
Abstract
Cancer fatigue (CF) is a major issue facing cancer patients that can negatively impact their quality of life. This study describes the development and validation of the Cancer Fatigue (CF) scale for the assessment of fatigue in cancer patients. A total of 202 cancer patients at university hospitals in South Korea were recruited and completed the questionnaires. Descriptive analysis was performed to determine the participants’ socio-demographic characteristics; the construct validity was examined using exploratory factor analysis; internal consistency reliability of the scale was estimated for the meaningful total scale and factors; and confirmatory factor analysis was performed to confirm the repetitive reproducibility of the factors. Findings indicated that the CF scale had good psychometric properties. 67.89% of the variance was explained by four subfactors: socio-cognitive (six items), physical (five items), psycho-affective (three items), and social-relationship networks (two items). The Cronbach’s alpha of the 16-item CF scale was 0.89 for the total scale, and the range of Cronbach’s alpha for subfactors was .75 to .89, indicating that it is valid and reliable. The 16-item CF scale is a feasible and time-efficient tool for assessing the fatigue of cancer patients in the clinical setting. Healthcare providers may use this measurement tool to explore cancer patients’ fatigue and routinely track the effect of a customized intervention on CF. This study also informs healthcare providers in other countries about the fatigue characteristics of Korean cancer patients.
Introduction
Cancer incidence and mortality are steadily increasing despite the remarkable advances in medicine. Furthermore, the incidence and death of cancer patients are expected to increase because of an aging population and changes in health behavior and socio-environmental structure. Cancer fatigue (CF) is a significant issue facing cancer patients and survivors that can negatively impact their symptoms and quality of life (Al Maqbali, 2021; M. K. Jang et al., 2022). For clinical and research purposes, it is essential to effectively assess CF attributes from the patient’s point of view. Assessment of CF is important and should be performed during the initial cancer diagnosis, throughout cancer treatment, and after treatment using an accurate fatigue scale.
Literature Review
The distress experienced after a cancer diagnosis is not limited to problems caused by cancer but includes various physical, and psycho-social symptoms and socioeconomic difficulties (Al Maqbali, 2021; Thong et al., 2020). Common symptoms of late-stage cancer include fatigue, pain and weakness, nausea and vomiting, poor appetite and malnutrition, oral symptoms, constipation, diarrhea, depression, and anxiety (E. Choi & Henneghan, 2022). Among them, fatigue and weakness are quite subjective symptoms that more than 50% to 89% of cancer patients complain of, and often do not improve with enough rest (Rau et al., 2020; Shah et al., 2022). Fatigue is the most common side effect of cancer treatment and can last for months or years after its completion. As a biological factor, inflammation is a major cause of cancer, and CF occurs during chemotherapy and radiation therapy due to cell damage during treatment and the secretion of cytokines as an inflammatory reaction (Thong et al., 2020). Thus, reducing patients’ fatigue and pain, and treating the tumor is important in cancer management (M. K. Jang et al., 2021; Rau et al., 2020). More than 70% of patients complain of fatigue, and many previous studies have suggested that access to interventions such as physical activity, psychological education, cognitive behavior intervention, and mental and physical therapy are useful in its reduction (Lockhart et al., 2020; Maass et al., 2021; Rau et al., 2020).
CF is related to cancer or its treatment and is a subjective experience of continuous physical, emotional, and cognitive tiredness or exhaustion in cancer patients and cancer survivors (W. G. Lee & Kim, 2022; Yeun & Jeon, 2020). It is a multidimensional problem that encompasses a general sense of weakness, decreases in attention, motivation, and interest in daily life, and includes emotional instability (Weis et al., 2019). A major change in the last years has been an increased emphasis on the individual’s subjective perspective in assessing fatigue in cancer patients (National Comprehensive Cancer Network, 2022). Cancer patients describe their fatigue as differing from what they had previously experienced and reflecting noticeable loss of energy, exhaustion, and inability to perform some routinely performed before their cancer experience (Amarsheda & Bhise, 2022). Several studies (E. Choi & Henneghan, 2022; Ebede et al., 2017; M. K. Jang et al., 2021; Marker et al., 2022; Rau et al., 2020) including intervention studies, on chronic fatigue experienced by cancer patients, explored fatigue-related factors and relief, but it continues to be a major nursing problem and the identified interventions had different goals and mechanisms. Thus, it is necessary to precisely assess the degree of fatigue using a multidimensional tool to identify appropriate interventions. A wide range of patient self-reported instruments was used for fatigue assessment. In recent years, most studies have used instruments that evaluate unidimensional or multidimensional fatigue and have been tested to verify their validity, consistency, and reliability. There are still problems concerning the clinical interpretation of the scores obtained on these instruments and the comparison of fatigue measurements obtained by different instruments (Rau et al., 2020; Song et al., 2018).
