
Abstract
We conducted interviews with clinicians and staff involved in Veterans’ decisions about where to receive their health care to assess experiences with community care coordination and identify areas for improvement. Insufficient time and knowledge were cited as barriers to assisting Veterans in making decisions about whether to use community care resources. Concerns regarding quality of community care and lack of patient understanding on the implications of accessing community care also arose. Clinicians need to be able to help Veterans make informed choices about where to receive their health care and may require decision support that integrates their informational needs with their values and preferences, clarity on the referral process, and improved ways to measure and describe quality of care to Veterans. VA has recognized issues with community care and established new initiatives but the rollout is complex and ongoing.
Keywords
Introduction
Given the multiple health care systems in the United States, many patients have options for where to receive their care. Although Veterans have always had access to community care covered through their Veterans Health Administration (VHA) benefits, the 2018 Department of Veterans Affairs (VA) Maintaining Internal Systems and Strengthening Integrated Outside Networks (MISSION) Act (Government bill S.2372) allows for more Veterans to be eligible for and have more access to VHA-purchased health care provided by community clinicians (herein known as “community care,” as opposed to direct care provided by VHA at a VA facility) (US Department of Veterans Affairs, 2021). The MISSION Act emphasizes the importance of Veterans’ choice regarding where to receive care, and clinicians are presumed to be the source of information and discussion surrounding this choice. Questions remain as to how to best support clinicians and staff as they assist patients in decision-making about where to receive care, and simultaneously maintain high patient satisfaction and ensure Veterans receive the highest quality care.
The VHA Office of Community Care (OCC) stated the MISSION Act will consolidate, “VA’s community care programs into a new Veterans Community Care Program that will help to ensure Veterans choose VA by getting them the right care at the right time from the right provider” (US Department of Veterans Affairs, 2018). Indeed, the intent of the MISSION Act is to provide Veterans with more ways to access quality health care either within VA or through community clinicians via expansion of Veteran eligibility requirements and the community clinician network (US Department of Veterans Affairs, 2018). However, providing patients with more ways to access health care requires a significant amount of care coordination, a goal of the Office of Integrated Veteran Care (OIVC, formerly the Office of Community Care (OCC) during the time of this study). Care coordination is a cornerstone of high-quality patient-centered care, especially in patients with multiple and/or chronic conditions. These patients require input from multiple providers across institutions and this requires “deliberate organization, cooperation, and sharing of information,” as well as a robust infrastructure and planning process (Peterson et al., 2018). It is important to note that VA clinicians have reported challenges with care coordination, communication between systems, and reimbursement problems with the precursor to the MISSION Act, the CHOICE Act (Mattocks et al., 2017; Tsai et al., 2017).
It is crucial to assess clinician and staff beliefs about what information patients need, help clinicians understand the community care referral process, and determine what implications arise when patients choose community care. Given the process of community care referrals and coordination remains complicated, the aim of our study was to understand the process of community care coordination and to assess the experiences of VA entrants around helping patients make decisions about where to receive their care. We hoped to specifically answer the questions: What are existing determinants to clinicians and staff for helping Veterans make informed decisions? What are possible ways to improve the decision-making and care coordination processes for Veterans deciding whether or not they want to access community care?
New Contribution
Veterans have increasing choice of where to receive their health care since the Maintaining Internal Systems and Strengthening Integrated Outside Networks (MISSION) Act of 2018
Our qualitative interviews with clinicians and staff entrants show that there is a lack of knowledge about community care through VA, and that clinicians should be able to incorporate patients’ values and preferences
VA is poised to utilize existing and new resources to address needs of entrants to be able to deliver and better coordinate high-quality, patient-centered care
Methods
We conducted semi-structured interviews between February and October 2020 with clinicians (specialty care physicians, primary care physicians, mental health clinicians) from ten VA health care facilities across the U.S., and OCC staff from one VA facility (Table 1). We conducted interviews via phone or online video platforms, and they were all one-on-one except for one small group interview (4 participants). All participants completed the informed consent process using IRB-approved documents (VA Portland Health Care System/Oregon Health & Science University IRB#20861).
Self-Reported Participant Characteristics.

