
Abstract
Nicaragua has one of the highest adolescent fertility rates in Latin America and in the Caribbean. However, studies on adolescent pregnancies are limited. This study investigates the mechanism of early fertility among women aged 15 to 24 in northern central and eastern regions (NC-E) and the Pacific region (PAC), using data from the Nicaraguan Demographic and Health Survey 2011/12 (N = 2,600). Structural equation modeling analysis was conducted in NC-E and PAC to examine the associations between exogenous variables (ethnicity and residence), mediators (education, sexuality education, knowledge and attitudes on pregnancy prevention, and sexual behaviors), and outcome (early fertility). The results showed educational attainment and sexual behaviors were crucial mediators of early fertility in NC-E and PAC, whereas sexuality education was only in NC-E. Residence was an exogenous variable in both groups, whereas ethnicity was not. Although educational attainment and sexuality education would improve knowledge, they did not contribute to reducing risky sexual behaviors. Further discussions on ethnic differences and variables measuring the actual decision-making related to risky sexual behaviors are suggested.
Plain Language Summary
Nicaragua has one of the highest adolescent fertility rates in Latin America and in the Caribbean. However, studies on adolescent pregnancies are limited. This study investigates the mechanism of early fertility among women aged 15–24 in northern central and eastern regions (NC-E) and the Pacific region (PAC) (N=2,600), using data from the he Nicaraguan Demographic and Health Survey (Encuesta Nicaragüense de Demografía y Salud), conducted by the National Institute of Development Information (el Instituto Nacional de Información de Desarrollo) and Ministry of Health in Nicaragua (el Ministerio de Salud) in 2011 and 2012. Structural equation modeling analysis was conducted in NC-E and PAC to examine the associations between exogenous variables (ethnicity and residence), mediators (education, sexuality education, knowledge and attitudes on pregnancy prevention, and sexual behaviors), and outcome (early fertility). The results showed educational attainment and sexual behaviors were crucial mediators of early fertility in NC-E and PAC, whereas sexuality education was only in NC-E. Residence was an exogenous variable in both groups, whereas ethnicity was not. Although educational attainment and sexuality education would improve knowledge, they did not contribute to reducing risky sexual behaviors. This study provides new insights into adolescent pregnancy and childbearing mechanisms in Nicaragua by introducing the concept of mediating factors. The study also added new information on early pregnancy among young women in NC-E where adolescent sexual reproductive health has rarely been studied. Further discussions on ethnic differences and variables measuring the actual decision-making related to risky sexual behaviors are suggested.
Keywords
Introduction
Nicaragua has one of the poorest adolescent sexual and reproductive health (ASRH) indicators in Latin America and the Caribbean (LAC). Among ASRH indicators, the country has one of the highest adolescent fertility rates in LAC (World Bank, 2022) despite its high contraceptive use among adolescents (United Nations Population Fund, 2015). Furthermore, the decline in adolescent fertility rates has been slower than that in the total fertility rate, which has resulted in increased adolescent childbearing (United Nations Population Fund, 2015). Poor ASRH has a long-term adverse impact on an individual’s quality of life. Adolescent girls are particularly susceptible to unwanted and premature pregnancies, sexually transmitted diseases, and unsafe abortions due to their vulnerability to sexual abuse and violence. These factors severely impede women’s educational, economic, and social opportunities (United Nations, 1995). Additionally, adolescent girls are more likely to die from pregnancy-related health complications than older women.
Several studies in Nicaragua have focused on adolescent pregnancies and childbearing. Studies from the Nicaraguan Demographic and Health Surveys (Pérez et al., 2021; Samandari & Speizer, 2010) showed that adolescent pregnancies and live births decreased from 1987 to 2009 but increased thereafter up to 2013. Additionally, adolescent pregnancy was associated with living in low socioeconomic households, especially those with low education. A study focusing on the influence of community social capital on early sexual onset and childbearing (Mendez-Rojas et al., 2016) showed that teen childbearing was associated with a community with a high proportion of females having a child but negatively associated with higher education in the community. A door-to-door survey among adolescents living in poor neighborhoods of Managua, the capital of Nicaragua, showed that consistent condom use was associated with feeling comfortable in talking about sexuality with their partner (Decat et al., 2015). Semi-structured interviews on sexual awareness and decision-making in the community outskirts of León, the second largest city in Nicaragua, highlighted that social stigma hinders adolescents’ access to reproductive health services, social media influences adolescents’ sexual awareness, and sexual education represents a reliable source of information about sex (Larsson et al., 2022). These studies indicated that socioeconomic status, such as educational attainment, partner relationships and social norms on female sexuality in communities, could influence adolescent pregnancy or childbirth. Furthermore, social media and sexuality education can reduce early pregnancy and childbearing. However, these studies mainly focused on the influence of socioeconomic factors and not on the knowledge, attitudes, and behaviors to reduce adolescent pregnancy or childbearing. According to health behavior change models and theories, Social Learning Theory proposes that interactions among social demographic characteristics and cognitive factors, such as knowledge and attitudes, influence human learning and behavior (Bandura, 1971). The theory of Planned Behavior suggests that a person’s behavior is determined by their intention to perform the behavior (Ajzen, 1991). Thus, this study aims to assess the associations between knowledge, attitudes, behaviors, sociodemographic factors, and early pregnancy or childbearing.
