
Abstract
Primary progressive aphasia (PPA) is a neurodegenerative disease characterized by the insidious and progressive loss of speech and language skills. However, there is no standardized intervention method applied in patients with PPA. It was conducted a virtual survey of SLTs across Turkey, to collect information about the assessment, intervention and management of patients with PPA. A total of 285 SLTs participated the survey; 76.8% (n = 219) of the respondents were female, 58.9% (n = 168) were 1 to 2 years post graduation, 62.8% (n = 179) of them were master’s degree, and 46% (n = 131) were working in a rehabilitation center. All 285 participants included in the study stated that they did not create a therapy process for their clients with PPA and they performed the therapy processes applied in the classical aphasia treatment. Two hundred sixty-eight participants stated that they had more than six sessions with their clients, and 280 respondents. It is very important for all participants to plan functional interventions that require joint participation with the patient and their family/caregiver or friends, which will support communication and language and communication-oriented intervention. However, there is a need to develop specific evidence-based care pathways for people with PPA so that more efficient interventions can be made. Raising awareness among SLTs and other clinical service providers that rehabilitation is effective can increase the accessibility of interventions for individuals with PPA and lead to a more robust support system for individuals affected by PPA.
Keywords
Introduction
Primary progressive aphasia (PPA), a dementia syndrome clinically involving declines in understanding and expressing language through symbolic representations (E. J. Rogalski & Mesulam, 2009). While language impairments are persistent and prominent throughout the course of PPA, other cognitive and behavioral deficits may also occur with disease progression (Mesulam et al., 2021a, 2021b; E. Rogalski et al., 2011). In cases of PPA, symptom onset is usually before the age of 65. An estimated 60% of PPA cases are associated with some form of frontotemporal lobe degeneration and 40% with the neuropathology of Alzheimer’s disease. (Mesulam et al., 2014, 2021a; Roberts et al., 2022). Because the ability to communicate with others is devastatingly impaired in people with PPA, specific treatments and therapies addressing speech and language symptoms that can improve quality of life for individuals with PPA and their families/caregivers are of great importance (Roberts et al., 2022).
Three PPA variants have been identified as a result of clinical studies: the logopenic/phonological variant (l/phvPPA), the semantic variant (svPPA), and the nonfluent/agrammatic variant (nf/avPPA) (Gorno-Tempini et al., 2011). Patients with l/phvPPA exhibit a slow speech consisting of pauses and simple sentences because they have difficulty in finding words (Gorno-Tempini et al., 2004; M. L. Henry & Gorno-Tempini, 2010). Histopathologically, left posterior perisylvian temporo-parietal atrophy/hypometabolism is evident in the logopenic variant (Beeson et al., 2011; Marshall et al., 2018; Taylor et al., 2009a). Individuals with svPPA have anomia, single word comprehension deficits, and loss of semantic information. The first symptom of semantic memory deficiency is usually a deterioration in single word comprehension, followed by a deterioration in recognizing people and objects (Marshall et al., 2018). Patients with svPPA are fluent in daily speech, but repetition is avoided (Rahul & Joseph Ponniah, 2019). Histopathologically, svPPA cases are usually associated with anterior temporal lobe atrophy/hypometabolism (left greater than right) (Hodges et al., 2004; Mummery et al., 2000). In nf/avPPA, whose main clinical features are agrammatism in language production and/or quality of halting and effortful speech, apraxia of speech is usually observed as the first manifestation of the disease (Croot, 2018; Gorno-Tempini et al., 2004; Olney et al., 2017). When patients are asked to choose between alternatives such as yes/no or he/she, they often give the wrong answer, which they then self-correct (Warren et al., 2016). In nfvPPA, there are abnormalities in the left posterior frontal and insular cortex (Josephs et al., 2006; Marshall et al., 2016; Nestor et al., 2007). Patients with this variant have speech sound errors, altered prosody, anomia, and complex sentence comprehension impairment due to difficulties in motor speech planning (Gorno-Tempini et al., 2004; Mesulam, 2003; Tee & Gorno-Tempini, 2019).
Due to the lack of effective pharmacological treatments for the treatment of PPA, there is increasing interest in behavioral interventions that focus on specific speech/language deficits. These interventions include interventions for deficits such as agrammatism, anomie, phonological working memory, and apraxia of speech, and functional interventions such as compensatory strategies and environmental modifications (Machado et al., 2021). Although most studies report positive results, most of the evidence consists of case studies or series (Carthery-Goulart et al., 2013; Croot, 2018). Since there is no consensus on the types and duration of interventions, randomized controlled studies with larger samples are needed to increase the level of evidence. Therefore ideal is speech-language therapy tailored to the needs of the individual with PPA (Murray et al., 1998). Therefore, restitution and compensatory treatments should include communication partner support and environmental modifications (Schaffer & Henry, 2021). Treatment may also be intertwined with speech-language therapy to target neuropsychiatric and psychosocial sequelae with complementary approaches such as counseling and care partner training (Schaffer & Henry, 2021).
