
Abstract
The Domestic Violence Questionnaire (DVQ) is a measure that captures physical, sexual, economic, and psychological violence perpetrated against women. A team of local academicians and intervention experts evaluated several tools for domestic and gender-based violence, concluding that the DVQ fitted best in the context of evaluating the Living Peace intervention in conflict-affected eastern DRC. The purpose of this validation study was to: (1) validate the factor structure of the Swahili version of the DVQ, (2) to evaluate its convergent and divergent validity, and (3) to examine its internal consistency reliability. The factor structure was evaluated using Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) while concurrent validity and internal consistency reliability were evaluated using Pearson correlation and Cronbach’s alpha coefficients, respectively. The study participants were women, partners of men that participated in the Living Peace program, a community-based intervention program that works on promoting positive masculinity among men that are perceived to be violent by their community. Data were obtained from two independent purposive samples of 704 participants for EFA and 878 participants for CFA, selected from 60 villages in North and South Kivu, DRC. The results indicated that five and three-factor structures could be meaningfully interpreted in EFA, each with 66% explained variance. For comparative purposes, CFA was conducted on the two newly created factor models and the original factor model. All models reach good fit indexes, with the three-factor model demonstrating the best fit. Its standardized factor loadings ranged from 0.57 to 0.91. The internal consistency was α = .90 for the total scale and ranged from α = .75 to .926 per dimension. Finally, scores of DVQ were negatively correlated with mental well-being (r = −0.23, p < .001), and positively with depression (r = .435, p < .001), as hypothesized. The Swahili version of DVQ has excellent psychometric properties and can be applied to evaluate the physical, sexual, economic and psychological violence in victims of domestic violence in humanitarian crisis settings.
Plain Language Summary
The purpose of this validation study was: (1) To validate the factor structure of the Swahili version of the DVQ, (2) to evaluate its convergent and divergent validity, and (3) to examine its internal consistency reliability. The factor structure was evaluated using Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) while the concurrent validity and internal consistency reliability were evaluated using Pearson correlation and Cronbach’s alpha coefficients, respectively. The study participants were women, partners of men that participated in the Living Peace program, a community-based intervention program that works on promoting positive masculinity among men that are perceived to be violent by their community. Data were obtained from two independent purposive samples of 704 participants for EFA and 878 participants for CFA, selected from sixty villages in North and South Kivu, DRC. The results indicated that five and three-factor structures could be meaningfully interpreted in EFA, each with 66% explained variance. For comparative purposes, CFA was conducted on the two newly created factor models and the original factor model. All models reach good fit indexes, with the three-factor model demonstrating the best fit. Its standardized factor loadings ranged from 0.57 to 0.91. The internal consistency was α = 0.90 for the total scale and ranged from α = 0.75 to 0.926 per dimension. Finally, scores of DVQ were negatively correlated with mental well-being (r = −0.23, p < 0.001), and positively with depression (r = 0.435, p < 0.001), as hypothesized. The Swahili version of DVQ has excellent psychometric properties and can be applied to evaluate the physical, sexual, economic and psychological violence in victims of domestic violence in humanitarian crisis settings.
Keywords
Introduction
Eastern Congo is affected by extreme violence and conflict for several decades. It is estimated that more than 5 million people have lost their lives since 1988 (Kelly et al., 2021). The conflict-affected provinces of North and South Kivu, the geographical focus of this study, have been among the areas with the highest rates of violence and rape due to several armed groups (Kelly et al., 2021; Peterman et al., 2011). It is estimated that more than 120 militias and armed groups are active in eastern DRC (Global Centre for the Responsability to Protect, 2022) with an estimated 2,487 civilians killed by armed groups in North Kivu and South Kivu in 2020. Worryingly, a growing number of studies are documenting how living in a conflict-affected place may increase the risk of interpersonal violence, including domestic violence (DV), even long after the conflict is over (Kelly et al., 2021). In Liberia for instance, residents in more heavily conflict-affected districts were associated with a 50% increased IPV risk four years after formal peace was declared (Kelly et al., 2018). Therefore, the greatest threat of violence women face in the Democratic Republic of Congo (DRC) may not be from strangers but from their partners in their own homes (Peterman et al., 2011). DV is defined as “a behavior within an intimate relationship that causes physical, sexual, or psychological harm, including acts of physical aggression, sexual coercion, and psychological abuse and controlling behaviors” (WHO, 2010).