In addition, studies in the Atlantic region of Nicaragua are scarce. Adolescent pregnancy and childbearing in Nicaragua have been researched primarily in the capital, the Pacific region, or in the country overall, but not in the Atlantic region, or northern central and eastern Nicaragua. This region has a culture, language, ethnicity, politics, and history distinct from the Pacific region (Sollis, 1989). For example, it is inhabited by indigenous people, such as the Miskitu, Mayangna, and Rama, and Afro-descendants such as Kriol and Garífuna (International Work Group for Indigenous Affairs, 2022). Most indigenous people live in the Autonomous Regions of the Northern Caribbean Coast (RACCN), Autonomous Regions of the Southern Caribbean Coast (RACCS), Department of Río San Juan, and northeastern part of the Department of Jinotega; whereas most Afro-descendants live in RACCS (Renshaw, 2007). Owing to its geographical remoteness, the Atlantic region has often been neglected in academic studies. The international community has gradually increased interest in and recognition of indigenous peoples and ethnic diversity since the early 1980s. As a result, the Atlantic region has received renewed attention from the public and academic world (Sollis, 1989). However, studies in the Atlantic region, or northern central and eastern Nicaragua, are still lacking, especially in the research focused on adolescent pregnancy and childbearing.
Structural Equation Modeling
Regression models are predominantly used to examine the association between social determinants and health knowledge, behavior, and outcomes. Some studies suggest that certain variables indirectly affect health outcomes. However, these indirect and mediating associations cannot be adequately represented or explained using normal regression models (Vasconcelos et al., 1998). According to Bronfenbrenner’s ecological systems theory, multiple environmental levels affect individuals, which can in turn affect health knowledge and behaviors (Bronfenbrenner, 1979). Hence, structural equation modeling (SEM), an extension of multivariate regression analysis, is more appropriate for a multi-layered social system. In multivariate regression, a variable is either a predictor (an independent variable) or an outcome (a dependent variable). In SEM analysis, a variable can be an outcome of some variables and a predictor of others (Pedhazur & Kerlinger, 1982). Some studies have applied SEM analysis to examine the associations between social determinants and health knowledge, behaviors, and outcomes (Choi & Lee, 2022; Kiani et al., 2020; Shimamoto & Gipson, 2017; Wardani et al., 2014).
Purposes
This study investigates the mechanism linking sociodemographic status, knowledge, attitudes, and behaviors in the prevention of early fertility among young women in northern central and eastern Nicaragua using SEM analysis. In particular, this study first examines the direct associations between residence (urban or rural), ethnicity, education level, sexuality education, knowledge and attitudes on the prevention of adolescent pregnancy or childbearing, sexual behaviors, and early fertility. Second, the mediation associations of education, sexuality education, knowledge, attitudes, and sexual behaviors were assessed as potential mediating constructs for early fertility. Young women from the Pacific region were included in the comparison.
Methods
Data Source
This study used cross-sectional data from the Nicaraguan Demographic and Health Survey (Encuesta Nicaragüense de Demografía y Salud [ENDESA 2011/12]), conducted by the National Institute of Development Information (el Instituto Nacional de Información de Desarrollo [INIDE]) and Ministry of Health in Nicaragua (el Ministerio de Salud) in 2011 and 2012. ENDESA 2011/12 applied multistage stratified random sampling to generate nationally representative data on household living and economic conditions, general health, and sexual and reproductive health such as family planning, maternal and child health, gender issues, and HIV/AIDS. ENDESA 2011/12 includes four surveys: an individual survey of women aged 15 to 49 years, an individual survey of men aged 15 to 59 years, a household survey, and a couples’ survey. Prior to conducting the survey the questionnaires were field-tested in four municipalities with different socioeconomic and geographic locations to assess their validity and reliability (Instituto Nacional de Información de Desarrollo & Ministerio de Salud, 2013). The dataset was obtained from INIDE (https://www.inide.gob.ni/Home/endesa). An individual survey of women aged 15 to 49 years was conducted in this study.
Samples
For the individual survey of women aged 15 to 49 years, a two-stage stratified cluster sample design was applied, where the first step of sampling involved the selection of clusters and the second involved the selection of households. A representative sample of 15,266 women was selected using a stratified sample design. Data of women aged 15 to 24 years from eight selected departments of Nicaragua were extracted from the sample data. Of the eight departments, four—the Autonomous Regions of the Northern Caribbean Coast (RACCN), Autonomous Regions of the Southern Caribbean Coast (RACCS), Jinotega, and Río San Juan—were selected and categorized as departments in northern central and eastern Nicaragua (NC-E). These departments had the four lowest departmental wealth indices according to the household survey on living and economic conditions in ENDESA 2011/12 (Instituto Nacional de Información de Desarrollo & Ministerio de Salud, 2013). The other four departments were Carazo, Granada, Managua, and Masaya, which were categorized as the Pacific region departments (PAC), as they are located in the Pacific region, where relatively fewer indigenous people reside. PAC had the four highest departmental wealth indices in ENDESA 2011/12. The selected departments are illustrated in Figure 1. A total of 2,600 women were included in this study, representing 17.0% of the total sample of women aged 15 to 49 years in Nicaragua.
