
Abstract
Pay for Quality (P4Q) concepts are discussed as solution for ensuring quality in health care in the context of budgetary concerns. However, little is known regarding the application to and effectiveness for complex chronic treatments. This article describes the incentivization approach taken in Germany, where complex codes requiring specific quality criteria were implemented into the Diagnosis Related Groups (DRGs) system. Using two examples (early complex geriatric rehabilitation, multimodal rheumatological complex treatment), we analyze the quality indicators according to the Donabedian Model and contrast the effects regarding compensation to traditional treatments. In total, the approach allows taking into account treatment and financial requirements.
Introduction
Quality is one of the pillars of and aims in health care, but health care quality may be limited (Nunes et al., 2017) and even endangered by budgets (Barber et al., 2017). Ensuring guideline- and quality-oriented treatment geared to specific patient needs is therefore globally becoming the focus of policymakers in health care (Organisation for Economic Co-operation and Development [OECD], 2018; World Health Organization, 2016). More attention is also called for the needs of patients with complex conditions to ensure that combinations of treatments are possible and adequately compensated for.
One of the leverage points discussed is Pay for Quality (P4Q), also known as Pay for Performance (P4P). P4Q programs are designed to provide financial incentives to health service providers if these follow established guidelines. However, little is known about the effectiveness of P4Q in general (Scott et al., 2011) and even less regarding treatments of (multiple) chronic conditions (Millett et al., 2009). Moreover, research has focused on outcomes, which makes it difficult to apply to more complex issues like chronicity.
In Germany, P4Q in chronic care has therefore been intensively linked to structural and procedural quality criteria. These are expected to improve the outcomes but result in higher costs than standard treatments. This is why the incentivization is safeguarded by feeding in real-world cost data from reference hospitals. The system was created in 2007 and is continually updated.
This essay analyses the quality indicators of selected complex, interdisciplinary treatments in chronic care plus reports about their effects regarding compensations in contrast to traditional treatments.
Background
Quality in Health Care
For assessing quality in health care, the Donabedian Model is used internationally to differentiate and describe key indicators in three categories, the so-called quality triad: structure, process, and outcomes (Donabedian, 1986). Donabedian assumes that there is a causal relationship between the three indicators. Structural conditions affect the process of service provision, which in turn may influence treatment outcomes (Donabedian, 1988a).
Structure quality in health care includes the material and human resources necessary for the provision of services. Material resources are infrastructure and technical equipment. Human resources indicators specify staff skills, know-how, qualifications, and motivation (Donabedian, 1988a). Process quality refers to all actions of the medical, nursing, and therapeutic staff, and highlights the way in which services are provided (Donabedian, 1988b). Outcome quality indicators concern current and future changes in the patient’s state of health due to successful medical and administrative actions.
Complex Treatment
Complex treatment is an interdisciplinary, holistic therapy, by means of which the treatment team attempts to restore the functional ability of a patient. The primary objective is the restoration of quality of life and independence when performing everyday tasks.
Remuneration and Incentivization for Complex Treatments
Complex treatments are supposed to result in higher quality, but require more resources and are thus more costly than traditional ones. Therefore hospitals need higher remunerations to make the provision possible and attractive. In 2007, Germany introduced codes for complex treatments in the Diagnosis Related Groups (DRGs) system, a classification of similar cases based on the diagnosis used to specify required treatments and subsequent hospital remuneration. The major diagnostic categories (MDCs) subsequently classify the DRGs by organ systems or causes. MDC 01, for example, stands for Diseases and Disorders of the Nervous System. In the German Operations- and Procedures- Key (OPS) systematization, the details for each treatment are stated.
