
Abstract
Colombia has a mixed public-private health care system, and although official data indicate more than 95% of health coverage, research in this field has demonstrated the persistence of barriers to accessing health care services. This study aimed to analyze the conceptual framework of health services accessibility and develop measurement tools for its assessment using primary data and also to propose a method for ascertaining health services accessibility and availability using a territory-based approach. A mixed method study with concurrent design was carried out in four phases between 2014 and 2017. The starting points were a review of the literature and a documentary research that identified five conceptual frameworks for health services accessibility published between 1970 and 2013. It was found that the theoretical concept of health services availability has not been clear; the literature does not define it explicitly and does not differentiate it from the concept of health coverage. As a result, two measurement tools were developed: a Health Care Services Accessibility Household Survey and a Health Care Services Availability Questionnaire. These tools and the proposed method for ascertaining health services accessibility can be useful for government, institutions, and social and scientific organizations to monitor progress in guaranteeing the fundamental human right to health, declared in the Health Organic Law issued in 2015 in Colombia.
Introduction
Colombia has a mixed health care system, with medical and health services provision, parallel public and private financing and insurance intermediaries called Health Promoting Enterprises (EPS, as per its acronym in Spanish) that manage the resources. In 2001, the nation failed to meet its Universal Health Coverage (UHC) overall goal and reached only 60% of the population (Ministerio de Salud y Protección Social, 2018); in July of 2020 this coverage was 96.33% (Ministerio de Salud y Protección Social, 2018), which means a substantial advance in terms of health system performance in the nation. Nevertheless, despite reforms made to the system since its implementation in 1993, different sectors of Colombian civil society have criticized the structure and organization of the system due to persistent differences between UHC data and real accessibility to health services.
In particular, three facts contradict the statement that UHC and health services accessibility are equal. First, there is ample scientific evidence to demonstrate economic (Restrepo Zea et al., 2007), geographical, administrative (Alvarez et al., 2011; Bello & Bonilla, 2008; Echeverry-López, 2011; I. Jaramillo et al., 2000; Rodríguez & Roldán, 2010; Velásquez-De Charry et al., 2009; Vélez-Arango et al., 2007), cultural, regulatory, and supply-related barriers (Alvis-Guzmán et al., 2008; J. V. Jaramillo & Marín, 2009; Tovar-Cuevas & Arrivillaga-Quintero, 2014; Vargas-Lorenzo et al., 2010). “Bureaucratic itineraries,” as these barriers have been called by experts on the Colombian health system, persist (Abadia & Oviedo, 2009). When people enter the services, they face complex and excessive administrative procedures and difficulties accessing care, with delays in allocation of medical appointments and in diagnosis, treatment, and authorization for medicines delivery. Second, in Colombia, legal actions (Tutelas in Spanish) against the health system due to poor access to health care services have been increasing, reaching a record of 617,071 in 2016. (Defensoría del Pueblo, 2018). The latest report available about Tutelas in 2018 showed that 207,734 claims remain due to lack of access to health services (Defensoría del Pueblo, 2019). And third, the highest health authority in the nation, the Ministry of Health and Social Protection, has difficulties in regulating and guaranteeing the fundamental human right to health, in the context of a fragmented system and with the participation of multiple agents from public and private sectors (Domínguez et al., 2017).
Data on health services accessibility in Colombia are segmented into different sources of information. The “Integral Social Protection Information System” (SISPRO, for its acronym in Spanish) contains records of the number of people affiliated to the system, health facilities, hospital beds, operating rooms and physicians (per 1,000 people), and prenatal care and births in health facilities (Ministerio de Salud y Protección Social, n.d.). The “Quality of Care Observatory” provides indicators of timely access for medical appointments. Health insurance intermediaries and health institutions control data on accessibility to care for specific diseases; with regard to accessibility to health promotion and disease prevention programs, complete and reliable information is even more difficult to obtain. The fragmentation of the Colombian health system, with both public and private health insurers and health service providers, means that the nation does not have reliable information on accessibility beyond the indicators described here and UHC reports.