The prevalence of DV against women in humanitarian crisis settings like eastern DRC is high. The 2014 DRC Demographic and Health Survey (DHS) found that above 2/3 of ever-married women had experienced sexual, physical, or emotional violence by an intimate partner (Le Roux et al., 2020; Tlapek, 2015), placing the country at nearly twice the global prevalence (i.e., 1/3) of this form of violence (WHO, 2021). This figure is not significantly different from the prior 2007 DHS showing that 71% of women in DRC reported having experienced physical and emotional abuse in their homes (DRC Ministry of Planning, 2008). Using a different methodology, the Promundo’s IMAGES study (International Men and Gender Equality Survey), 45% of women in the Eastern DRC reported having ever experienced physical violence and 49% had ever experienced sexual violence from their partners (Le Roux et al., 2020; Slegh et al., 2014). The IMAGES authors further highlighted that rape as part of the conflict was reported by 22% of women. Happening in the homes, DV may still be underestimated as it may not be reported and may be accepted or condoned due to cultural norms and taboos that inhibit speaking out against this form of violence (Kelly et al., 2021; Ministère du Plan et Suivi de la Mise en œuvre de la Révolution de la Modernite et al., 2014; Parmar et al., 2012; Peterman et al., 2011).
Being a patriarchal society (Jonas et al., 2022), discrimination against Congolese women in all areas—health, education, access to economic and political rights and justice (Davis et al., 2014; WHO, 2021). Beliefs such as the one that men have a “right to sex” even if women refuse supported by 62% of North Kivu women and 48% of North Kivu men (Bronte, 2020) contribute to justifying sexual assaults. Similarly, almost a third of the men questioned stated that women “sometimes want to be raped,” and that a woman sexually assaulted «may enjoy it» (WHO, 2021). Additionally, there are other traditional believes that are misogynistic, such as the belief that having sex with a virgin confers power, good luck and even cures HIV/AIDS, a superstition behind the rape of young girls (WHO, 2021). About stigma, Congolese women and girls receive negative reactions from their community when disclosing violence experiences especially Sexual Violence (SV) (Murray et al., 2018). Community members’ blame might harm survivors’ relationships and marriageability (Glass et al., 2012; J T Kelly et al., 2011). Focus groups with SV survivors in the Democratic Republic of the Congo (DRC) found that survivors may experience barriers to revenue production and farming activities (Kelly et al., 2011). Loss of capacity to sustain one’s family can contribute to greater marginalization and loss of survivors in a vicious circle of marginalization and loss (Glass et al., 2012). This isolation can be severe; according to a research conducted in the DRC, 12.5% of SV survivors seeking medical assistance reported being compelled to leave their homes (Steiner et al., 2009).
Domestic violence is a public health and human rights issue given its magnitude and long-lasting consequences (WHO, 2010, 2019). The frequency and severity of domestic violence was repeatedly found to be associated with negative outcomes. Even so-called low levels of violence such as “pushing or shoving” are associated with depression (Mason & O’Rinn, 2014). Prior research has shown women who experienced DV have a risk of developing physical problems (Cheung et al., 2009; Imanishimwe et al., 2020; Kapiga et al., 2017), including difficulty accessing and using antenatal care services for pregnant women (Bahati et al., 2021), as well as mental health issues (Kapiga et al., 2017). Physical, sexual, psychological or emotional violence is positively associated with depression, low self-esteem, and PTSD (Calvete et al., 2007; Sharma et al., 2021) and negatively associated with mental well-being (Mootz et al., 2020).
To address the detrimental effects of DV, several authors developed and validated different tools to access domestic violence against women in many countries. The most commonly used tools are the domestic violence questionnaire (Indu et al., 2011); the abuse assessment screen (Weiss et al., 2003); the composite abuse scale (Hegarty et al., 2013); the conflict tactics scale-2 (Tiwari et al., 2010); the humiliation, afraid, rape, kick (Sohal et al., 2007); the hurt, insult, threaten, scream (Iverson et al., 2015); the index of spouse abuse (Cook et al., 2003); the ongoing abuse screen (Weiss et al., 2003); the ongoing violence assessment tool (Ernst et al., 2004); the parent screening questionnaire (Dubowitz et al., 2008); the partner violence screen (MacMillan, 2006); the slapped, things, threaten (Paranjape & Liebschutz, 2003); and the woman abuse screening tool (Wathen et al., 2008). A team of local academicians and intervention experts evaluated the content of the aforementioned tools looking at factor denominations and item formulation, concluding that the DVQ fitted best with the purpose of evaluating the impact of the Living Peace intervention in Eastern DRC. Furthermore, literature review and prior qualitative research, including the IMAGES study (Slegh et al., 2014) informed the decision (Basile et al., 2007; Indu et al., 2011; Tlapek, 2015; White et al., 2000; Zolotor et al., 2009).