In our current study, the search results of the measurement tools cited in the previous domestic study on fatigue in cancer patients until 2020 are as follows: The fatigue scale (Kim, 2006), the Fatigue Severity Scale (Goodwin et al., 2019), the Korean version of the FACIT-Fatigue Scale (Byun & Kim, 2012; Montan et al., 2018), Piper’s fatigue scale which was translated into Korean and modified by E. H. Lee (1999) and Y. Jang et al. (2017), and Multidimensional Fatigue Inventory-Korean version (MFI-K) (Song et al., 2018) were used. Since these fatigue measurement tools were developed by the original developer over a few decades ago based on Western society, considering the cultural and linguistic differences, the development of an updated cancer fatigue measurement tool suitable for Korean cancer patients would be useful. Moreover, the structure of Korean sentences is very different from the structure of English sentences. Korean sentences have the structure of subject + object + verb, even the meaning of positive and negative is placed at the end of the sentence. Overall, the translated CF measurement tool in the Korean version is very likely to be different from the CF measurement tool’s original version based in Western society. Therefore, it is meaningful and important to develop the latest CF measurement tool considering the above-described characteristics of CF, management, and socio-environmental characteristics of cancer patients.
Study Aim
This study aimed to develop a tool to measure fatigue in cancer patients and test the reliability and validity of the developed scale.
Methods
Research Design
This study is a descriptive investigation to develop a tool to measure cancer patients’ fatigue and verify its validity and reliability.
Research Setting
Participants were recruited from cancer centers and inpatient wards affiliated with university hospitals in South Korea.
Research Participants
A total of 202 cancer patients at university hospitals in Seoul and Chungju were enrolled to assess their fatigue levels. Eligibility criteria were inpatients and outpatients diagnosed with cancer, over 19 years, who could communicate and understand their native language (Korean) and were able to complete the questionnaire, and not suffering from a mental or cognitive disorder.
Ethical Considerations
This study was approved by the Institutional Review Board at a University and was conducted following the principles of the Helsinki declaration. All the information gathered was treated confidentially and anonymously. All participants had been explained this data; that would never be used for any other purpose, other than this research. Written informed consent was obtained from the participants of this study
Scale Development Process
Cancer Fatigue Concept and Initial Items Development Process
The theoretical and field phases were combined to determine the type of fatigue in cancer patients. The composition of the initial questions established a concept for the development of the fatigue measurement tool by identifying the properties of fatigue based on prior studies (Al Maqbali, 2021; Amarsheda & Bhise, 2022) and using data obtained through domestic and foreign literature reviews. In addition, we conducted in-depth interviews with 13 cancer patients while considering various factors: gender, age, duration of illness, the presence of chemotherapy, and the diagnosis stage. The content of the interviews was gathered through in-depth interviews using semi-structured questions to confirm the perceptions of cancer-related fatigue experienced by the patients. Then the interview contents were analyzed by using the content analysis technique.
The process mentioned above, combined the theoretical and field research stages to confirm participants’ perceptions of cancer-related fatigue. Throughout this process, a total of 186 items were extracted. To categorize the raw data, 85 items were derived through the elimination of similar or overlapping statements by repeatedly reading them. These 85 items were reviewed by three nursing professors with extensive nursing practice (major in oncologic nursing, and psychiatric nursing) and qualitative research experience, and two oncologic nurse specialists in a cancer hospital; the meaning and language of the items were revised and supplemented to derive the final 43 items.
Content Validity Verification
Content validity refers to how appropriately the content of the tool reflects the concept to be measured (Almanasreh et al., 2019). To determine the content validity of the 43 items, a group consisting of three nursing professors including a major in oncologic nursing, and psychiatric nursing, one oncologist (medical doctor) in the cancer center, three oncologic nurse specialists with 3 to 15 years of practical experience in a tertiary hospital, and two nursing doctoral students were selected. This was based on the suggestion that 3 to 10 experts should be used to verify content validity (Lynn, 1986). In the verification process, the deletion and addition of items with similar meanings, items unrelated to cancer fatigue, and items with ambiguous or overlapping expressions were confirmed, and the validity of each item was evaluated from a 4-point scale (“very valid” four points), the score for each item was evaluated as three points or four points, and the content validity index (CVI) by the final expert group was 96%. A CVI value above 0.78 was considered a fit for the scale (Polit et al., 2007). As a result of the content validity test, the draft questionnaire consisting of 40 initial CF items and participants’ socio-demographic and clinical characteristics with 19 items was developed.