At present, there is wide scientific evidence on the magnitude of inequalities in health services accessibility; nevertheless, this evidence is incomplete and difficult to interpret due to the diverse methodologies applied for its assessment. Globally, equity in accessibility to health care has been a central objective of many health systems; however, as described before, in Colombia, the evidence shows that there are serious problems. Linked health coverage data and health insurance affiliation data are not a good indicator of real access to health services, and the adverse consequences of this affect patients and their families.
Given the described scenario, this study aimed to analyze the conceptual framework of health services accessibility; to develop measurement tools for its assessment with primary data; and to propose a method for ascertaining health services accessibility and availability using a territory-based approach.
Methods
Type of Study
A mixed method study with concurrent design in four phases (Hernandez Sampieri et al., 2010) was conducted between 2014 and 2017. This design allowed triangulation of quantitative and qualitative data during data collection, data analysis, and data integration in the interpretation phase (Hossler & Vesper, 1993). Theoretical and empirical data were gathered simultaneously, results were compared, and congruence was assessed. Qualitative to quantitative data integration occurred at all phases and during analysis (Creswell & Clark, 2017; Creswell et al., 2003; Tashakkori & Teddlie, 2003).
The research project was approved by the ethics review committees of the Pontificia Universidad Javeriana Cali and the participating health care centers. Written informed consent was obtained from all participants.
Phases
Phase 1
Systematic review and documentary research. In this phase, the theoretical concepts and dimensions of health care services accessibility and availability were analyzed. A review of governmental documents, health surveys and Colombian health regulations, which served as reference frame for the design of measurement tools to assess accessibility, was also carried out.
Phase 2
Design of a Household Survey on Accessibility to Health Care Services (Encuesta de Acceso a Servicios de Salud para Hogares Colombianos- EASS by its acronym in Spanish) and a Health Care Services Availability Questionnaire (Cuestionario de Disponibilidad de Servicios de Salud- CDSS by its acronym in Spanish), as well as compiling the corresponding application manuals.
Phase 3
Content validity with experts and a pilot test. Five experts were selected to assess each instrument; the inclusion criterion was a minimum of 15 years’ experience as a provider or manager in a public or private health care center. For pilot tests, the EASS was administered in representative samples of households in two cities (Jamundi and Palmira), and the CDSS was administered in health care centers in Cali.
Phase 4
Design of a method for ascertaining health services accessibility with primary data and a territory-based approach.
Procedure and Analysis
In Phase 1, a systematic review of empirical and theoretical publications from 1970 to 2015 in the EBSCO, JSTOR, Proquest, ISI Web of Science, and Scielo databases was carried out. The main inclusion criterion was that documents explicitly described the concept of health care services accessibility. Keywords included combinations of (in Spanish and English) health services accessibility, conceptual framework, theory, and conceptual model. Information extracted from relevant publications included the following: year of publication, setting/country, definition of accessibility and availability and main conclusion. In this phase, the methods/techniques used to measure both accessibility and availability were also reviewed on a national and international scale.
Regarding health care services availability, a systematic search was carried out on the internet using keywords, both in Spanish and English: offer of medical care, availability of health care services, and medical assistance. The search included a selection of documents on current national regulations and operating conditions of health centers.
In Phases 2 and 3 of measurement tools development, the structure and assessment modules were defined based on the previous systematic review of literature and documentary research. During content validity, the experts used an evaluation sheet to record their views on the relevance and adequacy of each module and the wording of each item. After consolidating results, a discussion group was held with the experts to make final adjustments to each tool.
The EASS questionnaire was administered face-to-face in urban households in Jamundí and Palmira municipalities. Probabilistic, multi-stage, stratified, and cluster sampling was performed. The stratification variable was socioeconomic stratum (category established by law in Colombia that classifies the socioeconomic stratum from 1 to 6). The primary sampling units were neighborhoods, randomly selected. If there were two or more households in a dwelling, one of them was chosen at random. The stratified component of sampling was done with proportional allocation according to the size of each stratum. The sample size was calculated taking into account a non-use of health services proportion of 50%, a confidence level of 95%, an estimation error 5%, and a design effect of 2. Finally, 215 households were surveyed in Jamundi and 242 in Palmira. For its part, the CDSS pilot test was conducted in a convenience sample of eleven health care facilities in Cali. The questionnaire was administered face-to-face to managers and providers responsible for the services to be assessed.
