
Abstract
This study aimed to understand, from the users of Health Information Systems’ perspectives, the essential components these technologies must present to be considered appropriate for incorporation and use in the Brazilian Unified Health System. As a secondary objective, we organized the results in the dimensions of the RE-AIM framework to facilitate future translation into practice. Qualitative exploratory research was carried out through a questionnaire with open-ended questions. We built the questions based on the RE-AIM and RE-AIM QuEST frameworks. For data organization and analysis, we used the NVivo 12® software, opting for the thematic categorical analysis strategy in three stages. Twenty-nine primary care and hospital services professionals participated, including nurses, physicians, pharmacists, dentists, community health workers, and management positions. Among the five dimensions of the framework used, sixteen analytical categories emerged. Constructs related to the interoperability between different healthcare services, implementation costs, infrastructure, reduction of bureaucracy, and guarantee of information security were deemed essential when considering implementing a new information system. The sustainability of technology in health services was directly associated with its performance quality to ensure that health professionals do not abandon the use of its functions.
Plain Language Summary
This study aimed to understand, from the users of Health Information Systems’ perspectives, the essential components these technologies must present to be considered appropriate for incorporation and use in the Brazilian Unified Health System. As a secondary objective, we organized the results in the dimensions of the RE-AIM framework to facilitate future translation into practice. We conducted qualitative exploratory research using a questionnaire with open-ended questions. Twenty-nine primary care and hospital services professionals participated, including nurses, physicians, pharmacists, dentists, community health workers, and management positions. The results show that the interoperability between different healthcare services, implementation costs, infrastructure, bureaucracy reduction, and information security guarantee is essential when implementing a new information system. The sustainability of technology in health services was directly associated with its performance quality to ensure that health professionals do not abandon its functions.
Keywords
Introduction
Background and Rational
Despite being a reality in most healthcare settings in Brazil, using technologies such as Information Systems (IS) must overcome barriers to be considered adequate, safe, efficient, and sustainable. The territorial magnitude and the socio-economic disparity between different regions outline scenarios ranging from the lack of infrastructure for its adoption to the excess of information handled daily and fragmentation between the public and private health systems (Alves et al., 2022; Cavalcante et al., 2015).
Information System is a type of health technology that requires evaluation for incorporation in the Unified Health System (known as SUS—Sistema Unico de Saúde); a previous regulation study developed by our team identified that IS are not included in the list of products that demand analysis at this time (Alves et al., 2021). The Brazilian Society of Health Informatics (SBIS—Sociedade Brasileira de Informática em Saúde) provides on-demand certification for Electronic Health Record Systems (S-RES—Sistema de Registro Eletrônico de Saúde) based on good practices, functionalities, structure, content, information security, among other aspects. However, as a voluntary process it is at the discretion of developers and institutions that acquire the technology whether this certification is required (Sociedade Brasileira de Informática em Saúde, 2022).
After consulting the National Institute of Industrial Property (INPI—Instituto Nacional de Propriedade Industrial) in April 2021, using the portal “Fala.BR—Integrated Platform for Ombudsman and Access to Information,” we found that until December 2020, there were more than 600 Computer Programs patent records for the healthcare area in Brazil (Instituto Nacional de Propriedade Industrial, 2022). Considering nationally based Health Information Systems (HIS), from 2010 to 2018, approximately 54 were in operation (Coelho Neto & Chioro, 2021). The Brazilian National Health Information and Informatics Policy indicates the high number of available IS and their heterogeneity as one of the reasons for the need for reorientation and construction of an articulated National Health Information System (Brasil. Ministerio da Saude, 2015).
A scenario where several technologies are available but lack a well-defined evaluation for proper incorporation flow into healthcare services requires careful analysis from managers and professionals for IS adoption, considering its cost-benefit. From this perspective, studies exploring Dissemination and Implementation Science theories and models are relevant to support planning, evaluating, and incorporating the best available option according to specific needs (Colditz & Emmons, 2018). The RE-AIM framework can help researchers think about knowledge translation into practice, considering the importance of contexts in design, planning, and evaluation. Also, its use allows multi-level analysis in its dimensions (Holtrop et al., 2021).