According to the DVQ developers, items to measure domestic violence were selected from two questionnaires from India—the National Family Health Survey-3 Questionnaire (International Institute for Population Sciences, 2007) and the India SAFE Questionnaire (Kumar et al., 2005). The authors selected 11 items from the former, nine items from the latter, and six items commonly from both. They further conducted qualitative interviews for dimensionality and comprehensive coverage of items where 3 items were added based on expert opinion. Thus, a 29-item questionnaire was initially constructed with 17 and 12 items measuring psychological and physical (including sexual) violence respectively (Indu et al., 2011). The items of this questionnaire were conceived to represent the domains of physical, sexual and psychological violence, but Exploratory Factor Analysis (EFA) revealed five factors. “physical violence, controlling behavior, insulting behavior, neglecting behavior, and economic restriction” that explained 71.14% of the variance among the observed variables (Indu et al., 2011). The exploratory factor analysis also informed that 20 items to be retained in the final DVQ 13 items for psychological violence (i.e., controlling behavior, insulting behavior, neglecting behavior, and economic restriction) and 7 items for physical violence. The DVQ is a short, simple, self-administrable and discriminative instrument (Indu et al., 2011).
The current study aimed to examine the psychometric properties of the domestic violence questionnaire for the Congolese population. We hypothesized that the scores on DVQ would fit the five-factor model of the DVQ. We further hypothesized that the total scores of DVQ would be strongly and positively correlated with depression symptoms, but negatively correlated with mental well-being to confirm construct validity.
Methodology
Study Design
This cross-sectional study was conducted to examine the psychometric properties of the domestic violence questionnaire among adult Congolese women.
Sample
The sample was purposive made up of Swahili women speakers (N = 1,582) whose partners (husbands) are beneficiaries of the Living Peace intervention (LPint) in the eastern DRC. To be included in the LPint, men needed to be aged at least 18 years, living in a couple with a woman, and able to read and provide a written consent form in Swahili. In addition, men needed to be “perceived by community members as being violent.” To make such a determination, LPint facilitators collaborate with community leaders, family members, police and military hierarchy to select participants based on a consensus process. Community leaders and camp authorities were trained to have a common understanding of the identification of such families in their community or camp.
Measures
Data were collected using the 20-item Domestic Violence Questionnaire(Indu et al., 2011), the 15-item Hopkin Symptoms Checklist-depression subscale (Derogatis et al., 1974) and the 14-item Warwick-Edinburg Mental Wellbeing Scale (Clarke et al., 2011). The tools were adapted to the context of DRC (no items were removed and no major change in item content was needed) and translated into Swahili before the data collection process. In this process, a team of academic and field practitioners decided that the items of all scales should be scored on a 7-point Likert scale: Strongly disagree (1), to strongly agree (7).
Data Collection
Household-based, interview style using tablets. The data were collected as part of a larger RCT (Jansen et al., 2022). Data from the baseline were used and EFA and CFA were performed on group 1 (case group of the RCT) and group 2 (control group of the RCT) which are independent group
Ethical Consideration
The ethical clearance was obtained from the Institute Review Board of the University of Rwanda, College of Medicine and Health Sciences in Rwanda (No 157/CMHS IRB/2019); from Commission d’éthique de l’ Institut Supérieur du Lac á Goma (No 059/ISL/PCE/MB/2018). At the beginning of each data collection phase, informed consent was obtained from participants. The consent form had information about the study scope, design and timeline, confidentiality, study benefits and risks, and the right to refuse or withdraw from the research at any time. As interviews on domestic violence or Gender-Based Violence present a heightened risk for the survivors, especially when conducted in a household setting, the research team followed the WHO guidelines on intimate partner violence (WHO, 2013) and also trained the data collectors on safekeeping procedures.
Statistical Analyses
All analyses were performed using SPSS, version 28 and SPSS AMOS, version 28 (IBM Corp, 2021) statistical software packages.