Since one of the most important problems in PPA is language difficulties, it would be helpful for patients to benefit from speech and language therapy (SLT) services. Research-proven speech and language therapy interventions for patients with PPA are extremely rare and are usually limited to naming therapies because word-finding difficulties are common (J. D. Henry et al., 2012; Jokel et al., 2006). However, naming therapies are not usually the main limitation in communicative function in people with PPA. Therefore, interventions to address real-world communication function and interventions to support families/caregivers through conversation are needed (Volkmer et al., 2018). To contribute to the creation of evidence to guide effective communication-based interventions in PPA, the researchers worked to develop a communication skills training program for people with PPA and their conversation partners. Recent studies have documented the benefit of corrective and compensatory speech–language interventions for PPA (Cadorio et al., 2017; Carthery-Goulart et al., 2013; Cotelli et al., 2020; Volkmer et al., 2020a). SLTs in particular have been shown to play an important role in supporting people with PPA (Marshall et al., 2018).
There are insufficient studies on interventions for PPAs in Turkey. This study will contribute to increasing the awareness of SLTs in Turkey about PPAs and standardizing the therapy method applied.
Literature Review
Numerous studies have been conducted recently on the importance and benefits of speech language therapy for individuals with PPA (Machado et al., 2021; Suarez-Gonzalez et al., 2021). Evidence from studies has revealed that both restorative and functional interventions are necessary to improve communication skills in individuals with PPA (M. L. Henry et al., 2019; Machado et al., 2021; Suarez-Gonzalez et al., 2021). Restitution intervention approaches are used to regain lost skills of individuals with PPA. The most popular of these is the lexical retrieval therapy. For functional communication, treatment approaches aiming to improve the ability of the individual with PPA to function in their daily lives are used. These approaches include activities that families and caregivers participate in and that focus on keeping individuals with PPA involved in daily tasks or situations. The main desired improvement for SLTs and individuals with PPA is improvement in functional communication. It is therefore the central focus of collaborative goal setting (Volkmer et al., 2020b).
Despite increasing evidence that speech-language interventions are beneficial, the frequency of referrals for speech and language services for individuals with PPA is still not as expected. There are several possible reasons for this; (1) continuing skepticism about the value of speech and language therapy in the context of neurodegeneration, (2) lack of awareness of the role of SLT among the referrers, (3) the scarcity of SLTs specialized in the treatment of individuals with PPA, (4) and the existence of factors preventing access to face-to-face speech and language services, such as geographical barriers and economic situation (Taylor et al., 2009b; Volkmer et al., 2020a).
There are few studies on access to speech and language services for individuals with PPA in different countries. In a recent survey of 579 SLTs on aphasia rehabilitation, it was reported that the main goal of 74% of SLTs was to maintain or increase quality of life (Hilari et al., 2015). Similarly, it was documented that 97% (n = 173) of SLTs in the U.K. found the psychosocial approach important or very important in the management of patients with aphasia (Brumfitt, 2006). A study by Sekhon et al. (2015) in Australia revealed that 98% (n = 111) of SLTs can contribute to psychological well-being. It has been reported that 66% of Australian SLTs provide psychological counseling either frequently or very frequently (Rose et al., 2014). In another online survey, most respondents stated that more than half of their clients experienced psychological distress. Although 93% of respondents agreed that SLTs play an important role in the client’s psychological well-being, only 42% felt confident in addressing psychological needs. It was observed that the main barriers to this were time/workload pressure (72%), feeling inadequate/lack of education (64%), and lack of continuous expert support (61%) (Northcott et al., 2017).
Many SLT’s (Msc) report that they prioritize communication skills training in people with PPA (Kindell et al., 2015; Volkmer et al., 2018). In a recent study, it was observed that people with semantic PPAs develop successful speech with the use of facilitating behaviors by their families/caregivers (Taylor-Rubin et al., 2017). A randomized controlled trial is being piloted to support SLTs in providing communication education to people with PPA and their families (Better Conversations with PPA) (Volkmer et al., 2018). Kindell et al. (2015) introduced the idea of carer-focused person-centered dementia care in their study. In 2018, E. J. Rogalski and Khayum (2018) implemented a person-centered approach to facilitate their clients’ participation in their daily activities. In a survey conducted by Volkmer et al. (Volkmer et al., 2019), 84.8% of SLTs surveyed reported that they always or often choose communication partner training for family and caregivers. Considering that language difficulties are at the core of PPA and there are studies showing that meeting with SLTs improves the quality of life of people with PPA, it would be beneficial to refer people with PPA to SLTs. However, there are reports in Germany (Riedl et al., 2014) and Australia (Taylor et al., 2009b) that people with PPA rarely consult with SLTs. However, little is known about care pathways available to individuals with PPA and current barriers to accessing speech and language services in Turkey. Therefore, this study aims to answer the following research questions:
Materials and Methods
In this study, a questionnaire was developed to investigate the assessment and intervention areas of SLTs working in Turkey with at least a bachelor’s degree in speech and language therapy and working with at least one PPA patient. Ethics committee approval was obtained from Bahçeşehir University Scientific Research and Publication Ethics (Desc. N.: E-20021704-604.02.02-46411) for the study.
