
Abstract
Cultural competence is a continuously developing process that requires transition-to-practice program training to enable new graduate nurses (NGNs) to transfer their knowledge and skills to clinical practice in a culturally sensitive manner. The development and implementation of residency programs, including a cultural competence curriculum, could support this transition. This study aimed to evaluate the preliminary effects of a hybrid learning module of cultural competence for NGNs. A quasi-experimental design was used in a 3,000-bed hospital in North Taiwan. We randomly allocated 37 NGNs to the experimental and control groups. The Cultural Competence Scale for Pre-Graduate Students to Licensed Professionals (CS-SP) was adopted to measure cultural competence before and after the intervention. We evaluated the correlations between learning time and cultural competence scores using a paired t-test, chi-square test, and Mann–Whitney test for statistical analysis. The curriculum for the learning application comprised three courses covering six topics. The experimental group scored significantly higher in awareness and skills after the intervention (p < .05), but there was no significant improvement in knowledge or self-efficacy. The control group showed no significant differences in any of the cultural competence subscale scores after intervention. The Mann–Whitney test showed that different learning times led to significant differences in the mean cultural competence scores (Z = 3.04, p < .05). Integrating cultural competency education into web-based NGNs’ postgraduate year of nursing programs improved their cultural competence awareness and skills. The learning application can be adapted to target NGNs at different stages of the postgraduate year of nursing programs to maximize its benefits.
Plain Language Summary
New graduate nurses (NGNs) need to develop the cultural competence to provide sensitive care to diverse populations. One way to achieve this is through a residency program. To test the effectiveness of a hybrid learning module on cultural competence, a study was conducted in a hospital in North Taiwan. 37 NGNs were randomly assigned to experimental and control groups, and their cultural competence was assessed using the Cultural Competence Scale for Pre-Graduate Students to Licensed Professionals (CSSP) before and after the intervention. The web-based learning application included three courses covering six topics, which were integrated into the in-service education and training courses prescribed by the Taiwan government. The module design followed the American Association of Colleges of Nursing education curriculum to ensure that nurses acquire sufficient knowledge, attitudes, and skills for cultural competence. Mentors coached the learning objectives, and the experimental group showed improvement in awareness and skills. However, there was no significant improvement in knowledge or self-efficacy, and the control group did not show any significant improvement. The study found that integrating cultural competence education into the web-based NGNs’ nursing residency program improved their awareness and skills. The learning application can be adapted for NGNs at different stages of the residency program for maximum benefits. Future studies should include more participants and develop new content for cultural competence training at different stages of the program.
Keywords
Background
Cultural competence and skills are important aspects of professionalism for nurses to provide quality healthcare while considering culturally sensitive issues such as language barriers and cultural norms to religious beliefs and customs (Vandermause et al., 2021). Nurses with higher cultural competence may improve their support for patients to manage their disease (Dyrehave et al., 2022), perform better health behaviors, be involved in their own care, and equip themselves with knowledge and understanding of their disease (Faber, 2021). The World Health Organization (2009) emphasized the importance of providing cultural competence training as a global standard for the initial education of professional nurses and midwives. Additionally, International Council Nursing (2013) stated that nurses should be culturally and linguistically competent in order to understand and effectively respond to the cultural and linguistic needs of clients, families, and communities in a healthcare encounter.
Educational preparation and ongoing training in cultural competence are essential for healthcare professionals (Jongen et al., 2018). Continuous acquisition of skills, knowledge of practices, and adoption of appropriate attitudes enable nurses to demonstrate cultural competence while establishing rapport and understanding of clients’ language-related health and illness (Debiasi & Selleck, 2017). Newly graduated nurses (NGNs) struggle during their transition to professional practice, which can hinder their ability to learn about cultural competence (Murray et al., 2019), particularly within the first 3 months (Chang et al., 2019). Due to their limited experience in clinical care, NGNs may have high levels of cultural knowledge but lower levels of cultural competence skill.