This research is part of a mixed-method study that developed criteria for evaluating and incorporating Information Systems in the Brazilian Unified Health System (SUS), using concepts and frameworks from Dissemination and Implementation Science. After our team developed documental research (Alves et al., 2021), a literature review (Alves et al., 2022), and a systematic review, we identified a need for more evidence considering the IS users’ perspectives regarding the technology adoption in Brazil.
This qualitative approach addresses this gap, and we organized the results in the RE-AIM structure to facilitate research translation into practice. In addition to the theoretical and practical application to the Brazilian Unified Health System, structuring the results in the RE-AIM framework dimensions provides a model for other international researchers who may face similar challenges in this area of research.
Literature Review
Health data and information are essential for planning public policies, improving access and quality of care, and ensuring services reach the entirety of the population. However, there is still a significant difference between countries regarding their level of socioeconomic development and the adoption and quality of Health Information Systems (Alves et al., 2022; World Health Organization, 2020).
Studies have evaluated Health Information Systems from different perspectives, whether in the context of guidelines for developing countries (Ngugi et al., 2021), specific contexts and policies (Ahmadian et al., 2015), or even considering induced errors and performance quality (Yusof & Sahroni, 2018). In the Brazilian scenario, reviews consider the approach by institutional context, whether hospital (Pereira et al., 2016), primary care (Carreno et al., 2015), or the performance and quality of stored data (Correia et al., 2014).
Worldwide, user satisfaction is also a concern and directly related to the success of using Information Systems. A systematic review developed using quantitative and qualitative approaches to analyze the adoption of HIS found that ease of use, training, and leadership support are the most relevant influencing factors (Yusof et al., 2007). More recently, a study developed in seven countries of the European Union showed that, for health professionals, effectiveness and affordability matter the most (Eivazzadeh et al., 2018). Another research developed in Ethiopia also showed that health professionals’ computer literacy can interfere with user experience and satisfaction with the technology (Walle et al., 2023).
In a broader concept, an IS “collects, processes, stores, analyzes and disseminates information for a specific purpose” (Turban et al., 2005, p. 40). HIS must aggregate data, information, and knowledge to support planning and decision-making (Marin, 2010). An S-RES captures, stores, presents, transmits, or prints identified health information (Sociedade Brasileira de Informática em Saúde, 2022). These terms are often used synonymously (Marin, 2010; Waegemann, 2002), and we adopted this generalization in this research, including possibilities for discussing the Electronic Patient Record (EPR), all under the term HIS.
Objectives
This study aimed to understand, from the users of Health Information Systems’ perspectives, the essential components these technologies must present to be considered appropriate for incorporation and use in the Brazilian Unified Health System. As a secondary objective, we organized the results in the dimensions of the RE-AIM framework to facilitate future translation into practice.
Method
Study Design
This study is exploratory qualitative research (Polit & Beck, 2011). We initially planned to conduct in-person interviews; however, due to the COVID-19 pandemic (which resulted in sanitary restrictions and work overload for health professionals), we adapted the data collection strategy to use Google Forms®. Participants answered three objective questions of a descriptive nature of professional profile and open questions without restrictions on the size of the answers, which we designed to explore the phenomenon of Health Information Systems encompassing the five dimensions of the RE-AIM framework.
The RE-AIM model (R = Reach, E = Efficacy/Effectiveness, A = Adoption, I = Implementation, M = Maintenance), translated and culturally adapted to Brazil, is a dissemination and implementation science framework designed to help in the planning and evaluation process of programs, interventions, and policies, considering the adoption and implementation of sustainable actions while balancing individual and organizational contextual factors (Almeida et al., 2013). To structure the questions according to each of the five dimensions, we used the RE-AIM Qualitative Evaluation for Systematic Translation (RE-AIM QuEST) as a guide. RE-AIM QuEST was developed to strengthen the original RE-AIM model, enabling the expansion of qualitative approaches and identification of barriers in implementing initiatives and the role of contexts (Forman et al., 2017). Four experts in healthcare and the RE-AIM model validated the questions.