Factorial Validity
The Kaiser Meyer-Olkin Measure of Sampling Adequacy and Bartlett’s Test of Sphericity were used to assess the suitability of the data for factor analysis. Exploratory factor analysis (EFA) was first performed unrotated, using maximum likelihood extraction and eigenvalues > 1. Additionally, we performed EFA with oblimin rotation and enforced a five-factor solution to test the theoretical structure of the DVQ. CFA was then performed using maximum likelihood estimation. To investigate the model’s goodness of fit, several statistics were used: Overall χ2, root mean square error of approximation (RMSEA), comparative fit index (CFI), Tucker Lewis index (TLI), and the standardized root mean square residual (SRMSR).
For the RMSEA, values close to .08 or smaller are recommended, whereas for the CFI, GFI, and TLI, values close to .95 or greater are recommended (Brown & Moore, 2012; Byrne, 2012). And if all factor loadings were statistically significant and salient (>.30), the factorial validity was supported (McKenzie et al., 2021). For chi-square statistic, a well-fitting factor solution should have a non-significant χ2 statistic, but because the test is sensitive to sample size, we considered χ2 adjusted for the degree of freedom (χ2/df) that should be at most five (Byrne, 2012; Kline, 2010). When the fit was poor, we used the LM (Lagrange Multiplier) test to detect improvements in model fit (Awang et al., 2015; Collier, 2020).
Two independent samples were obtained for the EFA and CFA, respectively. Only observations without missing items were used, resulting in 1,582 observations in total, 878 for the EFA and 704 for the CFA.
Internal Reliability
Internal consistency was assessed by calculating the Cronbach’s-α coefficient (Cronbach & Meehl, 1955) and Mean Inter-Item Correlation (MIIC). Internal consistency estimates of a magnitude of 0.70 or greater are considered satisfactory (Nunnally & Bernstein, 1994) while the recommended range of MIIC is 0.15 to 0.50 (Clark & Watson, 2016).
Concurrent Validity
Total scores and subscales of DVQ were tested on correlation with depression symptoms and mental well-being using the Pearson correlation coefficient.
Results
Sociodemographic Characteristics
Most of the participants in groups 1 and 2 were recruited from North Kivu (69.0%, resp. 75.1%). Regarding education, the rate of illiteracy in both group 1 (45.2%) and group 2 (50.1%) was high. Further, the sample in both group 1 (60.7%) and group 2 (58.8%) were dominated by women with 1 to 5 children (60.7% resp. 58.8%), followed by those with 6 to 10 children (33.0%, rep.33.3%). Polygamy was observed in both group 1 (14.1%) and group 2 (13.3%). The most reported types of relationships in group 2 were marriages and free unions (58.2%, resp. 41.8%), whereas these relationships were almost equally distributed among participants from group 1 (50.3%, resp. 49.7%) (Table 1).
Demographic Characteristics (n = 1,582).

Factor Analyses
The results indicated that the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was 0.920 and Bartlett’s test of sphericity was significant (χ2 = 9203.293, df = 190, Sig. < .001), indicating that the data were amenable to factor analysis.
Exploratory Factors Analyses
In the original analysis performed by the tool developers (Indu et al., 2011), 20 items clustered in five-five factors were retained. We performed a similar exploratory factor analysis with orthogonal rotations on our Group1 data set, which resulted in an uninterpretable four clusters of variables. For comparative purposes, we restricted items to load in five factors that resulted in five clusters of variables, explaining 66% of the variance, which could be approximately interpreted in the same way as the original factor model. Next, items factor loadings of at least .40 with “no cross-loading” were retained, resulting in a form with 18 items (Table 2). Items 7 and 12 were removed from the questionnaire due to their cross-loadings.
Five-Factor Model Exploratory Factor Analyses.

Note. The red color indicates the items removed.
To further explore the structure of the DVQ, we performed Principal Axis factoring with Oblimin rotation which resulted in three clusters of variables, which were easily interpretable: as physical violence (items 13, 14, 15, 16, 17, and 18), socio-economic restrictions (item 2, 3, 4, and 8) and insulting behaviors (item 5, 6, 7, 9, 10, 11, 12, 19, and 20), explaining 66% of the variance. The unfaithful behaviors from the original five-factor models did fully become part of the “insulting behavior factor in the 3-factor model.” Item 1 with cross-loading item 12 with poor loading were removed from the scale, thus the final form was composed of 18 items (Table 3).
Three Factor Model of DVQ.

Note. The asterisk indicates the items removed.
Confirmatory Factor Analyses
Confirmatory factor analysis was performed on the Group 2 data and we tested all three models identified in the EFA: three-factor (18 items), five-factor (18 items), and five-factor (20 items). As the items showed acceptable skewness and kurtosis, we used a maximum likelihood estimation model with standardized coefficients. Observations with missing values were excluded. After estimating the models, goodness-of-fit statistics were obtained for all models.
