
Abstract
In comparison to a singleton birth, pregnancy, delivery, and child rearing in families with multiples is more complicated and is associated with more difficulties. This study sheds light on how parenting support hubs all over Japan recognize the difficulties of families with multiples, and how they support them. A questionnaire was distributed to regional parenting support hubs in Japan. The questionnaire coverage included rural to urban areas in all parts of Japan. The questionnaire was presented and answered using Google Forms, a website, a fax, or an e-mail attachment (n = 522). A factor analysis and t-tests were used to analyze the data. Regional parenting support hubs recognized that families with multiples have more difficulties and needs that require support than those with singletons, during both pregnancy and child rearing. However, they did not recognize any marked economic difficulties, which has been demonstrated to be an issue that affects families with multiples. Most regional parenting support hubs did not provide helpful support regarding speaking to parents of multiples, holding social events, or cooperating with other support groups, or rearing support hubs. When the helpful support measures that are recognized by parenting support hubs during the pregnancy/delivery period and the child-rearing period for families with multiple children are in comparison, such parenting support hubs recognized that families with multiples require more support during the pregnancy/delivery period. Parenting support hubs required information on the difficulties in supporting families with multiples and also required guidance on how such support should be provided. Parenting support hubs that cooperated with other hubs gave more support than those that did not. To link the recognition of the difficulties and needs of families with multiples to concrete measures, sufficient information on what is needed and how to support families with multiples should be provided. When presenting information on child rearing support for families with multiples, the importance of support during the child-rearing period should receive more attention. We found that cooperation is an important factor for enhancing parenting support.
Keywords
Background
The birth rate of multiple-child pregnancies and deliveries of multiples grew in the latter half of the 1980s and peaked in the last 20 years. This occurred because due to the increased use of fertility treatment and changes of treatment methods. In comparison to a single baby, pregnancy, delivery, and rearing of multiples is more complicated and is associated with greater difficulties. During the antenatal period, there are a number of differences between mothers of singletons and mothers of multiples. For example, in comparison to a singleton birth, the optimal antenatal period before delivery is a few weeks shorter in multiple births, and the fundal height of mothers of multiples is higher than that of mothers of singletons. Furthermore, the risks of gestational toxicosis are higher for mothers of multiples, and for these reasons, psychologically, more mothers of multiples feel unhappy and anxious in comparison to mothers of singletons (Wenze et al., 2015). Mothers of multiples thus face significant physical and psychological burdens.
In the case of multiple births, there are also difficulties during and after delivery. The mean birth weight of multiple is approximately 2,500 g, which is lower than that of a singleton (approximately 3,000 g), and approximately 95% of multiples are low-birth-weight babies. They tend to not feed at the breast well, and mothers regard them as difficult to rear (Taubman-Ben-Ari et al., 2010). Multiple-birthed babies sometimes have a history of admission to the neonatal intensive-care unit, which can affect the mother-infant relationship (Bolch et al., 2012). Mothers of twins had significantly lower sensitivity and were more unresponsive than mothers of singletons (Riva Crugnola et al., 2020). Twin infants were reported to have significantly more difficult and compliant behaviors than singleton infants (Riva Crugnola et al., 2020; Squarza et al., 2020). Furthermore, the risk of disorders, such as brain paralysis and developmental disorder, are higher for multiples than for singletons.
Multiples constitute a heavy burden on their family. Economically, multiple births increase the financial needs of families. Mothers of multiples were found to be paid less than other mothers (Glazebrook et al., 2004), and the cost of raising multiples is naturally higher than that of raising a singleton (Andrade et al., 2014). The economic burden of families with multiples is therefore greater than that of families with singletons. Physically, multiple-birth mothers struggle with muscle loss (especially after hospitalization), back pain, and insufficient sleep because they must rear multiple babies at the same time. Psychologically, mothers of multiples feel more anxious, and are more depressive than mothers of singletons, and their well-being is adversely affected (Andrade et al., 2014; Baor & Soskolne, 2012; Choi et al., 2009; Ellison & Hall, 2003; Lutz et al., 2012; Sheard et al., 2007). They feel that the postpartum period as stressful, overwhelming, and exhausting (Wenze et al., 2020). These factors are reported to persist at 9 months postpartum (Choi et al., 2009), and 1 year after birth (Vilska et al., 2009).