Construct Validity and Preliminary Items
The pilot test was conducted with 190 cancer patients at two higher general hospitals in Seoul Korea to validate the 40 initial CF items. Twenty-two items were derived as six factors in the step 1 factor analysis by a varimax rotation of 140 questionnaires (excluding those with insufficient responses). For the validity test, items with a factor loading value of 0.50 or greater and a cross-factor loading value of less than 0.35 were selected, and items with a factor loading value of less than 0.50 or a cross-factor loading value of more than 0.35 were deleted. Also, items with reliability of less than 0.70 were deleted.
Concept Validity and Reliability Verification
To verify the validity and reliability of the 22 items extracted from the pilot test study, the written questionnaire was collected and analyzed from 202 cancer patients at university hospitals in Seoul and Chungju. These cancer patients who had not participated in the preliminary scale development phase were asked to complete the questionnaire with 22 items CF scale including the specific cancer diagnosis and sociodemographic data for each patient. The number of samples for factor analysis was selected based on that at least 4 to 5 times the number of items was appropriate (H. C. Choi, 2019).
Test-Retest Reliability
Ambulatory cancer patients who were not receiving active cancer treatment were recruited in a study to assess the test–retest reliability of the new scale. They completed the written questionnaire in the outpatient clinic, and they took this survey by telephone after an interval of about 2 weeks.
Data Collection & Analysis
Data collection from May 25 to June 31, 2020, was conducted with written questionnaires made by the researchers distributed to cancer patients and collected. The collected data were analyzed as follows. Descriptive statistics were used for the participants’ demographic characteristics, and the CVI was used for the content validity of the items. The revised item-total correlation coefficient was obtained for the correlation between each item and the whole, and items with low correlation were removed. Whether the data were appropriate for factor analysis was confirmed by Kaiser-Meyer-Olkin (hereinafter referred to as Kaiser-Meyer-Olkin (KMO) and Bartlett’s test of sphericity. The composition validity was confirmed by factor analysis of principal component analysis using Varimax rotation. Factor extraction was based on an eigenvalue of 1.0 or more, a cumulative percentage of variance explained by the extracted factors of 60% or more, and a factor loading of 0.40 or more (Li, 2016). Pearson’s correlation coefficient was used as the correlation matrix between sub-factors, and Cronbach’s alpha was used for the consistency reliability test. To confirm the items’ convergence and discriminant validity, a multi-attribute/multi-item matrix analysis was conducted on the relationship between the item and the lower scale. To confirm the criterion validity, Pearson’s correlation coefficient was used for the score by sub-area of cancer fatigue and the overall cancer fatigue relationship. Confirmatory factor analysis (CFA) was performed to confirm the repetitive reproducibility of the factors. Test-retest reliability was assessed by Pearson’s correlations comparing the scores reported on two separate occasions.
Results
Participants Characteristics
Participants’ general and clinical characteristics are shown in Table 1.
Participants’ Socio-Demographic and Clinical Characteristics (N = 202).

Note. M = mean; SD = standard deviation; QOL = Quality of Life; CF = cancer fatigue.
Missing values were excluded; a,b,cDuncan test; †Numeric scale.
A total of 202 cancer patients answered the 22 preliminary items, with an average age of 55.1 ± 11.45 years, and 112 were male (54.6%). For marital status, 162 (79.0%) were married, and 22 (10.7%) were widowed. For education, 27 (13.2%) were college graduates or higher and 23 (11.2%) graduated high school. A total of 130 (63.4%) worked, and 70 (34.1%) were unemployed. Seventy-eight participants (38.0%) practiced no religion, 52 (25.4%) reported being Buddhist, and 49 (23.9%) identified as Christian. For average monthly gross income, 36 (17.6%) reported less than 1 million won, and 47 (22.9%) reported more than 4.01 million won. One hundred twenty-five (61%) of the people who paid for treatment were the most likely to pay for themselves. One hundred thirty-three (64.9%) answered that the primary caregiver was a spouse, and 144 (70.2%) answered that they had cancer insurance. Cancer diagnosis types were 59 gastric cancer (29.2%), 56 breast cancer (27.7%), 37 lung cancer (18.3%), 30 colon cancer (14.9%), and 20 rectal cancer (9.9%). The duration of the cancer was 2.03 ± 1.00 years, and the average CF (item mean) was 2.21 ± 0.53. There was a significant difference in the degree of fatigue according to gender and level of education. When also asked, “How much pain do you feel when you have no pain ‘0’ and severe pain ‘10’?.” The average pain level of the participant felt was 3.39 ± 2.37, when asked as the same method, the quality of life was 5.79 ± 1.59.