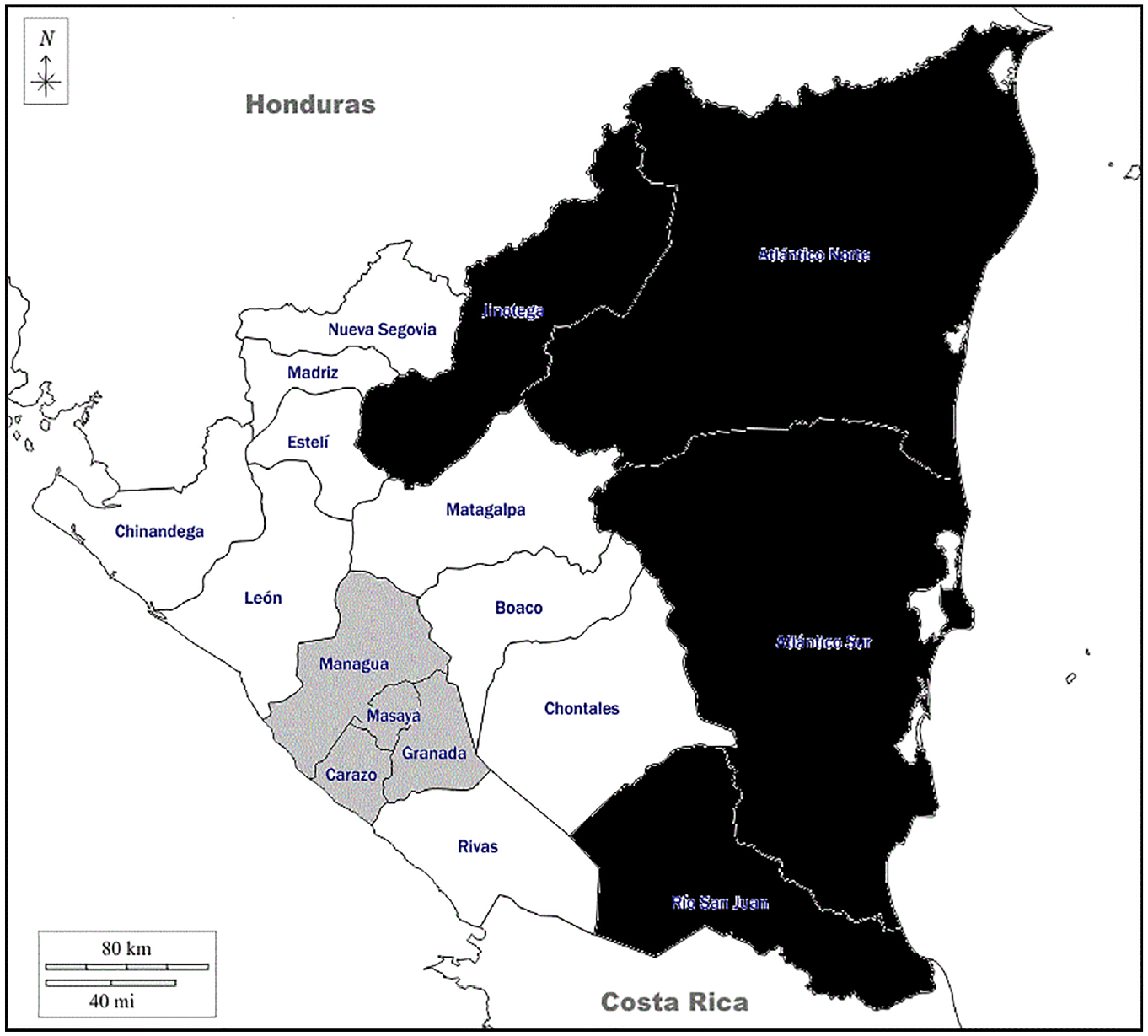
Map of Nicaragua with departments.
Model Development
A hypothetical model was established for conducting structural equation modeling (SEM) analysis based on existing health behavior change models and theories, such as Social Learning Theory and Theory of Planned Behavior (Figure 2). “Ethnicity” and “residence” were treated as the exogenous variables. In structural equation modeling (SEM), the term “exogenous variable” is used instead of “independent variable.” The exogenous variable is “a variable that has paths coming from it and none leading to it” (Pedhazur & Kerlinger, 1982, p. 158). “Highest education level” and “sexuality education” were treated as the first-level endogenous variables or mediators. Instead of dependent variables, the SEM analysis uses the term endogenous variables, defined as “a variable that has at least one path leading to it” (Pedhazur & Kerlinger, 1982, p. 158). “Sexual and reproductive health (SRH) knowledge,”“SRH attitudes,” and “risky sexual behavior” were treated as second-level endogenous variables or mediators. These three variables were hypothesized to have the following associations: 1. “SRH knowledge” has direct associations with “SRH attitudes” and “sexual behaviors”; 2. “SRH attitudes” has a direct association with “sexual behaviors”; and 3. “SRH knowledge,”“SRH attitudes,” and “sexual behaviors,” have a direct association with the outcome. “Early fertility” was treated as an outcome.
