
Abstract
Intimate partner violence (IPV) is highly prevalent in many countries, including Saudi Arabia. Studies have shown that 1 in every 10 women in Saudi Arabia is a victim of IPV. This is slightly lower than the prevalence of IPV in the WHO African, Eastern Mediterranean, and South-East Asia Regions, where approximately 37% of women in long-term partnerships report having experienced physical and sexual IPV during their lifetime. This review identified and analyzed the available empirical studies that explore IPV in Saudi Arabia. Nineteen (n = 19) studies were retrieved from three databases, including Medline, CINAHL, and PsycINFO, as well as Google and Google Scholar. Only empirical studies published in the English language and involving Saudi Arabian citizens were examined. We identified 13 studies that explored the prevalence of IPV and 11 studies that discussed factors associated with IPV. Eight studies examined the effects and consequences of IPV, six studies reported attitudes, perceptions, and knowledge related to IPV, and only three studies investigated victim response to IPV. Nineteen studies included women and only one study involved men as research participants. The findings suggest that previous studies undertaken in Saudi Arabia used quantitative approaches and gathered data via questionnaires, and therefore participants were not given the chance to describe how they defined different forms of IPV. More specifically, previous studies failed to explore the problem of IPV through the lens of Saudi men, creating a research gap related to defining their attitudes and perceptions of this phenomenon.
Plain Language Summary
This study aimed to identify the available empirical studies that examined the issue of intimate partner violence (IPV) in Saudi Arabia. A scoping review approach was used to explore the range, nature, and extent of literature on the topic. Nineteen (n = 19) studies were retrieved from three databases, including Medline, CINAHL, and PsycINFO, as well as Google and Google Scholar. The findings suggest that no effort has been made to understand the Saudi population’s perceptions of IPV, its definitions, or the reasons for its occurrence. Therefore, IPV is a sensitive and hidden issue that is not openly discussed in Saudi Arabia. This makes intensive and in-depth exploratory research about IPV even more important in the country.
Introduction
Intimate partner violence (IPV) “… refers to any behavior within an intimate relationship that causes physical, psychological or sexual harm to those in the relationship” (World Health Organization [WHO], 2012, p. 1). The term “IPV” also captures a wider array of violent phenomena and acknowledges that violence can happen in any intimate relationship irrespective of gender, marital status, or sexual orientation.
IPV can take many forms, including sexual, physical, and psychological abuse, and stalking (Centers for Disease Control [CDC], 2015). Sexual violence refers to any “forced sexual intercourse and other forms of sexual coercion” (WHO, 2012, p. 1). It includes rape, vaginal, oral, or anal sex by physical coercion or any painful, humiliating, or unwanted sexual acts (Australia’s National Research Organisation for Women’s Safety, 2019). Physical violence is the most common type of IPV and may involve beating, kicking, hitting, or slapping one’s partner and/or the use of physical force to inflict pain, cause disability, injury or even death (WHO, 2012). Psychological violence is mainly inflicted through controlling behavior (National Institute of Justice, 2007). Various acts include belittling, intimidation, threats of harm, insults, constant humiliation, and threats to take away children (WHO, 2012). Stalking-only recognized as a crime recently-refers to the act of closely to the act of closely and constantly monitoring another person’s activity and movement as a repeated behavior to make them feel insecure and intimidated (National Institute of Justice, 2007).
In Saudi Arabia, like many other Muslim countries, marriage is the only way a couple can legally live together (Coker, 2018). Marriage is traditionally arranged by tribes or families (Long, 2005; Zuhur, 2011) and individuals are encouraged to marry their cousins or other relatives to further strengthen family ties (Zuhur, 2011). Until year 2000, men could have more than one wife; however, monogamy is now encouraged. The historical context of IPV in Saudi Arabia is difficult to piece together for various reasons except for the modern period. Stories shaping the historical context of Saudi Arabia started to emerge only recently and have become more prevalent now that Saudi women can leave the country. Saudi women have fled Saudi Arabia in greater numbers because they can now access help through social media (Hennessy-Fiske, 2017). However, it is still too early for social media–assisted escape opportunities to contribute to the formation of an extended history of abuse in Saudi Arabia. Indeed, as Thomas and Housden (2017) pointed out, major social media platforms, such as Skype, Facebook, YouTube, and Twitter, were only launched just over a decade ago. In 2005, King Abdulla established the National Family Safety Program (NFSP) by decree to prevent IPV and child abuse. To combat IPV, NSFP provided training for healthcare professionals (Almuneef & Al-Eissa, 2011). Although the government acknowledged IPV, no clear laws were developed to criminalize IPV until 2013, when an organized media campaign was launched (Nabbout, 2018).