Our results showed that all standard indices suggested an acceptable fit of the original model (i.e., five factors, 20 items): χ2 (151) = 501.064, p = .000, χ2 adjusted for degrees of freedom (χ2/df) was 3.318, the Goodness of Fit Index (GFI) was .935, the root mean square error of approximation (RMSEA) was .057, the comparative fit index (CFI) was .950, and the Tucker–Lewis index (TLI) was .937. Some of the indices (GFI and TLI) were below the recommended thresholds, even though they were close, indicating that the model did not have a good fit. The factor loadings of this model ranged from 0.53 to 0.938 (except for items 19, 1, and 8 with 0.396, 0.448, and 0.48 respectively).
The new five-factor models (18 items) demonstrated a good fit for all standard indices (χ2 [114] = 324.903, p = .000, χ2/df = 2.850, GFI = .951, CFI = .965, RMSEA = .050, TLI = .953) and the three-factor model (χ2 [119] = 314.142, p = .000, χ2/df = 2.640, GFI = .947, CFI = .968, RMSEA = .048, TLI = .959).
However, the three-factor model with 18 items had the best fit compared to the other two models with factor loadings ranging from .53 to .946 (except item 19, item 18 and item 5 with 0.50, 0.50, and 0.521 respectively). The factor loadings for the new five-factor model (18 items) fluctuated from .57 to 91 (except item 19 with 0.43), Table 4.
Factor Loadings from Confirmatory Factor Analyses.
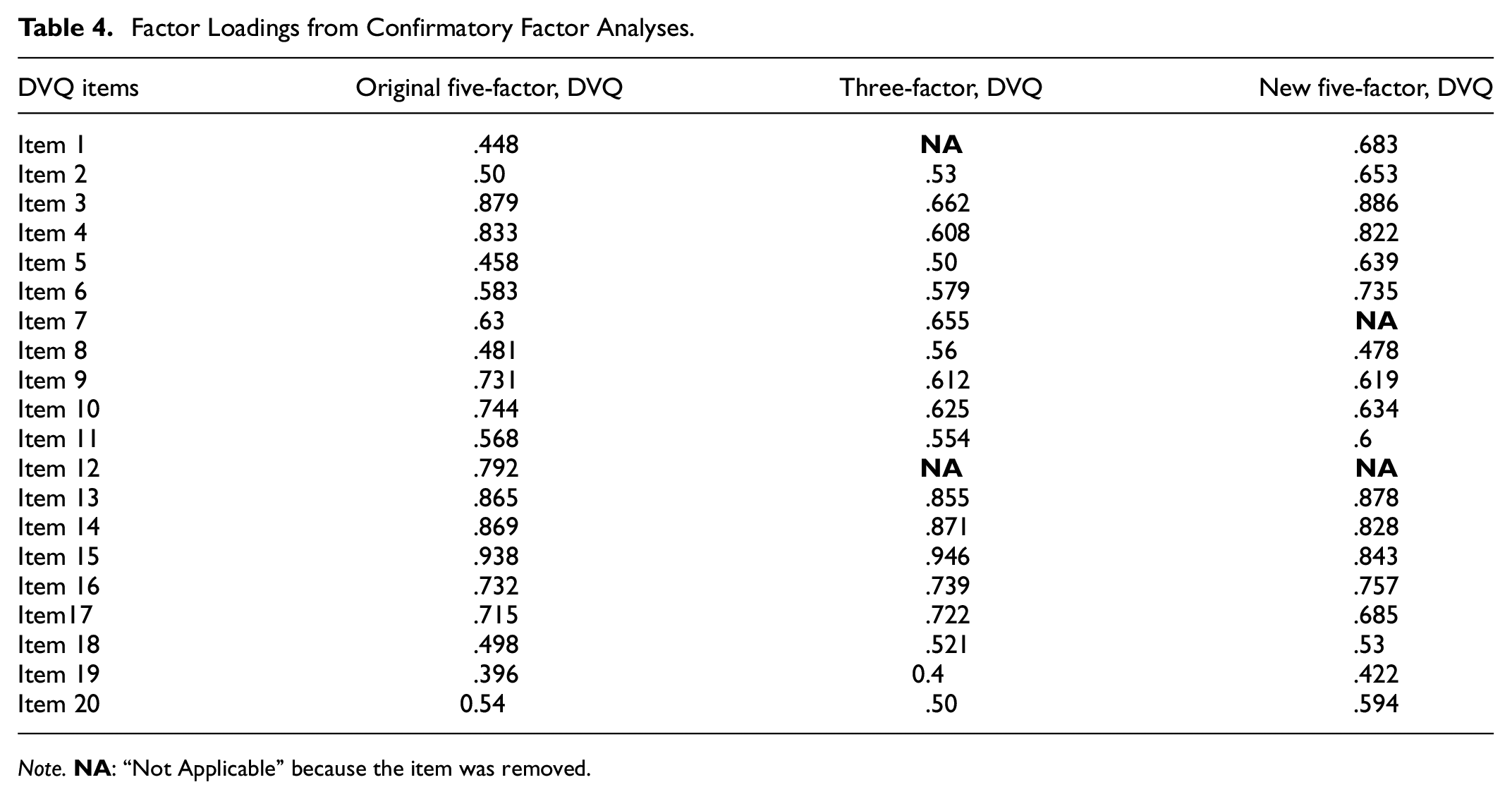
Note.
