
Abstract
Despite current efforts, adherence to heart failure (HF) selfcare remains suboptimal. There is a need to identify modifiable factors that promote self-care adherence. Evidence suggests that patient activation and health literacy (HL) are modifiable and may be useful for improving HF self-care. However, more research is needed to understand the influences of these variables on HF self-care. The aim of this study was to examine the relationships between patient activation, health literacy, and self-care adherence in a diverse group of adults with HF. This study used a correlational, cross-sectional design. Correlation and regression tests were used to analyze associations among variables. Stratified random sampling was applied to attain a study sample that was 50% persons of color (POC). Of the 174 participants, 51% were female and 48.5% were POC with a mean age of 62 years. There was no significant relationship between HL and HF self-care adherence. There was a small, positive correlation between HL and dichotomized high/low activation levels (r = .163; p < .05). There was a small, positive correlation between patient activation and HF self-care behaviors (r = .151; p < .05). However, regression tests showed patient activation was not a predictor of selfcare (B = 0.173, p = .064). Persons with HF may perform self-care activities when highly activated, regardless of HL status. Patient activation was not a reliable predictor of self-care adherence. More research is needed to elucidate the influence of patient activation and HL on HF self-care behaviors.
Introduction
Heart failure (HF) is an incurable, chronic syndrome, affecting at least six million Americans and 64 million people worldwide (James et al., 2018; McDonagh et al., 2021; Virani et al., 2021). Projections show that the incidence and prevalence of HF is continuing to grow with the aging population (Virani et al., 2021). As HF progresses, hospitalizations are prevalent, making it a leading diagnosis in hospitalized persons aged 65 and older (Benjamin et al., 2019). Furthermore, persons of color represent almost half of the HF population and have the highest rates of hospitalization (Liljeroos et al., 2020; Morris et al., 2020). By 2030, it is forecasted that the annual expenditure for HF will increase by more than 200% in the United States which is cause for alarm (Heidenreich et al., 2011).
Heart Failure Self-Care
Persons with HF are typically taught self-care strategies for minimizing HF symptoms and maintaining clinical stability by their health care providers. In HF self-care, persons are asked to actively engage in monitoring bodily symptoms, weighing daily, eating a low salt diet, and adhering to prescribed medications (Heo et al., 2021; Moser et al., 2012). Unfortunately, self-care adherence among persons with HF is low (Jaarsma et al., 2013; Meraz, 2020; Meraz et al., 2023; Seid et al., 2019), leading to worsening HF symptoms, increased hospitalizations, and higher mortality rates (Lesyuk et al., 2018; Liljeroos et al., 2020; Turrise, 2016). High adherence to HF self-care has been associated with better mental health, physical functioning, improved quality of life and better HF outcomes (Hood et al., 2018; Ruppar et al., 2016; Vellone et al., 2017). Thus, encouraging adherence to HF self-care is an essential aspect of supporting persons with HF.
To improve HF self-care, it is imperative to identify modifiable factors that promote adherence. According to Riegel et al. (2022), HF self-care is dependent on individuals’ decisions to engage in self-care behaviors. It is heavily influenced by person-related factors and individual characteristics. Sociodemographic also factors affect HF self-care adherence, however, the degree of influence is not fully understood. In one study, HF self-care adherence was inversely related to older age, low income, inadequate social support, lower educational levels, and inadequate health literacy (White-Williams et al., 2020). In contrast, another study found no association between age, income, and HF self-care (Baah et al., 2021). Moreover, being married, having some college education, and being of Asian race only marginally explained the variance in HF self-care in this study (Baah et al., 2021). To date, studies of the influence of race and gender on HF self-care have consistently yielded inconclusive results (Baah et al., 2021; Graven et al., 2021; Koirala et al., 2018). Although sociodemographic factors may have some impact on HF self-care, other personal factors may be more important in motivating self-care adherence.