Step 1 Factor Analysis and Reliability Results
As shown in Table 2, the results of the step 1 factor analysis were presented. The KMO index and Bartlett sphericity test were performed to check whether each item is suitable for factor analysis. As a result, the KMO value was 0.895, which is more than 0.80. The sphericity test found that it was not the identity matrix (p < .001). Therefore, the preliminary survey questions were found to be appropriate for factor analysis. Factors in each item were determined as items satisfying factor loading >0.50, and items with cross-factor loading <0.35. Six factors were derived because of determining the items that satisfy the factor loading value and the cross-factor loading value. The 22 items of six factors determined in the factor analysis was shown in Table 2. Cronbach’s alpha for the total of all items was .90, and the internal consistency coefficient for factors 1 to 6 were 0.88, 0.83, 0.78, 0.76, 0.84, and 0.79, respectively.
Step 1 Factor Analysis for the Cancer Fatigue.

Note. KMO = Kaiser-Mayer-Olkin.
Step 2 Factor Analysis and Reliability Results
As shown in Table 3, the results of the step 2 factor analysis were presented. Among items 24, 15, 37, and 38 tied to Factor 5, item 24 “I feel that my memory has declined” and item 15 “I feel like I want to die (euthanasia, etc.), when I am tired” were removed because they were inappropriate in meaning as a factor. In the same way, a few items whose meanings were inappropriate with the factors were removed, and a secondary factor analysis was conducted again. The KMO index and Bartlett sphericity test were performed to check whether each item is suitable for factor analysis. As a result, the KMO value was 0.895, which is more than 0.80. The sphericity test found that it was not the identity matrix (p < .001). Therefore, the preliminary survey items were found to be appropriate for factor analysis. Factors in each item were determined as items satisfying factor loading >0.50, and items with cross-factor loading <0.35. Four factors were derived because of determining the items that satisfy the factor loading value and the cross-factor loading value. The 16 items of four factors determined in the factor analysis was shown in Table 3. Cronbach’s alpha for the total of all items was .89, and the internal consistency coefficient for factors 1 to 4 were 0.89, 0.84, 0.75, and 0.78, respectively.
Step 2 Factor Analysis for the Cancer Fatigue.

Note. KMO = Kaiser-Mayer-Olkin.
Test-Retest Reliability
For the reliability of the test-retest, the first written survey was conducted on fifteen cancer patients receiving outpatient clinic, followed by a phone call 2 weeks later. The CF scale had good stability (average test-retest reliability r = .75, p < .001) and good internal consistency (Cronbach’s alpha coefficient for all 16 items = 0.89).
Factor 1: Socio-Cognitive Factor (Six Items)
Factor 1 consisted of the following six items. “I can’t enjoy activities (work, hobbies, etc.) due to fatigue”; “I need help with my daily life when I’m tired”; “It’s harder to concentrate more than before.,”; “Compared to before, I do not have the strength to care for the people around me (family, colleagues, etc.),” “Due to fatigue, my body does not obey my thoughts when performing all kinds of activities (exercise, shopping, driving, doing housework, reading the newspaper, etc.),” and “When I am tired, I feel miserable.”
Factor 2: Physical Factor (Five Items)
Factor 2 consisted of the following five items. “There are physical symptoms (dizziness, nausea, blurred vision, muscle pain, fever, chills, etc.) that appear when I am tired”; “I am tired from side effects (nausea, vomiting, etc.) from anti-cancer treatment (such as chemotherapy, radiotherapy, immunotherapy, operation, and pain treatment)”; “When I’m tired, I lose my appetite”; “I have no desire for sex”; and “If I am too tired, I can’t get a good night’s sleep.”
Factor 3: Psycho-Affective Factor (Three Items)
Factor 3 consisted of the following three items. “When I’m tired, I feel helpless, and I don’t want to do anything, which gets annoying”; “When I’m tired, I have no energy and I cannot use any energy.” “I feel more tired when I do something I don’t want to do.”
Factor 4: Social-Relationship Network Factor (Two Items)
Factor 4 consisted of the following two items. “If I cannot do social activities (meetings), I get stressed and tired.”; “I think loneliness aggravates fatigue.”
