
Abstract
Since the medical reform implemented by the Chinese government in 2016, more attention has been paid to family doctors and the key role they play in safeguarding citizens’ health. Therefore, it is necessary to explore the factors that affect the motivation of family doctors to provide contracted services. In this study, factors influencing the motivation of family doctors to provide contract services are divided into intrinsic motivation and extrinsic motivation. Intrinsic motivation includes family doctors’ sense of professional belonging, occupational motivation, and occupational efficacy, while extrinsic motivation includes the attraction, support, and promotion of contract services, as well as pressure from government and community health service institutions. And the environment in which family doctors operate during their contracted services. The questionnaire was designed with a sample size of 536 family doctors in Jiangsu Province using logical reasoning method. Stata16 software is used for empirical analysis using linear regression method. The empirical analysis is conducted using the linear regression method. A family physician’s motivation is categorized into two perspectives: intrinsic and extrinsic motivation. Significant findings unveiled that; (i) Family physicians’ sense of professional belonging (β = .026, p < .01), professional motivation (β = .076, p < .05), and professional efficacy (β = .148, p < .01) had a significant positive on their contract services, (ii) Promotion (β = .085, p < .01), the attractiveness of family physicians’ contract services (β = .092, p < .01) and contract service support (β = .137, p < .01) showed a positive effect, whereas (iii) intense pressure (β = −.079, p < .01) experienced by family physicians could negatively affect their contract services. Among the intrinsic and external factors, only intense pressure negatively affects family physician contracted services. This finding indicates that decision-makers should adopt feedback mechanisms at the various health levels to encourage workers to measure motivational levels and output themselves.
Background
As countries worldwide strive to achieve the Sustainable Development Goals, the vital role of the health workforce must be recognized (Zhang et al., 2019). Due to this, the Chinese government, in 2009, proposed a new medical reform plan, which emphasized improving the medical services at community centers as one of the most important goals of the medical reform plan (The Central People’s Government of the People’s Republic of China, 2009). In 2011, the State Council issued the “Guiding Opinions on establishing a General Practitioner System” (The Central People’s Government of the People’s Republic of China, 2011). It proposed the establishment of a general practitioner system that is hierarchical and suitable for Chinese nationals.
In China, the general practitioner, often known as the family physician, is meant to promote health care, and bidirectional consists of specialized care between primary and secondary or tertiary institutions. Implementing a family physician system is an effective strategy for increasing the utilization of Community Health Centers (CHCs) and achieving new medical reform goals. The family physician system is an important measure to construct a hierarchical diagnosis and treatment system, which can guide patients at the grassroots level for treatment, thereby promoting the efficiency of medical and health resources utilization (Huang et al., 2018; Zhao et al., 2017). It is different from the western family doctor system. Chinese family physicians mainly focus on the elderly, infants, and pregnant women, providing health management and education with less attention on door-to-door services.
General physicians, nurses, and public health professionals from the family physician teams sign contracts every year according to the wishes of residents. Health records, frequent physician exams, health management, clinical care, follow-ups, and referrals are all provided by the team (World Health Organization, 2010).
The system of family physicians is often considered the core of primary healthcare, which is the first level of professional care provided to populations without restrictions on access and addressing the health need of the majority of the citizens. In many countries, patients usually receive primary healthcare from general practitioners. According to the connotation of the contracted services of family physicians, family physicians can not only provide medical services but also provide corresponding nursing services. The family doctor system reduces hospitalization costs and provides more effective and equitable care (Shang et al., 2019). Hence it can save healthcare resources by managing medical cases, producing positive net benefits for patients (Fleming et al. 2000).
Currently, family physicians in China are primarily community physicians (Li et al., 2017). The healthcare system service delivery and professional title evaluation focus on the clinical specialist model (Jing et al., 2015; Maignan et al., 2009; Meng et al., 2009). The Chinese state council published recommendations in September 2015 pushing for developing a graded diagnostic and therapeutic system, indicating the need to develop general practitioners’ talent teams.