Personal Factors and Heart Failure Self-Care
Specific personal factors have been identified as influencing HF self-care adherence (Attaallah et al., 2016). In particular, attitudes, emotions, and beliefs may positively or negatively impact self-care adherence (Albert et al., 2014; Meraz, 2020; Meraz et al., 2023; Sedlar et al., 2021). When attitudes or beliefs about the outcome of a self-care task (i.e., following a low salt diet, adhering to medications) are positive, performing the task is more likely (Meraz et al., 2023). Conversely, appraising a self-care task as difficult, not beneficial, or inconvenient may stimulate nonadherence (Meraz, 2020; Meraz et al., 2023; Sedlar et al., 2021). Self-efficacy, the optimistic belief in one’s ability to successfully perform self-care tasks, has consistently been associated with better self-care (Koirala et al., 2018; Meraz et al., 2023; Riegel et al., 2022). Depression and negative emotions, on the other hand, adversely influence self-care adherence decisions (Liljeroos et al., 2020; H. Patel & Ghosh, 2017). Previous research also illustrates that equipping HF patients with the necessary knowledge, skills, and confidence to manage their HF may lead to sustained changes in self-care behaviors (Bidwell et al., 2018; Jaarsma et al., 2017).
Patient Activation
Patient activation appears to be modifiable (Aung et al., 2016) and increasing patient activation may be a strategy for generating improvements in HF self-care adherence. Patient activation signifies the level of patients’ involvement with managing their own health and refers to the extent to which they have the knowledge, skills, motivation, belief, and confidence to manage chronic illness, take steps for positive behavior change and to partner with healthcare providers for disease management (J. H. Hibbard et al., 2004). Accordingly, increasing levels of patient activation has been associated with improved self-care behaviors in chronic disease, including HF (Newland et al., 2021). Like HF self-care, low patient activation is common among those with low income, less education, and older age (Golubinski & Wild, 2021; McCabe et al., 2018). There is growing evidence to suggest that patient activation may be useful in individualizing and evaluating interventions for improving self-care behaviors for chronic illness (Beckie et al., 2017; Bos-Touwen et al., 2015; Dunlay et al., 2017; Jacobson et al., 2018; Prey et al., 2016; Young et al., 2017). However, studies have been inconsistent in demonstrating a predictable association between patient activation and improvements in HF self-care adherence (Shively et al., 2013).
Health Literacy
Since understanding self-care instructions may be vital to effective self-care adherence and decision-making (Riegel et al., 2022), health literacy might be important to both patient activation and self-care adherence. Health literacy is defined as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” (Ratzan & Parker, 2000). Indeed, in the U.S., health literacy is a better predictor of health than race, age, employment status, educational level, or income (Bresolin, 1999; Winkelman et al., 2016). Multiple studies have observed a relationship between health literacy and patient activation among those with chronic illness(s) (Dunlay et al., 2017; Huang et al., 2021; Smith et al., 2013). Thus, it is postulated that health literacy and patient activation are related constructs in the HF population as well.
The results of studies examining the impact of health literacy on HF self-care are mixed (Chen et al., 2014; Jo et al., 2020; Kuhn et al., 2021; J.-R. Wu et al., 2017). While some studies have demonstrated no significant relationship between HF self-care adherence and health literacy, the findings of a recent study by Erünal and Mert (2020) suggests that health literacy may be a predictor of HF self-care behaviors. Health literacy and patient activation may work together to influence HF self-care adherence, however more research is needed to understand these associations. Thus, the objectives of the current study are listed as follows: (1) Examine the relationships between patient activation, health literacy, and self-care in a diverse group of adults with HF and (2) Determine the effects of patient activation and health literacy on HF self-care adherence.
Methods
Participants and Procedure
A correlational, cross-sectional, survey design was used to study a convenience sample of 174 adults with HF who were recruited in July 2020 (Meraz et al., 2022). Institutional Review Board (name of IRB blinded for review #1577400-1) approval was acquired prior to initiating study activities. Qualtrics (www.Qualtrics.com), a commercial online sampling company, was utilized to recruit participants who met the study inclusion and exclusion criteria from panels of people who had had been pre-screened and profiled for research surveys. Qualtrics was chosen to achieve a study sample that represented the general population of HF patients by race. Stratified random sampling was applied to gain a racially diverse sample of approximately 50% persons of color. Persons of color, in this study, were defined as anyone who did not self-identify as White.