Reliability
Reliability was estimated using the Cronbach’s alpha and Mean inter-item correlation (MIIC) for the different factor models. As shown in Table 5, the original DVQ had Cronbach’s alpha of α = .908 and MIIC = .33 and subscales ranged from α = .65 to .926 and the MIIC range is .327 to .692. For the new 5-factor model (18-items), Cronbach’s alpha was α = .89 and MIIC = .32; while subscales ranged from α = .70 to .926 and MIIC range is .38 to .67. For the new 3-factor model (18-items), Cronbach’s alpha was α = .90 (MIIC = .32) and subscales range from α = .75 to .926 and the MIIC range is .34 to .67.
Internal Consistency of the DVQ Using Cronbach’s Alpha and MIIC Scores.

Note. n = number of items.
Items 7 and 12 were removed.
Items 1 and 12 were removed.
As shown in Table 6, the corrected item-total correlation (CITC) was above .4 for all items except item 1 and below .75 for all items following the recommended range for this measurement, indicating the good relationship of items within the construct.
Descriptive Statistics and Item-Total Correlation of 20-Item DVQ.
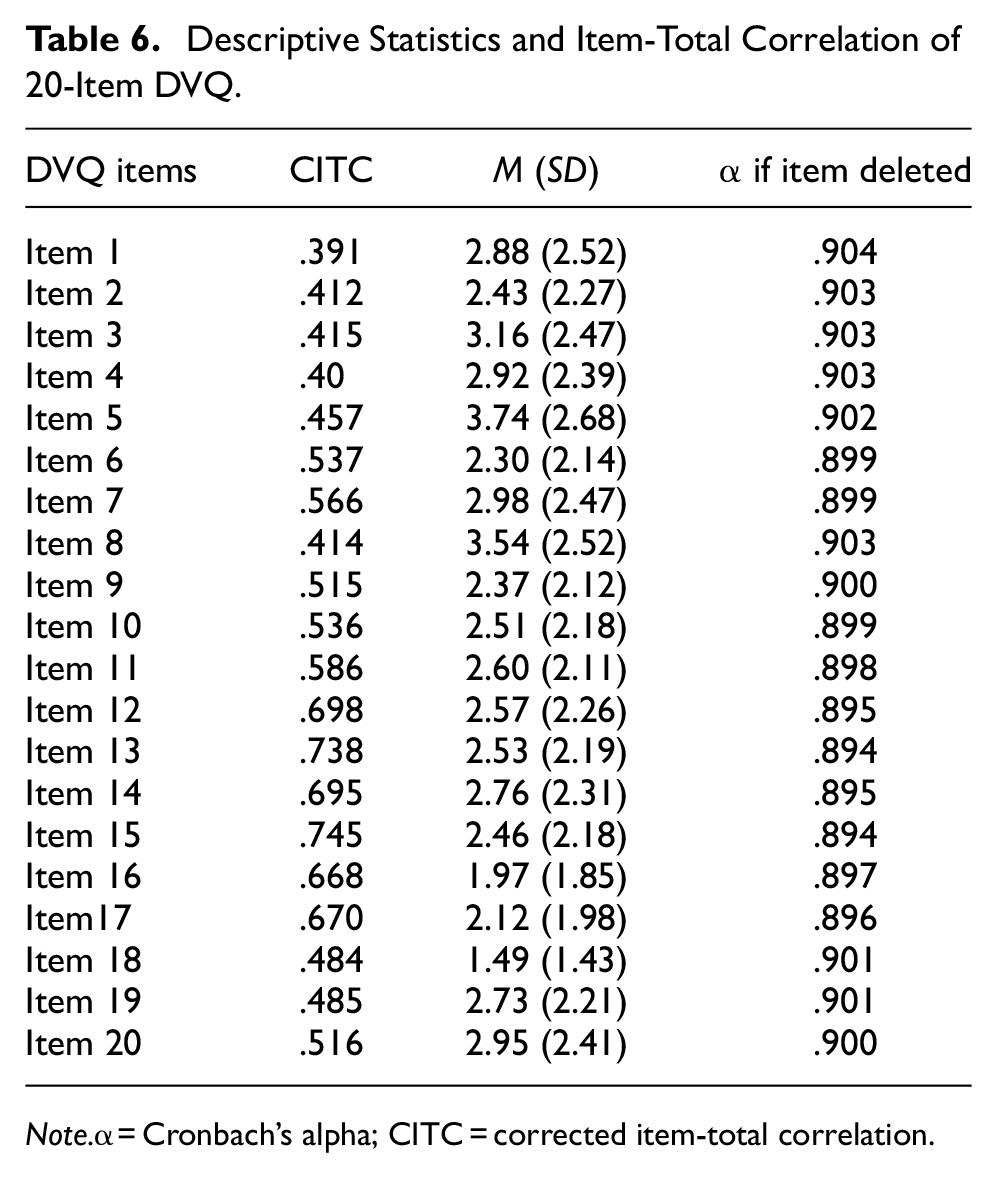
Note.α = Cronbach’s alpha; CITC = corrected item-total correlation.
Concurrent Validity
To assess the concurrent validity of the three DVQ models, we analyzed correlations between the scores in the subscales of the DVQ and depression symptoms, and mental wellbeing. The existence of statistically significant correlations was verified and confirmed between all measurements proposed in the direction expected, that is, negatively correlated with mental well-being, and positively with depression symptoms (Table 7).
Inter-Correlation Between Three Factor Model, Depression and Mental Wellbeing.

p < .001.
Discussion
To the best of our knowledge, this the first study to evaluate the psychometric properties of the Swahili version of the Domestic Violence questionnaire (DVQ) among female survivors of domestic violence in DRC. These women had partners (men) who were perceived by community members and local leaders as using violence at home against their wives and children. We tested the psychometric characteristics of the DVQ (Indu et al., 2011) in the DRC