It has examined the elements influencing residents’ decision to contract with family physicians (Feng et al., 2020; Zhang et al., 2019). They discussed the difficulties inherent in developing a family physician system (Lu et al., 2016; Zhang et al., 2013) and examined community attitudes toward family physicians in China (Huang et al., 2018). Scholars also emphasized the importance of developing a stable relationship with the family physician’s contracted services (Hou et al., 2014; Shang et al., 2019). They empirically investigated family physician contract services awareness in Zhejiang province. They discovered that both the awareness rate and contracting rate of family physician contract services are undesirable among the inhabitants. As a result, it was advised that the government should increase public awareness of family physician contract services, extend coverage, provide customized contract schemes to satisfy the needs of various groups, and stimulate the development of family physician contract services.
Several research projects have been carried out to evaluate the effect of the family physician-patient contract. Still, most have focused on comparing agreement and non-contract patients on, for example, blood pressure or blood sugar control or the corresponding patient satisfaction and treatment compliance (Chen et al., 2019; Zhang & Wang, 2018; Zhao et al., 2017). Some scholars have also pointed out that motivation significantly impacts service performance (Rong, 2018; Xiaoyang, 2017). However, while the professional Self-image of family physicians has already been the subject of scientific investigation (Natanzon et al., 2009), there has been little scientific research about the image of family physicians from the perspective of their specialized colleagues.
Improving workers’ performance has gained attention, especially in the public sector (Gould-Williams, 2003).To the best of our knowledge, a handful of research has been conducted on the role of motivational factors contributing to family physician’s contract services (Jing & Fang, 2020; Li et al., 2019). These are thus worth exploring for research and policy purposes. The study, therefore, aims to specifically investigate the several impacts of motivational factors affecting family physician contract services in Jiangsu province. Contributive, most previous literature assessed the individual effects of motivational factors in one model. Still, this study, unlike others, employed a multiple linear regression model to determine the motivational factors affecting family physician construct services. We aim to identify the role of motivation that affects family doctor-patient choice in Jiangsu province. Our findings may catalyze to improve healthcare system delivery in China.
The key to achieving corporate objectives of delivering quality health care, fulfilling consumer needs, and achieving the Sustainable Development Goal (SDG 3) is improving the motivation and performance of health workers (Willis-Shattuck et al., 2008).
Motivation is one of the driving forces among health workers that can potentially contribute to progress toward achieving the WHO health system goals, which include increased health level and equity, sensitivity to reviewing clients’ non-medical expectations, protection from socioeconomic risk, and increased efficiency (Maslow, 2013; World Health Organization, 2007). The importance of investing in health workforce motivation is emphasized in the global conference on primary health care 2018 (Muthuri et al., 2020; World Health Organization and the United Nations Children’s Fund [UNICEF], 2018) and the World Health Association reports (Maslow, 2013; Willis-Shattuck et al., 2008; World Health Organization, 2007).
Motivation is the power for an action that subjects an individual to positive behavior or a factor that encourages a change of cause movement to ensure action efficiency (Parasuraman et al., 1985). In the 1950s, service motivation was concerned with the discipline of public management. It was believed that the service motivation of members or individuals of public organizations could become a sufficient force to promote shared services (Teng ya, 2013; Wang et al., 2017). The family physician system is a crucial system currently promoted by the Chinese government. It ensures that the new family physicians implement comprehensive, continuous, practical, and appropriate medical care services. An indication that family physicians have contracted services to perform their rules based on specific policy guidance. However, the unstable development of medical and health resources in the urban and rural areas, and inadequate system and mechanism, to an extent, this has restricted the implementation of family physician contract service (Fang Huiying et al., 2018; Lin Feng et al., 2017; Pu Xiaoying et al., 2017; Reitz et al., 2018; Zhang Yimin et al., 2018). Therefore, the study explores the motivation of family physician contract service within the Jiangsu province of China. According to Afful-Broni (2012), there are two types of motivation: intrinsic and extrinsic motivation. Intrinsic motivation means performing a task that is inherently interesting or enjoyable (Ryan & Deci, 2000).
The intrinsic motivation for family physicians’ contract service mainly comes from their attitude, which is the activity and process of directly promoting family physicians to carry out contract service. Among them, the sense of professional belonging refers to the input of the family physician’s contract service content, mode, and requirements, as well as the pursuit and degree of the family physician’s contract service value and ideal. Career motivation refers to the role played by family physicians in providing relevant health examinations and health education, which enables the community residents to develop a healthy lifestyle and realize their self-worth. Professional efficacy refers to level of trust and self-confidence in their professional skills, professional quality, organization and coordination, and communication.