Results of Confirmatory Factor Analysis (CFA)
The results of the CFA were shown in Figure 1 and Table 4. Confirmation of construct validity is based on convergent validity and discriminant validity. Convergent validity refers to the reliability of the measurement variables representing constructs, and discriminant validity refers to the extent the scale measuring the concepts measures them as different (C. H. Li, 2016). In the measurement of the factor loading, lambda (λ) values were all ≥0.5 and ≤0.95, and all CR values indicating conceptual reliability or synthesis reliability were ≥1.965, which was statistically significant. All average variance extracted (AVE) values were satisfied as ≤0.5. Discriminant validity is determined by looking at whether AVE > Φ2, that is, rejecting the hypothesis that concepts are identical (Φ = 1). Figure 1 presented that the correlation coefficient between Factors 1 and 2 is .77, and the square of the correlation coefficient is .59, with a correlation coefficient of .32 between Factors 2 and 3, the square of the correlation coefficient was .10, and the correlation coefficient between Factors 3 and 4 was .54, with the square of the correlation coefficient as .29. Table 4 presented the AVE values of each factor are .817, .765, .802, and .888 for factors 1 to 4, respectively, which are all larger than the square of the correlation coefficient, demonstrating that there is discriminant validity. Table 4 presented the fit of the model. For each index of the CFA, GFI (Goodness of fit index), TLI, and NFI (Normal fit index) were all >0.9, and RMR (Root mean square residual) and RMSEA (Root mean square error of approximation) were all <0.05, proving the suitability of the CFA model.

The correlation and discriminant validity of the model.
Effect of Each Path of Confirmatory Factor Analysis (CFA) for the Cancer Fatigue.
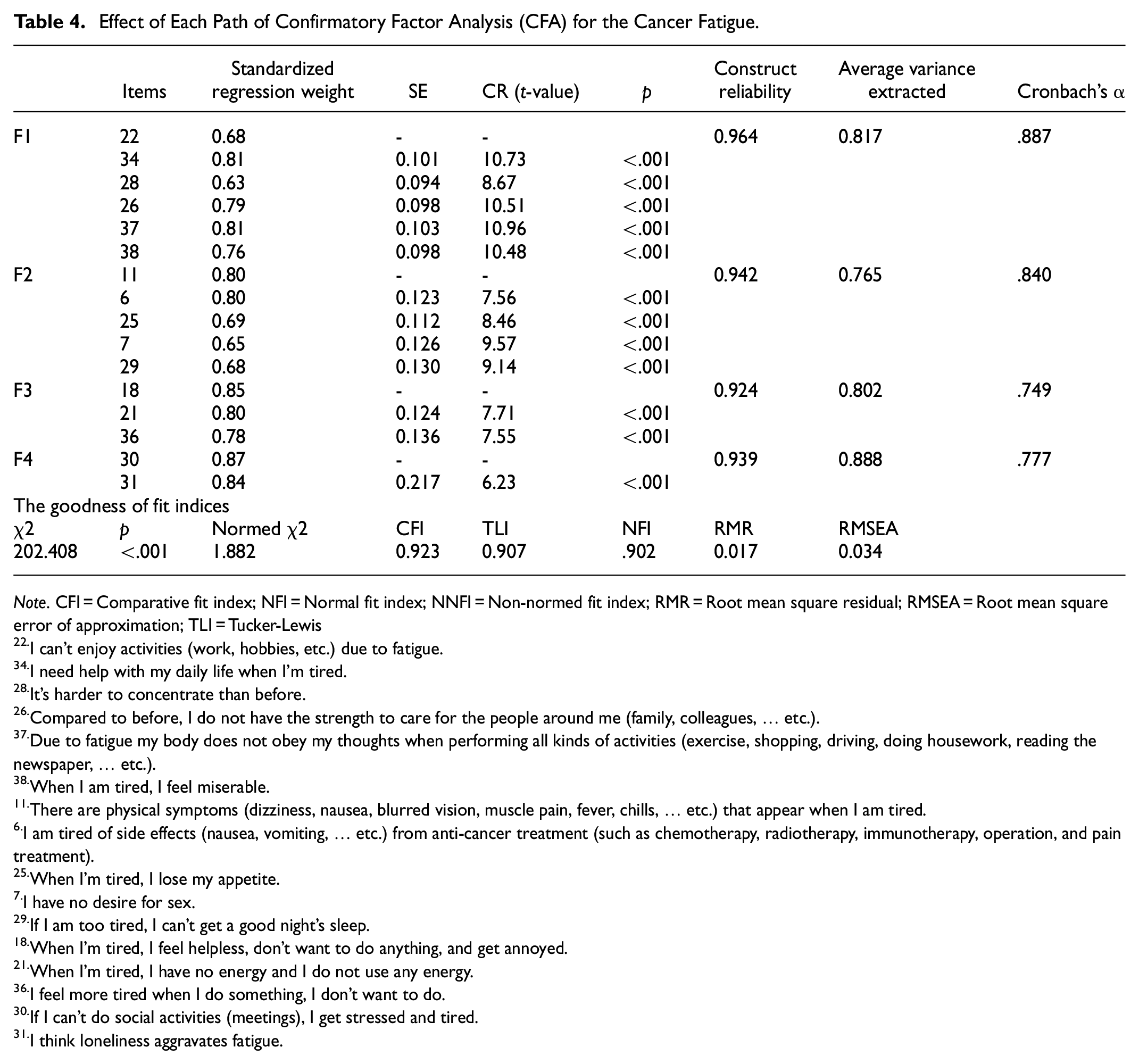
Note. CFI = Comparative fit index; NFI = Normal fit index; NNFI = Non-normed fit index; RMR = Root mean square residual; RMSEA = Root mean square error of approximation; TLI = Tucker-Lewis
I can’t enjoy activities (work, hobbies, etc.) due to fatigue.