Participants
The survey was on a voluntary basis, all participants signed the informed consent form before answering the questionnaire. Between October 1, 2022 and December 1, 2022, survey questions were sent online to SLTs (n = approximately 1,500) wotking in Turkey and registered in the professional registry. The power of the study was determined using the G*Power (G*Power 3.1.9.2, Duesseldorf, Germany) package program (Faul et al., 2007). Power analysis was performed in sample selection; Type 1 error rate was calculated as α = .05 and type 2 error rate β = .20, power of the test 1- β = .80 and effect size 0.25. In line with this information, it was shown that at least 159 individuals should be included in the study. The study included 265 SLTs who have at least a bachelor’s degree in speech and language therapy, were working in a related field, and had experience working with at least one PPA patient. SLTs who had no experience of working with people with PPA were not included in the study.
Working Procedure
Electronic permission was obtained from Dr. Anna Volkmer for the survey to be used in the study. The original version of the survey was translated into Turkish by two academic SLTs and a linguist with good command of English. The Turkish version of the survey was then backtranslated back into English by a certified translator. After it was determined that the survey was compatible with the original, a pilot study was carried out with 30 people. The pilot study was conducted online, with easy sample selection from individuals meeting the inclusion criteria. The survey was then made available to SLTs online for two months.
Survey Questions and Analysis
The Current Practice Evaluation Survey was developed by Anna Volkmer et al. (2019) as a comprehensive and versatile measure to identify current applications of SLTs to PPA. There are open-ended and multiple-choice questions in the questionnaire, which consists of five sections and 32 items. In the survey, the questions were grouped as “clinical background,”“number, type, and source of patients,”“time spent on management of people with PPA,”“specific assessment and intervention approaches,” and “outcome measures and planning for the future.”
Sociodemographic Information Form and Current Practice Evaluation Questionnaire were shared on platforms with SLTs using the online survey method. The explanations in the consent form were submitted for the approval of the participants at the beginning of the online survey, and an online survey was conducted for the individuals who agreed to participate in the study. The final survey is reported in Supplemental Appendix S1. Survey data were collected and stored confidentially online using the database management system Qualtrics (Version March 2020, Qualtrics, Provo, UT, USA).
NCSS (Number Cruncher Statistical System) 2020 (Kaysville, Utah, USA) program was used for statistical analysis. Descriptive statistical methods (mean, standard deviation, median, frequency, percentage, minimum, maximum) were used for evaluating the study data. Fisher-Freeman-Halton exact test was used to compare qualitative data. Statistical significance was accepted as p < 0.05.
Results
The demographic data of 285 respondents participating in the study are shown in Table 1; 76.8% (n = 219) of the participants were female and 23.3% (n = 66) were male. Of the SLTs surveyed, 35.1% (n = 100) had a Bachelor’s degree, 62.8% (n = 179) had a Master’s degree, and 6.1% (n = 6) had a Doctorate degree; 58.9% (n = 168) of the surveyed SLTs had 1 to 2 years of professional experience, 35.8% (n = 102) had 3 to 4 years of professional experience. Of the participants, 46% (n = 131) were working at the University application and research center, 20% (n = 57) were working in the Public hospital, and 16.8% (n = 48) were working in the Private Counseling Center.
Demographic Information of the Respondents.

Note. ENT = ear nose throat.
More than one option is marked.