Extrinsic motivation includes an activity to obtain an outcome, such as incentives, salaries, and other tangible rewards (George et al., 2005). Among others, extrinsic motivation is constituted by motivating factors to mobilize their service enthusiasm, including guidance. This also includes cultivating skills and literacy related to the family physician’s contract service, guaranteeing performance rewards, welfare benefits, and professional title promotion channels. In addition, community residents’ awareness and trust in family physicians’ service goals, service content, and service capabilities will stimulate their service motivation to a certain extent. The support of family physician contract service mainly includes the policy support made by the government, community health service institutions, and spiritual assistance from community residents. The promotion of family physician contract service is a series of rules and management factors that the government and society supervise and restrict family physicians from carrying out responsibilities. It mainly includes norms and codes of conduct, performance evaluation, reward and punishment, and community residents’ independent supervision. The pressure on family physicians employed for services mainly stems from the stress response caused by their working environment and nature, including the ability to meet work needs, excessive workload, the influence on opinion, and residents’ trust.
Methods
Data Source
Jiangsu Province started the pilot family physician contract service since 2013. It has innovated in practice and developed in innovation. After promoting urban and rural planning and the “single point” signing, it has formed a family physician signing service system with the signing of the first diagnosis at the grass-roots level as the main body. A total of 13,000 family physician teams were set up in the province. In 2020, the signing rate of permanent residents was 40.31%, and the signing rate of key groups was 74.63%, of which the signing rate of primary care was 20.12%, and the renewal rate was 90%. The proportion of business income directly related to signing services increased steadily, with a maximum of more than 30%. The overall satisfaction of signing targets and family physicians exceeded 90% and 80%.
The paper focuses on the connotation of family physicians’ contract service motivation and designs the corresponding questionnaire using the literature research method, Delphi method, and expert consultation method. A structured questionnaire in Chinese was created using eSurvey Creator, an online survey creation tool. The study participants were chosen solely based on their availability and willingness to participate in the survey. This study relied on responses from family physicians to the survey question. Additionally, the questions posed were closed-ended to prevent the possibility of bias in the responses. The surveys were delivered via social media sites such as WeChat and participants’ emails, with an introduction explicitly describing the survey’s goal and the criteria for becoming a respondent. Respondents were informed that there were no hazards associated with participating in the study.
Additionally, a confidentiality declaration was included to assure responders that their data would not be linked to their identities or other personally identifiable information.
Additionally, respondents were advised that participation in the study was voluntary. If they choose to leave at any stage by exiting the questionnaire, any responses provided up to that point would be retained. The researchers’ contact information was included to allow respondents to contact them directly if they had any additional concerns about the study.
Finally, a checkbox containing the following statement: “The goal and nature of this research have been adequately described, and I accept participating in this study.”“I accept that I may withdraw from the study at any time without penalty,” was offered as a checkbox for responders to indicate their agreement to participate in this study.
Variable Interpretation
Analyzing motivation is complicated due to various contributing factors, both external and internal (Mbindyo et al., 2009). However, the self-designed questionnaire was compiled according to the survey’s intent, based on literature and expert consultation. The survey items mainly covered three parts; (a) demographic information, including age, gender, educational level, title and years of work, and personnel monthly income, (b) intrinsic motivation, and (c) extrinsic motivation. The study identified intrinsic factors which respondents perceived as influencing their contract services. Afful-Broni (2012) asserts that intrinsic motivation provides satisfaction as power, prestige, status, and self-confidence. It includes factors like the sense of belonging; and external esteem factors. The intrinsic motivation of family physicians’ contract service mainly comes from their attitude, which is the activity and process of directly promoting family physicians to carry out contract service, which includes primarily three dimensions of family physicians’ sense of professional belonging, career motivation, and professional efficacy. Among them, the purpose of professional belonging refers to the input of the family physician’s contract service content, mode, and requirements, as well as the pursuit and degree of the family physician’s contract service value and ideal. Career motivation refers to the role played by family physicians in providing relevant health examinations and health education, which enables the community residents to develop a healthy lifestyle and realize their self-worth. Professional efficacy refers to the level of trust and self-confidence of family physicians in their professional skills, professional quality, organization and coordination, and communication.