Once data were available from both the EASS for households and the CDSS for health care facilities, these data were organized in an evidence matrix by dimensions, modules, and items. In the case of the EASS, a descriptive analysis was carried out using frequency tables for categorical variables and measures of central tendency, dispersion, and “shape” for quantitative variables.
Finally, after triangulating the qualitative and quantitative data, adjustments were made accordingly to obtain the final versions of the measurement tools. In Phase 4, guidelines were defined to assess accessibility to health care services with primary data using a territory-based approach.
Results
The Concept of Health Care Services Accessibility
Twenty-five documents published between 1970 and 2013 that explicitly conceptualize accessibility were reviewed. The documents were classified into five categories/frameworks: accessibility to health care services in terms of (a) the decent minimum of health care, (b) the health care market, (c) factors and multicausality, (d) needs, and (e) social justice and the human right to health (Arrivillaga & Borrero, 2016). Figure 1 summarizes the results.
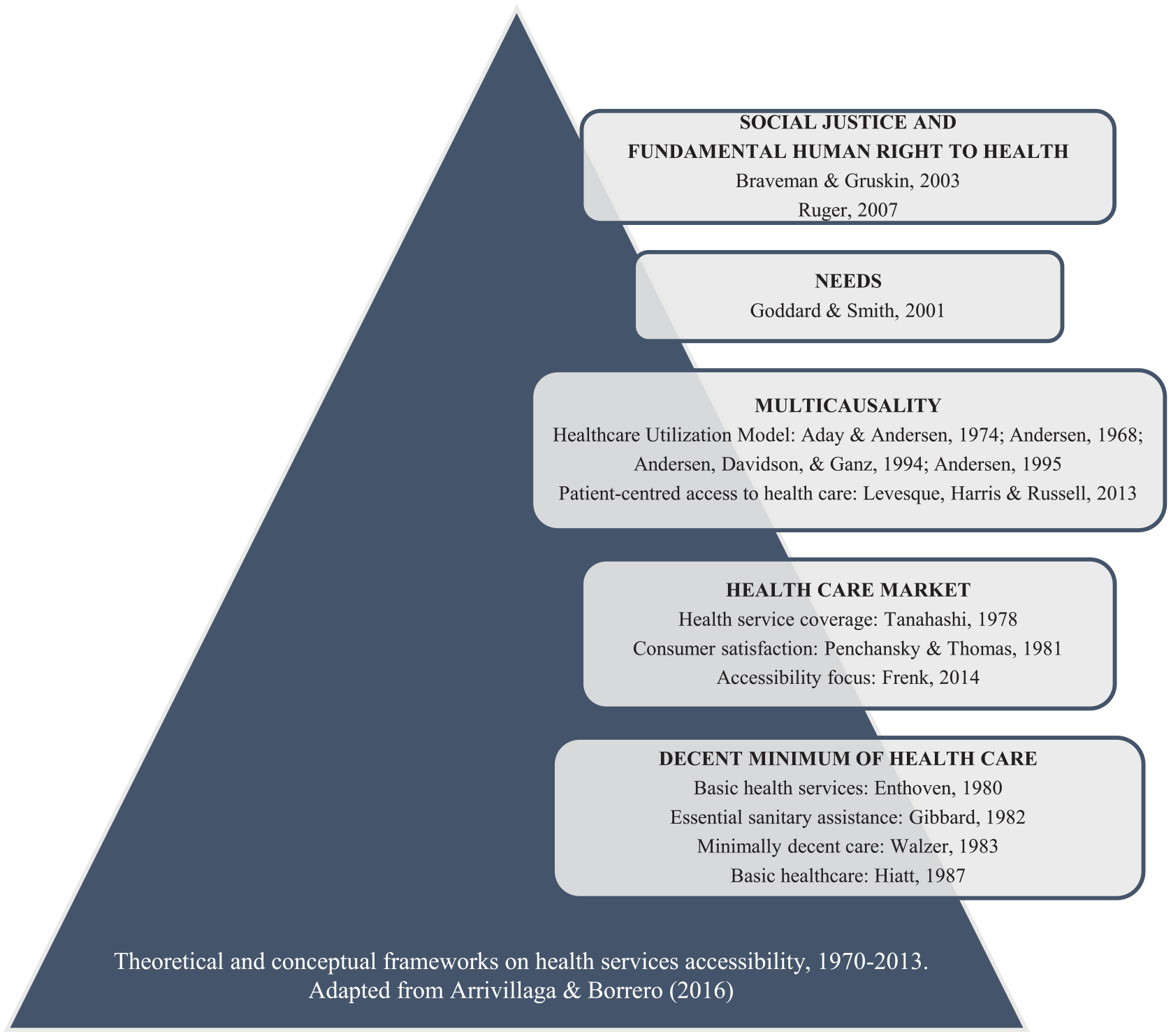
Theoretical and conceptual frameworks on health services accessibility, 1970–2013.