Data Collection
In the Reach (R) dimension, we asked participants about their perceptions regarding users impacted by an HIS, the ideal proportion of technology reach, and possible factors that could interfere with including new users. In Efficacy/Effectiveness (E), we discussed what they expect regarding performance from an HIS (requirements, functionalities) for daily use and the goal of using this type of technology. For the Adoption dimension (A), we considered both individual and organizational points of view on the factors that can interfere with the processes of adoption and use of an HIS. Participants raised aspects that institutions must consider in the Implementation (I) dimension. Regarding the Maintenance dimension (M), participants focused on aspects related to the use of technology in the medium and long term.
We described the open-ended questionnaire in Table 1 with the notes provided to the participants to facilitate their understanding of the topic.
Open-Ended Questionnaire.
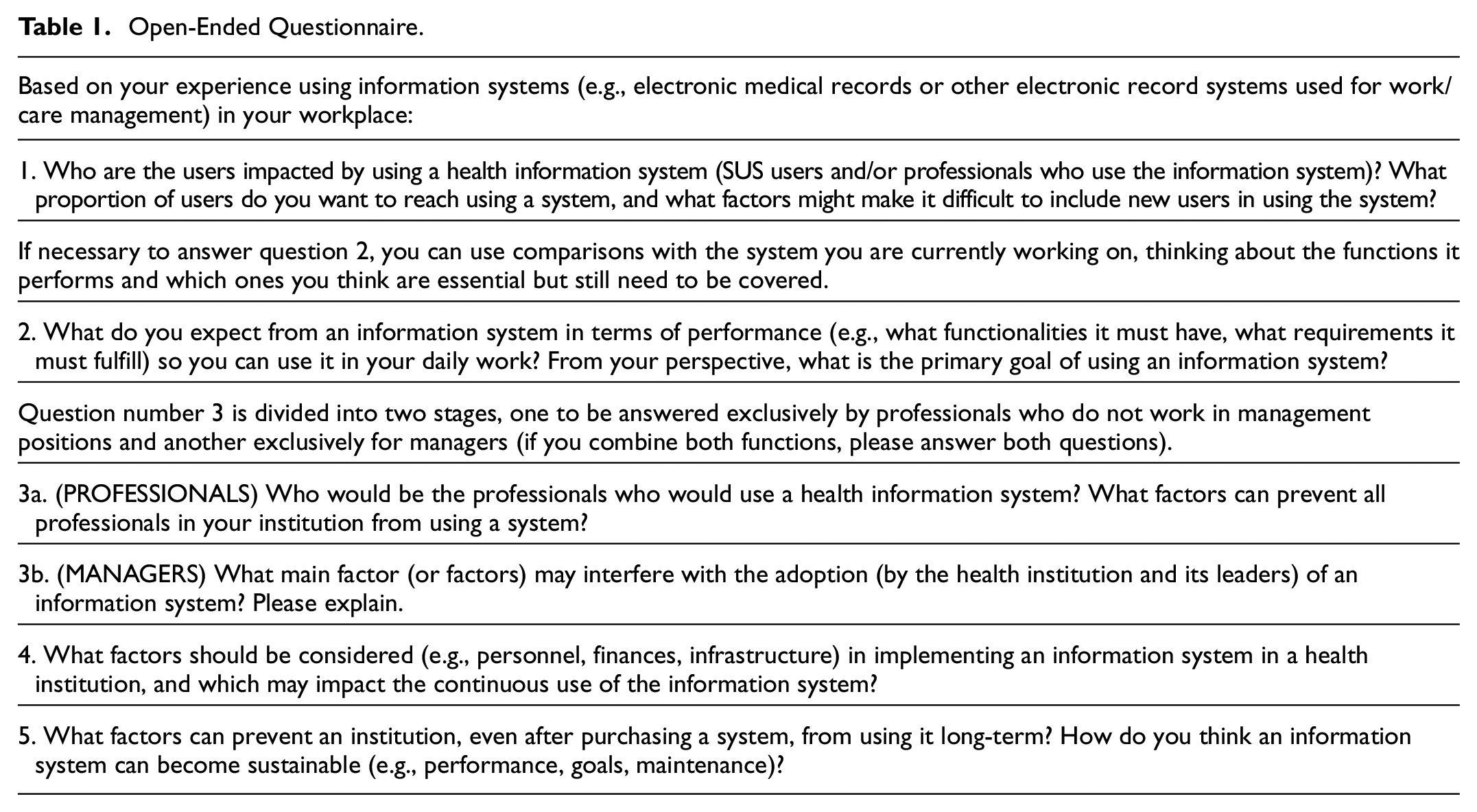
Data collection took place from March to May 2021, and we ended this process when we reached saturation based on the observation of theme repetition (Bardin, 2011). We collected all data in Portuguese, and the questions presented in Table 1 represent a direct translation from Portuguese to English solely for inclusion in this article.
Participants and Scenario
The eligibility criteria included professionals from different academic backgrounds working in health services at the Primary Care and Hospital levels and those working in health management positions. The exclusion criteria considered professionals working for less than three months in the institutions or those who did not use Information Systems daily.
The research was in Florianopolis, Santa Catarina, Brazil, in primary care and hospital settings. We chose the municipality of Florianopolis due to its prominent position on the national scene regarding Primary Health Care services.
After the Research Ethics Committee approved the project, we contacted health departments responsible for conducting research in both settings. At the hospital, the Head of the Research Management Unit sent the invitation via email to the institution workers. In Primary Care, the Florianopolis School of Public Health provided the research team with emails for 12 Primary Healthcare Centers coordinators. The research team sent these coordinators an initial email invitation to participate in the study and to invite further all health professionals currently providing patient care at their facility if they fit the eligibility criteria (described above).