The extrinsic motivation mainly includes the attractiveness, support, promotion of contract services, pressure from the government, community health service institutions, and the environment practiced by the family physicians during their contract service. Among others, the attractiveness of a family physician’s contract service is constituted by a series of motivating factors to mobilize their service enthusiasm, including the guidance and cultivation of skills and literacy related to the family physician’s contract service, guaranteeing performance rewards, welfare benefits and professional title promotion channels of the family physician’s contract service. Also, community residents’ awareness and trust in family physicians’ service goals, service content, and service capabilities will stimulate their service motivation to a certain extent. The support of family physician contract service mainly includes the policy support made by the government, community health service institutions, and spiritual assistance from community residents. The promotion of family physician contract service is a series of rules and management factors that the government and society supervise and restrict family physicians from carrying out responsibilities. It mainly includes norms and codes of conduct, performance evaluation, reward and punishment, and community residents’ independent supervision. The pressure on family physicians employed for services mainly stems from the stress response caused by their working environment and nature of work, including the ability to meet work needs, excessive workload, the influence of public opinion, and residents’ trust.
Sample
Jiangsu province is one of the pioneers in implementing the family doctor system in China. Therefore, Jiangsu Province is selected as the research area in this paper. Due to the differences in the level of urban economic development and cultural environment in different regions of Jiangsu Province, this paper selected Wuxi, Zhenjiang, Nantong, Taizhou, Yangzhou, Xuzhou, Suqian, and Lianyungang to investigate the different situations in southern, central, and northern Jiangsu Province. According to the principle of random non-equal distance, a total of 600 questionnaires were distributed to family doctors who have worked in primary medical institutions in the above cities for more than 3 years. After removing some questionnaires with incomplete information and inconsistent contents, 536 valid questionnaires were obtained, with an effective recovery rate of 89.3%. The necessary information of the surveyed family doctors is shown in Table 1.
Basic Information of the Family Physicians Surveyed (Unit: Person).

Data Analysis
The raw data acquired via questionnaire distribution is neither helpful or significant until it is transformed into information that can be used to make decisions. The data analysis procedure includes condensing the data to a manageable amount, summarizing it, and making statistical judgments. As a result, the following processes are considered when evaluating the data collected. Except for demographic variables, data relevant to the analysis’s significant components are coded using a five-point Likert scale. Notably, a strongly disagree reaction has an intensity of 1, but a strongly agree response shows that the response was allocated to the response’s strength. Following that, the study assessed the study sample to determine the relationship between motivating factors and teamwork using key component analysis, which reduces the number of variables used to evaluate a certain construct via factor analysis. Finally, the linear regression method investigates the relationship between motivation and family physician construct services. Notably, all data analysis necessary for the technique, as mentioned earlier, is possible utilizing SPSS and STATA 15.0. The following section summarizes the specifics of the statistical approaches employed in the investigation.
Results
The descriptive statistics show that the proportion of female family physicians (67.2%) is significantly higher than that of male family physicians (32.8%). The number of family physicians age 20 to 30 accounted for 48.1%. In comparison, those aged 31 to 40 revealed 19.2%, indicating that the family physicians in Jiangsu Province are relatively young. In terms of educational attainments, family physicians surveyed were mainly composed of Junior College (33.0%) and undergraduate (48.2%) levels. With professional title evaluation, 20.0% were not evaluated, 3.0%, 30.2%, and 16.8% had junior, intermediate, and senior titles. Of the family physicians surveyed, 33.4% had served for 5 years or less, 29.1% had 6 to 15 years, 17.7% had 16 to 25 years, and 17.2% had worked 26 years or more. Concerning the establishment, 48.9% of the family physicians were owners, and 49.8% of the contracted family physicians were employed. Regarding salary, 34.9% of family physicians had a monthly income of less than 3,000 yuan, and 36.6% received 3,001 to 5,000 yuan.