Nurse residency programs with training schemes were designed to help NGNs’ transition from students to RNs (Ackerson & Stiles, 2018). Hybrid learning, which integrates both face-to-face and technologically mediated interactions between students, teachers, and learning resources, can positively impact the achievements of pre-registration nursing students (Jowsey et al., 2020). Lu et al. (2016) proposed a hybrid learning approach that uses online videos and in-class teaching in nursing residency programs.
A systematic review reported that cultural competence education was mainly offered through traditional face-to face teaching to participants (Oikarainen et al., 2019). Recent studies have demonstrated the effectiveness of cultural competence training using online or technological methods, such as Facebook-based education for healthcare students (Chang et al., 2017), e-learning for public health workers (Chae et al., 2021), web-based education for palliative care nurses (Bhat et al., 2015), and mobile applications for RNs (Sung & Park, 2021). As such, online learning programs could be a useful strategy for improving clinical skills under time restrictions for health professionals, such as nurses during the COVID-19 pandemic or night shifts (Al-Mugheed et al., 2022; Slobodin et al., 2021; Wilson et al., 2018).
In this study, we developed and tested a hybrid learning module consisting of a web-based application for cultural competence learning and three face-to-face case discussions with mentors. This study describes the development and distribution of learning modules among NGNs. Additionally, this study examined the effectiveness of the hybrid learning module in increasing NGNs’ cultural competence.
Methods
Study Design
This study used an experimental pre-test and post-test design.
Participants and Setting
We recruited NGNs from a hospital in Northern Taiwan with 3,000 beds who met the following inclusion criteria: (1) newly graduated and qualified; (2) had worked for more than 1 week but less than 3 months and had not begun the nurse residency program; and (3) were working in internal medicine or surgery wards.
The exclusion criteria were as follows: (1) nurses who had participated in a nurse residency program before or (2) nurses scheduled for a night shift in the first 3 months after graduation because they were unable to meet with a mentor to discuss cases. We used G*Power, Version 3.0 (Faul et al., 2007) to calculate the total sample size required for a medium effect size of 0.50, a power of 0.80, and a significance level of .05. According to the results, we needed a sample size of at least 20 participants for each group.
The principal investigator provided details of the study to the hospital administrator, who then forwarded the information and consent to the NGNs via the hospital email service. A total of 90 NGNs met the inclusion criteria and were invited to participate in this study; of these, 40 (44.4%) agreed to participate and provided their email address to us. We used Microsoft Excel’s random-selection function to assign computer-generated code numbers for the agreed participants and randomly allocated 20 participants each to the experimental and control groups. The NGNs in the intervention group (N = 20) received security codes to log into the website. Control group participants (N = 20) received written guidelines and were informed about library resources. Throughout the study, we concealed NGNs’ group allocations from their mentors. Figure 1 shows a schematic overview of the study design and the participant flow.

The study design and participant flow.
The Hybrid Learning Module
The module design in this study was based on the American Association of Colleges of Nursing (2008) education curriculum to ensure that nurses attain cultural competence by acquiring sufficient knowledge, attitudes, and skills. We integrated the components of cultural competence into the 3-month in-service education and training courses for NGNs in the 2-year postgraduate training programs prescribed by the Ministry of Health and Welfare (Taiwan) (2020) and adopted the learning experiences of cultural competence revealed in our previous study (Chang et al., 2019) to design the topics of three courses for NGNs (Figure 2).
