’s needs at a time when they need it. The aim of this assistance links back to the notion of parent and family skills training. In working intensively with the family, the worker can build trust and identify what support is required, whilst also addressing resistance that might be generated from previous and on-going child protection service involvement (Forrester, 2012). In delivering this support in the home environment, the family can be empowered and supported to take control for themselves and promote positive family functioning. In addition, building trust with a worker can assist with changing preconceptions of edge of care and wider support services within a population who have generally had negative experiences engaging with services. This is seen to result in more effective engagement with edge of care services and increased positive engagement with wider services.
Strengths and Limitations
This synthesis brings together data from a number of different edge of care service provisions. In doing so we have been able to identify key mechanistic components that influence edge of care service delivery. Through this approach we have been able to identify further outcomes from such service provision which go beyond a child not being taken into care. However, through the synthesis we found that papers were not always explicit about the “type(s)” of problems families experienced which has limited our understanding of the contextual conditions surrounding and influencing the identified mechanisms and thus the outcomes they produce.
A key strength of the synthesis was the incorporation of advisory group consultation at key points within the data collection. This consultation allowed for emerging findings to be discussed with key stakeholders connected to edge of care service delivery in England and provided a platform to discuss, test and refine our thinking as the synthesis progressed. In addition, we were able to explore practical based information as to how mechanisms link together and the potential outcomes they could produce, thus ensuring the synthesis could produce meaningful practical outcomes.
A key weakness of the synthesis was the lack of cultural diversity in the included papers. Also, in terms of selection bias, most papers included all families/individuals who accessed the service being reported on and did not include those who had declined support from the service. The literature focused on when interventions do work, and therefore information is missing in respect of when edge of care provision might not work, who it might not work for or the situations that it does not work within. In addition, mechanisms and contexts were rarely explicitly stated within literature. In the context of community delivered interventions, it is therefore not possible to unpack all the intricacies related to the implementation of the approach(s) within available secondary literature. We therefore may have missed identifying mechanisms and contexts within which they operate.
Our synthesis focused on identifying and exploring core components which enable edge of care services to be effective. There are components that, in direct contrast to this, prohibit or reduce effectiveness of such interventions. Investigating these components in more detail will further evidence the development and refinement of future services in order to avoid what is evidenced to “not” work.
Conclusion
This synthesis has highlighted specific contextual, mechanist and outcome configurations which contribute to the developing evidence as to how edge of care services are able to benefit the populations they serve, with the ultimate aim of reducing the number of children entering care. In generating evidence-based understandings in the form of programme theories relating to the effective components of edge of care service provision, and using formal theories to enhance their explanatory potential, this research is able to inform development and delivery of future edge of care services. Through disaggregating context and mechanism components, alongside the associated outcomes they produce, generative mechanisms related to parent and family skills training, home based response to individual need, dedicated worker time, and rapid response are identified as central to effective edge of care service provision.
The realist synthesis approach taken has provided additional insights into the workings of edge of care services, and what it is that makes them effective, which goes beyond outcomes typically generated through more conventional methodologies.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241260998 – Supplemental material for Mechanisms That Promote and Support Family Preservation for Children at the Edge of Care: A Realist Synthesis
Supplemental material, sj-docx-1-sgo-10.1177_21582440241260998 for Mechanisms That Promote and Support Family Preservation for Children at the Edge of Care: A Realist Synthesis by Sam Redgate, Deborah Smart, Simon Barrett, Carrie Barron, Samantha Burns, Hilda Frost, William McGovern, Vikki Peart, Emma Adams, Hayley Alderson, Eileen Kaner and Ruth McGovern in SAGE Open
Footnotes
Acknowledgements
We would like to thank our practice partners, Julie Firth, Tara Renwick and Pete Xeros from North Tyneside Council for their valuable insight and input into this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by ARC NENC open funding. EAA was supported by the NIHR School for Public Health Research (SPHR) Pre-doctoral Fellowship, Grant Reference Number PD-SPH-2015 and is now supported by the NIHR Applied Research Collaboration (ARC) North East and North Cumbria (NENC) (NIHR200173). EK holds an NIHR Senior Investigator award, as well as being Director of the NIHR ARC North East and North Cumbria. The views expressed are those of the authors and not necessarily those of the NIHR, Department of Health and Social Care, or any of the other funding or organisational bodies.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.