Reliability and Validity
This paper focuses on the intrinsic and extrinsic motivation of family physician’s contract service to improve quality and efficiency. The specific indicators and items are shown in Table 2. The Cronbach α coefficient tests the reliability of the scale. The test results show that the Cronbach α coefficient of all indicators is more significant than .7, implying that the scale’s reliability is good. In terms of the validity test, all the indexes’ factor loads are more important than 0.6, which specifies that the indexes designed in this paper have good aggregate validity.
Description and Measurement of Specific Indicators.

Note. Likert’s 5-point scoring method was used for the scale. The responses of all items were as follows: strongly disagree = 1; disagree = 2; general = 3; agree = 4; strongly agree = 5.
Regression Analysis
Grounded on the Grossman production function theory, this study considers the motivation of family physician contract serves as the output factor and the endogenous and external motivation as the input factor and establishes the model as follows

(1) where H denotes the motivation of family physicians to sign up for service, I represents endogenous motivation, O shows external motivation, X represents other control variables β1, β2, and βi denotes parameters with estimation, µ signifies effects related to individual service motivation, mainly reflecting the influence of some unobservable factors on service motivation.
Table 2 shows the results of the hierarchical regression analysis. Equation 1 examines the relationship between the control variable and the dependent variable. Equations 2 to 4 studied the relationship between professional sense of belonging, professional motivation, and professional efficacy of the family physician’s contracted service. Regarding the influence of the endogenous power, Equations 5 to 8, respectively, investigate the influence of family physicians’ contracted service significance, contracted service support, contracted service thrust, and contracted service pressure on their external motivation.
Variable Description and Descriptive Statistics
Table 3 presents descriptive statistical analysis for the various variables employed in the study. The results show family physicians overall motivation is insufficient when compared with the mean values in Table 3. Therefore, the study further calculates the intrinsic and external motivation of the surveyed family physicians. It is found that family physicians’ motivation in terms of a sense of belonging, career motivation, and occupational efficacy is fair, suggesting that they have low motivation looking at the mean values. The team understands the profession’s importance and service quality and is eager to do better.
Variable Assignment and Descriptive Statistics.
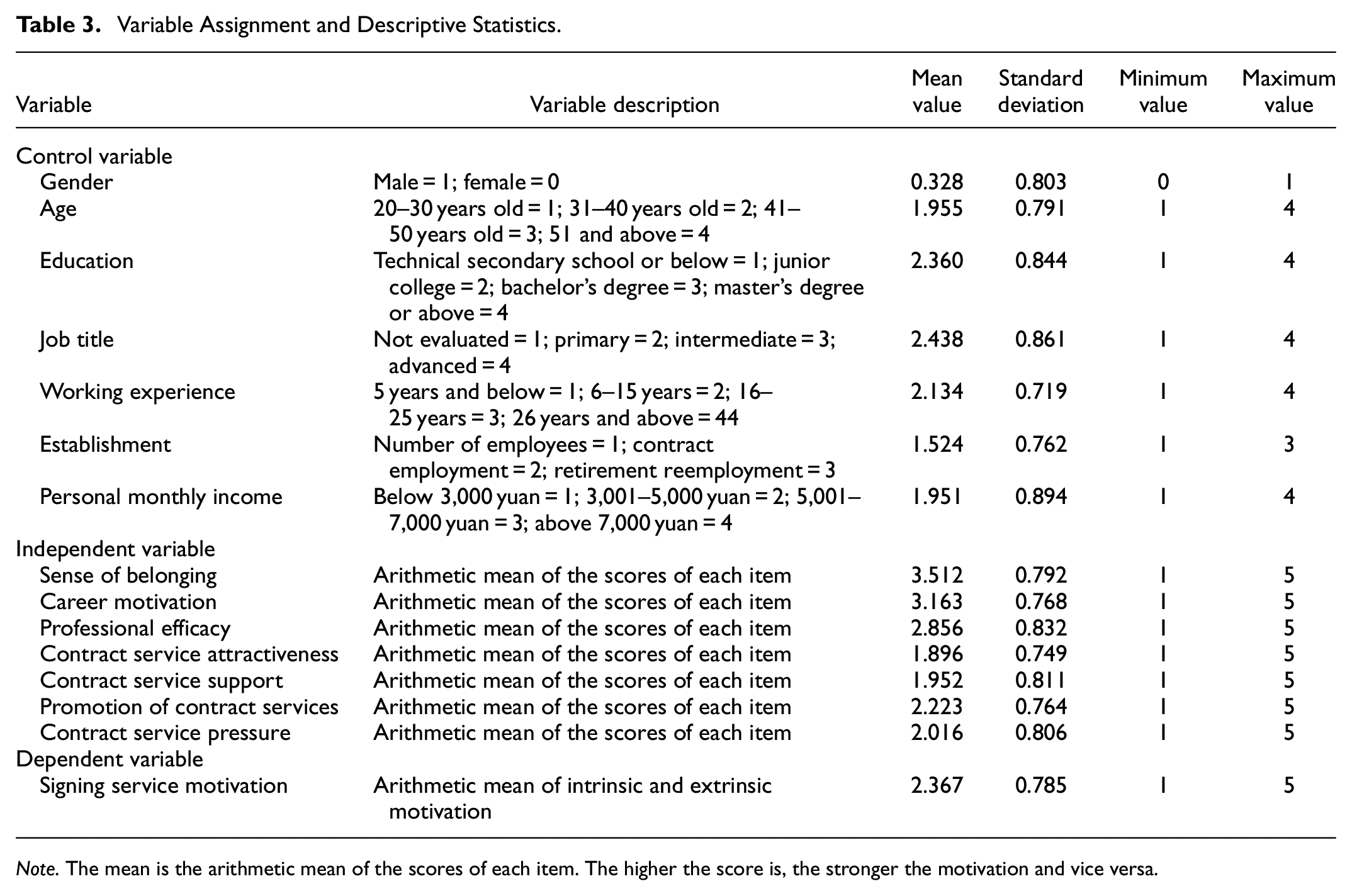
Note. The mean is the arithmetic mean of the scores of each item. The higher the score is, the stronger the motivation and vice versa.
The external motivations of the family physicians surveyed, such as the attraction of contracted services, support of contracted services, push of contracted services, and pressure of contracted services, are generally low. They demonstrate that overall external motivation for family physicians’ contracted services is insufficient and, to some extent, limits their quality of service.