Multiples are also at a greater risk of abuse than singletons. In Japan, a nationwide survey on child abuse revealed that 10% of victims were products of multiple birth (Tanimura et al., 1990). Among twins, one twin was more likely to be abused than both; it has been suggested that, in twins, the difference in development or in their response to parents increases the stress of child-rearing and encourages favoritism, resulting in the abuse of only one of the twins rather than both. Thus, the pregnancy, delivery, and nurture of multiples are associated with greater economic, physical, and psychological burdens in comparison to singletons.
For the above reasons, it is helpful to provide parenting support to families with multiples (Kehoe et al., 2016). The level of satisfaction with social support only showed a positive association with parenting stress in the mothers of twins, and not in the mothers of singletons (De Roose et al., 2018). Thus, the provision of social support by medical institutions is suggested to be important. In the puerperium period, nursing care in the context of the home increased safety and self-confidence among mothers, and such care was shown to be particularly relevant for mothers of multiples (Andrade et al., 2014). It is found that information support functioned as a protective factor for families with multiples with high stress levels (Lutz et al., 2012), which families with multiples tend to have. In the pediatric setting, it is suggested that greater attention is needed to address maternal depression in families with multiples.
Regional, multidisciplinary, and collaborative care are needed in the perinatal period (Chalmers et al., 2001; Myors et al., 2013), and such social support and professional activity are often indispensable for families with multiples (Baor & Soskolne, 2012). Despite the fact that many parents of multiples expressed interest in any form of mental health treatment, few of them received it (Wenze & Battle, 2018), possibly due to insufficient human resources (Futakawa & Nagayama, 2014). In Japan, regional governmental support is delivered by public health centers. While the human resources are insufficient, some private organizations provide families with places in which they can meet with other families, obtain useful information, and consult with staff about child rearing. These types of organizations function well as a regional security bases for families that are close to them. One such type of organization is referred to as a regional parenting support hub. This is a place that provides support itself and which connects families to other families or appropriate support organizations.
Regional parenting support hubs in Japan are a governmental enterprise providing regional parenting support. They are managed by social welfare conferences or non-profit organizations that have received a mandate from the local government. They were established against a background of the recent Japanese trend toward nuclear families, which makes it difficult to carry on the tradition of parenting of previous generations, and trend toward weaker regional mutual support and less cooperative parenting. Regional parenting support hubs were organized to overcome these issues and establish a place for parents and supporters in their local areas to gather and develop relationships without constraints, support each other, consult with each other, and study together. In this background, regional parenting support hubs have spread throughout Japan, with more than 7,000 as of 2019 (MHLW, 2020). In almost all developed countries, which have more working mothers than Japan, parenting support centers focus on childcare. In New Zealand, however, there are play centers for infants-toddlers and their parent; however, they are educational. In the U.S., family resource centers do exist, however, their mission is primarily to help prevent and treat instances of child abuse and neglect. Regional parenting support hubs are thus a unique Japanese system for providing parenting support that fit the needs of Japanese parents who seek general advice and who would like to have a community center that they can visit and to talk with staffs or other parents from the prenatal to infant parenting period. Most pregnant women are informed of the existence of regional parenting support hubs, and many like to visit them.
As mentioned previously, many studies have described the difficulties of families with multiples, but how regional parenting support organizations recognize these difficulties and actually provide support are unknown. Regional parenting support hubs are local regional support organizations for parents, and their provision of a place to stay might be particularly important for parents of multiples. How then do the parenting support hubs recognize the difficulties and needs of families with multiples in comparison to families with singletons, and how do they actually support families? We hypothesized that they did recognize the difficulties faced by these families (hypothesis 1) but did not support them despite their need because few mothers of multiples receive mental health support despite their interest in receiving such support (Wenze & Battle, 2018) (hypothesis 2). Do the parenting support hubs recognize the difficulties of families with multiples in the parenting period in comparison to those in the pregnancy/delivery period? We hypothesized that they understood these difficulties in the parenting period as well as pregnancy/delivery period because the risk of abuse of multiples is well known (hypothesis 3). Finally, we sought to shed light on what is important for ensuring a high level of recognition and support. We hypothesized that the hubs that cooperate with other organizations well would recognize the difficulties faced by families with multiples because cooperation with other organizations is important for perinatal support (Myors et al., 2013), and it might enhance the ability to obtain information on the difficulties they face (hypothesis 4).