For this study, inclusion criteria were adults over 18 years old, able to read English, taking prescribed medications for HF, and living independently in a community-setting. Exclusion criteria were a history of a heart transplant and drug-related HF. Individuals who potentially met the inclusion and exclusion criteria were invited to take part in the study and volunteered by following a survey link offered by Qualtrics. To minimize selection bias, potential study participants were asked survey questions to confirm study eligibility. The survey immediately closed for ineligible participants. Eligible participants advanced to an online consent form.
Sample size was determined by an a priori power analysis to achieve 95% power for detecting a moderate-small effect size of 0.15 (f2) at an α-level of .05. This sample size allowed for control of possible confounding effects of demographic variables (age, educational level, income, marital status, gender, and race) on independent variables.
Measures
Heart Failure Self-Care
Heart failure self-care adherence was assessed with the European Heart Failure Self-Care Behavior Scale (EHCScB-9; Jaarsma et al., 2003). The EHCScB-9 is a valid and practical measure of HF self-care behaviors (i.e., weighing daily, adhering to medications, exercising, adhering to diet recommendations, and monitoring HF symptoms). This 9-item, Likert-type scale, has a standardized score from zero to 100 with a score above 70 indicating adequate self-care. The EHFScB-9 is an internally consistent and valid measure of HF-related self-care behaviors with 40 a Cronbach alpha of .80 (Lee et al., 2013). In this study, the Cronbach alpha was .81.
Patient Activation
Patient activation was assessed using the Patient Activation Measure (PAM; Patient Activation Measure® (PAM®). Insignia Health, 2020). The PAM is a 13-item 5-point Likert scale. Raw scores are transformed to a scaled score of 0 to 100. The higher the patient activation score the higher the self-care activation. The PAM divides individuals into one of four patient activation levels based on the empirically derived activation score (Patient Activation Measure® (PAM®). Insignia Health, 2020). The higher the patient activation score, the higher the activation level. Patient activation levels are: (1) believing that self-care is important, (2) having the confidence and knowledge necessary to act, (3) taking action to maintain and improve one’s health, and (4) staying the course even under stress (J. H. Hibbard et al., 2004). In psychometric testing, person reliability (Rasch 0.85 and 0.87) and criterion validity (Cohen’s kappa 0.8, 0.9, 0.9; p < .001 for all three kappas) were acceptable in measuring activation levels. Reliability of the PAM has been established with a Cronbach alpha of .87 (J. H. Hibbard et al., 2004). The Cronbach alpha in the current study was .91.
Health Literacy
Health literacy was measured using the Newest Vital Sign (NVS) health literacy instrument (Weiss et al., 2005). This 6-item measure assesses participants’ ability to read and use information from a food nutrition label. One point is given for each correct answer for a maximum of 6 points. A score of four or greater specifies adequate health literacy. The NVS has demonstrated adequate reliability with a Cronbach alpha of .76 (Weiss, 2018). Similarly, the Cronbach alpha for the NVS in the current study was .77.
Data Analysis
Data was analyzed using SPSS version 27.0. Correlational statistics were used test the associations between patient activation, health literacy, and HF self-care. Linear regression models were used to check the predictive effects of patient activation and health literacy on HF self-care adherence. Patient activation and health literacy were entered into the preliminary linear regression models as independent variables and HF self-care was entered into the models as a dependent variable. Alpha (α) of .05 was used to determine significance levels.
To summarize demographic characteristics of the sample, continuous variables were reported as means and standard deviations and discrete variables as counts and percentages. Descriptive statistics were calculated for each study variable. Distributions of the continuous and ordinal variables were examined to check for normality. Chi-square and t-tests were used to test for differences between patient activation, health literacy, HF self-care adherence and demographic variables. The direction and strength of associations between study variables were measured with correlational tests. As seen in past studies, correlations of patient activation were tested using continuous PAM scores (0–100), activation levels 1 to 4, and dichotomized activation levels of low (level 1 and 2) and high (level 3 and 4; Aung et al., 2016; Masterson-Creber et al., 2017).