Estimation of Motivational Factors on Family Physician Contract Services
The linear regression method estimates the relationship among constructs formulated in the study. Table 4 gives the findings of the linear regression methods. Hence, the outcome of the regression analysis concerning investigating the effects of social demographic, intrinsic and extrinsic motivational factors on family physicians contract services. The investigation is carried out in eight main stages. The R2 values for each estimated model are evidenced by how well the model is described in the study.
Linear Regression Analysis Results.

Note. ***, **, and * are significant at the statistical levels of 1%, 5%, and 10% respectively.
For the second equation, in addition to the control variables, a sense of belonging between family doctor contract services is introduced. The results of this equation showed that there was a significant positive relationship between family doctors’ sense of belonging and their service motivation (β = .026, p < .01). In addition, age, organization, and personnel’s monthly salary will also affect contract services. In Equation 3, occupational motivation was added to the control variables to test its role in family doctor service motivation. The results showed that occupational motivation had a positive impact on family doctor contract services, and the estimated coefficient β was .076, which was statistically significant at the 5% level. However, only two control variables (age and establishment) were significant, with age showing a positive effect and establishment showing a negative effect on doctors’ contracted services.
The fourth equation combines professional effectiveness and control factors to examine its impact on family physician contract services. It was further found that occupational efficacy had a positive effect on family doctor contract motivation (β = .148, p < .01), while control variables had no significant effect. In terms of extrinsic motivation, the analysis results of Equation 5 showed that when control variables and contract service attraction were added to the equation, the results showed a significant positive correlation between family doctors’ contract service motivation and the dependent variable (β = .092, p < .01). The analysis results of Equation 6 showed that when control variables and contract service support were added to the equation, the results showed a significant positive correlation between family doctors’ contract service motivation and the dependent variable (β = .137, p < .01). Similarly, the seventh equation infuses the promotion of contract services by family doctors. It was found that increasing the promotion of contract services could significantly improve the enthusiasm of family doctors in providing services (β = .085, p < .01). Finally, stress is added to Equation 8. Different from the above variables, the relationship between stress and family doctor contract services is significantly negatively correlated, and the estimated coefficient β is .079 at the 1% significance level.