Data Analysis
For data treatment, we opted for the thematic content analysis strategy, divided into three stages: pre-analysis, material exploration, and treatment of results (Bardin, 2011), carried out with the support of the NVivo 12® software (Figure 1). In the pre-analysis stage, we organized the files, imported them into the software, and defined the analysis objectives. During the material exploration, we read the open-ended questions in the NVivo 12® software with coding in three phases: open, axial, and selective. In open coding, we identified codes by relevance—related to the study topic and simultaneous creation of memos; in the axial, we grouped codes by meaning and created the analysis categories; in the selective, the codes grouped were read with greater abstraction, looking for correlations between the categories and the dimensions of the RE-AIM model.

Data analysis process.
We defined the units of analysis as sentences. We analyzed one question at a time to encode the information by dimension, according to the organization chosen for data collection. In the third and final step, corresponding to the treatment of the results, we made inferences in the materials with the help of nodes and codes created in the software. We contextualized the categories elaborated in the RE-AIM dimensions and discussed the findings.
Ethical Considerations
This study respected Resolution 466/12 of the National Health Council, with the participants agreeing on a Free and Informed Consent Term. We stored the data respecting the guidelines of Circular Letter No. 2021/CONEP/SECNS/MS. The Universidade Federal de Santa Catarina Research and Ethics Committee approved our study (approval no. 3.996.082). To refer to the participants we adopted the codes (P1, P2, P3 …)—with “P” referring to the participant, followed by the numeral according to the questionnaire carried out, and their professions—maintaining their anonymity.
Results
Twenty-nine health professionals and managers who work in health care services participated. In primary care, participants cover the four health districts of the municipality (North, Center, South, and Continent), with a sample of three health centers per district, totaling 12 participating units. In the hospital context, all workers who attended the inclusion criteria received an invitation.