The media have played a significant role in changing the mindsets of Saudis regarding the treatment of women and pressuring authorities to enforce protective legal measures. An advertisement that ran in 2013 in Saudi national newspapers became an important landmark in the history of women’s rights in Saudi Arabia (Speiser, 2015). The advertisement featured a powerful image of a woman in a burqa with the skin around one of her eyes seriously bruised. Speiser (2015) showed that the media message was also promoted by the royal family; although the advertisement was produced by the international ad agency Ogilvy, the King Khalid Foundation—an organization that oversees the not-for-profit sector and advocacy—promoted the advertisement. It created significant change and prompted a nationwide discussion on women’s rights and IPV (Speiser, 2015). Less than 3 months after the advertisement, the Saudi Council of Ministers passed legislation banning any form of abuse in the workplace or at home. Therefore, the law forced courts to give out 12-month prison sentences coupled with fines of 50,000 SAR (=$ 3,300) to men convicted of perpetrating IPV (Speiser, 2015). However, the issue is still very relevant as many incidents are settled out of court by bribing the victim’s relatives to silence the victim.
Before Saudi Arabia established an IPV reporting center in 2016, Saudi women had no way of speaking up about IPV, regardless of their socioeconomic status (Nabbout, 2018). A social protection center was established by the Ministry of Labor and Social Development. Its responsibilities include receiving reports and addressing cases of IPV (Shiraz, 2016). During its first 3 days, the center received 1,890 reports related to IPV (Nabbout, 2018). In addition, the government has established social organizations which have a primary goal of protecting families from IPV, such as Al-Wafaa in Riyadh and Al-Bir in Jeddah. These institutions are responsible for increasing awareness about the impacts of IPV and empowering Saudi women by spreading information about their important role in society (Alsehaimi & Helal, 2021). Most recently, and as part of the Saudi vision 2030, “Saudi Arabia’s sweeping plans to overhaul its economy in coming years are matched by proposals for social transformation that extend to ways of tackling IPV, increasing city park space and reducing road deaths” (McDowall, 2016, p. 1). It is worth noting that 19 million SAR will be spent on raising awareness about IPV and 9 million SAR will be spent on IPV services (McDowall, 2016). However, research related to IPV in many countries, including Saudi Arabia, is scarce. To the best of our knowledge, very few efforts have been made to aggregate studies conducted in Saudi Arabia and limited information is known about the situation and possible causes of IPV in Saudi Arabia. Therefore, this study aims to aggregate and review available empirical evidence related to IPV among Saudi populations. The findings of the review will help to illuminate the current IPV situation in Saudi Arabia and also identify gaps in the available knowledge base to develop future research ideas. In addition, it will aid the development of culturally appropriate and specific interventions that can be used in Saudi Arabia.
Methods
For this study, a scoping review approach was used to explore the range, nature, and extent of literature on the topic (Arksey & O’Malley, 2005). This approach helps identify research gaps, theories, evidence, and key concepts (Grant & Booth, 2009; Halas et al., 2015).
Eligibility Criteria
Studies that explored IPV in Saudi Arabia and were published in a peer-reviewed journal, based on primary research, used empirical data (quantitative, qualitative, and mixed methods), written in the English language, and involved Saudi citizens were included in the review. Studies not published in English, scholarly or theoretical articles, editorials or commentaries, and gray literature such as master’s theses and doctoral dissertations were not included in the review.
Data Sources
Various search engines, including MEDLINE, CINAHL, and PsycINFO were used. Keywords used in the search included “domestic violence” AND “Saudi,”“domestic violence” in “Saudi,”“intimate partner violence” AND “Saudi,”“intimate partner violence” in “Saudi,”“wife abuse” AND “Saudi,”“wife abuse” in “Saudi,”“spousal violence” AND “Saudi,”“spousal violence” in “Saudi,”“women abuse” AND “Saudi,”“women abuse” in “Saudi,” and “violence against women” AND “Saudi.” Google and Google Scholar were also searched to identify studies not published in indexed journals. The reference list of each article was scrutinized to identify further studies that may not have been listed in the searched databases.
Study Selection
A total of 72 potentially relevant articles were identified. Fifty-three of these articles were excluded for various reasons, including lack of relevance (n = 18), inaccessibility (n = 1), lack of peer review (n = 1), non-empirical work (n = 3), being master’s and doctoral theses (n = 7), and being gray literature (n = 3). In addition, eight studies were excluded because the sample did not include Saudi citizens. Finally, 19 studies were included in this review. Figure 1 shows a PRISMA diagram illustrating the process and number of included and excluded studies.