The Institute for the Hospital Remuneration System (InEK) in Germany is responsible for determining the values for each specific DRG based on cost data annually submitted by reference hospitals. An average total cost for each DRG is calculated and used as basis for assessing the cost weight of each. In 2017, cost weights were calculated using the following formula:
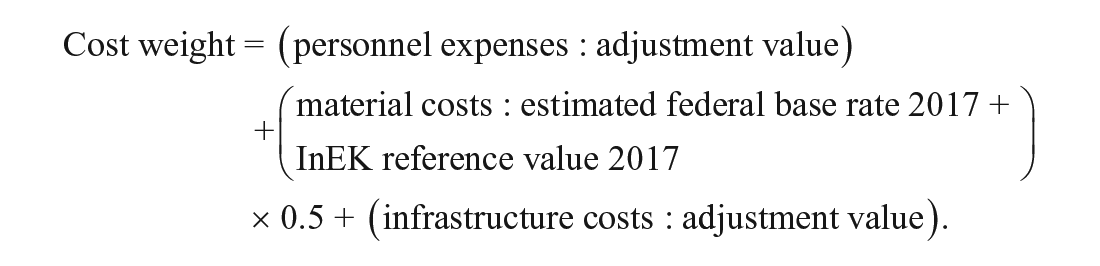
The adjustment value is a monetary value determined by the InEK that refers to the material cost adjustment to calculate cost weights of personnel and infrastructure. The federal base rate is an amount used to calculate a DRG. It forms the basis for the remuneration of hospital services, since the cost weight of a DRG determines the DRG revenue. The average value of a cost weight is 1.0. Thus, a patient case which has a higher cost weight than 1.0 according to its DRG classification is more costly compared to the average. To make the provision of complex treatments feasible, these need to be adequately paid for.
Several other countries also experiment with adaptations in the DRG system to allow for better care for chronically ill patients, for example, Italy. In 2012, a test of an innovative organizational model for chronic care (called Chronic Related Groups) was started in the Lombardy Region. In this model, the health care providers must in advance state a quota of necessary resources and then ensure continuity of care to chronically ill patients by providing, with the predefined quota, all outpatient services required for good clinical management (e.g., outpatient consultations, therapy, home hospitalization, prosthetics). A total of 207 primary care physicians and 22,500 patients with chronic illnesses were enrolled to pilot test the model in Bergamo (Italy) (Sorlini et al., 2012), which is now continued with a focus on telemedicine (https://www.interregeurope.eu/policylearning/good-practices/item/1303/good-morning-creg-chronic-related-group/). In Germany, the main focus is on remuneration and quality criteria for complex treatments.
Analysis
We use the Donabedian quality indicators to analyze the additional actions required in complex treatments as outlined in the OPS. We show the cost weights for selected indications with and without complex treatments using the example of early complex geriatric rehabilitation and multimodal rheumatological complex treatment.
Early Complex Geriatric Rehabilitation (OPS 8-550)
Early complex geriatric rehabilitation therapy targets multimorbid patients with multiple chronic conditions, in which motor and cognitive functions are often significantly impaired. When the need for an inpatient treatment is assessed, limited or missing communication skills, lack of outpatient services, or cognitive difficulties are essential indications for which treatments can and should be chosen.
Outcome quality
Once the need for acute geriatric treatment is clear, the treatment team defines a treatment plan taking into account the physical and psychosocial needs and abilities of the patient. Emotions can be assessed using the geriatric depression scale (Sheikh & Yesavage, 1986), cognitive skills through the mini–mental state test (Folstein et al., 1975), and mobility, for example, with the Tinetti test (Tinetti, 1986). Standardized geriatric assessment has to cover at least four areas, and an assessment of the present social situation at least five areas: social environment, living environment, indoor/outdoor activities, need for nursing/aids, and legal injunctions. Then, objectives are stated and (at least) evaluated at discharge. In addition, an outcome indicator testing the self-care skills of a patient has to be assessed, for example, using the Barthel index (Mahoney & Barthel, 1965).
Structure quality
The chief physician leads the team and has the final responsibility. Team members must meet certain minimum standards in terms of professional qualification and experience (see Table 1: structure quality). Regarding professions, all the following have to be available at the hospital and can be part of the team: physiotherapists, occupational therapists, speech therapists, oral/maxillofacial specialists, and psychologists/neuropsychologist. This emphasis on the interdisciplinary nature of the treatment makes it clear that the focus of OPS 8-550 is on structure and mainly staff.
Geriatric Early-Stage Complex Treatment.