I need help with my daily life when I’m tired.
It’s harder to concentrate than before.
Compared to before, I do not have the strength to care for the people around me (family, colleagues, … etc.).
Due to fatigue my body does not obey my thoughts when performing all kinds of activities (exercise, shopping, driving, doing housework, reading the newspaper, … etc.).
When I am tired, I feel miserable.
There are physical symptoms (dizziness, nausea, blurred vision, muscle pain, fever, chills, … etc.) that appear when I am tired.
I am tired of side effects (nausea, vomiting, … etc.) from anti-cancer treatment (such as chemotherapy, radiotherapy, immunotherapy, operation, and pain treatment).
When I’m tired, I lose my appetite.
I have no desire for sex.
If I am too tired, I can’t get a good night’s sleep.
When I’m tired, I feel helpless, don’t want to do anything, and get annoyed.
When I’m tired, I have no energy and I do not use any energy.
I feel more tired when I do something, I don’t want to do.
If I can’t do social activities (meetings), I get stressed and tired.
I think loneliness aggravates fatigue.
Discussion
This study aimed to develop a suitable CF measurement tool for cancer patients, with high validity and reliability. The developed CF scale was found to be a reliable and valid instrument for assessing fatigue in Korean patients with cancer. Our findings can be concisely summarized into three points: (a) The cancer fatigue dimension considering the latest trends Korean socio-cultural context was grouped into four subfactors; (b) The developed CF scale proved an appropriate factor structure in Korean cancer patients; (c) The CF scale showed good validity and reliability in several cancer patients sufficient for testing the psychometric properties of this 16-item scale.
The KMO scale and Bartlett sphericity test were used to determine the appropriateness of factor analysis for the preliminary tool, increasing the sample relevance of the preliminary tools. In addition, six factors were extracted from the analysis of the collected data for the 22 items preliminary tool, and each item’s factor loading was higher than 0.35, proving that the preliminary tool had high construct validity. Moreover, all C.R values indicating conceptual reliability or synthesis reliability were 1.965 or higher and were statistically significant, and the AVE values were all satisfied as 0.5 or higher. After analyzing the tool’s reliability, Cronbach’s alpha for the final 16 items was .89, indicating high internal consistency. In the reliability analysis by the factor, the values for factors 1 to 4 were all higher than 0.60, indicating that each factor is appropriate to measure patients’ cancer fatigue. Considering the cultural and linguistic differences pursued by this study, a direct comparative discussion was limited as no cancer fatigue measurement tool recently developed in the Asia region. Okuyama et al. (2000) have been reported which developed and verified the cancer fatigue scale for Japanese cancer patients. Their research reported the cancer fatigue scale, which consists of 15 items with three subscales (physical, affective, and cognitive), Cronbach’s alpha coefficient of a total scale was.88. However, their study was similar to previous studies based on Western society.
We herein discuss the subfactors constituting the CF scale. The four subfactors of the CF scale derived from the results of this study have distinctive characteristics from fatigue measurement tools developed in Western society. Unlike the fatigue measurement tools already used in Korea (K-R-PFS, M. K. Jang et al., 2021; MFI-K, Song et al., 2018), the socio-cognitive factor classified as the first factor was the highest at 24.9% of the total variance of 67.9%. This is different from the fact that most existing tools had the highest variance of physical (or behavioral) factor as subscales. In other words, it can be inferred that Korean cancer patients complain more about fatigue based on socio-cognitive factor caused by environmental interaction than physical fatigue. In addition, the social-relationship network factor, which was not included in the previously used tools (K-R-PFS, MFI-K), was classified as the fourth factor. This grouping can be attributed to Koreans’ traditional values (Confucianism and Familism) and the social atmosphere that values interpersonal relationships (Hong, 2019). These phenomena could be explained by the fact that the new CF scale was developed for Korean cancer patients, not those with chronic diseases, and by geographical, cultural, and linguistic differences from Western societies.