Number of Patients, Variants, and Distribution of Characteristics
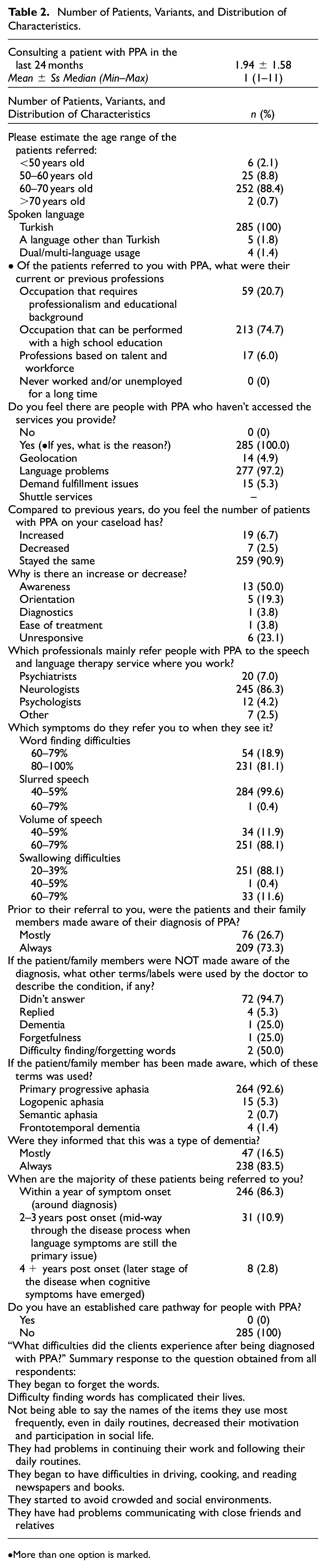
The characteristics of PPA patients are given in Table 2. The number of patients diagnosed with PPA encountered by the respondents in the previous 24 months ranged from 1 to 11, and the mean number was 1.94 ± 1.58; 84.4% (n = 252) of the patients were between 60 and 70 years old, 8.8% (n = 25) were between 50 and 60 years old, six (2.1%) patients were younger than 50 years old and two (0.7%) patients were older than 70 years. While all of the patients could speak Turkish, five patients could speak a language other than Turkish, and four patients could speak two or more languages other than Turkish; 74.7% (n = 213) have a profession that can be practiced with high school education, 20.7% (n = 59) have a profession that requires professionalism and educational background, and 6.0% (n = 17) have professions based on talent and workforce. Neurologists had referred 86.3% (n = 245) of individuals with PPA, 7.0% (n = 20) psychiatrists, and 4.2% (n = 12) psychologists referred to SLTs. The reasons why individuals with PPA could not reach SLTs were language problems in 97.2% (n = 277), geographical reasons in 4.9% (n = 14), and demand fulfillment problems in 5.3% (n = 15). Before being referred to the respondents, 73.3% (n = 209) of the clients and their families/primary caregivers had been informed about the diagnosis of PPA; 92% (n = 264) of the respondents to the question “Which of these terms would you use to patients if the patient/family member was informed about the diagnosis before?” stated that they used the term PPA; 86.3% (n = 246) of the respondents stated that the majority of PPA patients were referred to them within 1 year (with a diagnosis) after the onset of symptoms. All respondents stated that they did not create a special therapy process for their clients with PPA and that they utilized the therapy processes used in classical aphasia.
Number of Patients, Variants, and Distribution of Characteristics.
More than one option is marked.
“What difficulties did the clients experience after being diagnosed with PPA?” the most common answers given to this question included “they began to forget words,”“difficulty finding words has complicated their lives,”“the fact that they could not say the names of the items they used most frequently decreased their motivation and participation in their social life,”“they had problems in continuing their work and following their daily routines”“they began to have difficulties in driving, cooking, and reading newspapers and books,”“they started to avoid crowded and social environments,” and “they have had problems communicating with close friends and relatives.”
Time Spent on Management of People With PPA
The answers regarding the time spent in the management of PPA patients is shown in Table 3; 99.3% (n = 283) of the respondents stated that they did not set a limit on how long individual therapies would last with patients after the diagnosis of PPA, and 94.7% (n = 268) of them stated that they performed more than six interventions.
Time Spent on Management of this Patient Group.

More than one option is marked.
“Please estimate how many sessions you spend on the following when working with patients with PPA and / or their families.” When answers to this question were examined, 94% (n = 268) of the respondents planned one intervention for direct language and communication assessment, and 6% (n = 17) of the respondents planned two or more sessions; 2.1% (n = 6) of the respondents planned one intervention for swallowing evaluation, and 90.2% (n = 257) of the respondents planned one intervention to contribute to the diagnosis of PPA (variant determination). It was determined that all respondents (n = 285) planned two or more interventions for functional interventions to support communication. For swallowing disorders, 2.5% (n = 7) of the respondents planned one intervention and 0.4% (n = 1) planned two interventions; 88.4% of the respondents (n = 280) planned one intervention for education/information for the family, and 1.8% (n = 5) of the respondents planned one intervention for the training/information intervention for employees. For language and communication-oriented intervention that requires joint participation with patients and their families/caregivers or friends, 91.9% (n = 262) of the respondents planned one intervention and 1.4% (n = 4) planned two or more interventions; 88.1% (n = 251) of the respondents did not plan an intervention for cognitive status assessment, 98.9% (n = 282) of the respondents did not plan an intervention for the case analysis meetings and meetings with other units, and 99.6% (n = 284) of the respondents did not plan an intervention for group therapy.
“If you are providing functional interventions to support communication, in what setting do you think they would ideally take place?” Respondents answered 1.4% (n = 4) inpatient treatment, 96.8% (n = 276) outpatient treatment, and 1.8% (n = 5) home care to this question. The average number of interventions performed by the respondents to support the functional communication of patients with PPA was 16 ± 5 (range, 8–30).