Sample
There were no exclusion criteria for clinicians and OCC staff (coordinators and managers). The only inclusion criterion for clinicians was they had to have experience with referring patients to community care. We used convenience sampling through 1) the VA Access Research Consortium who gave our contact information to potential participants, 2) direct emails to potential participants identified by entrants, and 3) specialty-specific VA listservs (US Department of Veterans Affairs, 2020). We oversampled for specialty care physicians since specialty care is the largest driver of referrals to community care (Mattocks et al., 2021b) and we stopped interviews after information power on our focused topic was satisfactory (Malterud et al., 2016).
Data Collection and Analysis
We used a semi-structured interview guide that focused on participants’ experiences with the MISSION Act, how they communicate with Veterans about care options, and suggestions to help coordinate decision-making and community care (Supplemental Appendix 1). The guide was developed among our multidisciplinary team consisting of nurse and physician scientists and social scientists. We used probing questions with participants to gain more information. Two social science investigators (SEG and ML), experienced in qualitative health services research, conducted the interviews and led analysis. Interviews lasting between 30 and 66 minutes were digitally recorded and transcribed verbatim for accuracy. SEG had worked on a prior study with one of the participants, but no others were known to the interviewers.
Our team utilized an integrated approach of deductive and inductive thematic analysis to interpret interview data. We began with deductive rapid analysis to develop an initial understanding of the interviews (Beebe, 2005). SEG and ML created transcript summaries, organized by domains based on the interview guide sections: Thoughts on MISSION Act, Information for patients, Quality of care, and Relationships/communication with providers. We reviewed transcripts and summaries again using a consensus process for inductive analysis to identify emergent themes that arose from the data. SEG and ML updated the study team co-authors (physician- and nurse-scientists experienced in qualitative research and study coordinators) on new findings and patterns regularly. We created matrices of transcript summaries to illustrate and organize qualitative findings and allow for further thematic analysis across domains and participants.
We then reviewed the literature to find a model that would help organize and analyze the data. We found the Development Model for Integrated Care (DMIC) as a useful framework (Minkman, 2012). The DMIC classifies 89 elements in 9 clusters: roles and tasks, patient-centeredness, delivery system, commitment, quality care, performance management, interprofessional teamwork, transparent entrepreneurship, and results-focused learning. We organized our findings based on the DMIC elements and categorized each theme in terms of the DMIC clusters. Given the roles and responses of our interviewees and the emergent themes, we provide results only on the first five clusters. Roles and tasks incorporates aspects of “agreements among care partners on tasks,” ensuring that all professionals are informed of what is happening with the patient and establishing a coordinator to assist in care coordination. Patient-centeredness includes, but is not limited to, providing understandable information to patients, being able to offer information from care partners in a collaborative way, and using a protocol for systematic follow-up of clients. Delivery system is an important cluster because it encompasses the use of a single health record by all clinicians involved in care, as well as offering case management for complex cases. Commitment focuses on collaboration in pursuit of a goal. Quality care focuses on the design of the pathway and use (or not) of evidence-based practices. These clusters will be highlighted in our results below.
In order to contextualize the findings, we present the referral process as described by our participants (Figure 1). First, participants reported that established patients usually discuss referrals with their primary care provider (PCP) or specialist, although new patients without a PCP may be referred automatically to the OCC. Community care coordinators (CCCs) reported the steps following referral are complex. Specifically, they described the administrative burden required for each step, including multiple nurse coordinators, case managers, and finance administrators involved depending on the individual case. They explained the process more simply as such: The CCCs determine eligibility and evaluate options for the patient. A CCC then calls the patient to schedule an appointment with a community clinician, and sometimes provides further information regarding available options. Next, the patient goes to the community clinician. Finally, the patient either continues with the community clinician, working with the OCC to streamline care, or they return to VA. The findings are organized around the flow of the community care referral process, allowing themes to emerge in sequential order (Figure 1).

Process of VA patient referral to VA-purchased care from community clinicians (i.e., “community care”).
Results
We interviewed 20 participants, with the plurality being specialty care physicians (38%). The majority self-reported White race (81%) and were from the Western part of the U.S. (71%) (Table 1). Half of the sample was male. While our interviews were conducted during the COVID-19 pandemic, our participants did not discuss the pandemic as a factor in community care coordination, except the community care coordinators (CCCs) who briefly mentioned a perceived increase in wait times for access to community care.