Discussion
Improving health workers’ performance in China has recently of great concern. One of the main factors that enhances job efficiency is motivation. The current study examines the motivational factors influencing family physician contract services in the Jiangsu province of China. Results from Equation 1, as seen in Table 4, show that gender, age, educational background, and working years of family physicians have no significant impact on the motivation of family physicians to sign up for service. In contrast, personal monthly income, title, and establishment significantly impact the contractual service motivation of family physicians. Good remuneration impacts the level of satisfaction of family physicians and motivates them to give their very best. In other words, lower salaries could hinder family physicians’ ability to meet their regular expenditures, contributing to divided attention and job performance. In earlier studies, a similar finding was reported.
Nonetheless, once salaries are satisfactory and paid on time, it encourages employees to concentrate and dedicate themselves to their assigned roles. They are more inspired to give their all, which leads to better results. This finding relates to the earlier suggestion that improved salaries and benefits are major financial incentives for workers to be retained in the health sector.
As can be seen from model 2, this study identified respondents perceived intrinsic motivational factors to influence their motivation for the contract service. A surge in the perceived sense of belonging increases the motivation of family contract services. That is to say, the explanation of contract services among family physicians is indistinguishably tied to the feeling that they belong to a greater community that shares common interests and aspirations. However, when family physicians feel left out and isolated at work, it can result in lower organizational commitment and engagement. The need to belong has been attributed to the fundamental human motivation that has a powerful influence on cognitive processes, emotional patterns, behavioral responses and health, and well-being.
Equation 3 findings demonstrate that family physicians’ professional motivation substantially positively affects the signing of contract service. This form of motivation can be words of encouragement or incentives given to family physicians to enhance their performance at the workplace. In addition, giving full attention to family physicians’ professional skills, recognizing the professional value of family physicians, and encouraging residents to choose family physician contracted services can improve family physicians’ motivation to sign for service.
The final form of intrinsic factor to be discussed is professional efficacy. Similarly, professional efficacy showed a positive effect on family physician contract motivation.
Based on the results, it is known that self-efficacy could affect the perception of work, satisfaction, and task performance of family physician contract services. Thus, family physicians with increased self-efficacy can become innovative less stressed as they are confident to succeed. In turn, this impacts their performance and the degree to which they endure in the face of difficulties. Some research supporting the results of this study is being conducted in Senegal, China, and for Jordan.
The next strand of the study considers the motivation of other family physicians to sign contract services. The meaning of this effects of external motivation on family physician contract services. Contract service support, promotion, and attractiveness play a significant role in improving them finding could be that when family physicians become conscious that their actions have been acknowledged both privately and publicly, they are motivated to work hard. However, when health authorities do not appreciate the commitment of family physicians, they could become irritated and fail to give their utmost. This gradually gives rise to apathy for the duties and roles assigned, leading to a decline in overall performance.
Besides, a surge in promotion and attractiveness of contract services positively motivates contract services among family physicians in the Jiangsu province. The possibility is that; family physicians may look to their employers for promotion when their time is due. When this does not happen, they believe their efforts are not good enough and need the organization. This, in turn, can result in less effort and performance of family physicians. When this fails, they tend to think that their efforts are not reasonable enough and not needed by the organization. They then tend to put in minimal efforts, which gradually affect their performance. Fortunately, when family physicians are promoted at the appropriate time, they become motivated and find more effective ways to improve their commitment to services demanded from them by their organization—leading to improved performance. Related studies of Jing and Fang (2020) support these findings.
Contrary to the above, family physicians’ experience of intense pressure has a negative impact on their contract services. This is possible because higher pressure can result in less efficient output by family physicians, which can contribute to lower productivity and work quality. The result of this finding agree with the current findings of the study.