Factor 1 was grouped as a socio-cognitive factor with six items (items 37, 34, 26, 38, 22, and 28). The environment surrounding human-being refers to an objective situation that can affect an individual’s cognition and behavior (Nickerson, 2022), and the objective situation in our current study was a cancer diagnosis. Although the items in the FACIT-Fatigue Scale (W. G. Lee & Kim, 2022; Montan et al., 2018) are not grouped by subfactors, the items “I have trouble starting things because I am tired” and “I have trouble finishing things because I am tired” are both similar to the item 37 “Due to fatigue, my body does not obey my thoughts when performing all kinds of activities (exercise, shopping, driving, doing housework, reading the newspaper, … etc.). .” Among the FACIT-Fatigue Scale item “I need help doing my usual activities,” and “I am frustrated by being too tired to do the things I want to do” were consistent with the items “I need help with my daily life when I am tired (item 34),” and “When I am tired, I feel miserable (item 38). .” Those grouped as a cognitive-mood subscale in the Jang et al. study (2021) using the Korean version of the Revised Piper Fatigue Scale (K-R-PFS), the item “I do not have the strength to take care of my family compared to before” was similar to the item 26 “Compared to before, I do not have the strength to care the people around me (family, colleagues, etc.).” In addition, the item “It is difficult for me to pursue a hobby I liked before” coincided with item 22 “I can’t enjoy activities (work, hobbies, etc.) due to fatigue” in this study.
Factor 2 grouped five items (items 11, 6, 25, 7, and 29) as physical factors. A study by Oberguggenberger et al. (2017) suggested that fatigue reduced sexual activity based on the significant difference between cancer patients who answered that they “feel tired” from the item “there is a change in sexual behavior.,” “there was no desire for sex.” Previous studies (M. K. Jang et al., 2021; Thong et al., 2020) indicates that all anti-cancer treatment (such as chemotherapy, immunotherapy, radiotherapy, etc.) negatively affects reproductive cells, resulting in amenorrhea, azoospermia, and infertility be inferred that reduced daily activity will eventually become a physical factor. Hence, it is thought that “I have no desire for sex” is closer to a physical factor. Some previous studies (E. Choi & Henneghan, 2022; Miaskowski et al., 2021; Rau et al., 2020; Stulz et al., 2020) have also indicated that cancer patients often experience anxiety, depression, fear, and stress, as well as social unemployment, decreased interpersonal relationships, and sexual problems, the grouping for this item needs further consideration in the future. Among the items on the FACIT-Fatigue Scale (W. G. Lee & Kim, 2022; Montan et al., 2018), “I am too tired to eat” was consistent with item 25 “When I’m tired, I lose my appetite.” A study (Goodwin et al., 2019) of systematic lupus erythematous patients and multiple sclerosis patients using the Fatigue Severity Scale (FSS), listed “Fatigue interferes with my physical functioning” as fourth among nine items, but no detailed physical functions were identified.
Factor 3, the psycho-affective factor, had three items (items 18, 21, and 36). Emotions are mental and physiological states related to various feelings, thoughts, and actions or a conscious mental reaction (such as anger or fear) subjectively experienced as strong feelings usually directed toward a specific object and typically accompanied by physiological and behavioral changes in the body (Rebecca et al., 2021). Among the problems described by cancer patients, signs such as fever, skin rash, and increased pulse rate can be objectively measured, but subjective symptoms such as pain, fatigue, digestive disorders, depression, etc., may be difficult to objectively measure (M. K. Jang et al., 2022). However, these symptoms cause suffering and increase patients’ burden (Amarsheda & Bhise, 2022; Maass et al., 2021; Weis et al., 2019). Therefore, developing a tool to quantify and evaluate the degree of these subjective symptoms will be useful to recognize the symptoms and their degree and can also be useful to evaluate changes and reactions in the cancer treatment process and determine the effectiveness of the appropriate intervention. The items at the emotional level are thought to cause emotional changes when cancer patients’ fatigue worsens and can be measured schematically in the third psycho-affective factor of this study. Among the FACIT-Fatigue Scale items (W. G. Lee & Kim, 2022; Montan et al., 2018), “I feel weak all over,” and “I feel listless,” are similar to the items belonging to Factor 3 of this study. Also, Y. Jang et al. (2017) had an item that was consistent with “I don’t want to do anything,” as the third psycho-affective factor. In addition, the seventh of the nine items of the FSS (Goodwin et al., 2019), “Fatigue interferes with carrying out certain duties and responsibilities,” was similar to the psycho-affective items of this study.