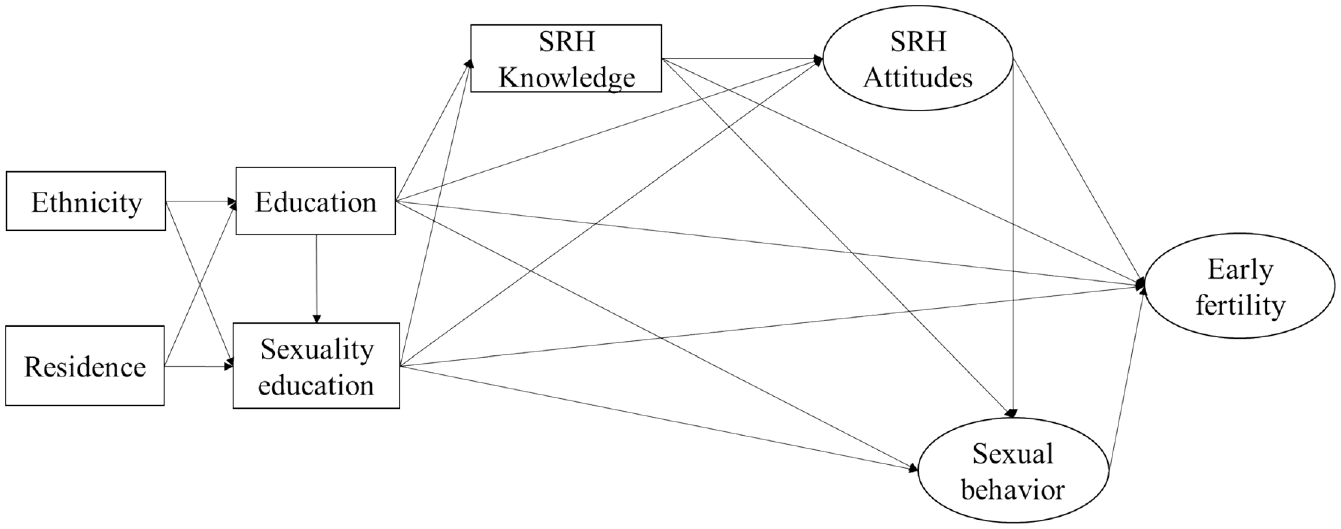
Path diagram of hypothesized model.
Measures
The variables for the SEM analysis in this study included both measured and latent variables. A latent variable is a hypothetical construct that consists of multiple measured variables. This study employed three latent variables: “SRH attitudes,”“sexual behavior,” and “early fertility.”“SRH attitudes” and “sexual behavior” consisted of three measured variables, and “early fertility” consisted of two measured variables. The other variables were the measured variables.
Regarding coding, this study employed a reverse coding system, where an indicator was coded with a higher value if the content or phenomenon referred to by the indicator was undesirable. For example, “highest education level” was categorized into five levels where 5 = no education and 1 = higher (over secondary) education, as a lower education level was considered undesirable.
Exogenous Variables
“Ethnicity” was coded as 1 = non-indigenous (for Latinos, people of mixed Spanish and indigenous descent, and others), 2 = Afro-descendants, and 3 = indigenous (indigenous people in the Atlantic, such as Miskitu and Mayangna, and Pacific region—such as Nahoa and Chorotega). “Residence” was dichotomized and coded as 0 = urban and 1 = rural.
First-Level Mediators
“Highest education level” and “sexuality education” were treated as the first-level mediators. Five-level coding was used for “highest education level”: 1 = higher education (over secondary), 2 = secondary education, 3 = primary education (grades 4–6), 4 = primary education (grades 1–3), and 5 = no education. “Sexuality education” was coded as follows: 1 = had sexuality education both in and out of school, 2 = had sexuality education in school only, and 3 = never had sexuality education. The topics of sexuality education in Nicaragua covered human body development, male and female reproductive organs, menstruation, pregnancy and childbirth, contraceptive methods, STI, and AIDS (Instituto Nacional de Información de Desarrollo & Ministerio de Salud, 2013).
Second-Level Mediators
“Sexual and reproductive health (SRH) knowledge,”“SRH attitudes,” and “risky sexual behavior” were treated as the second-level mediators, where “SRH attitudes” and “risky sexual behavior” were examined as latent constructs with three measured variables. “SRH knowledge” consisted of knowledge on pregnancy prevention and risky sexual behaviors. Pregnancy prevention had two questions on pregnancy: (a) a woman can get pregnant the first time she has sex and (b) a woman is most likely to become pregnant following her menstrual cycle. Risky sexual behavior assessed knowledge of three forms of prevention to reduce the risk of HIV/AIDS: abstinence, having only one partner, and using a condom every time one has sex. These three forms are also considered to prevent adolescent pregnancy and early childbearing (Kalmuss et al., 2003). The scoring was “0” for a correct answer and “1” for an incorrect answer. The total score of all the questions was used as a variable (the total score ranged from 0 to 5).
“SRH attitudes” consisted of three measured variables related to women’s SRH empowerment—attitudes toward male’s decision-making power, attitudes toward violence, and attitudes toward sex negotiation. Attitudes toward male’s decision-making power were assessed using the following four questions: (a) a good wife obeys her husband even if she disagrees with him, (b) family problems should only be discussed within the family, (c) the man has to show his wife/partner that he is in charge, and (d) other people should intervene if the man mistreats his wife/partner. The scoring was “0” if the response was no and “1” if the response was yes or do not know. The total score of the four questions was used as a variable (the total score ranged from 0 to 4). Attitudes toward violence used a question concerning a woman’s acceptance of physical abuse by her husband or partner in the following four situations: (a) if she does not do housework, (b) if she disobeys him, (c) if she asks him if he is unfaithful to her, and (d) if she refuses to have sex with him. The scoring was “0” if the response was no and “1” if the response was yes or do not know. The total score of the four situations was used as a variable (the total score ranged from 0 to 4). Attitudes toward sex negotiation assessed a woman’s perceived ability to negotiate sexual relations using the following two questions: (a) it is a woman’s obligation to have sexual relations with her husband or partner even if she does not want to, and (b) the man decides whether to use a condom even if the woman wants to use it. The scoring was “0” if the response was no and “1” if the response was yes or do not know. The total score of two questions was used as a variable (the total score ranged from 0 to 2).