Frequency of Using Assessment Tools When Working With Patients With PPA
“How often do you use the following assessment tools when working with patients with PPA?” When looking at the answers to this question; 71.6% (n = 204) of the respondents stated that they always use Language Assessment Test for Aphasia, 92.3% (n = 263) of the respondents stated that they always use interviewing the patient or his/her family regarding the patient’s medical history/communication and personality traits, and 81.1% (n = 231) of the respondents stated that they always use observing or evaluating functional activities and communication features. In addition, 92.3% (n = 263) of the respondents stated that they never used the Mini Mental Test, 81.1% (n = 231) of the respondents stated that they never used the Pyramid Palm Trees Test, and 43.3% (n = 123) of the respondents stated that they never used the Social Life Participation Scales (Table 4).
Distribution of Questions Regarding Evaluation and Therapy Methods.
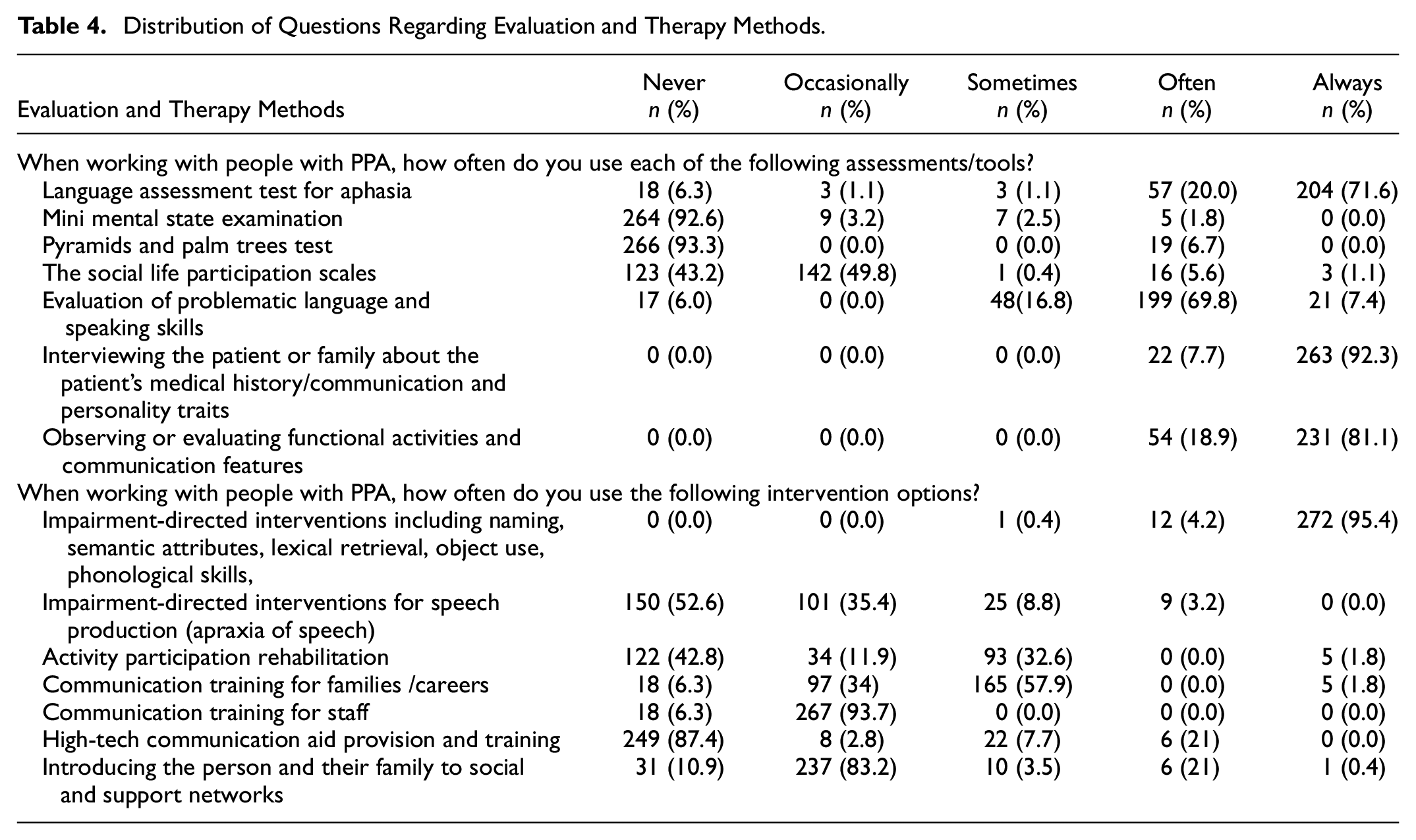
“How often do you use the following therapy modalities when working with patients with PPA?” 272 (95.4%) respondents stated that they always used the disorder-based intervention method used for their phonological skills, naming, semantic studies, word recall, and functional word choice; 93.7% (n = 267) of the respondents indicated that they rarely use functional communication training for employees, 83.2% (n = 237) rarely use the method of creating social and supportive environments for patients and their families, 57.9% (n = 165) sometimes use the functional communication training method for families and caregivers; 52.6% (n = 150) of the respondents stated that they never used disorder-based interventions for apraxia of speech, 42.8% (n = 122) activity-based studies and functional communication activities, and 87.4% (n = 249) advanced technological supportive assistance training (Table 4).