Method
A questionnaire was distributed to regional parenting support hubs throughout Japan. We asked all parenting support hub liaison councils in Japan, and the questionnaire was presented to 720 regional parenting support hubs that were located in each region. The questionnaires were answered by Google Forms, website, fax, or as an e-mail attachment. We sent explanatory text describing the purpose of the survey and ethical considerations, including considerations regarding the anonymity of the respondents and hubs, confidentiality, and arbitrary property, along with the questionnaire and it was deemed that informed consent had been given when respondents agreed to answer.
The respondents’ names and contact information were collected in preparation to respond to queries with the protection of respondent’s privacy. We asked some individuals in charge of parenting support to answer the questionnaire in order to check the contents and it took approximately 10 to 15 minutes to answer. Participants received a prepaid card worth 1,000 yen.
Participants
The respondents were the administrators of the parenting support hubs, and one response was accepted from each hub (n = 522, response rate: 72.5%).
Survey Design
To develop the questionnaire, we conducted two interviews at regional parenting support hubs in Sousha City, Okayama Prefecture and Shirakawa-City, Fukushima Prefecture, which are located in Western and Eastern Japan, respectively, concerning their operation, cooperation, and coproduction with the government, especially regarding the support of parents of multiples. This was done in order to gain a better understanding of the reality of the situation concerning the operation and cooperation of these hubs, which was unknown. The questionnaire was then developed based on the interviews. We extracted various answers, categorized the qualitative data from their narratives, and created question items. We then checked the accuracy of the expression and whether the items could measure what we wanted to know. It was distributed to regional parenting support hubs throughout most of Japan in cooperation with the parenting support hub liaison council in Japan.
Measures
The questionnaire inquired about the support measures available for parents of multiples. All of the following measures were original measures developed by the authors:
A scale asking about the background of the parenting support hubs (nine items, e.g., number of staff members, days of operation during the week).
A scale asking about how the hub handled the special needs of families with multiples (three items, e.g., “we speak to all families with multiples” and “we hold networking events for parents of multiples.”).
A scale asking about their recognition of the special difficulties and needs of families with multiples (25 items, e.g., “bathing difficulties” and “need for information on play areas”). The answers were 1 (not different from families with singletons), 2 (a little different from families with singletons), or 3 (definitely different from families with singletons).
A scale asking about cooperation with the local government in supporting families with multiples (three items, e.g., “cooperation with parenting support organizations for multiples” and “cooperation with other child parenting support hubs”).
Scale asking about the support that was deemed helpful for families with multiples (18 items each for the gestation period and child-rearing period, e.g., “enterprises providing support in the prenatal and antenatal period” and “cooperation of parenting support organizations and health organizations”). The answers were 1 (not different from families with singletons), 2 (a little different from families with singletons), or 3 (definitely different from families with singletons).
A scale asking about the measures deemed helpful for families with multiples in comparison to families without multiples (11 items, e.g., “information on governmental efforts to support families with multiples” and “information on support and policy expected by families with multiples”). The answers were 1 (not different from families with singletons), 2 (a little different from families with singletons), or 3 (definitely different from families with singletons).
Data Analyses
First, we described the sample demographics and practical approaches enacted by parent support hubs for families with multiples. A factor analysis was then performed to extract factors, and to evaluate the factorial structure and factor reliability of the scale asking about their recognition of the special difficulties and the needs of families with multiples measure. Paired t-tests were used to compare the hubs’ recognition of difficulties faced by families with multiples during pregnancy/delivery vs. while parenting. In addition, we compared the hub’s recognition of the difficulties faced by families with multiples according to their cooperation using independent t-tests. We thus conducted a factor analysis of the original measures and then compared the means of variables using t-tests. All statistical analyses were conducted using the IBM SPSS statistics software program (ver.24).
Results
Sample Demographics
The number of full-time and part-time staff members at the responding regional parenting support hubs ranged from 0 to 46 (M = 3.17) and 0 to 112 (M = 5.30), respectively (Table 1). More than half of the hubs were open on holidays. The mean number of daily users ranged from 0 to 370 (M = 24.32); families with twins or super-twins accounted for less than 1 user per day.