We characterized the participants by the health care service in which they work, their technical training, and their current position (in this case, it is possible to accumulate more than one answer, e.g., nurse and manager), in addition to the time of experience with using Health Information Systems (Table 2).
Characterization of Participants About Workplace, Training, and Time Using Health Information Systems at Work.

During the data analysis, 16 main categories emerged from the participants’ reports. We formed and distributed these categories based on the five dimensions of the RE-AIM framework (Figure 2).

Distribution of analytical categories among RE-AIM dimensions.
Reach
The Impact of using Information Systems
An information system should reach all users—the professionals who handle the technology in their work process and the SUS users who benefit from the care provided—as the use impacts everyone to some extent. This 100% reach depends on the characteristics of the service (in primary care by population registered in the territory and hospitals by demand). In both cases, the technology must reach all the professionals who somehow participate in health care actions (directly or indirectly).
We are all impacted by the use of a health information system, professionals, and patients—the proportion of 100% of the Brazilian population. (P7—Nurse)
Limiting Factors
However, despite the consensus on needing to reach all SUS users, workers, and health service managers, the study participants identified factors that limit this impact from an individual point of view, mainly centered on insufficient infrastructure (technology, equipment) and difficulties with the systems handling and performance.
Limitation of physical space to install equipment (PCs and peripherals), limitation of the amount of equipment, lack of personal interest in acquiring new knowledge, discouragement by the use of many systems that are not integrated with each other. (P18—Hospital Manager)
Efficacy/Effectiveness
Performance and Work Process
An information system must facilitate the work process, providing agility and practicality, incorporating a friendly layout and easy access to the most critical information for care provision.
I expect an agile, easy to use, intuitive and simple system. This makes information about the appointments visually available. A system that it is not heavy, which means, that it runs easily on the internet, that it has stability, that it does not “fall” during use. (P17—Nurse)
Communication, Interoperability, and Care Coordination
Also, the professionals emphasized the need to communicate and exchange information between different professionals through integrating data from the other healthcare levels, enabling the development of better plans and acting as an instrument to carry out care coordination.
Integrated system, with all functionalities: records of outpatient clinics, hospitalization, imaging exams and analyses, requests for opinions, records of appointments and absences, medications in use, appointments. All performed at different levels of care and even in the private sector. (P22—Physician)
Management and Control of Indicators
The participants think that using a solid information system also helps to qualify the management process by providing reliable data and reports and, consequently, planning, evaluating internal processes, and reducing costs.
Generate reports, cross-reference data, monitor indicators, so that processes can be managed in an optimized way. Today, the system does not allow the generation of almost any report, it does not integrate information, it greatly limits the possibilities of managing various processes. (P8—Nurse)
Information Security
HIS must provide security, privacy, and protection of users’ personal information. Participants clarified that the data must reach specific professionals—according to their attributions and responsibilities—requiring different information access levels.
Enable access to health information only for health professionals and make available to other health workers (administrative, for example) only information necessary for registration and registration update. (P11—Nurse)
Quality of Care and Patient Safety
Finally, all these elements related to the effectiveness of Information Systems converge on the primary goal of improving the quality of care provided and ensuring patient safety.
We hope to improve and expand the assistance offered to SUS users with safety and quality, in addition to optimizing the work of health professionals and improving the resolution of health institutions in the SUS and implementing the electronic medical record for access to all levels of health care. (P9—Pharmacist)
Adoption
Qualification, Training, and Organizational Culture
The user’s level of knowledge about the technology is one of the factors that can interfere with Information Systems adoption, making evident the need for planning and offering qualifications and training by the institutions. In addition, organizational culture also needs work. It is crucial to expand the dialogue between workers and local managers and the involvement of users in choosing technology based on their daily needs.
What can prevent its use is the lack of training and/or unwillingness to use it, which can be mitigated with awareness-raising and professional updating activities. (P12—Nurse)
Finance and Infrastructure
The demand for financial resources to invest in the purchase and maintenance of systems and the guarantee of adequate infrastructure for their use are also determining factors for the technology adoption from the participants’ perspective.