We found four main themes based on either the deductive use of interview guide domains or through emergent findings coupled with the DMIC framework as a guide: 1) clinicians’ lack knowledge of community care processes, 2) OCC process challenges, 3) quality of care concerns, and 4) problems with coordination and continuity of care. Additional illustrative quotes are in Table 2.
Illustrative Participant Quotes by Theme.
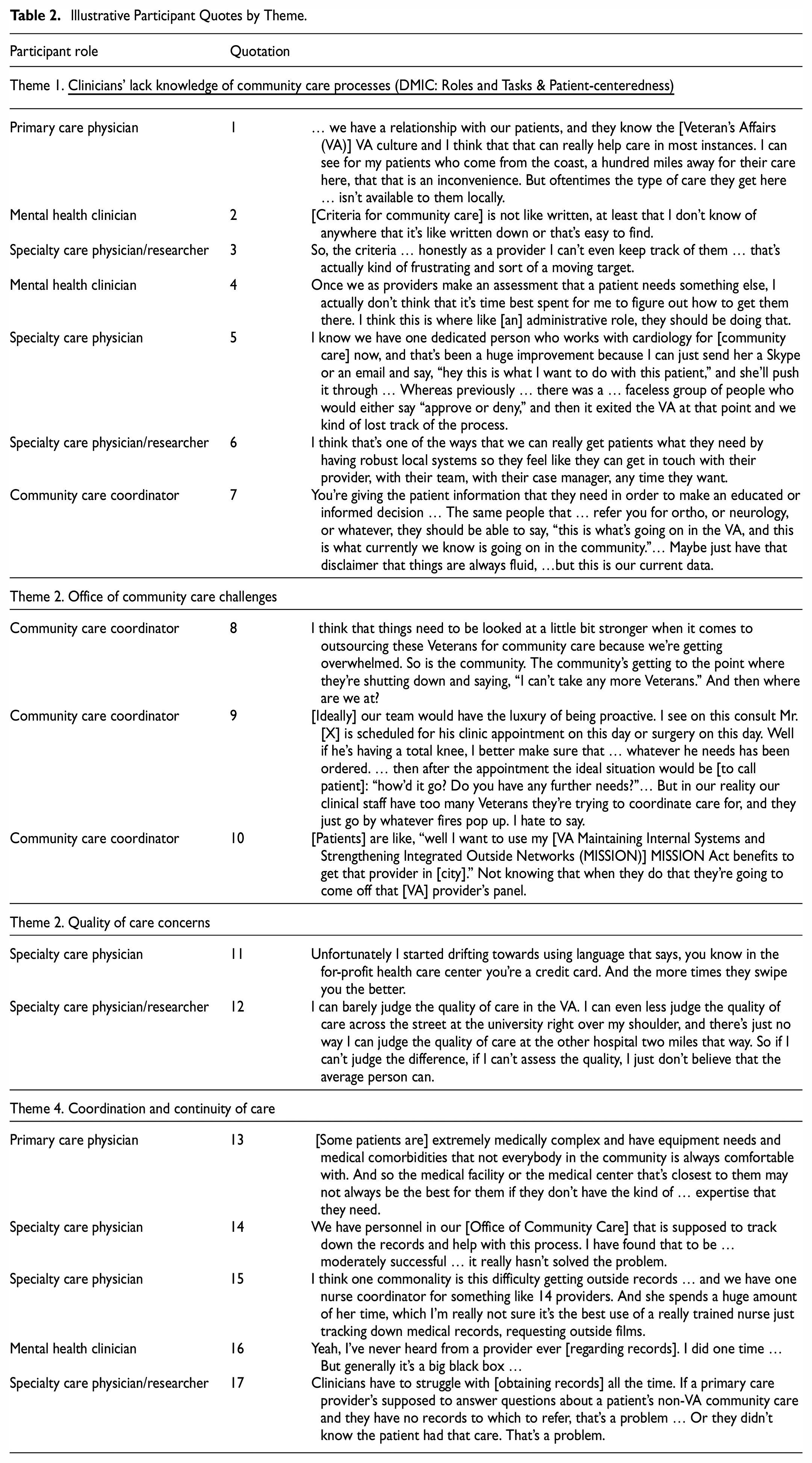
Clinicians’ lack knowledge of community care processes (DMIC: Roles and Tasks & Patient-centeredness)
All participants discussed that conversations with patients about where to receive care should start with eliciting the patients’ preferences and assessment of desire to stay within VA. Most clinicians reported the majority of their patients wanted to stay within VA. All participants endorsed that it is important to explain to patients the implications of choosing non-VA health care. Clinicians reported that when patients are referred for community care, most of the time it is not so much a “decision” as 1) VA lacks specific service options, or 2) patients select care closer to home for convenience, while maintaining other care within VA. However, some clinicians reported that “convenience is not always what’s best,” and additional factors should be discussed, such as continuity, quality of care, and Veteran-specific provisions like specialized mental health treatments or VA clinicians having more education and sensitivity about military culture (quotation 1).