Practices of the Responding Child Parenting Support Hubs (n = 522).

Standard deviation.
Percentages of hubs among the hubs that completed the individual items.
Most of the responding child parenting support hubs held face-to-face consulting, less than half held telephone consulting, and only a few held mail consulting. A web site, blog, or leaflet was often used to make announcements. Almost half of the respondents had established user support projects, and one-third provided temporary childcare.
Approaches Specialized to Families With Multiples
Support in the Facility
Most child parenting support hubs provided some specialized support for families with multiples (Table 2). For example, there were bi-monthly network events for families with multiples known as “twins clubs” in Kyoto-City, Kyoto-Prefecture. In Shirakawa-City, Ishikawa-Prefecture, one parenting support hub opened exclusively for multiples on Fridays. Approximately half of the parenting support hubs spoke to all families of multiples, meaning that those families were more proactively contacted in comparison to families with singletons, and introduced to some services that were helpful to families with multiples (e.g., temporary childcare, housekeeping assistance, and child-rearing circles).
Specialized Approaches for Families With Multiples (From Pregnancy to 3 Years of Age).

Standard deviation.
Networking Event for Parents With Multiples
Only 16.35% of parenting support hubs held networking events for parents of multiples. Among them, the mean annual frequency of networking events was 7.96, and the mean number of parents who attended such events was 5.21 pairs.
Regional Child-Parenting Support Information Service
Approximately three quarters of the parenting support hubs provided multiple-children-specialized information (76.05%). Almost half of the parenting support hubs introduced daycare centers (43.68%) and child rearing support services (53.45%).
Cooperation With Child Parenting Support Organizations for Multiples or Local Government
Cooperation With Parenting Support Organizations
Most of the regional parenting support hubs (71.65%) did not cooperate with parenting support organizations (Table 3).
Cooperation With Any Parenting Support Organizations for Multiples or the Local Government (Multiple Choice).

Cooperation With Other Parenting Support Hubs
Approximately half of the hubs cooperated with other parenting support hubs (51.53%). Among those, a relatively large number of hubs (30.6%) exchanged information on support for families with other organizations.
Cooperation With Local Governments
Approximately two-thirds of the hubs cooperated with local governments in some way (63.42%). One-third delivered and shared information on families with multiples with the government as necessary (33.33%) or asked the local government to introduce parenting support hubs (32.57%).
Recognized Difficulties and Needs of Families With Multiples in Comparison to Families of Singletons