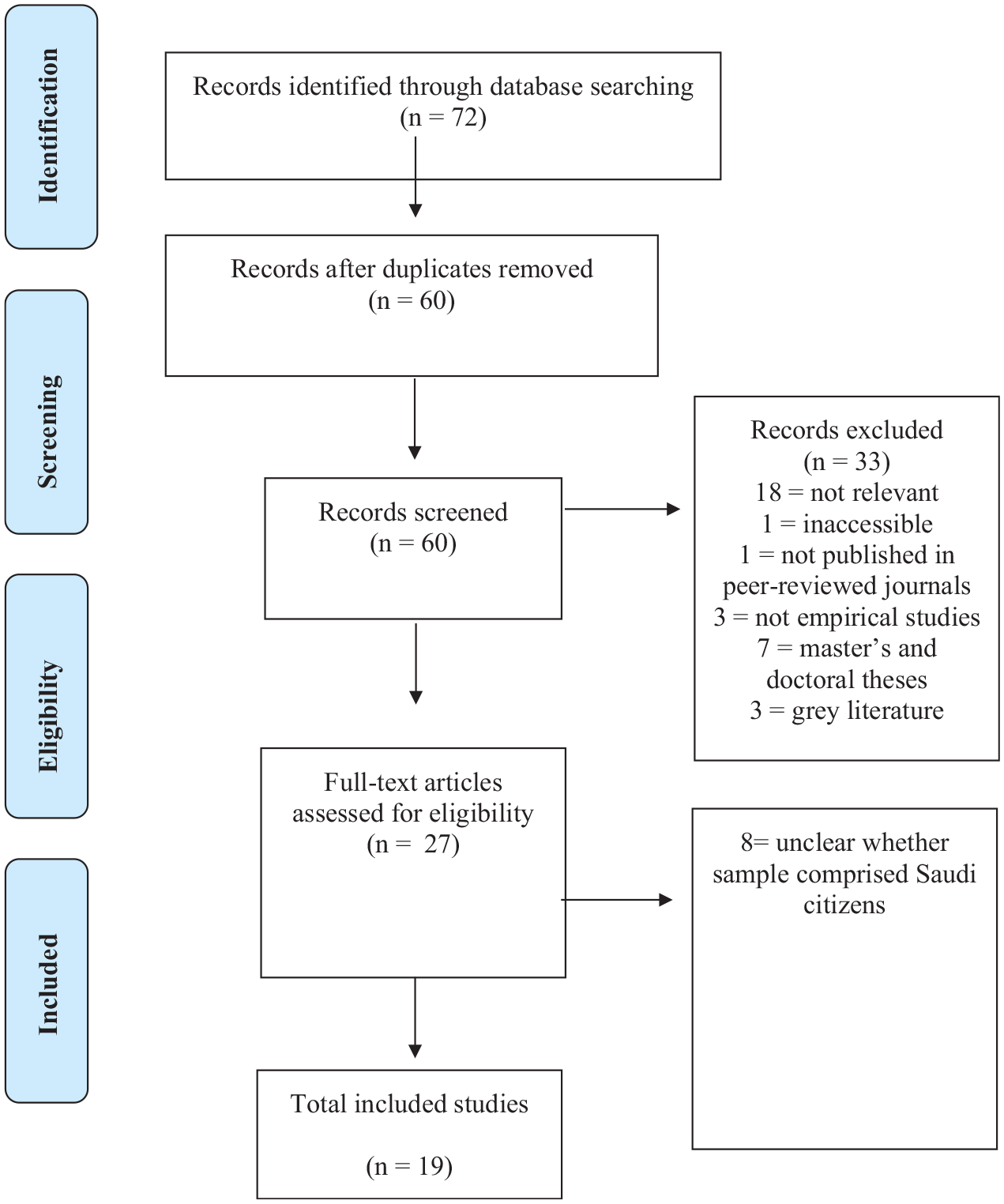
PRISMA flow diagram.
Data Extraction
Data were extracted using a specially developed extraction tool to identify information about the date of publication, authors, study location, study design, number of study participants and their demographic characteristics, and methods of data collection and data analysis. Five themes were developed to present the narrative findings and insights from the included studies.