“Sexual behavior” consisted of age at first sexual intercourse, number of sexual partners, and contraceptive use. These three indicators are factors that prevent adolescent pregnancy and early childbearing, as described in the paragraph on the latent variable of SRH knowledge (Kalmuss et al., 2003). Age of first sexual intercourse was coded as “1 = 10 to 14 years old,”“2 = 15 to 19 years old,”“3 = 20 to 24 years old,” and “4 = never had sexual intercourse.”Number of sexual partners was coded as “1 = never had sexual intercourse,”“2 = 1 partner,”“3 = 2 to 5 partners,”“4 = 6 to 10 partners,” and “5 = 11 partners or more.”Contraceptive use was coded as “1 = never had sexual intercourse,”“2 = used any method of contraception,” and “3 = never used contraceptive methods.”
Outcome Variable
“Early fertility” was examined as a latent variable, which included two measured variables: age at primigravida and age at first parturition. Four-level coding was used as follows: 1 = never been pregnant or had a child, 2 = 20 to 24 years old, 3 = 15 to 19 years old, and 4 = 10 to 14 years old.
Data Analysis
Descriptive statistics are presented according to the two department groups: NC-E and PAC. To compare the two groups, the Mann–Whitney U-test was conducted for continuous variables and Pearson’s chi-square test for categorical variables. SEM analysis was performed to investigate the associations among a set of variables of a hypothetical model (Figure 2) in both NC-E and PAC. As the first step of the SEM analysis, the magnitude and significance of the factor loading between each indicator and the latent variable were assessed in the measurement model. Loading is considered absolutely important in forming the latent variable when it is ≥.50, and statistically significant (Hair et al., 2020). Goodness of fit was then tested using measurement and structural models. The goodness of fit of the measurement model evaluated the goodness of the observed variables to represent their latent variables, whereas the goodness of fit of the structural model evaluated the goodness of the relationship between latent variables. The following fit indices were used to determine the overall fit of the model: comparative fit index (CFI) and Tucker-Lewis index (TLI) as incremental fit indices, and root mean square error of approximation (RMSEA) and standardized root mean square residual (SRMR) as absolute fit indices (Kline, 2016). An incremental fit index or relative fit index, assesses the ratio of the deviation of the user model from the baseline model to the deviation of the best-fitting model from the baseline model. On the other hand, an absolute fit index does not compare the user model with a baseline model but instead compares it to the observed data. The model is considered a good fit with values in the ranges of CFI >0.90, TLI >0.90, RMSEA <0.08, and SRMR <0.08 (Kamel & Broc, 2019). Measurement invariance was also tested to determine whether the latent constructs were consistently measured across NC-E and PAC. Measurement invariance was also tested if the latent constructs are measured consistently across NC-E and PAC. In the last step of the SEM analysis, the path coefficients of both the direct and indirect associations among a set of variables of a hypothetical model (Figure 2) were computed, and the significance of each association was tested.
Although there is no established sample size requirement for SEM analysis, there are widely accepted rules-of-thumb on sample size estimation method, “10-times rule” method, which builds on the assumption that the sample size should be greater than 10 times than the estimated parameter in order to avoid statistical errors (Kline, 2016). Simultaneously, the sample size should not be too much larger than the minimum sample size requirement (Kline, 2016). The estimated parameter of the hypothesized model for this study was 114, which means that the sample size should be 1,140 or larger. The sample size per group was 1,356 for NC-E and 1,244 for PAC; thus, the study fulfilled the sample size requirements. Additionally, the sample size of this study was not too large than minimum sample size requirement.
The present study used SPSS Statistics 27 (IBM Corp., Armonk, NY, USA) to perform descriptive statistics and R 4.1.1 (The R Foundation for Statistical Computing, Vienna, Austria) with the lavaan package (version 0.6-10) for SEM analysis. The significance threshold was set at p < .05.
Ethics
The relevant authorities approved the study design, and no participant consent was required as this analysis used publicly available data from national surveys with anonymized databases. Therefore, ethical issues were addressed by the institutions conducting the surveys.
Results
Descriptive Statistics
Table 1 shows the demographic and outcome variables for all samples used in this study (N = 8,810). Of the 2,600 women aged 15 to 24 years old (mean = 19.41, SD = 2.80), 1,356 (52.2%) were from departments in northern central and eastern Nicaragua (NC-E) and 1,244 (47.8%) were from departments in the Pacific region (PAC).
Descriptive Characteristics of the Participants.

Comparisons between NC-E and PAC showed statistically significant differences in all variables except for knowledge of risky sexual behavior (p = .673). The statistics showed that: (a) 70.6% of women in NC-E lived in rural areas, whereas 26.1% lived in PAC; (b) nearly 20% of women in NC-E were indigenous, whereas almost all women (94.1%) in PAC were non-indigenous; and (c) over 40% of women in NC-E never had sexuality education compared with 16.4% women in PAC. Both groups showed high outcomes in primigravida and first parturition during adolescence, although women in NC-E showed higher rates (primigravida: 49.1% [= 10.3% + 38.8%] in NC-E and 37.4% [= 4.1% + 33.3%] in PAC; first parturition: 41.0% [= 5.0% + 36.0%] in NC-E and 31.2% [= 1.9% + 29.3%] in PAC).
SEM Analysis
The goodness-of-fit test for the measurement model showed RMSEA = 0.078, SRMR = 0.031, CFI = 0.954, TLI = 0.922. For the structural model, RMSEA = 0.076, SRMR = 0.037, CFI = 0.950, TLI = 0.926. All goodness-of-fit values for both the measurement and structural models were within the acceptable range of fit. The test of measurement invariance showed partial invariance across groups, indicating that the factorial invariance between NC-E and PAC was relatively weak. Due to the relatively weak invariance, this study described the SEM results of each group separately, instead of conducting a statistical test to compare the hypothesized model across the two groups.