and present (i) psychometric evidence of the validity and reliability of the original 20-item DVQ in Swahili; (ii) an improved 5-factor 18-item version of the DVQ that resolves model fit issues of the original DVQ and allows for clear interpretation of the factors; and (iii) an improved 3-factor 18-item version of the DVQ that presents the best model fit and allows for clear interpretation of the factors.
We performed exploratory factor analysis to verify whether the factor structure from the original analysis would also emerge from our data. This was not the case as this analysis lead to an uninterpretable 4-factor model. We then forced the exploratory model in 5 factors (as in the original model), but also explored other factor models; including a 3-factor model. After analysis, it turned out that the 3-factor model was easily interpretable and produced the best model fit for our data set. The three-factor solutions accounted for 66% of the total variance of women’s exposure to domestic violence. As suggested by Pettet al. (2003), it is desirable to have factor solutions explaining at least 50% of the total variance; and thus, these three identified factors adequately explained the women’s experience of domestic violence. We then went ahead with a CFA on an independent data set, with data collected from the same target population. Using fit estimations based on maximum likelihood estimation, the CFA has verified the adequacy of the five-correlated factor model (χ2/df = 3.318, GFI = .935, RMSEA = .057, CFI = .950, TLI = .937) proposed by tool developers (Indu et al., 2011), the new five (χ2/df = 2.850, GFI = .951, CFI = .965, RMSEA = .050, TLI = .953) and the new three factor models (χ2/df = 2.640, GFI = .947, CFI = .968, RMSEA = .048, TLI = .959). Using Brown’s (2015) recommendations of values of RMSEA close or less to .08 and CFI close to .95 or greater and TLI close to .95 or greater, we see that the new five (18 items) and three-factor (18 items) models both have a good fit (with the three-factor model having the best fit). However, the original model (20 items) does not have a good fit; even though the values come close to the recommended levels.