When clinicians placed consults for patients to receive community care, many reported their role provides insufficient time or knowledge to help patients make informed decisions about their options. For example, it is difficult to keep track of criteria and understand the process for community care (quotations 2–3). As one mental health clinician stated about the difficulties of communicating about the process when they lack knowledge about it themselves:
[the community care process] feels like a black box. I make the referral … then some stuff is going to happen, and then eventually [the patient] will get an appointment maybe, but I never know.
Some clinicians said they inform patients that it might take longer to get care in the community compared to waiting for a VA appointment based on their experiences referring patients. A few clinicians and CCCs said they relate potential challenges with coordination and continuity of care outside of the VA. Almost all clinicians related that they did not have information regarding care quality, wait times, and implications of choosing community care and it would add to their already overburdened workload to try to find it.
Clinicians reported wanting a “high-touch” dedicated person who could “advocate and partner with the Veteran” to assist them through the community care referral process (quotations 4–5) and provide more patient-centered care. Clinicians reported that they were unsure as to the current scope of CCCs’ roles, and their role in communicating about community care. Participants as a whole expressed the desire for better and easier options for communication methods for patients who want to contact VA staff, more tailored knowledge for clinicians and patients about the roles and processes embedded within the referral process, and more tools to show patients the implications of choosing community care (quotations 6–7), such as a smart website or information within the electronic health record to aid in decision-making.
2. Office of Community Care Process Challenges (DMIC: Delivery system & Patient-centeredness)
After receiving a consult from the referring provider, the CCCs contact patients to discuss scheduling and ask if the patient has preferences for a specific clinician (Figure 1). The CCCs all reported feeling overwhelmed due to short staffing and complicated processes, and would like to have time to provide more proactive care for patients (quotations 8–9). Because of staffing shortages, patients can wait several months for a call from the CCC to coordinate non-critical care, a delay also noted by some clinicians.
All CCCs echoed clinicians that patients do not understand the implications of going outside VA for care (quotation 10) and described additional implications clinicians may not know. For instance, patients may be taken off the VA panel if they receive community primary care, prescriptions might be slower, care coordination is troublesome, or they might receive bills for services. One CCC noted that there are implications for clinicians too in that they are “still liable for all” of the patient’s care until they are seen in the community, meaning prescriptions and follow-ups are still the VA clinicians’ responsibility.
Wait times are often shorter to see a VA clinician, but patients may assume the community will be faster and opt for a community referral. Clinicians felt information about wait times was not accurately provided to patients to help them make informed decisions. Some suggestions were to have easier ways for Veterans to contact VA staff with questions about community care and providing easily accessible information about current wait times.
3. Quality of care concerns (DMIC: Quality care)
The reason for staying with VA was generally perceived to be because VA “has all that Veteran expertise in-house.” Participants reported that VA clinicians tend to be more sensitive to Veteran-specific needs and behaviors, for example, treatment for post-traumatic stress disorder. Every participant suggested that VA could improve promoting information about the high quality of VA health care through billboards, advertising campaigns, or through interpersonal channels within OCC. As one specialty care physician said:
We really do provide outstanding care and the wait times are pretty good and people really care about Veterans’ health … And I would say that the care in the community, that the responses that I hear, is a little more variable.
Clinicians considered quality of care very important when referring patients to community care. Specialists, as opposed to PCP’s who routinely refer patients to the community for specific procedures not offered at VA, reported having relationships with high-quality clinicians at their academic affiliates who they could recommend to patients. However, when patients asked for referrals closer to their home, specialists were often unaware and unable to offer a specific recommendation based on quality. Clinicians who did not have relationships with non-VA clinicians reported having difficulty providing recommendations. Many participants expressed concern over the quality of community health care. For example, one PCP said:
I think one thing that makes me nervous is how well are we vetting the doctors and other folks that we’re sending our Veterans to.