Results
Study Characteristics
Focus
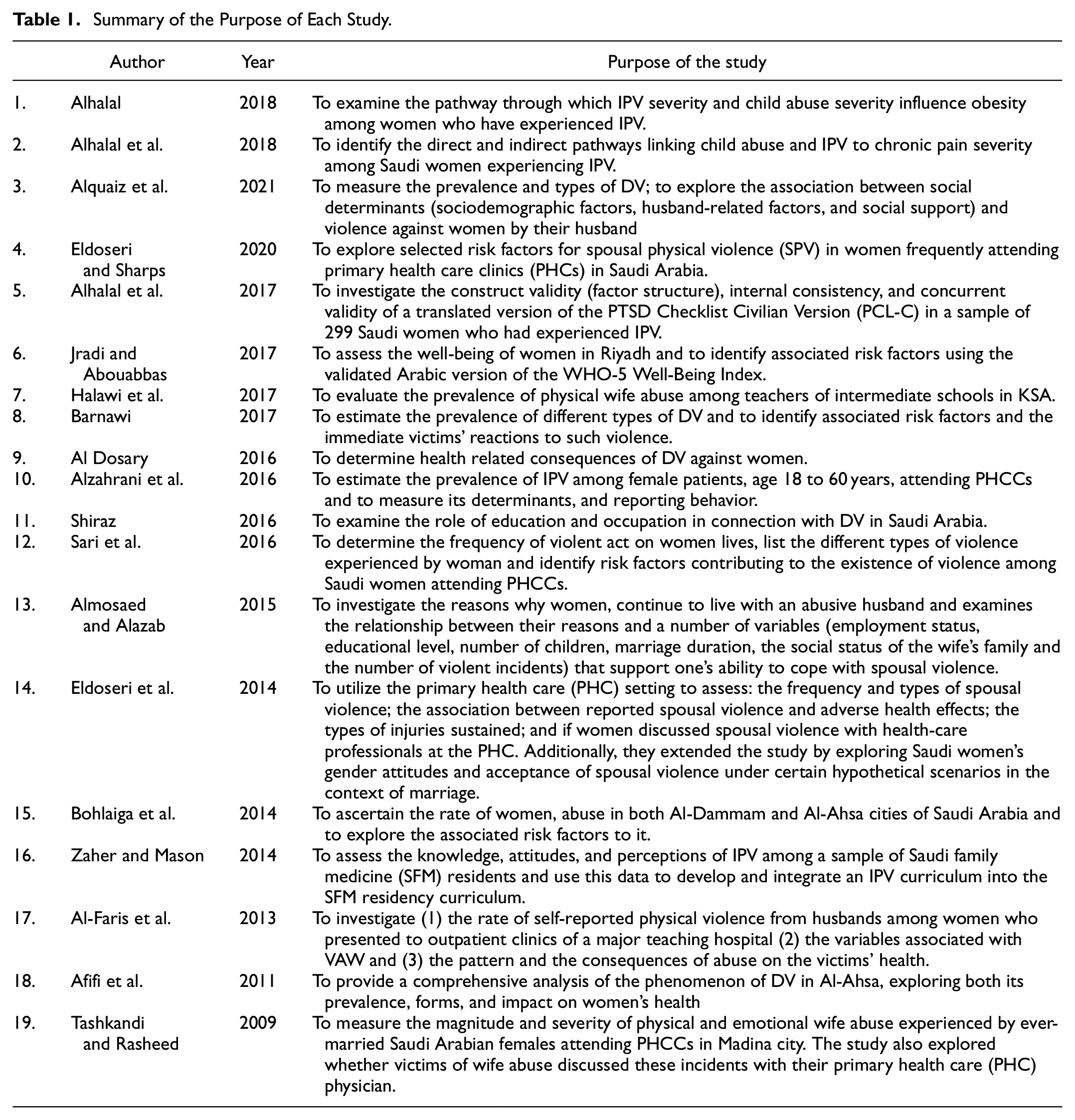
The issue of IPV in Saudi Arabia has only recently been explored and the first relevant study was only published in 2009. Table 1 summarizes the purpose of the included studies. IPV against women by men was the primary focus of 18 studies. Most studies explored the perspectives of female victims of IPV, and only one examined the perspectives of health professionals (men and women) about IPV (Zaher & Mason, 2014). Table 2 summarizes the settings, methods, sampling and participants, data collection techniques, and findings of these studies.
Summary of the Purpose of Each Study.
Summary of the Geographical Setting, Methods, Data Collection Techniques, and Participants.

Many studies reported the prevalence of IPV (n = 13), the factors associated with IPV (n = 11), and the effects and consequences of IPV (n = 8). Others reported attitudes, perceptions, and knowledge of IPV (n = 6) and victim response to IPV (n = 3). Table 3 presents the outcome data of each study and Table 4 presents a summary of critical findings.
Outcome Data of Each Study.

Summary of Critical Findings.

Setting
IPV was explored in 4 of 13 Saudi Arabian provinces. The studies were conducted in hospitals (n = 14), shopping malls, colleges, and government shelters (n = 4) and through an online survey (n = 1). The sample size in the studies ranged from 30 to 2,000. All the studies were quantitative; 17 out of 19 studies used cross-sectional designs, and two studies used descriptive designs (see Table 2).