Process quality
To ensure procedural quality, the number and type of treatment sessions as stated in the OPS have to be covered during a (minimum) 14-day inpatient stay and documented (Table 1: process quality). The OPS may only be coded during the time the patient is in need of acute inpatient treatment. Moreover, the entire interdisciplinary team has to meet once a week, document the meeting and actions between meetings regarding professional groups, retrospective outcomes, and prospective goals when required.
Figures 1–5 show examples of financial implications of the OPS, taking into account the requirements on the structure, process, and outcome quality. The illustrations also demonstrate the importance of the assignment to an MDC. The figures present the cost weights: the left side regarding the conventional DRG without a complex treatment, the right side those for a complex treatment (Institute for the Hospital Remuneration System).

Geriatric DRGs without and with complex treatment.

Geriatric DRGs without and with complex treatment.

Geriatric DRGs without and with complex treatment.

Geriatric DRGs without and with complex treatment.
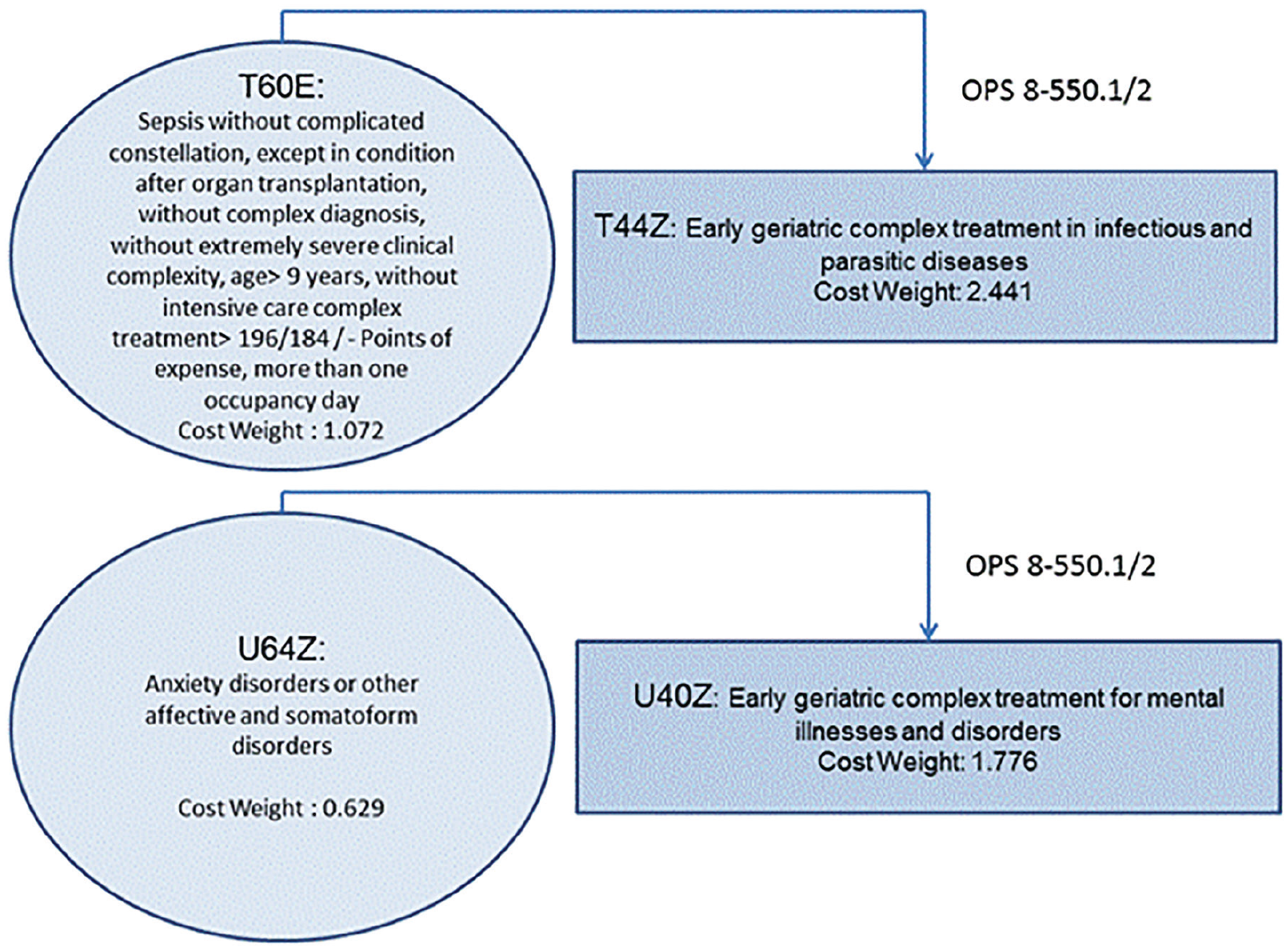
Geriatric DRGs without and with complex treatment.