All participants acknowledged the challenges involved with assessing and comparing quality given the interpretive nature of quality, as well as the lack of usable and appropriate metrics (quotations 11–12).
4. Problems with coordination and continuity of care (DMIC: Delivery system & Commitment)
All participants discussed the importance of high-quality coordination and continuity of care for patient outcomes. Many also reported that continuity of care is especially hard to facilitate appropriately when people are going in and out of VA for different specialties or procedures, and the difficulties are compounded for patients with complex care needs. The PCPs all agreed that complex situations are best managed within one system to prevent lags in care between submitting a community care consult and scheduling the visit, as well as coordination challenges between community and VA clinicians (quotation 13). One PCP said:
I know that our [division chief], one of his ideas, is [to encourage patients with less complex needs] to go to the community when they qualify. Because that allows us to see these more complex patients that really need very good coordinated care.
Every participant expressed difficulties in obtaining medical records from community clinicians (quotation 14–17). One specialist reported what all echoed: “[getting records is] the hardest thing for us in dealing with the downstream implications of the MISSION Act.” Many reported hearing similar complaints from patients. Occasionally VA staff are able to track down records, but many times it falls to the clinicians to acquire the records and this equates to a “poor transfer of information.” The time and effort required to request and obtain records was seen as an immense burden.
Several clinicians indicated the desire for a dedicated person to handle records requests, and a few wondered if that was, or could be, the job of someone in the OCC.
Discussion
First, our findings suggest clinicians’ experiences with community care left them feeling ill-equipped to help patients make decisions or give recommendations about care options in the community, largely because they do not have the knowledge, time, or resources to provide guidance. Second, we learned the Office of Community Care referral process is complex, and it might be helpful for clinicians and patients to have more access to information about the process. Third, we found that VA employees are concerned about the quality of care outside of the VA; however, there were mixed opinions on how to measure care in a way that patients and clinicians can understand and discuss. Lastly, we found that coordination and continuity of care are highly important aspects of care but are hard to manage when patients use community health care. There was the perception that patients do not fully appreciate or understand the implications, like losing their VA PCP or burden of sharing records that can intensify the care coordination efforts needed, when they use community health care.
The DMIC notes that patient-centeredness involves provision of understandable information to the patient, flexible adjustments for integrated care, and protocols for systematic follow-ups. These are all elements that our participants reported as being areas for improvement since clinicians and staff are unable to provide needed information and follow-up for patients referred to community care due to time and knowledge constraints. Clinician time and knowledge were also limitations during the precursor to MISSION known as CHOICE (Stroupe et al., 2019). In response to identified problem areas with community care referrals, policymakers have created the VA Referral Coordination Initiative (RCI), which aims to better position staff to provide information and discuss preferences to guide Veterans through this process. However, the rollout of the RCI is complex and ongoing (Veterans Health Administration, 2021). Alternatively, VA could streamline certain necessary care to be automatically referred to the community while focusing on the services VA does exceptionally well, leaving the choice largely out of patient and clinician hands. Indeed, within a delivery system as complex as VA community care, there needs to be agreements on standardized processes between all interested parties on how patients move through the system and how they are managed with connections to electronic databases (Minkman, 2012). To develop a successful delivery system for community care VA could use a user-centered design approach for development (Still & Crane, 2017).
Confusion about the process in general matches with the DMIC, which states there is “need for clarity about one another’s experience, roles, and tasks in the care chain” (Minkman 2012). Participants reported it would be helpful to have more information about the community care referral process, such as who is responsible for which tasks, phone numbers for questions, or information about VA wait times. For instance, patients may not know that VA wait times have improved in recent years and are often shorter than in community settings (Penn et al., 2019). Participants in our study recommended more access and training to increase knowledge about the community care referral process. Our results indicate need for improvement within OCC processes, including more knowledge of referral processes to increase patient-centeredness. The RCI addresses training and knowledge by aiming to improve understanding of the community care referral process and to redirect personnel and training available for referral coordination. The DMIC points to the importance of integrating care specific to a patient, meaning having tailored conversations with patients that can provide all of the required information while also incorporating values and preferences. Currently it is unknown how or if the RCI addresses all components of patient-centered care and decision-making.