Data Collection
Some studies used pre-tested, standardized questionnaires including the World Health Organization (WHO) Violence Against Women questionnaire (Afifi et al., 2011; Alquaiz et al., 2021; Alzahrani et al., 2016; Barnawi, 2017; Eldoseri et al., 2014; Jradi & Abouabbas, 2017; Shiraz, 2016) and Composite Abuse Scale (CAS), NorVold, Domestic Abuse Questionnaire (NOVAQ and NORAQ) (Al Dosary, 2016; Sari et al., 2016), the Physician Readiness to Manage Intimate Partner Violence Survey (PREMIS) (Zaher & Mason, 2014), the Conflict Tactics Scale, the Lie scale, the Kansas Marital Satisfaction Scale (Tashkandi & Rasheed, 2009), and the Hurt-Insult-Threaten-Scream (HITS) instrument (Alzahrani et al., 2016). Other instruments used included the PTSD Checklist-Civilian version, (PCL-C), the Centre for Epidemiologic Studies-Depression (CESD) Scale, body mass index (BMI) and waist circumference, and the Chronic Pain Grade (CPG) scale (Alhalal, 2018; Alhalal et al., 2017; Alhalal, Ford-Gilboe et al., 2018). Several studies used self-administered questionnaires (Al Dosary, 2016; Almosaed & Alazab, 2015; Alzahrani et al., 2016; Barnawi, 2017; Bohlaiga et al., 2014; Halawi et al., 2017; Shiraz, 2016), while others used structured interviews (Afifi et al., 2011; Alhalal, 2018; Alhalal et al., 2017; Alhalal et al., 2018; Alquaiz et al., 2021; Eldoseri et al., 2014; Eldoseri & Sharps, 2020). Only one study used semi-structured interviews (Tashkandi & Rasheed, 2009). Only five studies reported the validity and reliability (Bohlaiga et al., 2014; Jradi & Abouabbas, 2017; Shiraz, 2016; Tashkandi & Rasheed, 2009; Zaher & Mason, 2014) of the instruments used.
Prevalence of IPV Among the Saudi Population
Thirteen studies reported the prevalence of IPV in Saudi Arabia (see Table 3). Most studies (n = 11) focused on the prevalence of physical IPV. Others explored emotional (n = 7) and sexual IPV (n = 5). Common acts of physical IPV included slapping (Al-Faris et al., 2013; Alquaiz et al., 2021; Tashkandi & Rasheed, 2009) and pushing or shoving (Alquaiz et al., 2021; Tashkandi & Rasheed, 2009). The lifetime prevalence of physical IPV ranged between 7.5% and 57% and the prevalence during the last 12 months ranged between 16% and 40%.
Commonly reported acts of emotional IPV included insults and threatening behavior, shouting, belittling, and intimidating (Afifi et al., 2011; Alquaiz et al., 2021; Tashkandi & Rasheed, 2009). The lifetime prevalence of emotional IPV ranged between 7.5% and 75.10%, and the prevalence during the last 12 months ranged between 32.8% and 69%.
Commonly reported acts of sexual violence were rape, having sex out of fear, forced shameful behavior, and forced sexual acts that were degrading, humiliating, or unacceptable (Afifi et al., 2011; Alquaiz et al., 2021). The lifetime prevalence of sexual IPV ranged between 5.9% and 34.3%, and the prevalence during the last 12 months was 10% (Barnawi, 2017).
Out of 13 studies, five reported the prevalence of more than one type of IPV (physical, emotional, and sexual) during a lifetime and the last year (Afifi et al., 2011; Alquaiz et al., 2021; Bohlaiga et al., 2014; Sari et al., 2016; Tashkandi & Rasheed, 2009). The lifetime prevalence of IPV ranged from 33% to 57.80% and the prevalence during the last year ranged from 11.90% to 20%.
Only one study explored controlling behavior, including keeping a partner away from friends, ignoring and treating a partner indifferently, restricting a partner’s contact with family, suspiciousness, and restricting a partner’s access to health care (Alquaiz et al., 2021). The prevalence of controlling behavior was 36.8% (Alquaiz et al., 2021). A few studies explored other forms of IPV, including social and economic IPV, and the prevalence was reported to be 34% and 26%, respectively (Barnawi, 2017).
Causes and Associated Factors of IPV
Eleven studies reported factors connected to IPV in Saudi Arabia (see Table 3). Due to the high number of studies reporting factors connected to IPV, the median of these studies was calculated (see Table 5). The findings suggest that men were more likely to perpetrate IPV if their wives were previously divorced (53.2%), unemployed (43.3%), or had low levels of education (20%). Husbands’ low income (43.5%), the presence of multiple wives (35.1%), and unemployment (29%) were also identified as predictors of IPV. Only two studies discussed the role of occupation and education in connection with IPV among Saudi women (Almosaed & Alazab, 2015; Shiraz, 2016). Women with lower levels of education and employment experienced higher levels of violence and were more likely to accept and cope with violence. Experiencing childhood abuse was also identified as a risk factor for perpetrating IPV and perceiving it as normal (Al-Faris et al., 2013).