For example, the treatment of a geriatric patient with heart failure is reimbursed with a cost weight (CW) of 2.052. For a federal state base rate of €3.400 (the federal state base rate is a uniform national rate for hospital services), this means a remuneration of approx. €7.000 (corresponds to DRG F48Z) for the treatment. If OPS 8-550 with a rating of 0.849 (corresponds to DRG F62C) is not applied, the remuneration would be approx. €2.900 (Figure 2). Figure 4 shows the example of a pelvis and femoral neck fracture. If the hospital does not apply OPS 8-550, it charges for DRG I66F; the revenue is approx. €2.950 for a CW of 0.868. If it applies OPS 8-550 and charges for DRG I41Z, it receives approx. €6.500 for a CW of €1.909.
Multimodal Rheumatological Complex Treatment (OPS 8-983)
Multimodal rheumatological complex treatment is for patients suffering from rheumatic pain with increased disease activity who cannot be treated adequately on an outpatient basis.
Outcome quality
Assessments in this OPS cover a range of aspects.
Disease activity is measured using the Disease Activity Score (DAS) at the beginning and at the end of the treatment (Table 2: process quality, outcome quality).
Multimodal Rheumatoid Complex Treatment.

The DAS in the current version 28 covers swelling and tenderness of the 28 relevant joints (metacarpophalangeal [MCP] and proximal interphalangeal [PIP] joints, thumb interphalangeal [IP] joints, wrist, elbow, shoulder and knee joints), the erythrocyte sedimentation rate, and patient assessment of his or her current state of health using VAS (visual analog scale). The DAS 28 value can be between 0 and 10 (Fransen & Van Riel, 2009), with zero for a complete lack of disease activity and 10 for the greatest disease activity.
OPS 8-983 also specifies assessment tools for certain impairments, for example, the Bath Ankylosing Spondylitis Functional Index (BASFI) as the tool for assessing the degree of functional limitations in patients with ankylosing spondylitis (van Echteld et al., 2006).
Regarding functional restrictions, the patient has to answer 18 questions on everyday activities. The degree of disability is assessed based on the answers (Raspe et al., 1990).
Pain progression should also be measured, by means of the VAS or the Numeric Rating Scale (NSR). The patient indicates a number between 0 and 10, where 0 means “no pain” and 10 means “unbearable pain” (Ferraz et al., 1990).
Structure quality
The treatment team is led by a doctor of internal medicine specialized in rheumatology, a specialist in orthopedics and trauma surgery who has also been trained in orthopedic rheumatology, or a doctor of orthopedics specialized in rheumatology. The hospital must still provide qualified staff in at least three of the following areas: physiotherapy/physical therapy, occupational therapy, pain therapy, cognitive behavioral therapy, and person-centered psychotherapy (Table 2: structural quality). Three of these areas must be used for the specific indication (Table 2: process quality).
Process quality
The treatment team has to ensure that pain therapy, physiotherapy, or physical therapy begins immediately (Table 2: process quality). Failure to do so or to provide less than 11 hrs of treatment per week equals not fulfilling the OPS requirements and results in not receiving extra remuneration.
Service providers can apply the OPS revenue code only starting from a minimum of 14 days of acute inpatient treatment. In the figure below, we show the financial implications of being in a position to apply the code for complex treatment or not by using examples of rheumatological treatments.