Conclusion
Healthcare workers are an essential element in the functionality of the health system. The current study investigates the effect of motivation on family physician contract services within the Jiangsu province of China. The results from the study revealed that intrinsic motivation such as a sense of belonging, professional motivation, and efficacy positively affect family physician contract services. In the case of extrinsic motivation, all constructs (service support, promotion, and attractiveness) except pressure similarly had a positive impact on family physician contract services. Precisely, pressure experienced by family physicians reduces their service motivation. It is therefore recommended that;
The results show that improving self-efficacy will improve the motivation of family doctors to provide services. However, for the current Chinese family doctors, their education background, income, and social status are lower than those of large urban hospitals, which makes it difficult for them to have a higher self-evaluation. Therefore, we should change the existing evaluation criteria and establish diversified evaluation criteria to affirm the work achievements of family doctors, so as to improve their self-efficacy.
The surge in self-identity has increased the incentive for family doctors to sign up for services. Therefore, it is necessary to reshape the health culture and help family doctors to affirm the value of themselves and their affiliated primary medical institutions. It also ensures that family doctors can participate in all stages of designing motivational factors that directly affect their performance, thus enhancing their sense of self-belonging.
Intense pressure can have a negative impact on the contracted services of family doctors. This finding suggests that policymakers should implement feedback mechanisms that enable employees to assess their level of motivation and performance, aiding in the relief of their career anxiety and stress. In addition, performance standards will be measured by those directly related to the job and derived from a thorough job analysis. This finding suggests that policy makers should adopt feedback mechanisms at different levels of health to encourage family physicians to measure levels of motivation and self-output.
Finally, service, promotion, and attraction have improved the enthusiasm of family doctors to provide services, which requires health managers to formulate and implement policies to provide good policy environment and smooth promotion channels for family doctors, so as to improve the service level and value of Chinese family doctors and promote the health level of the whole people.
Future research will further focus on the mechanism of intrinsic motivation and extrinsic motivation, including possible mediating and moderating effects. The effect of time lag on influencing factors will also be taken into account.
Limitation of the Study
There are some deficiencies in the research. First of all, the data of the questionnaire comes from the subjects, and it still cannot be ruled out that a few subjects’ responses are not accurate enough, their answers are not serious, and the answers they choose show a central tendency. Secondly, the study was based on the large sample data of regional quality monitoring, and the data results still need to be interpreted by combining research methods such as interview and observation. Meanwhile, the study excluded all family doctors who received contract services but were officially on leave or absent due to illness, as well as all categories of auxiliary staff who did not directly provide care to patients in the hospital. In addition, this study only focuses on the one-way influence of internal and external factors on the motivation of Chinese family doctors to provide contract services, which may also be the limitation of this study. Finally, the research is a horizontal study, but the service provision of family doctors is a process, and the longitudinal study on the service provision motivation of family doctors needs in-depth analysis, so as to further enrich the research on the influence mechanism of the contract service motivation of family doctors.
Footnotes
Acknowledgements
We also wish to render our sincere gratitude to the department of Social health insurance for making their available facilities for this extended period of research.
Abbreviations
Community Health Centers (CHCs) and family physician contract service (FDCs).
Author Contributions
XX responsible for the conception and design of the study. Specifically, XX determined the research theme of family doctor service motivation, and organized investigations and data collection. JL and LZhao collected and perform the analysis, and all authors carried out the interpretation of data. Specifically, JJ was responsible for the coding and preliminary processing of the data, and LZhao was responsible for further analysis of the data such as regression analysis. XX, SAW led the drafting of the manuscript. Specifically, XX was responsible for the construction of the paper framework, and SAW was responsible for writing the English manuscript. XX and LZhao were both involved in critically revising the manuscript for important intellectual content. Specifically, they are responsible for the response to the review comments and the corresponding revision work of the manuscript. All the authors read and approved the final manuscript, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is funded by the Natural Science Foundation of China (72274081, 71904066) and the Social Science Foundation of Jiangsu Province (20SHD002).
Ethics Approval and Consent to Participate
The study was assessed and approved by the Jiangsu University Ethics Panel with number 406/2019. A written informed consent was obtained from participant following the explanation of the purpose and the significance of the study. We confirmed that all methods were carried out in accordance with relevant guidelines and regulations.
Consent for Publication
Not applicable.
Availability of Data
The datasets employed by the researchers in the analysis of the study is available by the authors upon reasonable request. We confirmed that informed consent was obtained from all participants.