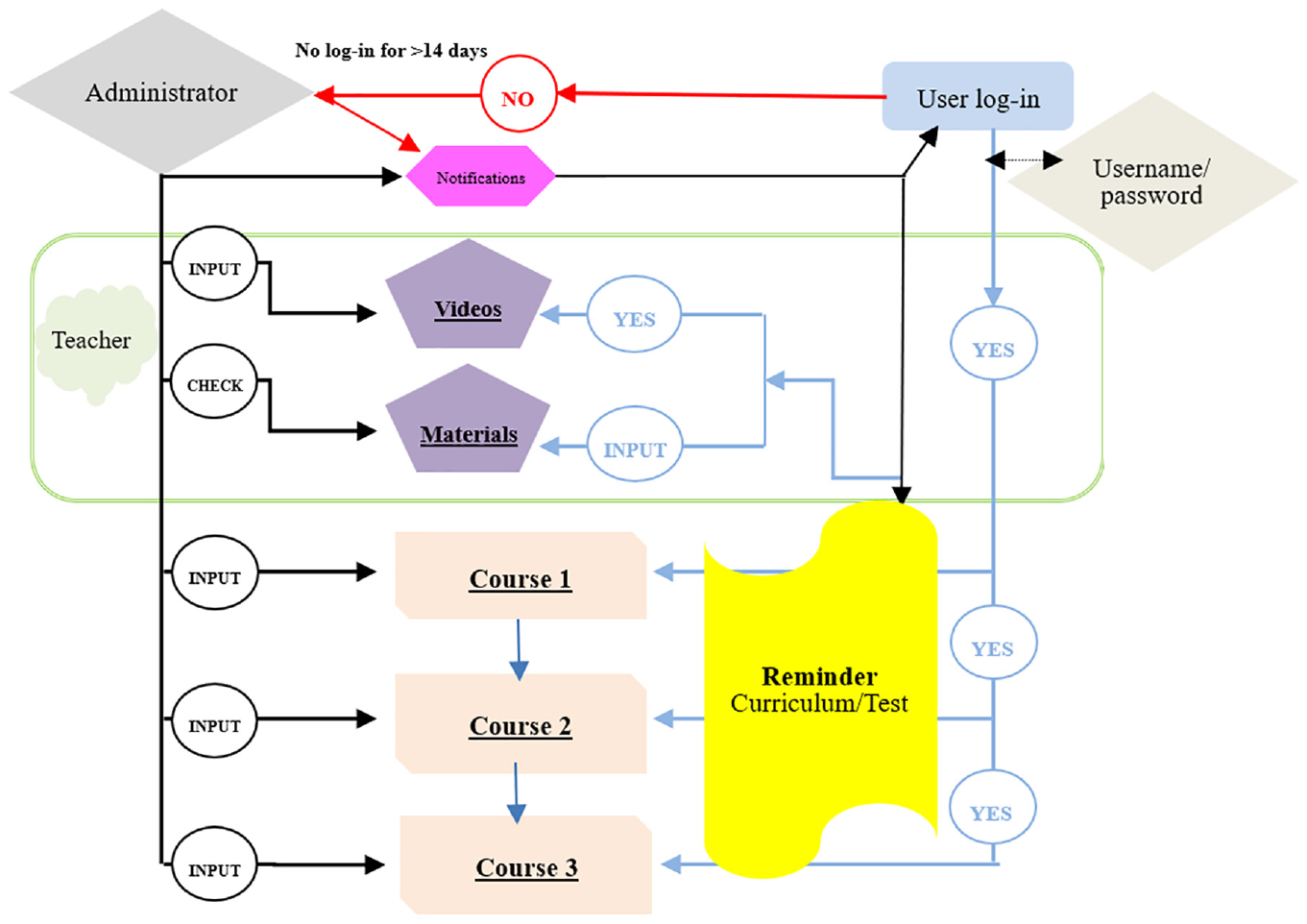
Flowchart of learning application on cultural competence for NGNs.
Web-Based Learning Application of Cultural Competence
As shown in Table 1, the curriculum comprised three courses and six topics, with each topic lasting 20 min (120 min total). The NGNs consecutively completed the topics over 3 months. Participants were able to study at their own convenience, and the backend program accumulated their study hours to verify their level of completion. Additionally, the program kept track of the total number of participants who had completed all six topics.
Objectives and Content of Learning Modules in Web-Based Applications.