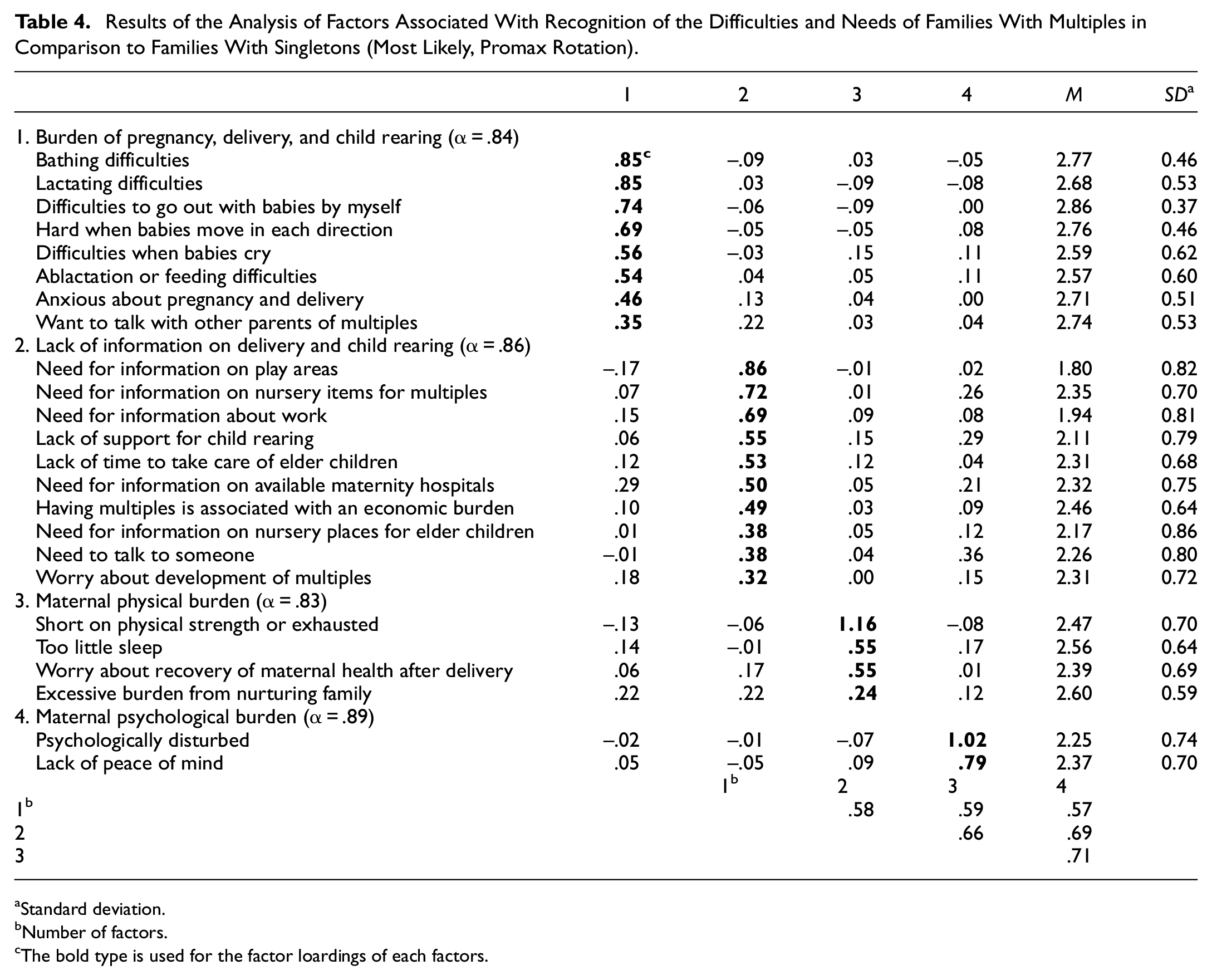
Almost all of the scores for questions about the recognition of the special difficulties and needs unique to families with multiples were more than 2 points, which is the central value between the minimum and maximum values (Table 4). This indicates that child parenting support hubs recognize that families with multiples have various difficulties and needs that are different from families with singletons. The items that had a mean of <2 points included “need for information on play areas (1.80)” and “need for information about work (1.94).”
Results of the Analysis of Factors Associated With Recognition of the Difficulties and Needs of Families With Multiples in Comparison to Families With Singletons (Most Likely, Promax Rotation).
Standard deviation.
Number of factors.
The bold type is used for the factor loardings of each factors.
We conducted a factor analysis (promax rotation, most likely) of the 25 items and extracted 4 factors because of the shape of scree plots. Promax rotation was adopted because correlation between factors were assumed. The loading of the items on these four promax-rotated factors is shown in Table 3. The “burden of pregnancy, delivery, and child rearing” factor consisted of eight items, including “bathing difficulties” and “lactating difficulties,” which reflected the burden of pregnancy, delivery, and child rearing of multiples. The “lack of information on delivery and child rearing” factor consisted of 10 items, including “need for information on play areas” and “need for information on nursery items for multiples,” which meant that they recognized that families lacked information on delivery and child rearing. The “maternal physical burden” factor consisted of four items, including “short on physical strength or exhausted” and “too little sleep,” which reflected the physical burden associated with rearing multiples. The “maternal psychological burden” factor consisted of two items, “psychologically disturbed” and “lack of peace of mind,” which reflected the psychological burden associated with rearing multiples.
Differences in the Recognized “Difficulties and Needs of Family,” With Multiples According to the Cooperation Practices of Parenting Support Hubs
Independent sample t-tests were conducted to analyze the differences in the scores of each factor related to recognizing the difficulties and needs of families with multiples (Tables 4 and 5) according to the cooperation practices of parenting support hubs (Table 3). Factor scores were the mean scores of the items of each factor. P values were determined with Bonferroni correction.
Difference of Recognized Difficulties and Needs of Families With Multiples According to Cooperative Activities of Parenting Support Hubs.

Number of participants.
Effect size: Cohen’s d.
Mean.
Standard deviation.
Statistical significance (Bonferroni corrected).
p < .05. **p < .01. ***p < .001.