The Rate of Factors Associated with IPV.

Attitudes, Perceptions, and Knowledge of IPV
Limited studies explored attitudes, perceptions, and knowledge of IPV among Saudi populations (see Table 3). For example, three studies explored women’s perspectives on why some men commit IPV (Al-Faris et al., 2013; Barnawi, 2017; Halawi et al., 2017). Common reasons included socio-cultural influences, social stressors on men, unfaithfulness, poor income, and alcohol or drug use (Barnawi, 2017; Halawi et al., 2017). Other reasons include women disobeying their husbands, leaving home without permission, refusing sex, and not completing housework (Al-Faris et al., 2013).
Two studies explored the attitude toward accepting IPV in Saudi Arabia (Bohlaiga et al., 2014; Eldoseri et al., 2014). Their findings suggest that most women do not accept violence (92%); however, 8% of women had either no objection or had an accepting attitude toward violence (Bohlaiga et al., 2014) in situations such as a wife’s infidelity (Eldoseri et al., 2014), disobedience to her husband, and leaving the house without permission (Al-Faris et al., 2013). No research was conducted to explore men’s attitudes toward IPV in Saudi Arabia.
Only one study evaluated knowledge of IPV among health care professionals (Zaher & Mason, 2014). The participants identified alcohol or drug use as a reason for the occurrence of IPV. The findings also suggest that the sample showed low knowledge and preparedness to identify and manage the disclosure of IPV.
Victim Response to IPV
Victims’ responses to IPV in Saudi Arabia have been relatively unexplored by existing studies (see Table 3). Complaining and speaking with one’s own family, being abusive to them, and requesting divorce or separation were the most common responses from women exposed to IPV. Other common responses included leaving home and going to social services, police, judges, and human rights organizations, complaining to sheikhs and friends, going to the hospital, visiting a doctor, and talking to the husband’s family and friends (Afifi et al., 2011; Alzahrani et al., 2016; Barnawi, 2017).
Findings from the studies suggest that as many as 41.4% of Saudi women do not disclose their experience or seek help for various reasons, including financial dependence on the husband, fear of divorce, fear of leaving their children in case of divorce, acceptance of maltreatment, and hope that the husband will stop the abuse. Children were the most common reason (37.8%) for not disclosing experiences of IPV (Afifi et al., 2011).
Effects and Consequences of IPV
Eight studies reported the effects and consequences of IPV (see Table 3), including mental health problems such as depressive symptoms and post-traumatic stress disorder (PTSD). Other health impacts experienced by victims included chronic pain, poor health status, somatic complaints (Afifi et al., 2011; Al Dosary, 2016; Barnawi, 2017; Eldoseri et al., 2014), suicidal thoughts, and drug abuse (Afifi et al., 2011; Eldoseri et al., 2014). Obesity among Saudi women was also reported as a common consequence of IPV (Alhalal, 2018; Alhalal et al., 2017; Alhalal et al., 2018).
Discussion
This review aimed to aggregate available evidence about IPV in Saudi Arabia and, therefore, outline critical findings and implications for practice, policy, and research (Tables 4 and 6). Of the 19 studies reviewed, three were conducted in similar settings by the same primary author (Alhalal, 2018; Alhalal et al., 2017; Alhalal et al., 2018), as were a further two (Eldoseri et al., 2014; Eldoseri & Sharps, 2020). This raises questions about the impact of the findings because of the authors’ aims and the use of similar or identical samples. Furthermore, all studies involved female participants, apart from one which explored health professionals’ perceptions and knowledge of IPV. In addition, most of the studies have been conducted by female researchers, for understandable reasons. Due to the sensitivity of IPV both culturally and personally, male researchers may face many obstacles in discovering IPV among Saudi women and vice versa. Moreover, all the reviewed studies employed a quantitative approach using questionnaires. Most studies used a cross-sectional design, precluding the exploration of the other relative variables affecting the issue or of the phenomenon in depth. Most studies did not report the validity and reliability of the questionnaires.
Implications for Practice, Policy, and Research.