The themes for the three courses were based on modules stipulated by the nursing residency program, which were delivered using videos, audiovisual presentations, and reflective feedback forms. Cultural competence courses were designed based on NGNs’ learning experiences regarding culturally diverse patient populations, covering topics such as diet, religion, ethnicity, and language (Chang et al., 2019). Moreover, the videos were heavily drawn from life experiences and news events to reflect and enhance the understanding of cultural differences (Antón-Solanas et al., 2021). For example, Modules 1-2 in Course 1 cover the topic of dietary habits. In these modules, a case study on the dietary habits of Muslim women was presented using a video produced by our team. A multicultural approach to different dietary habits was then explained, followed by a discussion between the participants and the mentors on the content of the assessment during hospital admission. Each video was less than 5 min, and the audiovisual presentations were limited to 15 min to avoid overwhelming learners. We can verify on the platform whether students have fully viewed the video (see Figure 3).

Screenshots of the main page, courses, reflection board and record area.
Case Discussions With Mentors
NGNs met with their mentors for 1 hr every month in the first 3 months of the 2-year postgraduate training program. Each session introduced cultural competence practice along with learning objectives, which were coached by mentors. Participants identified the key details important to their cultural competence skills in caring for their clients. The process of reflective discussion for sharing different or alternative perspectives on educational articles and materials was also documented by participants as part of their training assignments.
Measurements
We collected the following data through self-reported questionnaires on the web-based learning application.
Demographic data from the participants: gender, ethnicity, highest degree earned, cultural competence education during nursing school, and experience of caring for patients from diverse cultures.
Culture competence: The Cultural Competence Scale for Pre-Graduate Students to Licensed Professionals (CCS-SP) was adopted to assess cultural competence. The Chinese version of the 49-item CCS-SP underwent a multistep validation process, including interviews with health professionals and people from multiple ethnic populations, item reduction based on exploratory factor analysis, and internal consistency analysis (Chang, 2013). Confirmatory factor analysis results revealed that a second-order latent factor model of the CCS-SP with 26 items supported a four-factor solution with favorable convergent and divergent validity, accounting for 62% of the variance in cultural competence (Chang et al., 2017). Of the 26 items, four concerned knowledge, including two true/false questions, on which the participants were scored according to the number of correct answers they provided. The remaining 22 items, which were scored using a five-point Likert-type scale, included three items concerning awareness (5 = strongly agree, 1 = strongly disagree), nine items concerning self-efficacy (5 = 100% confident; 1 = 0% confident), and ten items concerning skills (5 = always; 1 = never). The total score was 114, and higher scores indicate greater cultural awareness, self-efficacy, and skills. Completing the online assessment took approximately 10 to 15 min.
Moreover, we also accumulated the learning time that participants enter and stay in the web-based learning application of cultural competence to confirm the completion of each course and by dividing the cumulative time by the total learning time of 120 min.
Data Collection
The experimental group received an email within 2 weeks of agreeing to participate and signed the consent form. The email provided login information, enabling them to register on the learning app in April 2020. The pre- and post-intervention tests in this study were conducted online via hyperlinks to a Google Docs questionnaire. We sent email and SMS reminders to any participant who did not log in within 1 week to complete the pre-intervention questionnaire or failed to log in for more than 2 weeks during the learning process. Participants who failed to log in for more than 1 month were considered to have declined to participate and were excluded from the study. The participants in the experimental group completed the post-intervention test within 1 week of completing all modules. Those who failed to complete the post-intervention test were prompted to do so via SMS.
The control group received paper-based pre-intervention test questionnaires and took part in the current postgraduate year (PGY) curriculum (in-class and online courses) after completing the questionnaires. We conducted the post-intervention tests after both groups had completed 3 months of learning.