Regarding the decent minimum of health care, accessibility has been defined as the ability to ensure a set of specific services, of a specific level of quality, with a specific and maximum level of personal inconvenience and costs for patients, and in possession of a specific amount of information that the population must have to reach the services. This perspective guided the recommendations of the World Bank in 1993, raised in “Investing in Health” (World Bank, 1993), where countries were oriented to define basic health services packages.
As to the health care market, there are different positions on whether the emphasis should be on the initial contact, in the offer or supply, on the health care process per se, or on the characteristics of the demand. This supply and demand dynamic dominated conceptual models on health access and has been strengthened with multicausal explanations (Bashshur et al., 1971). In terms of factors and multicausality, the idea of consuming health care services is anchored by accessibility models organized in levels, ranging from the individual to the political level. Hence, accessibility is a result of offer-related factors such as location, availability, cost and convenience of services, as well as demand-related factors, such as disease burden, knowledge, attitudes, skills, and self-care. The most representative conceptual model often quoted in the literature comes from Andersen and colleagues (Andersen, 1995).
In respect of needs, two conceptual orientations regarding the principle of distribution of health services stand out: a horizontal alignment, stating that all people with equal needs should be treated equally; and a vertical, which suggests that people with greater needs be more generously treated than people with lower needs (Culyer & Wagstaff, 1993). Alternatively, it has been suggested that there are studies on disparities in accessibility that have not paid attention to the concept of need and that are based on assumptions such as that the levels of need are the same in all groups. As a result, it has been recommended that the operational concept of need should be derived from the analysis of people in each population group, according to their health needs and social circumstances (Goddard & Smith, 2001). Finally, the approaches in terms of social justice and human right to health exceed the concept of accessibility in itself and frame it in ethical principles of redistributive social justice and equity. Authors oriented to this focus have stated that it is necessary to ensure the human right to health as a framework for the organization of health systems and services, in which all individuals in a society must have the equal possibility of being healthy, taking in to account socioeconomic conditions (Braveman & Gruskin, 2003; Ruger, 2007).
The Concept of Health Care Services Availability
Nineteen articles published between 1990 and 2015 were reviewed. In conceptual terms, findings showed that authors do not explicitly define health services availability and do not differentiate this concept from offer or universal health coverage. In empirical terms, the results describe a range of variables to assess service availability. The review highlights studies on sexual and reproductive health services, communicable diseases, and medication availability. It is important to point out that no research was found in Colombia that offered measurement tools to assess services availability. Table 1 details the studies found and the variables used to measure health services availability, organized in six categories: general characteristics of health service, type of health service, health care records and programs, human resources, infrastructure, and equipment and supplies.
Studies and Variables to Assess the Health Care Services Availability, 1990–2015.