Direct Associations
Figure 3a and b show the path coefficients and p-values for each path in the NC-E and PAC. In the measurement models, all factor loadings between each indicator and latent variable were ≥.50 and statistically significant. The results of the significance tests within the structural model show that 15 out of 19 paths in NC-E had significant direct associations. “Residence,”“highest education level,”“sexual and reproductive health (SRH) knowledge,” and “sexual behavior” had significant direct associations with all variables that they shared direct paths with. “Sexuality education” had significant associations, except with “SRH attitudes.”“SRH attitudes” were not significantly associated with any variable except “highest education level” and “SRH knowledge.” The paths from “SRH knowledge” to “sexual behavior” and the outcome had negative path coefficients. The PAC results showed that 11 of 19 paths had significant direct associations. As in NC-E, “residence,”“highest education level,” and “sexual behavior” had significant direct associations with all variables that had direct paths with them. However, “SRH knowledge” did not. Furthermore, “SRH attitudes” had no significant associations with any variable except “highest education level.”
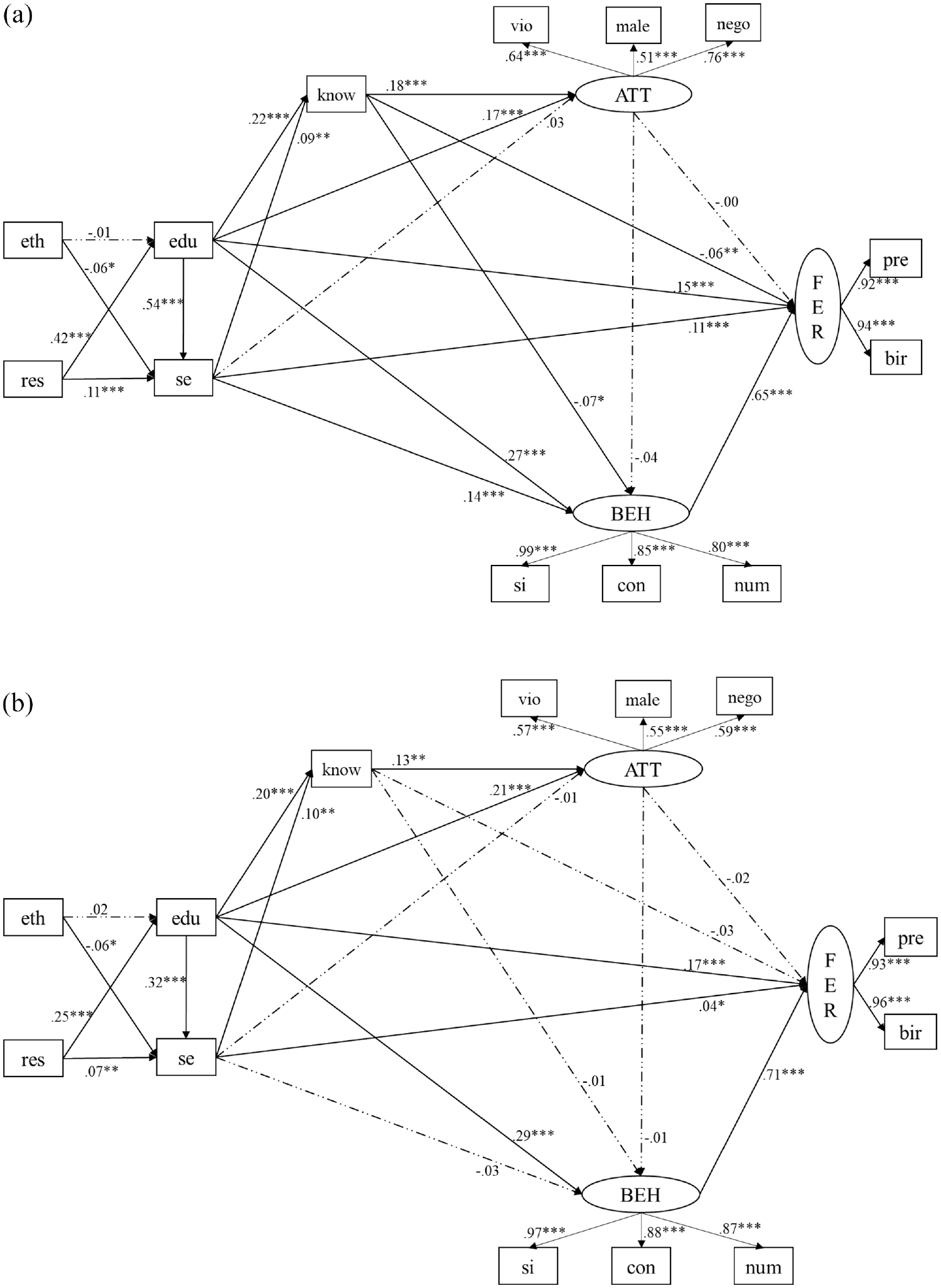
Direct associations between the variables. (a) Departments in northcentral and eastern Nicaragua (NC-E), (b) Departments in the Pacific region (PAC).