Ethical Considerations
This study was reviewed and approved by the Regional Ethical Review Board of Taoyuan Gang Gung Memory Hospital (no. 201700220B0). The principal investigator provided the hospital administrator with details of the study and forwarded the information to NGNs via the hospital’s internal email system. The NGNs who agreed to participate and submitted their written consent forms received an email detailing the study procedure. Only participants who completed both the pre-and post-intervention questionnaires and educational courses received a gift voucher worth US$5 mailed to the address they provided.
Statistical Analysis
We compared the baseline characteristics between the two groups using independent t-tests for continuous variables and chi-square tests for categorical variables. Descriptive analyses were performed using mean ± standard deviation and percentage (number), and intergroup comparisons were conducted using Fisher’s exact test and t test. However, as the assumptions of normality and equal variances are not met, we performed the Mann–Whitney–Wilcoxon test, a nonparametric statistical test, to compare the learning time and cultural competence scores during the three-month learning period. The statistical significance was set at p < .05. For data processing and statistical analyses, we used IBM SPSS Statistics for Windows, Version 23.0 (Armonk, NY: IBM Corp.).
Results
Table 2 shows the demographic characteristics of the participants in each group. All the participants were women. Most participants were of Hokkien ethnicity and had university degrees. A total of 67.57% had experience caring for patients from diverse cultures and special population groups, 10.81% had learned cultural competence in school, and 16.22% were fluent in English. There were no statistically significant differences between the groups in terms of demographic and descriptive characteristics.
Demographic Data and Cultural Competence Subscales of Participants (Baseline Measurements).

Note. χ2 is Fisher’s exact test. M = mean; SD = standard deviation.
Table 3 describes the results for cultural competence, knowledge, awareness, self-efficacy, and skills within the study groups across the periods. The experimental group had significantly higher scores for awareness and skills in the post-intervention test than in the pre-intervention test (p < .01, p = .05, respectively). We found no significant improvement in knowledge or self-efficacy. The control group showed no significant differences in the scores on any of the cultural competence subscales between the pre-and post-intervention tests. We found no significant changes in the total cultural competence scores of the experimental and control groups over the 3-month learning period (Table 3).
Comparison of Cultural Competence of NGNs in Intervention and Control Groups.

p < .05. **p < .01.
The cumulative learning time of the experimental group was 80.69 min (SD 12.21; range 41.38–120 min). We divided the participants into two groups according to the learning time: 41 to 80 min and 81 to 120 min. The mean cultural competence score of those with a learning time of 41 to 80 min was 89.89, increasing by 7.60 over the mean pre-intervention test score. Those with a learning time of 81 to 120 min scored an average of 93.18, an increase of 9.89 over the mean pre-intervention test score. The Mann–Whitney test showed that different learning times led to a significant difference in the mean cultural competence scores (Z = −3.04; p < .05), implying that extended engagement periods in learning resulted in higher cultural competence scores (Table 4).
Differences Between Cumulative Learning Time and CC Scores During the 3-Month Program.

Note. CC = cultural competence; MD = mean of difference.
p < .05.
Discussion
This study integrated cultural competence into a nurse residency program using a hybrid learning module. NGNs who adopted this method had significantly higher cultural competence awareness and skills than those who participated in the conventional PGY curriculum. Research has shown that practical hands-on training experiences provide more effective instruction for NGNs than visual, verbal, or aural teaching strategies (Yu et al., 2021). NGNs want to learn and practice specific procedures, protocols, and specialized knowledge when they begin working professionally (Lee et al., 2019). Training in clinical scenarios, including hands-on and simulation-based training, has been shown to improve skill-related outcomes in NGNs (Kim et al., 2018).
Aggar et al. (2021) investigated the use of smartphone-and tablet-based learning systems to assist NGNs in their communication and leadership skills. They found that the application significantly improved NGNs’ self-efficacy, leadership, and communication skills. Moreover, NGNs rated it highly for easy accessibility and the interactive function of learning feedback. Similar to previous studies, we found that hybrid learning approaches for NGNs, including both in-person and web-based courses, can positively influence NGNs’ cultural competence awareness and skills (Jowsey et al., 2020).