Health Care Services Accessibility Household Survey
As a starting point, and considering aspects from the discussed reviews, the author defined accessibility to health care services in an integral sense as the availability, offer and effective use of preventive, care and rehabilitation services, to respond to population specific needs, and that these services are sufficient, timely and quality-focused, guaranteeing the human right to health (Arrivillaga et al., 2016). This definition encompasses three dimensions of accessibility: how available the services are, how much health institutions promote them, and how much they are used by the population. The logic behind this definition is directly related to the effective response to health care needs with an emphasis on fundamental human right to health, regardless of the ability of individuals to pay for health services.
With this definition, a household survey was designed to collect primary data on accessibility to preventive services, curative and rehabilitation services, and out-of-pocket expenses. After content validity process with experts, and pilot test in 457 households, the final version of the “Health Care Services Accessibility Household Survey” (EASS by its acronym in Spanish) and its respective application manual were designed. The EASS comprises 63 questions distributed in five modules that take 45 to 50 min altogether to administer. The structure of the survey is shown in Table 2.
Structure of the Accessibility to Health Care Services Household Survey (EASS), Colombia, 2017.

Source. Adapted from Arrivillaga et al. (2016).
Health Care Services Availability Questionnaire
In a similar way to which the concept of accessibility had been developed, the concept of availability was defined as a set of human and technical resources, infrastructure and medical supplies for care, in accordance with the particularities of each health service and program and current health regulations, designed to respond to the population’s specific needs, in a sufficient, timely and quality-focused manner, and guaranteeing the human right to health.
With regard to Colombia, a review of health regulation regarding care centers was also carried out. Resolution 0429 of 2016 (Comprehensive Health Care Policy, PAIS by its acronym in Spanish) and Resolution 2003 of 2014, which defines the requirements for health centers operation, were analyzed. In turn, Resolution 412 of 2006, which establishes clinical guidelines for health care, early detection, and care of diseases of public health interest, was reviewed.
Having completed the review, the identification of variables to assess health services availability used in previous studies, the assessment of content validity with experts, and the pilot test in 11 health care facilities, the Health Care Services Availability Questionnaire (CDSS by its acronym in Spanish), was finalized. The CDSS assesses general characteristics of the health service, health care services programs, human resources, infrastructure, and equipment and supplies. The questionnaire can be adapted for its application in health centers with different health care levels, and if it is required to assess availability at all levels, traceable health services can be selected by age groups, as exemplified in Table 3.