For example, if a patient is treated for rheumatoid arthritis without complex treatment, the cost weight amounts to 0.714, which corresponds to approx. €2.430. If complex treatment can be claimed, the cost weight is 1.493, which corresponds to a revenue of €5.080. Treatment of fibromyalgia yields a cost weight of 0.872 (corresponds to €2.970). With complex treatment, the cost weight is 1.493 (€5.080; Figure 6).

Rheumatologically treatment without and with complex treatment.
Concluding Remarks
Ensuring and adequately remunerating treatment quality for patients with chronic multiple conditions via P4Q approaches is the focus of this article. In Germany, this is done by complex codes that are elements of the DRG system. These codes include specifications regarding structural-, procedural-, and outcome-related requirements.
Effects of Complex Chronic Treatments
As could be shown, these requirements are closely related and thought to positively influence the outcomes for chronically ill patients with complex symptoms. P4Q can thus have positive effects on the design of processes (Rosenthal et al., 2016; Yang et al., 2016). Moreover, stating process and timeframe requirements of complex treatments can improve the structure of hospital processes and interface management, which has so far been rather neglected (Shaw et al., 2010).
However, evaluating structures in isolation cannot provide information on the quality of treatment processes and outcomes (Shaw et al., 2010). Moreover, process criteria give no indication whether a patient’s health will actually improve (Sorian, 2006). Thus, a combined perspective is called for and needs to be investigated. Studies on patient satisfaction support the notion of improved outcomes due to complex treatments (Romeyke et al., 2017). Still, research on the effectiveness of complex treatments is limited, especially considering quality criteria, and concerning behavioral (adherence) aspects.
Effectiveness of Complex Chronic Treatments
A meta-analysis demonstrates that a treatment that has been designed specifically for geriatric patients, as opposed to conventional treatment, may reduce the likelihood of admission to a nursing home (Bachmann et al., 2010). However, another meta-analysis draws attention to the need for further research on acute geriatric early rehabilitation (Buecking et al., 2013) so that interventions and their consequences are best possibly understood and used.
A study on the efficacy of complex rheumatological treatment that included several years of documentation on the state of health of a patient with fibromyalgia describes positive results with regard to pain and mental health, which could still be observed 18 months later (Romeyke et al., 2018). A randomized study of 130 patients also demonstrated that rheumatological complex treatment reduces pain and depression (Romeyke & Stummer, 2014).
Requirements of Complex Chronic Treatments
The interdisciplinary orientation of all treatments investigated here sets special requirements for the team structure and team processes. In addition to professional qualifications, good interpersonal relationships between service providers (Heinemann, 2002) based on good interprofessional communication are needed. The therapeutic plan and evidence-based assessments serve as guides. The implementation of complex treatments can be simplified by developing procedure-based clinical pathways (Romeyke & Stummer, 2012), which also improve procedures.
It is important that service providers or their representatives are involved not only via cost-referencing hospitals but also in the development and design of complex treatments. This can significantly increase the acceptance of the tool. In Germany, this process involves professional medical associations, which formulate the contents of complex treatments each year, based on an analysis of evidence-related therapeutic measures. Professional medical associations should, therefore, continue to interpret the codes. This is also vital to avoid patient-related adverse effects of P4Q (Chang et al., 2012) due to ambiguity regarding remuneration (Romeyke & Stummer, 2012). The potential payer-related adverse effect is falsifying patient documentation (Allen et al., 2014) to obtain financial benefits. Guarding against this is ensured by case supervision and review by the Medical Review Board of the Statutory Health Insurance Funds (MDK, Medizinischer Dienst der Krankenversicherung).
Overall, the analysis of P4Q in the context of chronic complex treatments suggests that combining
medical, nursing, and therapeutic expertise with
binding structures,
specified processes, and
tools for evaluating results in the sense of Donabedian allows
(a) taking into account not only the individual requirements of chronically ill patients but also (b) adequately remunerates service providers.
Footnotes
Acknowledgements
The authors would like to thank the anonymous reviewers for reviewing the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.