Results
Sample Demographics and Descriptive Statistics
The mean age of the sample (n = 174) was 62.22 (SD = 13.78) and ages ranged from 19 to 91 years. Forty-nine percent (n = 85) of participants were male and 51% (n = 89) were female. A study sample of approximately 50% persons was color was nearly achieved with 48.5% (n = 84) of participants self-identifying as persons of color (Black 24.1%; Asian 11.5%; Other 8.6%; American Indian or Alaskan Native 2.9%; Native Hawaiian or Pacific Islander 1.1%) and 51.5% (n = 90) as White. Of the study sample, 6.9% (n = 12) self-identified as Hispanic. The majority of participants were married (61.5%, n = 107) college graduates (60.9%, n = 106). The annual household income was relatively evenly distributed in the study sample with 36.2% (n = 63) reporting <$50,000, 36.8% (n = 64) reporting between $51,000 and $100,000 and 27% (n = 47) reporting > $100,000. Most participants reported living in urban (n = 107) versus rural areas (n = 67). A small number of participants (10%; n = 17) were hospitalized for HF in the 6 months prior to the survey. Please see Table 1 for full demographic characteristics of this sample.
Demographic Characteristics of the Sample a (n = 174).
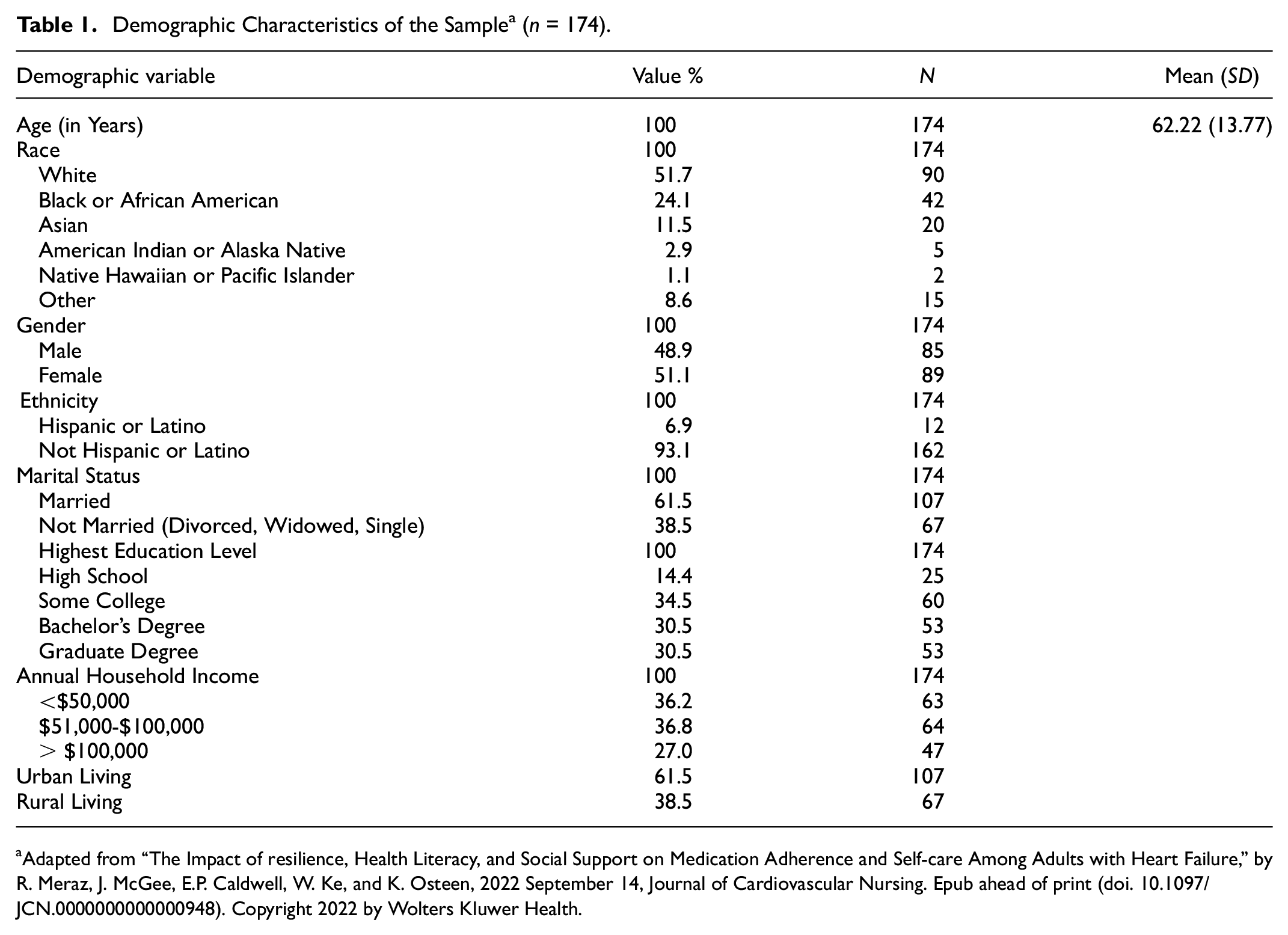
Adapted from “The Impact of resilience, Health Literacy, and Social Support on Medication Adherence and Self-care Among Adults with Heart Failure,” by R. Meraz, J. McGee, E.P. Caldwell, W. Ke, and K. Osteen, 2022 September 14, Journal of Cardiovascular Nursing. Epub ahead of print (doi. 10.1097/JCN.0000000000000948). Copyright 2022 by Wolters Kluwer Health.
Instrument Scores
Heart Failure Self-Care
The mean self-care score was 54.26 (n = 174; SD = 21.16), indicating inadequate self-care among the study sample. There were no significant differences in HF self-care adherence by race, age, gender, marital status, level of education, annual household income, or urban versus rural among this study sample (n = 174).
Patient Activation