Exemplification of Health Services by Age Group and Levels of Care, Used to Assess the Health Services Availability. Colombia.

Method to Assess Health Care Services Accessibility With Primary Data and Territory-Based Approach
Following all of the above, local accessibility of health services can be assessed using primary data, without the intermediary of health insurance entities. This method allows a summary appraisal of the real level of accessibility, beyond the universal health coverage indicator, and would enable government health authority actions to guarantee the fundamental human right to health. The proposed method is presented in Figure 2.
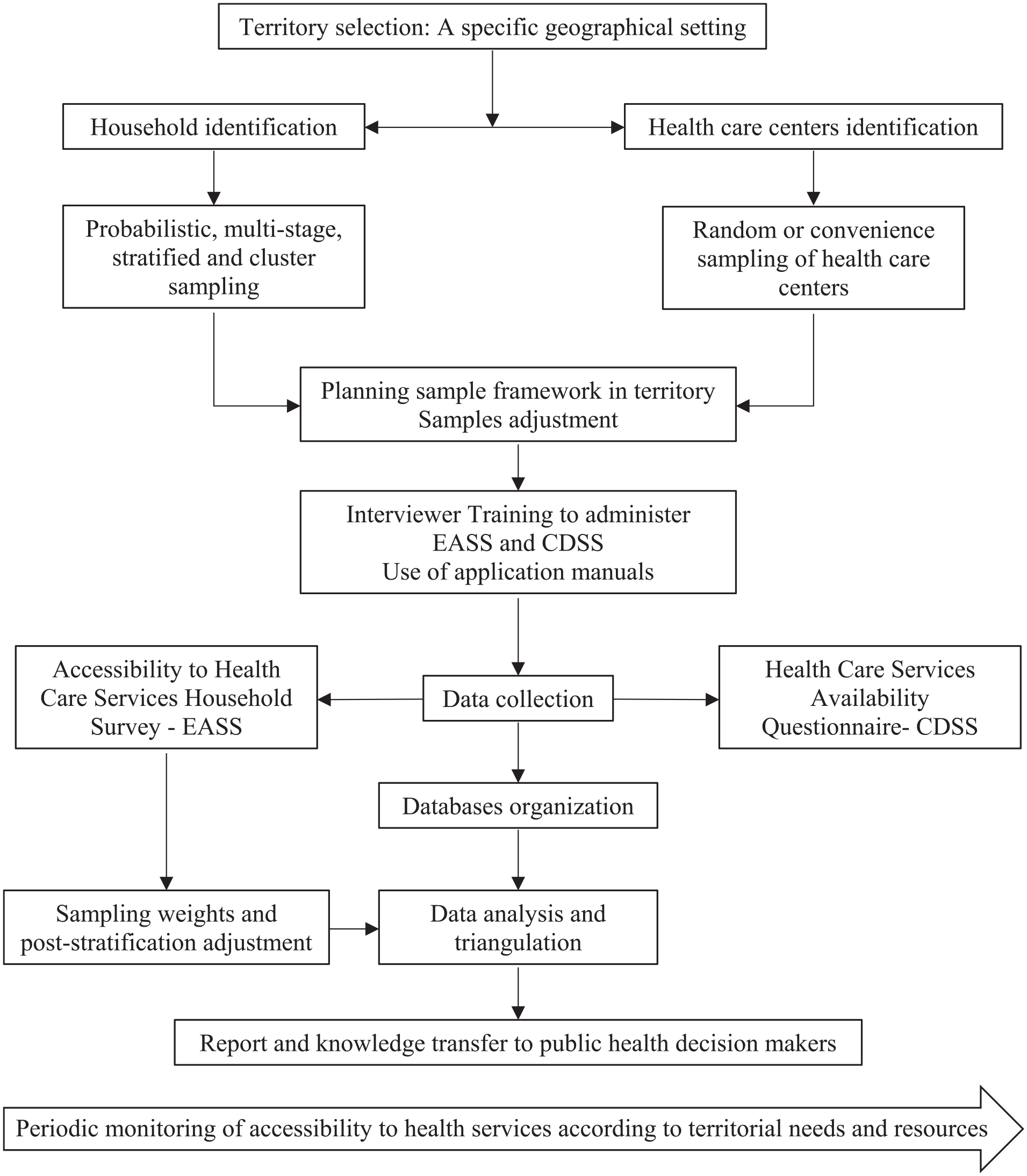
Method for the assessment of accessibility to health care services in Colombia with primary data and territorial approach.
Discussion
In 2008, the World Health Organization defined universal health coverage as the capacity of health systems to respond to the needs of the population, which includes assessing infrastructure, human resources, health technologies, provision of medications, and financing (World Health Organization, 2008). For its part, universal accessibility has been defined as the absence of geographical, economic, sociocultural, organizational, or gender barriers that prevent people from using comprehensive health services (Pan American Health Organization, 2014). As other authors have pointed out, there is currently a debate about whether health coverage is equal to accessibility, and Colombia is no exception. On one hand, there are sectors of the government that defend percentage of people affiliated to the health system as an indicator of universal health coverage; on the other hand, some sectors argue that such affiliation does not imply effective accessibility to health services (Evans et al., 2013).
It must be recognized that Colombia has made progress in terms of affiliation to the health system, reaching 97.2% of the population according to the information available to 2016 (Gaviria et al., 2016). This is presented by government and insurance sectors as evidence of achievement of universal coverage in health. However, there is wide scientific evidence, gray literature, legal actions (Tutelas), and press reports that show the contrary (Abadia & Oviedo, 2009; Defensoría del Pueblo, 2018; Espectador, 2019; J. V. Jaramillo & Marín, 2009; Tovar-Cuevas & Arrivillaga-Quintero, 2014). Across the nation, real accessibility problems persist and clearly affect most citizens, who constantly claim a lack of guarantees and numerous violations of their fundamental human right to health. These problems have multiple determinants, such as the health system structure with financial intermediation of funds, a fragmented insurance scheme with public and private health service providers, and an inadequate and insufficient distribution of health services offer with urban-rural geographical disparities (Vargas-Lorenzo et al., 2010).