It was also noted that four studies reported the prevalence of IPV in the Riyadh region (Al-Faris et al., 2013; Alquaiz et al., 2021; Barnawi, 2017; Jradi & Abouabbas, 2017), three studies reported the prevalence of IPV in Makkah region (Alzahrani et al., 2016; Eldoseri et al., 2014; Eldoseri & Sharps, 2020), two studies were conducted in the Eastern region (Afifi et al., 2011; Bohlaiga et al., 2014), and two studies took place in the Madinah region (Sari et al., 2016; Tashkandi & Rasheed, 2009). As the samples were from urban areas and the biggest cities in Saudi Arabia, no studies investigated the experiences of participants from lower socioeconomic classes. Moreover, the lifetime prevalence rate of IPV undoubtedly varies between regions in Saudi Arabia, as was clearly shown by the various studies (Afifi et al., 2011; Alquaiz et al., 2021; Bohlaiga et al., 2014; Sari et al., 2016; Tashkandi & Rasheed, 2009). Some regions, such as Madinah, have recorded a high lifetime prevalence rate of IPV (57.8%) (Tashkandi & Rasheed, 2009). On the other hand, the Eastern region has reported the lowest lifetime prevalence rate of IPV (33%) of all regions (Bohlaiga et al., 2014). Furthermore, the most common types of IPV among Saudi women, in order of frequency, were emotional IPV, physical IPV, and torture, while the least common form of IPV was sexual. However, this finding could be due to reporting issues. Nevertheless, the prevalence of two or three types of IPV over a lifetime was slightly high in comparison to the median rate of each form (physical, emotional, and sexual). Therefore, to verify the validity of this result, the lifetime median prevalence of physical, emotional, and sexual IPV was calculated (see Table 7). The median prevalence of emotional IPV was 33.4%, the median prevalence of physical IPV was 22.9%, and the median lifetime prevalence of sexual IPV was 9.8%. Therefore, the median prevalences of all forms of IPV were 33.40%, 25.90%, and 9.80%, respectively, and the median result of these numbers is 25.90%. This contradicts some of the prevalence findings that have been previously highlighted (Afifi et al., 2011; Alquaiz et al., 2021; Bohlaiga et al., 2014; Sari et al., 2016; Tashkandi & Rasheed, 2009), indicating the logical prevalence of IPV nationally.
Prevalence Rate of IPV.

Previous international studies that have been conducted on the prevalence of IPV have shown that partner violence against women had a high lifetime prevalence of 37.7% in Southeast Asia and 23.2% in high-income regions. Low- and middle-income regions within the Americas had a rate of 29.8%, the Eastern Mediterranean region had a rate of 37%, Africa had a rate of 36.6%, the Western Pacific had a rate of 24.6%, and the rest of Europe had a rate of 25.4% (García-Moreno et al., 2013). Therefore, the IPV prevalence rate identified in this review was lower than in regions such as Southeast Asia, Eastern Mediterranean, and Africa. However, regions such as the Americas, the Western Pacific, and Europe had IPV prevalence rates that were similar to the rate identified by this review, which was 25.90%. Furthermore, a wife’s unemployment was identified as a risk factor for IPV in this review, which is consistent with previous studies conducted in western regions (Anderberg et al., 2016). However, employment was identified as a risk factor for IPV in China, contradicting the findings of this review (Zhao et al., 2022). Furthermore, it is important to highlight that one of the factors positively linked to IPV in this review was divorced marital status. This corroborates a study conducted in China that suggested a wife’s marital status (remarriage, cohabitation, divorce) was associated with IPV (Zhao et al., 2022). Additionally, in line with a previous systematic review of IPV, this review indicated that men experiencing a lower income level was related to female IPV victimization (El-Moslemany et al., 2022). In this review, unfaithfulness was one of the common reasons for IPV. This corroborates the findings of other studies that have identified a link between dishonesty and IPV and argued that a woman’s infidelity, in particular, was a risk factor for IPV (Ibragimova, 2010). Alcohol or drug use was also identified as a common reason for IPV. This is consistent with prior studies of available data that have shown a strong association between IPV and substance use (Bacchus et al., 2018; Devries et al., 2014; Jennings et al., 2012). Speaking about IPV to the wife’s family was a common response to IPV in Saudi Arabia. This is consistent with previous studies conducted in Uganda and Nigeria (Katushabe et al., 2022; Okenwa et al., 2009). However, contrasting the findings of previous studies, this review revealed that most women in Saudi Arabia do not disclose their IPV experiences (Katushabe et al., 2022; Okenwa et al., 2009). Mental health problems such as depression, PTSD, and suicidal thoughts were reported as consequences of IPV in Saudi Arabia. Indeed, IPV has previously been reported as resulting in far-reaching psychological issues and mental health problems, including PTSD, depression, and suicide attempts (Devries et al., 2013; Pico-Alfonso et al., 2006). Despite similarities between the findings of this review and those of prior studies, the significant differences highlighted above suggest that more research is necessary to fully understand the issue of IPV in Saudi Arabia, particularly regarding attitudes, perceptions, and responses to IPV.