Mediating Associations
Table 2a and b list the significant mediating paths between the exogenous variables (residence and ethnicity) and outcome. Of the 46 mediating paths, nine and two paths had significant paths in NC-E and PAC, respectively. In NC-E, all the mediating paths between “residence” and the outcome mediated “highest education level,”“sexuality education,” and/or “sexual behavior.” The mediating paths between “ethnicity” and the outcome mediated “sexuality education” and/or “sexual behavior,” but not “highest education level” (Table 2a). Three mediating paths in NC-E had negative coefficients (Table 2a): “res->edu->know->BEH->FER,”“eth->se->BEH->FER,” and “eth->se->FER.” Of them, the path “res->edu->know->BEH->FER” is a competitive mediation, where the indirect and direct effects point in opposite directions (one is positive while the other is negative) (Hair et al., 2021). More precisely, “know” was a competitive mediator, as the coefficient of the path “edu->BEH” is positive (β = .27), while the indirect effect “edu->know->BEH” showed negative coefficients (β = .22 × (−.07)) (see Figure 3a). In PAC, the mediating paths between “residence” and the outcome mediated “highest education level” and/or “sexual behavior,” but not “sexuality education” (Table 2b). Additionally, “ethnicity” was not an exogenous variable. “SRH attitudes” was not a mediator in both groups. This variable was not significantly associated with a second-level mediator (“sexual behavior”) or the outcome (“early fertility”), so no significant mediating paths were formed between exogenous variables and the outcome via “SRH attitudes” (see Figure 3).
List of Significant Mediating Paths.

Note. Res = residence; edu = highest education level; se = sexuality education; know = SRH knowledge; BEH = sexual behavior; FER = early fertility.
Discussion
This study was designed to investigate the mechanism linking sociodemographic status, knowledge, and attitudes toward sexual and reproductive health (SRH), sexual behavior, and early pregnancy among young women in northern central and eastern Nicaragua (NC-E) and in the Pacific region in Nicaragua (PAC). SEM analysis was conducted to assess both the direct and mediating associations of education, sexuality education, SRH knowledge and behavior as potential mediating constructs for early fertility.
Four key findings were obtained from the SEM analysis. First, the results showed that “highest education level” and “sexual behavior” acted as mediators between an exogenous variable (“residence”) and an outcome (“early fertility”) in both groups. This indicates that educational attainment and risky sexual behavior play a crucial role in early fertility among women in both groups. Women living in rural areas have lower educational attainment, indicating risky sexual behaviors, and leading to a higher chance of early pregnancy and childbearing. These results are supported by previous studies that examined the factors associated with SRH outcomes (Greenway et al., 2012; Lam et al., 2013; LeVine et al., 2004). This study further illustrated that educational attainment and risky sexual behaviors function as mediators between sociodemographic factors and early fertility.
Second, “sexuality education” acted as a mediator between an exogenous variable (“residence”) and an outcome (“early fertility”) among women in NC-E, in addition to “highest education level” and “sexual behavior.” The results indicate that women with low educational attainment tend not to have sexuality education, which is associated with increased risky sexual behaviors. According to the descriptive results, 42% of women in NC-E never had sexuality education, much higher than the women in PAC (16.4%). Previous studies have shown that sexuality education positively impacts risky sexual behavior (Kirby, 2011) and reduces instances of teenage pregnancy (Paton et al., 2020). These results suggest that sexuality education plays an important role in reducing adolescent pregnancy and childbearing in NC-E departments. Unlike the women in NC-E, sexuality education did not act as a mediator in the PAC. Although 75% of women in PAC have had sexuality education, this was not related to a reduction in early pregnancy and childbearing. Adolescents learn about sexuality within the school system but are influenced by their peers and the media (Pathfinder International et al., 2007). PAC departments are more densely populated and urbanized than NC-E departments. Adolescents can be exposed to more media sources and peer pressures that affect sexual behaviors more than sexuality education.
According to ENDESA 2011/2012, topics of sexuality education in Nicaragua cover human body development, male and female reproductive organs, menstruation, pregnancy and childbirth, contraceptive methods, STI, and AIDS. Although the topics cover biomechanical contents, they lack topics related to personal relationships and skills. Topics on personal relationships and skills can help young women learn about communication, negotiation, and decision-making regarding sexual relationships and sexual health. This may relate to the results that although “SRH knowledge” was associated with “SRH attitudes,”“SRH attitudes” was not associated with “sexual behaviors,” where “SRH attitudes” consisted the elements related to negotiation skills to reduce risky sexual behaviors. Given these results and discussions, the inclusion of personal relationships and skills in the sexuality education program is suggested to strengthen the sexuality education program, especially in the NC-E.
Third, residence—whether the woman lived in an urban or rural area—was associated with all mediating paths in both groups, acting as an exogenous variable, while ethnicity did not. As shown in the descriptive statistics, 70% of women in PAC lived in rural areas. Access to communities in rural areas is challenging in northern central and eastern Nicaragua because of dense tropical forests, long-lasting rainy seasons, scattered villages, and poor road infrastructure (Sollis, 1989). Indigenous people and Afro-descendants of Nicaragua live in urban and rural areas. This indicates that geographical remoteness affects educational attainment more than ethnicity in Nicaragua. Further investigation of differences related to ethnicity is recommended, as indigenous people and Afro-descendants of Nicaragua have distinct origins, histories, and characteristics. For example, Miskitu and Mayangna live in the northern Atlantic region and have retained their indigenous languages. By contrast, Rama in the southern Atlantic region speak Spanish and English. Although both Miskitu and Mayangna live in the northern Atlantic region, Miskitu live in the coastal region while Mayangna live inland. Furthermore, Mayangna are believed to have originated from the Pacific region (International Work Group for Indigenous Affairs, 2022; Renshaw, 2007).