The main factor that interferes with the adoption (by the health institution and its leaders) of an information system is the cost of installation, use and maintenance. All other questions are always secondary to the cost factor. (P27—Physician)
Users Involved
To ensure a process of conscious adoption of the technology, the participants point out that the ideal would be that all professionals—considering the restrictions on access by profile and information security—should participate in the process, whether directly or indirectly associated with health care provision.
All the professionals of the family health team (physicians, nurses, dentists, community health workers, administrative), (…) secondary and tertiary care professionals. (P19—Nurse)
Implementation
Financial Impact
The costs of implementing an HIS are among the most relevant topics when thinking about its acquisition and guaranteeing its quality and continuity of use. While they can become costly to the institution, cost-benefit analyses are essential. In the case of a technology considered adequate, it can generate financial results (in addition to assistance) in the long term.
A well-developed information system can act in a way that has an impact on reducing the institution’s costs. (P23—Nurse)
User Engagement
To implement a System, users should engage individually, associating this engagement with the organization’s culture. Also, a dialogic relationship with those responsible for the operational part and technology improvements is needed.
It is critical that teams are motivated to accept and contribute to change. Without the interest of the users of the system, the obstacles are potentiated and will certainly lead to low adherence to the new system. (P1—Pharmacist)
Operational Support
Health institutions must address the need for available and trained information technology teams during implementation.
Quick response from technology developers to system “bugs” and user feedback. Developers’ commitment to product maintenance, performing updates according to the needs of stakeholders. (P11—Nurse)
Maintenance
Maintenance and Support
One of the factors associated with long-term maintenance, use, and technology sustainability is related to the need for constant support for its use. It applies to the user’s learning and adaptation phase with the system, as in the daily work after implementation.
Lack of support for necessary adjustments based on the reality of each municipality. I believe that to be sustainable, the system must always be updated based on the reality experienced by the users of the system. (P29—Nurse)
Financial Sustainability
Human resources, infrastructure, purchase, and maintenance are different factors that converge to the need to spend financial resources to guarantee the satisfactory use of the System.
High maintenance cost. (P6—Physician)
Quality assurance
The technology must present the indicated effectiveness elements to guarantee health professionals’ adherence. A system that performs poorly or does not meet service needs may fall into disuse.
It can become sustainable in the long term when its contribution to the institution, to the work process and to the care offered overcomes the adversities and costs generated by its implementation. The continuity of any activity/action in health is given by the results it presented, the same can be applied to the Information Systems. (P12—Nurse)
Discussion
Reach and Effectiveness
We noted that participants were concerned about the reach the technology will have to SUS users and the possibility of the HIS being used by all professionals directly or indirectly involved in healthcare. However, aspects directly linked to the technology Adoption process can impact this scope, such as issues of infrastructure and user training, which highlights the necessary balance between the dimensions of the RE-AIM framework and their inseparable influence on each other (Holtrop et al., 2021).
When we think about Reach using the RE-AIM model, we consider the proportion of the target population and its representativeness since it seeks to reduce health disparities within the scope of these interventions (Almeida et al., 2013). In this sense, forming a network IS, developed locally and with the power to expand nationally, could help public health management processes reduce inequalities in the sector centered on patients and professionals who use technology (Marques et al., 2008).
Despite the growing demand for information and evidence, the HIS currently used in many countries does not suit their needs. According to the SCORE study (World Health Organization, 2020), integration with other sectors, private services, the overload of clicks and information to be filled in, and the need to use paper records are some of the quality indicators and difficulties identified at an international level and are like the findings evidenced in this research.
One of the participants’ quality indicators is associated with the product’s usability, which involves the ease of handling the system, a friendly interface, and an excellent human-computer experience. Despite the various usability concepts described in the literature, there is a consensus that this can be a decisive factor in the adherence and good use of the technology (Maia et al., 2020). The usability factor could lead to part of the guarantee of its sustainability in the institution as it can define whether the health professional uses its functions or not.