Strength and Limitations
This review has offered insights into the quality and quantity of studies that have been carried out on IPV in Saudi Arabia. It is essential to note that this study was not restricted to a specific study design, whether qualitative or quantitative. As such, it provides a comprehensive view of the perception of IPV in Saudi Arabia, concerning existing empirical evidence. Furthermore, the review revealed new insights into the median prevalence rate of IPV and the risk factors associated with IPV in Saudi Arabia. The review has also assisted in the identification of areas that require further investigation in this field. The likelihood of reporting literature containing the same samples could not be eliminated. This may have impacted the reported frequency of IPV. Additionally, it may also present an incorrect image and intensify the frequency of IPV in Saudi Arabia. The other limitation of the study is that we only incorporated research literature published in peer-reviewed journals and which had been published in the English language. There is also a possibility that some studies published in journals that were not indexed in CIHALL, Psych Info, or MEDLINE could not be identified.
Conclusion
This review aimed to identify the available empirical studies that examined the issue of IPV in Saudi Arabia. The studies examined demonstrate that IPV is prevalent in Saudi Arabia. However, the findings of the studies may represent the middle and upper socioeconomic classes of Saudi citizens because existing studies excluded samples from rural areas of Saudi Arabia, consequently excluding the experiences of lower socioeconomic classes. The prevalence of lifetime IPV varies between regions, raising questions about the representativeness and generalizability of IPV data among Saudi women. Furthermore, these studies may overestimate the prevalence of IPV in Saudi culture. However, although there is a chance of overestimation, it is apparent that IPV is a significant and serious social problem in Saudi Arabia. Furthermore, no effort has been made to understand the Saudi population’s perceptions of IPV, its definitions, or the reasons for its occurrence. Therefore, IPV is a sensitive and hidden issue that is not openly discussed in Saudi Arabia. This makes intensive and in-depth exploratory research about IPV even more important in the country.
Implications for Practice, Policy, and Research
The findings of this review highlight several implications for future practice, policy, and research. For example, professionals in the field of IPV should be adequately trained and formally qualified to deal with IPV-related concerns. This group consists of medical staff (such as nurses and physicians), social welfare workers (such as therapists, social workers, and counselors), and the legal profession (such as judges, lawyers, and the police). In addition, these professionals should remain up-to-date and educated on all aspects of IPV, both locally and globally. They should also regularly participate in IPV training to improve their knowledge of the issue. All organizations that deal with IPV should collaborate to develop joint solutions to the issues that they are unable to solve individually.
IPV should also be addressed by the legal system. The regulations and laws that govern the country’s civil, family, and criminal courts are entirely unwritten; codifying the legal system would provide greater clarity and uniformity to judicial judgments. Furthermore, neither government nor non-government IPV-related agencies in Saudi Arabia are currently held responsible for any shortcomings. Consequently, establishing a monitoring body would ensure that these agencies remain responsible and accountable and are successful in their tasks.
Further quantitative research is needed to recruit participants from a diverse range of socioeconomic classes, as the samples were recruited from urban areas and the biggest cities in Saudi Arabia. In addition, this study identified that earlier studies lacked a cultural interpretation of IPV from the perspective of Saudi men and women. Furthermore, there has been no research on defining Saudi attitudes and perceptions of IPV. There were other clear research gaps, including the perspectives of men, who can play a significant role in preventing IPV in Saudi Arabia. The available empirical research on IPV in Saudi Arabia employs quantitative approaches and collects data using surveys. The survey questionnaires use definitions of IPV that may be more appropriate for other countries and cultures. The authors often assumed that respondents’ definitions of IPV aligned with their own, which may not be the case due to cultural and social differences. In addition, given the sensitive nature of the topic, participants’ responses may be biased because they wish to conceal sensitive information. Therefore, researchers should not blindly impose the commonly accepted definition of IPV on this population. Instead, further qualitative research is necessary to provide a better understanding of IPV and, more specifically, the roles of Saudi men. Examining the role of Saudi men will identify the complex dynamics of abuse in marital relationships and explore the factors associated with IPV in Saudi Arabia. The results of this review also suggest that future research should identify Saudi men’s definitions of IPV to understand what behaviors they qualify as physical, emotional, or sexual IPV. This would avoid applying the western definitions of IPV to Saudi Arabia. Indeed, understanding how Saudi men perceive the phenomenon of IPV is worthwhile and will aid the development of culturally specific explanations of IPV in Saudi Arabia. Therefore, researchers in this area should use more qualitative research methods to identify Saudi men’s perspectives in cultural and social contexts. However, although qualitative research frameworks can explore delicate and difficult issues, the social problem of IPV is best understood through an intensive and logical method of understanding its factors and features. Charmaz (2014) states that grounded theory is a practical framework as it is an organized and logical, yet flexible, manifestation of the qualitative framework. Consequently, this framework could be useful in exploring participants’ understanding of IPV and it will help to construct culturally specific understandings of IPV.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Turki Alqurashi is supported and funded by Umm Al-Qura University, Kingdom of Saudi Arabia.
Data Availability Statement
The datasets generated and analysed during the current review are available from the corresponding author on reasonable request.