Other determinants include failures in the quality of care, more emphasis on medical care than on health promotion and disease prevention, cumbersome administrative processes that delay care, and even corruption with unlawful appropriation and deviation of resources for other purposes (Abadia & Oviedo, 2009; Grupo de Economía de la Salud Restrepo, 2013). In this context, the universal health coverage indicator is questionable and unachievable because of the lack of timely and effective accessibility.
With this situation in Colombia, the available data are often used for or against those who defend the health system or those who have criticized it for more than 25 years after Law 100 of 1993, which is considered the basis of the current system. As previously stated, the accessibility data of the Ministry of Health and Social Protection are limited, insufficient, and as fragmented as the system itself. To ascertain health services accessibility, this study aimed to develop measurement tools to collect primary data and design a method for its administration in specific geographical settings. The joint application of these tools would make it possible to contrast health services availability, their offer by health care centers, and effective use by the population. Analysis of these crossover data could drive local health plans design according to needs, both in epidemiological and sociodemographic terms.
The measurement tools developed would provide a comprehensive overview of real accessibility in Colombia and may be useful for monitoring progress in changing the health model proposed in 2016 with the Comprehensive Health Care Policy (PAIS by its acronym in Spanish). Similarly, it is recommended that accessibility be critically monitored at all levels of care, taking into account Law 1751 of 2015 or the Organic Health Law that protects the human right to health. Sectors interested in accessibility to health services are recommended to use the method proposed in this study especially when the health insurance intermediaries intend to expand their primary care services under the auspices of health service networks. This could worsen fragmentation between levels of health care and between urban and rural settings.
By mixing research and quantitative and qualitative data this study gained in breadth and depth of understanding. However, the difficulty in coordinating the times of implementation of each of the phases in its two components of accessibility assessment in households, such as the assessment of health services availability in the same cities, should be noted as limitations. It would have been ideal to apply the proposed method in each of the settings evaluated. Clearly, a research design of this nature is very complex, and its implementation takes more time and resources than anticipated. In practice, it was difficult to move from one phase to another based on the previous findings. Following studies will focus on validity of the proposed method to monitor health services accessibility in one or several cities in Colombia.
Conclusion
Colombia has an insurance-based public-private health care system, and although the official data indicate a universal health coverage rate of over 96%, research has shown the persistence of barriers in health care services accessibility. The conceptual analysis questions the theoretical bases of health policy in Colombia in terms of equity and the universality of accessibility. The EASS and the CDSS, which have been developed, are a contribution to assess households’ accessibility to health care centers, periodically and with primary data. The designed method allows several governmental, social, and scientific actors to monitor progress in guaranteeing the human right to health, declared in the Statutory Law issued in the nation in 2015.
Footnotes
Acknowledgements
This paper is one of the results of the macroproject “Development of a Center on Social and Health Inequalities with emphasis on the Colombian Pacific” (CIDSSA Project). I thank the Pontificia Universidad Javeriana Cali, Colombia, for financing the project, and my colleagues Yadira Eugenia Borrero for her contribution in the literature review on accessibility to health services, Victoria Eugenia Estrada, who contributed in the design and validation of EASS and CDSS, Juan Carlos Aristizabal and Mauricio Pérez for the statistical analysis of household survey data, Lina Rocío Hurtado for her contributions in documentary research, and Clara Inés Sánchez, Diana Liceth Mora and Víctor Manuel Botero who collected the data in the city of Palmira.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research and/or authorship of this article: This paper is based on funding by the CIDSSA Project, which received funding from Pontificia Universidad Javeriana, Cali, Colombia, under grants agreement numbers 4055, 4182, and 4413.