It is worth mentioning that, in Brazil and abroad, a series of technical norms discuss and give direction to this human-computer experience. They need to be considered both in developing and acquiring these technologies. Between 2008 and 2020, the Brazilian Association of Technical Standards linked more than 40 standards related to health informatics (Associação Brasileira de Normas Técnicas, 2022). Besides these regulations, there is the need to comply with the laws regarding information security, both the General Data Protection Law (LGPD) approved in 2018 and effective from 2020 (Bernardo et al., 2022) and those related to issues and ethics councils of each professional category involved in the care and access to users’ information.
A systematic review study that analyzed the implementation of Electronic Health Records from the perspective of the National Humanization Policy pointed out that the lack of training for the use of technology and the resistance of professionals in some cases can lead to the underutilization of their functions (Toledo et al., 2021). That could compromise the potential for Adoption—and, consequently, Reach—and for the Maintenance of these systems.
Shared care and the possibility of interprofessional communication emerged from the participants as central elements in guaranteeing the expected quality of an HIS. In the Brazilian Unified Health System, care coordination appears as one of the guidelines to be operationalized in primary health care, articulating attributes of communication, organization, and problem-solving capacity (Brasil. Ministério da Saúde, 2017). Thus, it is essential that when considering these technologies in different care settings, communication elements are organic to the analysis process for their incorporation.
Despite dealing with different regional work contexts and socioeconomic realities, a study in Rio de Janeiro showed that professionals consider the coordination of care an essential element for achieving comprehensive care. However, they point to the absence of integrated electronic medical record services that enable the exchange of information between primary care and other health services as a barrier in this process (Ribeiro & Cavalcanti, 2020), like the findings of this study. Nevertheless, interprofessional communication mediated by technology raises a greater depth necessary to overcome the mere “exchange of information” advancing care construction (Toledo et al. 2021).
Adoption, Implementation, and Maintenance
Based on these findings, it is necessary to highlight the crucial observance of issues related to interoperability between systems during the planning and evaluation processes of technology adoption. Interoperability is the characteristic that refers to the “ability of different systems and organizations to work together to ensure that people, organizations and computer systems interact to exchange information effectively and efficiently” (Brasil. Ministério do Planejamento, Orçamento e Gestão, 2012, p. 6). In Brazil, Ordinance No. 2073, August 31, 2011, regulates interoperability standards and health information for HIS in the three management spheres and private and supplementary health care (Brasil. Ministério da Saúde, 2011). However, the lack of a regulatory process to incorporate systems in a standardized way can interfere with acquiring technologies that respect the policies and regulations designed for SUS.
Another factor that directly influences both the Implementation and Maintenance of the use of technologies is their cost. A systematic review study with meta-analysis (Haried et al., 2017) identified that among the six topics most discussed by researchers in the HIS area, the triad cost, quality, and efficiency rank second in the debates, behind only studies that address issues related to care coordination.
Another systematic review (dedicated to studying the impact of these technologies from the point of view of healthcare quality and cost-effectiveness) identified that 60% of the analyzed articles that discussed this relationship reported a positive impact. In comparison, 16% reported a negative impact. However, according to the authors, despite being considered promising technologies in health, there still needs to be more evidence and discussion on this topic, requiring investment in new research in the area (Sadoughi et al., 2018). Factors associated with the costs of implementing technologies, such as the acquisition of equipment, software, investment in infrastructure, and training professionals, are often responsible for this imbalance between investment and return in the medium and long term (Snoswell et al., 2021).
The exercise of cost management in the Unified Health System is essential to guarantee the practical application of resources and, consequently, the SUS sustainability (Brasil. Ministério da Saúde, 2013). The participants showed concerns about these costs inherent to using HIS, which insert this topic as a transversal issue in the discussion, as it crosses the dimensions of Adoption, Implementation, and Maintenance, thus standing out as an agenda to be thought especially at organizational and systemic levels.