Regarding the differences in recognizing the difficulties and needs of families with multiples according to “whether or not hubs cooperate with other parenting support organizations” the results indicated that hubs that reported cooperating with other parenting support organizations recognized that families with multiples have greater difficulties and needs than families with singletons for all factors(i.e., “burden of pregnancy, delivery, and child rearing” (p < .05, d = 0.22), “lack of information on delivery and child rearing” (p < .001, d = 0.37), “maternal physical burden” (p < .01, d = 0.27), and “maternal psychological burden” factor(p < .001, d = 0.36).
Regarding the differences in recognizing the difficulties and needs of families with multiples according to “whether they cooperate with other parenting support hubs,” the results indicated that hubs that reported cooperating with other parenting support hubs recognized that families with multiples have greater difficulties and needs than those with singletons in two factors (i.e., “lack of information on Delivery and child rearing” (p < .05, d = 0.23) and “maternal psychological burden” (p < .05, d = .20).
Regarding the differences in recognizing the difficulties and needs of families with multiples according to “whether they cooperate with the local government,” there was no marked difference in recognizing the difficulties and needs of families with multiples.
Support and Policies Needed During the Perinatal Period for Families With Multiples in Comparison to Those With Singletons
Pregnancy and Delivery Period
Almost all of the scores for questions on the recognition of support and policy measures that are needed during the perinatal period in families with multiples were more than 2 points, which was the central value between the minimum and maximum values (Table 6). This indicates that parenting support hubs recognize that families with multiples have a greater need for support and better policies during the perinatal period than families with singletons. The items that showed mean scores of <2 were “environmental arrangement such as road construction (1.84)” and “job assistance (1.85).”
Support and Policy Measures Needed by Families With Multiples in Comparison to Families With Singletons (Pregnancy/Delivery vs. Parenting Period).

Standard deviation.
Effect size: Cohen’s d.
Statistical significance (Bonferroni corrected).
p < .05. **p < .01. ***p < .001.
Parenting Period
Almost all of the scores for questions about the recognition of support and policy measures that are needed during the parenting period by families with multiples were more than 2 points, which was the central value between the minimum and maximum values of scores. This indicates that child parenting support hubs recognize that families with multiples have a greater need for support and better policies during the parenting period than families with singletons. Items that showed mean scores of <2 included “environmental arrangement, such as road construction (1.90)” and “job assistance (1.86).”
Difference Between “Pregnancy and Delivery Period” and “Parenting Period”
We tested the differences in each item concerning the support and policy measures needed for families with multiples between the “pregnancy and delivery period” and “parenting period” by conducting t-tests. P values were determined with Bonferroni correction. Paired t-tests showed that the scores for the “pregnancy and delivery period” were greater than those for the “parenting period” for the following items: “cooperation of hospitals and health organizations (p < .01, d = .11),”“enterprise providing support in the postnatal and antenatal period (p < .001, d = .26),”“postnatal care enterprise (p < .001, d = .19),” and “information service for parenting of multiples (p < .001, d = 0.35),” which showed moderate to small effects. In contrast, the scores for the “pregnancy and delivery period” were less than those for the “parenting period” for the following items: “counseling with specialists such as children’s nurses (p < .001, d = .11)” which showed small effect.
What Is Deemed Helpful for Parenting Support Organizations to Support Families With Multiples
None of the scores for questions about recognizing what is deemed helpful for parenting support organizations to support families with multiples were <2 points, which was the central value between the minimum and maximum values (Table 7).
Discussion
Principal Findings
The main findings of this study were that although regional parenting support hubs recognized that families with multiples have greater difficulties than those with singletons during both the pregnancy and child-rearing periods (Tables 4 and 7), most did not provide the helpful support, which supported hypotheses 1 and 2 (Tables 2 and 3). The hubs felt that there was a lack of information on the difficulties experienced by families with multiples and how best to support them (Table 7). The comparison of support measures for the pregnancy/delivery period and child-rearing period for families with multiples recognized as helpful by parenting support hubs indicated that the hubs recognized that families with multiples require more support in the pregnancy/delivery period than during the child-rearing period with small to moderate effect sizes, which conflicted with hypothesis 3 (Table 6). Partly as we predicted in hypothesis 4, parenting support hubs cooperating with other parenting support groups showed a greater recognition of the difficulties and needs faced by multiples in comparison to hubs not showing such cooperation regarding all aspects investigated in the present study, including the child rearing (or pregnancy/delivery) burden, lack of information on delivery and child rearing, maternal physical burden, and maternal psychological burden, all of which showed small to moderate effect sizes (Table 5).