While there is evidence that VA health care in general is often as good or better-quality care than care in the community on most measures, including patient experience, our participants, and others, felt this information may not be fully accessible to Veterans (Anhang Price et al., 2018; Medicare.gov, n.d.; Miller et al., 2021; Vanneman et al., 2020). How best to make this information more accessible to patients, or even how to measure it, remains challenging (Hayford & Maeda, 2007; Mattocks et al., 2021a). Further, participants in our study felt that currently available quality metrics would not help most patients since they are difficult to measure and interpret, and may not be available for all non-VA or VA clinicians. Patients have preferences that go beyond quality metrics, including valuing relationships with clinicians (Lafferty et al., 2023). That being said, policy makers may be interested in vetting the quality of care of community providers and/or developing a sort of “preferred provider” network to provide more guidance for patients, fitting with the DMIC recommendations to create a multidisciplinary care pathway where all parties are in agreement about the goal, while always incorporating the patients’ needs and preferences.
Patients, including Veterans, in this and previous studies have expressed frustration at lack of communication between health care institutions leading to poor continuity of care (Mattocks et al., 2018; Miller et al., 2021; Noël et al., 2020; Lafferty et al., 2023). Needs assessments among all parties involved in the care chain could be helpful in making improvements, as well as ensuring goals are agreed upon, collaboration is encouraged, and awareness of the care chain (Minkman, 2012). VA may also need to update its data sharing systems and contracts to more efficiently and securely share medical records, especially as this is emphasized within the DMIC.
There are limitations of this study. Since the OCC participants were from one location, clinicians were from VA facilities affiliated with academic hospitals, this study is not generalizable, however qualitative research is generally not meant to be generalizable to all settings. There was a wide variety of specialties and referral types, therefore our results may not capture the full range of experiences across primary, specialty, and mental health care. We did not interview clinicians or staff providing community care, or Veterans for this manuscript. Veteran perspectives included herein are perceived by participants not accounting for their own biases about community care. We conducted subsequent interviews with Veterans about this topic (Lafferty et al., 2023). This study may suffer from selection bias in that those who participated may have felt very strongly about the MISSION Act, either positively or negatively. This study also suffers from moderator acceptance and recall biases.
Conclusion
Former Secretary of Veterans Affairs, Wilkie (2019), stated that Congress passed the VA MISSION Act to provide Veterans with more choices to access their health care, “based on what matters most: the convenience of (our) Veteran customers”. However, our participants suggested convenience was only one of many factors that patients must consider when choosing where to receive health care. As expected, the process is complex, but our participants suggested solutions including decision support that incorporates Veteran and clinician information needs surrounding the community care referral process along with Veteran values and preferences. clarity on the referral process, and improved ways to measure and describe quality of care. VA has recognized issues with community care and established new initiatives but concerns regarding patient care and interested party satisfaction remain.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440231204666 – Supplemental material for A Qualitative Study of VA Entrants’ Experiences Discussing Community Care With Veterans
Supplemental material, sj-docx-1-sgo-10.1177_21582440231204666 for A Qualitative Study of VA Entrants’ Experiences Discussing Community Care With Veterans by Sara E. Golden, Megan Lafferty, Anna Tyzik, Diana Govier, Jennifer Barton, Alan R. Teo, Samuel T. Edwards, Sarah S. Ono, Denise M. Hynes and Christopher G. Slatore in SAGE Open
Footnotes
Acknowledgements
We greatly appreciate the time and effort contributed by our partners at the Veteran Access Research Consortium, Office of Reporting, Analytics, Performance, Improvement, and Deployment, and the VAPORHCS Veterans Engagement Group.
Authorship Statement
All authors have made substantial contributions to the 1) conception and design, acquisition of data, or analysis and interpretation of data; 2) have contributed to drafting the article for important intellectual content; and 3) have provided final approval of the version to be published. Sara Golden takes responsibility for the content of the manuscript, including data and analysis.
Contributors
The Department of Veterans Affairs did not have a role in the conduct of the study, in the collection, management, analysis, interpretation of data, or in the preparation of the manuscript. The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs or the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided in part by an award to Drs. Slatore and Hynes from VA HSRD 19-481. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. It was also supported by resources from the VA Portland Health Care System, Portland, OR.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.