In the current study, Factor 4 was a social-relationship network factor with a total of two items (items 30, and 31). Item 30, “If I can’t do social activities (meetings), I get stressed and tired” is based on the social-relationship network factor, which refers to reducing daily activities and social activities due to fatigue. Human behavior can be influenced by both individual characteristics and environmental/situational factors (Nickerson, 2022). Therefore, social behavior occurs because of the interaction between the individual and the environment (Jeon et al., 2022). Cancer patients in the lonely group reported higher levels of social isolation (Miaskowski et al., 2021), as well as more severe symptoms of anxiety, depression, fatigue, sleep disturbance, cognitive dysfunction, and pain (Al Maqbali, 2021; M. K. Jang et al., 2022). Item 31 was “I think loneliness aggravates fatigue.” A study by Bruce et al. (2019) reported that social support and meaningful interpersonal relationships are important preventive factors against loneliness; therefore, the second item may belong to the social-relationship network factor. Furthermore, loneliness was reported as a risk factor that increases fatigue (E. Choi & Henneghan, 2022), and future continuous research on loneliness and fatigue in cancer patients is needed.
Strengths and Limitations
This study has several strengths. This study found a multidimensional pattern and perceptions of Korean cancer patients’ subjective perspectives of fatigue. It also was the study to update the cancer fatigue measurement tool for Korean patients and effectively intervene in cancer patients’ fatigue. This newly developed CF scale is a reliable and valid instrument for measuring CF and may prove useful in both clinical and research settings.
This study has a few limitations. The first concern in the factor analysis was to reduce the items, it was not possible to measure the same samples repeatedly; therefore, when applying the new CF scale, it will be necessary to verify the performance. Moreover, there is a limitation in that it has not been compared and verified with an objective fatigue measurement tool that can confirm the accuracy of the developed CF scale. The study’s setting was also confined to a particular geographic location in Asia. Despite these limitations, this study provides valuable insights into the CF scale’s perspectives among cancer patients in a Korean socio-cultural context. Further studies need to be conducted in various groups of cancer patients to confirm the psychometrics of the newly developed instrument for generalizability.
Relevance to Clinical Practice and Research
Accurate assessment of CF should be routinely undertaken in clinical settings to help identify the appropriate interventions, treatments, and management to reduce fatigue among cancer patients and survivors. Moreover, developing and verifying a systematical assessment tool for CF will enhance the quality of life of cancer patients. We suggest that further longitudinal research is also needed to discern these relations. The 16-item CF scale is a feasible and time-efficient tool for assessing the fatigue of cancer patients in the clinical setting. Healthcare providers may use this tool to explore cancer patients’ fatigue and routinely track the effect of a customized intervention on CF. This study also informs healthcare providers in other countries about the fatigue characteristics of Korean cancer patients.
Conclusions
This study was a methodological study to develop a measurement tool for fatigue in cancer patients. After developing the CF measurement tool, its validity and reliability were verified. Based on our findings, we attempted to understand cancer patients’ fatigue and provide basic data for the development of effective intervention programs.
In conclusion, the new CF scale consists of subfactors that are deeply related to cancer fatigue based on previous research and are classified by dimension considering the latest trends in the Korean context so that it has the advantage of being able to confirm the subjective and holistic views of Korean cancer patients’ fatigue. In the future, it suggests further expanding the number of samples and conducting repeated studies by applying the developed CF scale in this study, to further verify the reliability and validity of this measurement tool.
Footnotes
Acknowledgements
The authors thank Ho Yoon Bang, MD (Professor, School of Medicine, Konkuk University) for support with data collection. The authors are sincerely grateful to Judith A. Erlen (Emeritus Professor, School of Nursing, University of Pittsburgh) for her critical feedback and editorial support on this manuscript.
Author Contributions
All authors contributed to the study’s conception and design. Material preparation, data acquisition, and analysis were performed by E.J.Y and H.J.K. The first draft of the manuscript was written by H.J.K, and all authors commented on the manuscript’s writing, review, and editing. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Namseoul University Research Fund.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Namseoul University (IRB no.: NSU-202005-005-03).
Informed Consent Statement
Written informed consent to participate in the study and make publications with the obtained data was obtained from all participants with a talk-back method.
Data Availability Statement
The data presented in this study are available on request to the first and corresponding author. The data are not publicly available due to ethical issues.