The fragmentation and variety of HIS and issues related to costs directly affect the quality of technology used by professionals. Excess clicks and the need to feed information in several systems appeared in this research as indicators of Efficacy/effectiveness. However, they also emerge as limiting factors in Adoption and decisive in the Maintenance of the use of functions. Adopting a nationally based IS, with data and information integration, could be a strategy from an economic and usability point of view.
However, the Brazilian context of using these nationally based systems could be more transparent, and it is not easy to measure the amount of these technologies available (Coelho Neto & Chioro, 2021). Recently, the e-SUS AB System appeared as a strategy that would include the elimination of rework in the recording of information through data integration with other systems in the country (Brasil. Ministério da Saúde, 2014). Its use seems promising in optimizing the primary health care work process (Araújo et al., 2019). Still, there are significant challenges in its planning and implementation process to overcome (Schönholzer et al., 2021).
Nevertheless, the government is encouraging the use of e-SUS mainly in primary health care, and it is necessary to expand this campaign to other levels of care. It is possible to verify in the National Guidelines for the Implementation of the e-SUS AB Strategy (Brasil. Ministério da Saúde, 2014) that municipalities that already use their systems for the organization and management of services (possibly one of the more than 600 registered within the country) should export data to the nationally based Information System. However, this export guarantees that management at the federal level will have up-to-date health information but does not address interoperability, communication between different services, and care coordination.
Thus, when discussing the evaluation and incorporation of Health Information Systems in the SUS, it is essential to consider its sustainability at a broader level. It is necessary to ensure that this scenario of indiscriminate supply of products associated with gaps in the regulatory process does not reduce the universal health care system to a marketing space, from developing and purchasing these technologies, with private interests overcoming the public interest.
Study limitations: The open-ended questionnaire was a strategy to facilitate participation considering the COVID-19 pandemic scenario. However, this is a potential study limitation since the questionnaire does not allow researchers to get in-depth information compared to other qualitative strategies such as interviews and focus groups. Also, we conducted this research in a specific setting, the City of Florianopolis, one of the Brazilian municipalities with the best indicators of Primary Health Care. Thus, it is not possible to consider the study results as generalizable. However, it is worth noting that structuring the data collection method with RE-AIM and RE-AIM QuEST allows the replication of the methodological strategy and data analysis under the same perspective of the dissemination and implementation science.
This qualitative research is part of a mixed-method study, and the future scope of the works includes developing and validating a framework for evaluating and incorporating Information Systems in the Brazilian Unified Health System. Also, future research should expand the investigation of this phenomenon of health information systems to learn more from the perspective of the patients/SUS users themselves.
Conclusions
Talking to health professionals from different backgrounds working in primary care and hospital settings, we observed the essential components that can make an HIS appropriate for incorporation and use in the Brazilian Unified Health System. The IS must be able to reach all users, considering the level of care—primary care, specialized clinics, or hospitals. Also, from a performance point of view, technology must reduce bureaucracy, be agile, have a friendly interface, require few clicks, generate relevant information and good management reports, and provide a safe environment for accessing and storing confidential information.
Another decisive factor for using this technology is its ability to communicate and interoperate with other health services, enabling the development of more effective care plans and coordination between health care settings. The organizations must invest in infrastructure, offer training to professionals, guarantee support, and constantly improve the technology.
The use of the RE-AIM theoretical-methodological framework, specific to the dissemination and implementation science, made it possible to identify that—during the planning, evaluation, and incorporation process of an IS—the indicators associated with the individual analysis dimensions are codependent with the organizational ones, which demands analysis of all aspects in an inseparable way. In general terms, the quality level of the technology and its handling conditions are crucial so that its features do not fall into disuse, allowing these technological acquisitions to become sustainable investments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partly financed by the Coordination for the Improvement of Higher Education Personnel - Brazil (CAPES) - Funding Code 001.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.