Outcome Measures and Planning for the Future
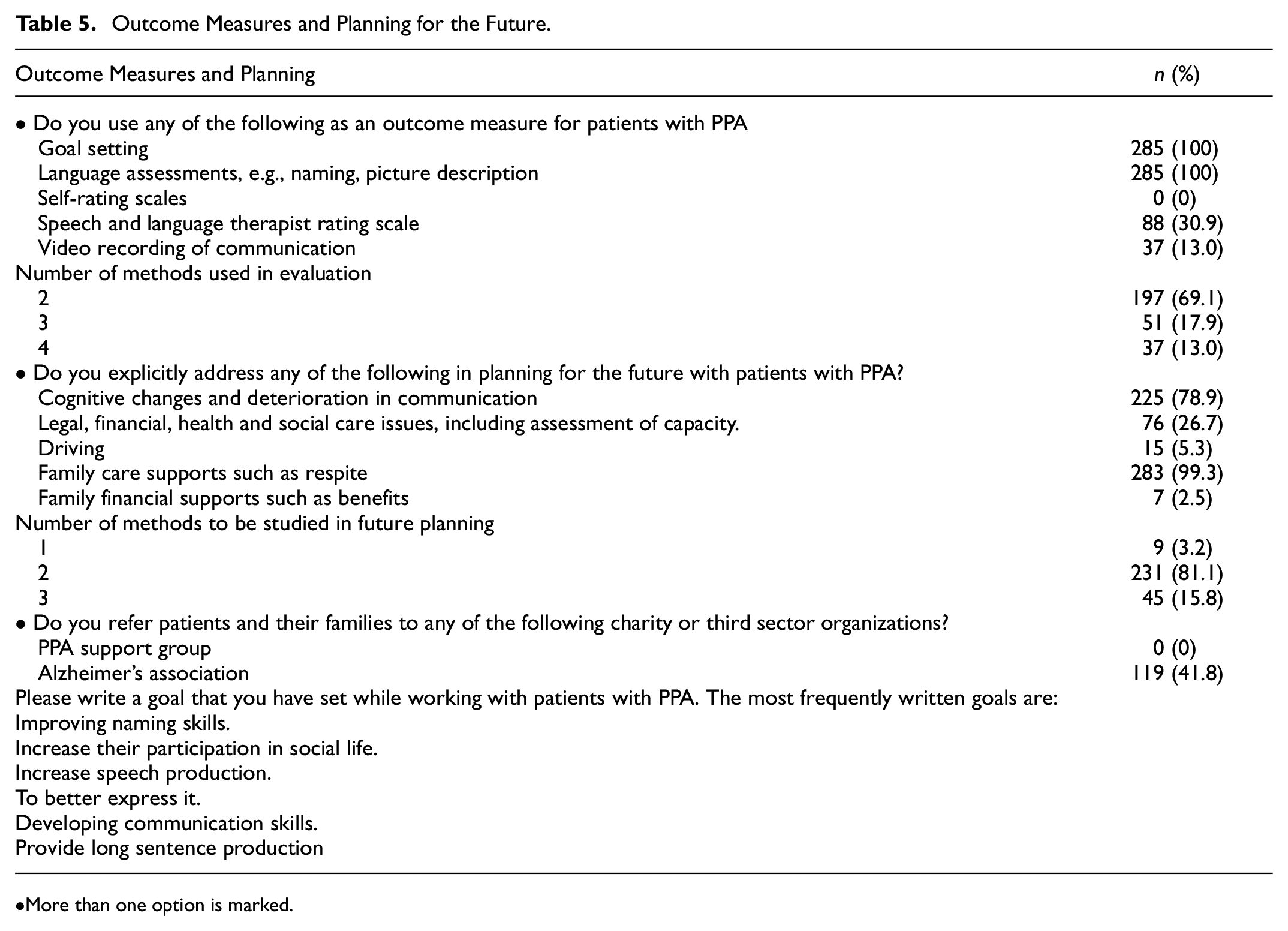
When the methods used by the respondents in the evaluation of patients with PPA were examined, all respondents (n = 285) stated that they used goal setting and language assessments, 30.9% (n = 88) used informal assessment scales of speech and language therapists, and 13% (n = 37) used video recordings during intervention (Table 5).
Outcome Measures and Planning for the Future.
More than one option is marked.