In this study, a web-based app was used to integrate cultural competence into the postgraduate year of nursing programs for NGNs, and the hybrid learning module app improved awareness and skills in cultural competence by integrating lecture learning and case discussion. Increasing awareness is the first step toward improving cultural competence. According to the study of Antón-Solanas et al. (2021), we adopted videos heavily drawn from life experiences and news events that provided NGNs with reference models to guide them when considering the needs and preferences of diverse patient populations. NGNs also honed their multicultural care skills through clinical discussions with NGN mentors. Similarly, Leung et al. (2021) found that internationalization-at-home activities could influence postgraduate health and social science research students to become more culturally aware. Interaction experiences of nursing staff with different cultural groups are considered as an important approach to enhance cultural awareness (Kaihlanen et al., 2019). Vandermause et al. (2021) examined the benefits of dramatization in exploring how nurses internalize messages about cultural differences. Additionally, McLennon et al. (2019) mentioned that cultural competence could be improved through various learning strategies, such as lectures and participatory activities. However, the course intervention in our study did not result in a significant increase in cultural knowledge or self-efficacy. Similar to our previous study, NGNs have a high level of cultural knowledge and self-efficacy (Lin et al., 2021). In this study, the knowledge and self-efficacy scores for NGNS were up to 70%, which increased slightly but not significantly after the intervention.
The time students spend learning on digital devices is a critical factor in their lesson internalization and attainment of learning outcomes (Karay et al., 2020). Our study showed that the completion rate for learning time was 67.2% and that the duration of learning time was related to NGNs’ post-intervention cultural competence scores. This finding is consistent with that of Doughty et al. (2021), who found that training completion significantly elevated NGNs’ clinical care ability. Few studies have analyzed the association between digital learning time and outcome differences. However, Nicoll et al. (2018) have found that formative learning assessments are necessary to present the outcomes of mobile learning. Our results showed a learning time completion rate of 67.2%, suggesting the need for a more in-depth analysis of the factors affecting learning times. Additionally, an analysis of the barriers and benefits of NGNs’ learning input could help improve the cultural competence curriculum design of nursing residency programs.
Limitations
This study had several limitations. We conducted our study at a single hospital with a small sample size, which limits its generalizability. Since this course involved voluntary participation and was adapted to the NGNs’ training schedule, the range of eligible participants was limited. As only 37 participants could be recruited, when divided into experimental and control groups to measure the study outcomes, there were less than 20 participants in each group. Future research could extend the recruitment time and expand the participant population to include NGNs at other medical facilities and at different levels to increase the sample size. Additionally, this study only analyzed learners’ outcomes and not instructors’ evaluations of their cultural competence. Future research should identify a more reliable means of collecting clinical data to substantiate the true impact of educational programs in the clinical setting.
Conclusions
Integrating cultural competence into NGNs’ nursing residency program using a web-based app improved their cultural competence awareness and skills. Those with a learning time of more than 60% scored significantly higher in cultural competence than those with a learning time below 60%. This application does not require a separate training program for cultural competence. It also allowed trainees in the PGY program to holistically develop cultural competency care. Hospital administrators must monitor NGNs’ learning time and incorporate bedside discussions to enhance their learning engagement. Future studies should recruit larger study samples and develop new content for cultural competence training targeted at NGNs at different stages of the nursing residency program, which would enhance the existing learning program and maximize the benefits of the app.
Footnotes
Acknowledgements
We thank all the participants in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Taiwan National Science and Technology Council (grant number: NSTC 102-2511-S-255-002-MY3 and NSTC 106-2511-S-255-011) and Chang Gung Memorial Hospital (grant number: BMRP 978 and CDRPF1H001).
Ethics Approval and Consent to Participate
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Regional Ethical Review Board of Taoyuan Gang Gung Memory Hospital (no. 201700220B0). Informed consent was obtained from all subjects involved in the study.
Consent for Publication
Not applicable.
Availability of Data and Material
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.