Average and SD for “What is Helpful for Parenting Support Organizations to Support Families With Multiples?”

Note. None of the scores for questions about recognizing what is deemed helpful for parenting support organizations to support families with multiples were <2 points, which was the central value between the minimum and maximum values.
Standard deviation.
The Comparison With Other Studies
Regional parenting support hubs recognized greater difficulties for families with multiples in comparison to families of singletons (Table 4). Specifically, they recognized that they have a heavier burden in the antenatal and postnatal periods, a greater lack of information, and have greater physical and mental stress. With the exception of economic difficulties (Andrade et al., 2014; Glazebrook et al., 2004), which regional support hubs did not recognize well as a difficulty faced by families with multiples, these results are closely in line with studies describing difficulties in baby rearing (Bolch et al., 2012) and physical and mental stress (Baor & Soskolne, 2012; Choi et al., 2009; Ellison & Hall, 2003; Lutz et al., 2012; Sheard et al., 2007) among mothers of multiples. Although the economic burden is suggested to be heavier in families with multiples than in those with singletons (Andrade et al., 2014), and despite mothers of multiples being paid less than those of singletons (Glazebrook et al., 2004), this study showed that parenting support hubs did not recognize that mothers of multiples had a greater need for information about work or job assistance than mothers of singletons (Table 4). Thus, the economic burden seems to be overlooked in support for families with multiples, and it would be helpful for parenting support hubs to recognize such economic difficulties when providing support.
Parenting support hubs are suggested to recognize that the difficulties of families of multiples were greater during the pregnancy/delivery period than during the parenting period (Table 6). Pregnancy and delivery of multiples are actually high-risk events, and a high level of medical care is required. However, the rearing of multiples imposes heavy burdens and is associated with a greater risk of child abuse in comparison to the rearing of singletons (Andrade et al., 2014; Baor & Soskolne, 2012; Bolch et al., 2012; Choi et al., 2009; Ellison & Hall, 2003; Glazebrook et al., 2004; Golombok et al., 2007; Lutz et al., 2012; Sheard et al., 2007; Tanimura et al., 1990; Vilska et al., 2009). Nevertheless, in many cases, no special care is provided to these families. This might have put dissuaded parents of multiples from joining parent support hubs. Therefore, when presenting information on parenting support for families with multiples, the importance of the provision of support during the child-rearing period should receive greater attention.
Emotional isolation is reported to strongly contribute to the experience of antenatal depression (Jones et al., 2014; Raymond, 2009). Thus, continuous community care is an important aspect of antenatal care (Earle, 2000; Homer et al., 2000). Recognizing the risk of isolation and having pathways of referral to peer support is important for antenatal care (Jones et al., 2014), and “low-tech” interventions, such as peer support, are helpful for supporting women with antenatal depression (Raymond, 2009). Mothers of multiples have 43% greater odds of having moderate/severe depression at 9 months postpartum in comparison to mothers of singletons, which is an issue that needs to be addressed (Andrade et al., 2014). Multiples often have a lower birth weight and require pediatric follow-up. Thus, greater attention is needed in medical institutions, such as pediatric clinics (Choi et al., 2009) and psychiatric nurses (Lau, 2011), in order to address or prevent maternal depression in families with multiples. This study showed that parenting support hubs recognized that enhancing families’ connectedness to society during the pregnancy/delivery period and the construction of regional support systems in the postnatal period are support and policy measures that are needed by families with multiples (Table 6). These results are consistent with the results of the abovementioned studies, and our study suggests that regional parenting support hubs recognize that the support of families with multiples is important for them to avoid becoming isolated.