“Which of the following do you think should be worked on in future planning with patients with PPA?” When asked this question, 78.9% (n = 225) of the respondents indicated that cognitive changes and deterioration in communication, 26.7% (n = 76) legal, financial, health, and social care issues, 5.3% (n = 15) driving, 99.3% (n = 283) care support, and 2.5% (n = 7) financial support should be worked on (Table 5).
To the “Do you refer patients and their families to any of the following charity or third sector organizations?” question, 119 (41.8%) of the participants stated that they referred individuals with PPA to the Alzheimer’s Association. (Table 5).
“Number of methods to be studied in future planning?” When asked this question, 81.1% (n = 231) of the participants indicated that two, 15.8% (n = 45) three and 3.2% (n = 9) one. (Table 5).
The most common answers given by the participants to the question “Write one of the goals you have set while working with patients with PPA”were increasing naming skills, increasing participation in social life, increasing speech production, enabling better expression, improving communication skills, and providing long sentence production (Table 5).
Discussion
This study was conducted to determine the current practices of SLTs working in Turkey for PPA. The results of the survey identified current usage patterns for SLTs serving in Turkey, general demographics, characteristics of patients with PPA, the most common assessment and intervention tools used by SLTs in Turkey, available care pathways, referral resources, and barriers to services. Thus, the results of this study include recommendations for both raising awareness about PPA and improving the care of individuals with PPA.
Two-hundred eighty-five SLTs participated in the survey; 58.1% of the surveyed SLTs had 1 to 2 years of clinical experience, and 35.8% of them had 3 to 4 years of clinical experience. Since the majority of SLTs participating in the survey have a maximum of 1 to 4 years of experience, we can say that awareness in this area has recently emerged in Turkey. In addition, the fact that 62% of the surveyed SLTs have a Master’s degree indicates that SLTs make efforts to improve themselves academically. The low number of SLTs with PhDs also thinks that SLTs have recently received their master’s degree, but have not yet completed their doctorate; 46% of the surveyed SLTs were working in rehabilitation centers and SLTs were distributed close to each other in all geographical regions of Turkey. As this survey study was conducted to determine the interventions of SLTs in patients with PPA, all of the SLTs surveyed had previously colsulted patients with PPA. In a survey conducted in Italy, 58.3% of the 336 SLTs surveyed stated that they do not consult individuals with PPA (Battista et al., 2023). However, in our study, there is no data on how many of all SLTs counsel individuals with PPA.
Patients with PPA are often poorly referred to speech and language services. Moreover, these referrals usually occur a few years after the onset of the disease. This delay between symptom onset and referral to intervention services makes it difficult to implement a comprehensive treatment plan. Similar to previous studies, in our survey study, SLTs stated that individuals with PPA were mostly referred by neurologists; 90.9% of the surveyed SLTs stated that the number of individuals with PPA they consulted did not increase compared to the previous year. This actually agrees with other data showing that there is not enough awareness yet about effective therapies of SLTs in individuals with PPA; 73.3% of the SLTs who participated in the survey stated that they always and 26.7% of them mostly stated that the individuals and family members who were referred to them were aware of their PPA diagnosis before they were referred. In addition, individuals with PPA and their families stated that they were informed that it is a form of dementia. This situation also shows that there is no problem in diagnosing PPA to individuals; 86.3% of surveyed SLTs stated that they were referred to individuals with PPA within 1 year of their diagnosis. In our study, all of the SLTs surveyed stated that individuals with PPA somehow had barriers to accessing speech and language therapies; 97.2% of the barriers for individuals with PPA to access speech and language therapies were due to language problems, 5.3% to demand fulfillment issues, and 4.9% to geographical reasons. The fact that the most common barrier is language problems may possibly be an indication that individuals with PPA are diagnosed late and that speech and language impairment is progressing. The second most common barrier demand fulfillment issues point to the lack of awareness that SLTs provide effective therapy in the treatment of individuals with PPA. Geographic barrier can be eliminated by using alternative treatment methods such as teletherapy in individuals with mild to moderate PPA. Survey results in Australia, Germany, the United Kingdom and Italy revealed barriers to accessing SLT services. These barriers are lack of experienced SLTs, lack of awareness of the role of SLTs, and geographic barriers. The results of the survey we conducted in Turkey are also similar to the results of previous studies.
“What difficulties did the clients experience after being diagnosed with PPA?” response to the question obtained from all respondents, it is seen that the individuals with PPA and their family relatives actually apply to the physician after the disease has progressed for a while and mostly when they start to have difficulties in daily routines. Since PPA awareness is still low in the community, patients and their relatives became aware of the disease after a while after the symptoms progressed. Although it has been reported that individuals with PPA are referred to SLTs within 1 year of onset of symptoms, in fact, this period is probably longer because the patient and their relatives are late realizing the disease.