Fourth, the mediation analysis showed that “SRH knowledge” acted as a competitive mediator in NC-E. In competitive mediation, the indirect and direct effects point in opposite directions (one is positive while the other is negative). This study showed that the path coefficient “edu->BEH” was positive (β = .27), while the indirect effect “edu->know->BEH” showed negative coefficients (β = .22 × [−.07]) (see Figure 3a). The results of previous studies examining the association between SRH knowledge and sexual risk behaviors varied in this regard. Some studies showed a positive association (Champion et al., 2013), while others did not (Needham et al., 2010). In this study, some factors underlying the path between “SRH knowledge” and “sexual behaviors” would influence the competitive mediation. As shown in the result, “SRH attitudes” was not a mediator between “SRH knowledge” and “sexual behaviors”: “SRH knowledge” was associated with “SRH attitudes,” whereas “SRH attitudes” was not associated with “sexual behavior.”“SRH attitudes” consisted the elements related to women’s empowerment on decision-making, acceptance of physical abuse by her husband or partner and sex negotiation. In Latin America, “machismo,” the beliefs that men are superior to women is prevalent, has influenced gender-based discrimination and violence (Carballo, 2015). Although the gender gap in Nicaragua has improved significantly between 2006 and 2021 in general (62 rank to 12 rank, mostly owing to educational attainment and political empowerment), health and economic participation and opportunity remain low (World Economic Forum, 2021). In particular, low decision-making power exists when it comes to women’s sexual and reproductive health (Japan International Cooperation Agency, 2012). Therefore, this “machismo” belief can be an obstacle for young women to have a decision-making power to prevent risky sexual behaviors, although they have sufficient knowledge of pregnancy prevention and risky sexual behaviors. This study used the existing dataset (ENDESA 2011/12) that did not include data on who (men or women) made the actual decision related to risky sexual behaviors. Further study is needed to investigate the gap between knowledge, attitudes, actual decision-making, and risky sexual behaviors in both genders.
This study had some limitations. The analysis used cross-sectional data and data from a Nicaraguan demographic and health survey collected within a specific time frame (2011 and 2012). Thus, only associations were established, and causal inferences or temporal relationships between the studied variables were not established. Furthermore, some questions were answered retrospectively and were susceptible to recall bias and memory lapse.
This study used data from a Nicaraguan Demographic and Health Survey conducted in 2011 and 2012, which is considered relatively outdated. However, it is still the most recent demographic and health survey in Nicaragua at the time of writing. Furthermore, studies focusing on adolescent SRH in the Central and Atlantic regions are lacking. The ENDESA 2011/12 is the only dataset that can be used to investigate the mechanisms of adolescent pregnancy and childbearing in this region. Therefore, data from ENDESA 2011/12 are acceptable for this study, even though certain sociodemographic and health indicators have improved over the last 10 years (Pan American Health Organization, 2019).
This study did not address ethnic or geographical differences within a group. The three major indigenous groups in eastern Nicaragua have distinct origins, histories, and characteristics, the perspectives of which were not included in this study. Miskitu and Mayangna live in the northern Atlantic region and retained their indigenous languages. In contrast, Rama living in the southern Atlantic region no longer speak their indigenous languages but Spanish and English. Although both Miskitu and Mayangna live in the northern Atlantic region, Miskitu live in coastal regions, while Mayangna live inland. It should also be noted that the four departments selected as the group from NC-E were not the same in terms of geographical perspectives. Jinotega is located in the country’s central area, with the western half of the department in mountainous areas, whereas the lowlands are similar to the rest of the Atlantic region. This study included Jinotega because the eastern half of the department is close to the Atlantic region in terms of geography and climate. The indigenous Mayangna also reside in the eastern part of Jinotega. These ethnic and geographical differences should be considered in future studies.
There was a limitation in the selection of indicators related to decision-making power related to risky sexual behaviors. This study used the existing dataset (ENDESA 2011/12) that did not include the data on who (men or women) made the actual decision related to risky sexual behaviors, not only the attitudes toward decision-making power. Future studies should assess the variables to investigate the gap between knowledge, attitudes, actual decision-making, and risky sexual behaviors in both genders.
Conclusions
Despite these limitations, this study provides new insights into adolescent pregnancy and childbearing mechanisms in Nicaragua by introducing the concept of mediating factors that would connect exogenous and outcome factors. The study also added new information on early pregnancy among young women in northern central and eastern Nicaragua (NC-E) where adolescent sexual reproductive health has rarely been studied. Educational attainment and sexual behaviors were crucial mediators in reducing early pregnancy and childbearing among young women in both NC-E and the Pacific region (PAC). Sexuality education was a crucial mediator in the NC-E but not in the PAC. Geographic factors had stronger associations with mediators of early fertility than ethnicity did. Although educational attainment and sexuality education are associated with improving knowledge on preventing early pregnancy, they did not contribute to reducing risky sexual behaviors. Further discussions on ethnic and geographical differences are needed, and elaboration of variables measuring the decision-making power of young women that would influence risky sexual behaviors is suggested for future studies. As implications for implementation, strengthening the sexuality education program is recommended, especially in the NC-E. The inclusion of the topics related to personal relationships and skills is also suggested for sexuality education programs. Additionally, the study suggested strengthening the program or the strategy for the empowerment of young women on decision-making and negotiation skills to hinder gender-based violence and risky sexual relationships.
Footnotes
Acknowledgements
I would like to express my gratitude to Dr. Sergio Ramón Gutiérrez Úbeda, Professor at the Center for Research and Health Studies of the National Autonomous University of Nicaragua; Dr. Marit Myvoll, a Sami social anthropologist and researcher at the Sámi Norwegian National Advisory Unit on Mental Health and Substance Use (SANKS/Sámi Klinihkka); and to Dr. Mette Kjær, Head of the Research Finnmark Hospital Trust, for their advice and guidance. I also would like to thank /Sámi Klinihkka and the Finnmark Hospital Trust for providing a supportive research environment.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.