While many studies have focused on the difficulties experienced by families with multiples in comparison to those with singletons (Andrade et al., 2014; Baor & Soskolne, 2012; Bolch et al., 2012; Choi et al., 2009; Ellison & Hall, 2003; Glazebrook et al., 2004; Lutz et al., 2012; Sheard et al., 2007; Tanimura et al., 1990; Vilska et al., 2009), the means by which parenting support organizations or communities recognize their difficulties and how they actually support families with multiples have received little attention. Among the few studies to shed light on support for families with multiples, a survey of medical institutions and public health centers suggested the need to establish an appropriate information and network system among medical institutions and local governments (Futakawa & Nagayama, 2014). Because the survey was only conducted in one prefecture in Japan, the results may have been influenced by some regional-specific factors. The results showed that despite most institutions and organizations recognizing the need to support families with multiples, most did not actually provide specialized support. One suggested reason for this was a workforce shortage in medical institutions and health organizations. We therefore suggest that regional parenting support hubs could play a key role in supporting families with multiples. In spite of that, few parents of multiples visit a hub. Parenting support hubs have to better recognize their needs and bridge the gap between what they need and what they can receive there, or they might provide outreach to the families because it would be difficult for the families with multiple babies to visit the hub.
Cooperation is suggested to be an important factor for enhancing parenting support (Table 5). With cooperation, parenting support hubs become more familiar with the difficulties of parenting and how to support parenting, and hubs can then help each other with difficult cases. Thus, parenting support hubs should be included in the network and cooperation among medical institutions, local government and regional parenting support hubs could then help support families with multiples. Human resource shortages and difficulties in cultivating routes of cooperation may be obstacles to cooperation; thus, the administrative construction of comprehensive cooperation systems is desired.
Strength and Limitations
The strength of this study is that it sheds light on how regional parenting support hubs, which are the local support organizations for child-rearing families, recognize, and support families with multiples. A weakness and limitation of the present study is that the results are based on a questionnaire that was conducted only in Japan. Furthermore, the questions in the questionnaires used in this study had not been validated. There were also statistical limitations. The P-values of the t-tests may have been significant because of the large sample size, and the effect sizes were small to moderate. These limitations should be taken into consideration when interpreting the results of this study. Despite these limitations, the survey in our study was held in most districts of Japan, including urban and rural areas, and thus represents unique and valuable research from a developed Asian country.
Conclusion
Families with multiples bear greater risks than families with singletons during both the prenatal and postnatal periods. The community must therefore pay attention to families with multiples not only in the prenatal period but also in the postnatal period, which is a time when families do not receive intense medical care. Parenting support hubs, which are a unique Japanese system and which support families in the antenatal period, can play a key role in helping families with multiples. Therefore, much more information should be provided to these hubs in order to help caretakers understand the difficulties faced by families with multiples and how to help them. Cooperation may be an important factor for understanding the difficulties associated with rearing multiples and how to support them, and cooperation with other parenting support hubs or with medical institutions and local governments could contribute to the provision of more effective support.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440231200140 – Supplemental material for Difficulties of Families With Multiples Recognized by Regional Parenting Support Hubs: A National Public Health Service Study in Japan
Supplemental material, sj-docx-1-sgo-10.1177_21582440231200140 for Difficulties of Families With Multiples Recognized by Regional Parenting Support Hubs: A National Public Health Service Study in Japan by Miki Mizumoto, Yoshiyuki Tachibana, Masashi Mikami and Taeko Matsuda in SAGE Open
Footnotes
Abbreviations
SD: standard deviation
d: Cohen’s d
Author Contributions
Conceived and designed the experiments: YT and TM. Performed the experiments: YT and TM. Analyzed the data: MiM and MaM. Wrote the paper: MiM and YT.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Health and Labor Sciences Research Grant on Children, Youth and Families (H28-Sukoyaka-Ippan-005, H29-Sukoyaka-Ippan-004) provided by the Japanese Ministry of Health, Labour and Welfare, the Research Grant of the Project for Baby and Infant in Research of Health and Development to Adolescent and Young Adult-BIRTHDAY (30AMED-6024) provided by the Japanese Agency for Medical Research and Development, the Research Development Grant for Child Health and Development (2020B-14) provided by National Center for Child Health and Development, as well as KAKENHI Grant Number JP20K14233 provided by Japanese Ministry of Education, Culture, Sports, Science and Technology.
Consent to Participate
We sent an explanatory text describing the purpose of the survey and ethical considerations, including considerations concerning the anonymity of the respondents and hubs, confidentiality, and arbitrary property, along with the questionnaire and deemed that informed consent had been given when respondents agreed to answer the questionnaire.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.