With the studies conducted in recent years, awareness has been raised about patients with PPA. However, despite the research studies that have been done, the evidence base for non-pharmacological treatment is insufficient (Roberts et al., 2022). There is little literature on the management of speech and language symptoms in people with PPA, and the bulk of these studies were impairment-focused interventions such as word retrieval (Carthery-Goulart et al., 2013). The reason why there is still no complete agreement between studies and clinical practices is that the needs of people with PPA are not fully understood and traditional methods continue to be applied in speech and language therapy (E. J. Rogalski & Khayum, 2018). Having clear and evidence-based care pathways is very important for standard care (Seys et al., 2017). There is no generally accepted care pathway for people with PPA or frontotemporal dementia. Therefore, it can be difficult to provide best practice care for people with PPA with the involvement of SLTs. In studies with SLTs, the most popular assessments of individuals with PPA have been observed to be informal interviews, functional observation, and the stroke aphasia language series. SLTs in the U.K. report that they prefer functional communication interventions when working with the PPA patient group (Volkmer et al., 2018). All of the SLTs participating in the survey stated that they do not have a specific therapy method for individuals with PPA. According to the results of the survey, classical aphasia therapy is applied to individuals with PPA; 94.7% of surveyed SLTs apply at least six therapy interventions. The majority of SLTs stated that they used the Language Assessment Test for Aphasia, while the majority of SLTs stated that they did not use Mini Mental State Examination and Pyramids and Palm Trees Test. The vast majority of SLTs always interview to their relatives about the patient. Similar to the results of previous studies, 95.4% of the surveyed SLTs stated that they always use impairment-directed interventions such as “naming, semantic attributes, lexical retrieval, object use, phonological skills”. However, most of the SLTs surveyed stated that they do not perform interventions for speech production (apraxia of speech), activity participation rehabilitation, communication training for staff, high-tech communication aid provision and training and introducing the person and their family to social and support networks. In addition, nearly half of the respondents (40%) stated that they referred patients and their families to any non-profit or third sector organizations. This probably reflects the lack of cooperation between relevant organizations and SLTs.
The results from the studies done so far show the necessity of maximizing the efficient use of speech and language therapy services. Therefore, all healthcare providers should be educated about the potential benefit of speech and language therapy for people with PPA, and evidence-based speech and language therapy clinical practice guidelines should be developed for the care pathway for PPA. Online free therapy resources should be provided, such as the currently implemented “Better Conversations with PPA” (34) package (Volkmer et al., 2018). The “Communication Bridge” intervention, a telehealth service delivery model by Roberts et al., will both provide effective speech-language intervention to people with PPA and evaluate the effectiveness of these interventions (Roberts et al., 2022). The facts that 58.9% (n: 168) of the SLTs participating in the study had 1 to 2 years of experience post-graduation, and 86.3% (n: 246) of patients with PPA were referred to SLTs within 1 year of symptom onset show that there has been an awareness in the Turkey in recent years.
Conclusion
This section includes the major findings of the study, limitations, and recommendations for future research.
Major Findings
In this study, it was evaluated the assessment and intervention practices used by SLT participants in Turkey. Since there is no proven intervention for PPA, it was determined that all participants applied classical aphasia therapy. Patients with PPA are referred to SLTs for short periods of time. Most of the SLTs were recent graduates within 1 to 2 years, and most SLTs have master’s degrees. However, it is very important for all participants to plan functional interventions to support communication and language and communication-oriented intervention that require joint participation with the patient and their family/caregiver or friends.
Limitations
The study has some limitations. The small sample size and the inability to reach all SLTs working in Turkey are an important limitation. In addition, potential biases in survey responses are also among the limitations of this study.
Future Research Directions
Increasing awareness of the benefit of rehabilitation among SLTs and other relevant health professionals through studies can facilitate access to intervention for individuals with PPA. Thus, the daily lives of individuals with PPA and their families can be better supported. In future studies, identifying the perspectives of individuals with PPA will be important to better understand the barriers faced by individuals with PPA. Finally, studies should be conducted on how best to support individuals with PPA and their families. Thus, it will be easier to choose the interventions applied for individuals with PPA and the difficulties experienced by SLTs can be minimized.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440231188928 – Supplemental material for Perspective of Speech and Language Therapists in Turkey on Primary Progressive Aphasia
Supplemental material, sj-docx-1-sgo-10.1177_21582440231188928 for Perspective of Speech and Language Therapists in Turkey on Primary Progressive Aphasia by İbrahim Can YAŞA in SAGE Open
Footnotes
Acknowledgements
I express appreciation to Dr. Anna VOLKMER (University of College London) who supported me to work with PPA with many different perspective and gave permission to use the survey. I would like to thank all the speech and language therapists who participated in the survey. I would also like to thank Yiğitcan PERKER who assisted in the electronic management of the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics committee approval was obtained from Bahçeşehir University Scientific Research and Publication Ethics (E-20021704-604.02.02-46411) for the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.