Furthermore, our findings indicate that the factor structures differ from those of the DVQ hypothesized in development and validated among Indian women aged 18 to 55 years (Indu et al., 2011). For instance, the item 8 “Did not allow you to partake in decision-making,” loaded on a factor related to the financials or economy in Congolese context, but in the Indian context, it belonged to the factor related to neglect (Indu et al., 2011). This may also explain why the items linked to insulting behaviors and neglecting behaviors in the Indian study are loading in one and the same factor in the DRC study. Also, four items composed of the factor “controlling behavior” were emerged into distinct factors “unfaithful behaviors” (did not permit to meet/interact with female friends, restricted interaction with your family members) and “social interaction restriction” (Irritated/suspicious/angry if you talked to other men, accused you of being unfaithful) in this study. A number of reasons could explain the differences in the factor structure in the India and DRC study, including cultural differences, education level and stigma related to reporting violence (Jonas et al., 2022; Kelly et al., 2011; Murray et al., 2018).
Reliability analysis also showed DVQ presented excellent values for internal consistency. All the item-total correlation coefficients were above .2, which showed good discriminating ability (Chen et al., 2019). Moreover, The Cronbach’s α coefficient of the total scale was .91 and that values of each subscales were α = .70 to .93, which are similar and even, in some cases, superior to those obtained in the original study on the DVQ. Regarding concurrent validity, this study presents new results about the relationship between domestic violence as assessed by DVQ and different variables of interest. A direct positive relationship was validated between depression symptoms and DVQ scores, congruent with prior findings, thus providing support for the internal validity of the DVQ (Andersen et al., 2022; Calvete et al., 2007; Sharma et al., 2021). Second, mental wellbeing presented significant negative correlations with DVQ scores (Mootz et al., 2020). These results are congruent in sign and size with findings described in previous literature (Calvete et al., 2007; Mootz et al., 2020; Sharma et al., 2021), thus providing support for the external validity of DVQ.
Study Strengths and Limitations
The main strength of the study is the large sample size (i.e., 1,582 participants). The study also involved a highly relevant target group as the participants were women whose partners were perceived to be violent in their families by other community members. Finally, the study took place in a high conflict setting, where it is difficult to get data from, but where needs are high as we know that societal conflict also increases domestic violence. The main limitation of this study is the lack of test-retest reliability.
It will be necessary to perform additional psychometric validation studies of the 18-item DVQ in different contexts and with different target populations to further evidence the reliability and validity of the tool; and include comparative concurrent validation with other well validated domestic violence tools.
Conclusion
The results showed that the original factor structure of the DVQ didn’t fit with our data set. However, when analyzing the data, a 3-factor model emerged that was clearly interpretable and delivered excellent psychometric properties. It can be concluded that the 18-item Swahili version of the domestic violence questionnaire is valid and reliable for evaluating physical and sexual violence, but also more invisible forms of violence as psychological and economical violence among women exposed to intimate partner violence in DRC. It thus gives information regarding the presence and nature of violence in couple relationships of Congolese women from a large sample, allowing its comparison with findings produced in India and elsewhere. Therefore, we promote the use of the DVQ as a reliable and valid tool to measure domestic violence in DRC. We also promote the use of the DVQ in different settings, but suggest performing psychometric analysis in such cases, as our study has demonstrated that the factor structure can be different in different contexts.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241255440 – Supplemental material for Psychometric Validation of the Domestic Violence Questionnaire in Swahili Among Congolese Female Survivors of Domestic Violence
Supplemental material, sj-docx-1-sgo-10.1177_21582440241255440 for Psychometric Validation of the Domestic Violence Questionnaire in Swahili Among Congolese Female Survivors of Domestic Violence by Stefan Jansen, Japhet Niyonsenga, Epaphrodite Nsabimana, Mihigo Bonaventure, Eugene Rutembesa, Henny Slegh and Jean Mutabaruka in SAGE Open
Footnotes
Acknowledgements
The authors would like to thank all the participants who voluntarily agreed to participate in this study. Their patience and willingness to contribute to the study is greatly appreciated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is funded by a registered charity in England and Wales that finds solutions to complex humanitarian problems through research and innovation (ELRHA) which means Enhancing Learning and Research for Humanitarian Assistance (Reference number: #32443).
Ethical Consideration
The ethical clearance was obtained from the Institute Review Board of the University of Rwanda, College of Medicine and Health Sciences in Rwanda (No. 157/CMHS IRB/2019); from Commission d’éthique de l’ Institut Supérieur du Lac à Goma (No. 059/ISL/PCE/MB/2018).
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.