The mean patient activation score was 70.03 (n = 174; SD = 17.2), indicating an activation level of 3 (i.e., taking action to maintain and improve one’s health). The mean activation level was 3.2 (SD = 0.846). Grouped by low (levels 1–2) and high (levels 3–4), participants on average had low patient activation (M = 1.82, SD = 0.389). There was no significant difference in patient activation by race, age, gender, marital status, annual household income, urban versus rural, or educational level in this study sample (n = 174).
Health Literacy
The mean NVS health literacy score of this sample was 3.71 (n = 174; SD = 1.94), indicating low health literacy. There was no significant difference in health literacy scores by gender or level of education. Health literacy scores were significantly lower in unmarried (M = 3.22, SD = 2.03; t(172) = 2.637, p = .009) participants under the age of 65 (M = 3.04, SD = 2.11; t(172) = −4.407, p < .001) compared to those aged 65 and over (M = 4.28, SD = 1.59) and married (M = 4.01, SD = 1.84). Those with an annual household income < $50,000 had significantly lower health literacy scores (M = 3.16, SD = 1.961; F(2,171) = 4.06, p = .019) compared to those in the $51,000 to $100,000 (M = 4.02, SD = 1.89) and >$100,000 (M = 4.02, SD = 1.87) groups. Health literacy (t = 4.367, p < .001) was significantly lower among persons of color compared to White participants. Persons of color in this study were more likely to be under the age of 65 (M = 56.64; X2 = 19.160; df = 1; p < .001; Cramer’s phi = −.332), unmarried (X2 = 4.305; df =1; p = .038; Cramer’s phi = .157) and have an annual household income < $50,000 (X2 = 5.735; df = 1; p = .017; Cramer’s phi = −.182) compared to White participants (Meraz et al., 2022).
Correlations
Health literacy, patient activation, self-care scores and demographic variables (i.e., age, gender, race, marital status, educational level, income) were correlated to identify relationships amongst variables. Based upon the bivariate correlations, there were several significant correlations amongst independent variables. There was a significant, small correlation between greater HF self-care and living in an urban area (r = .154, p < .05). There was a significant, moderate positive correlation between health literacy and age (r = .301, p < .01) and race (r = .300, p < .01). There was also a significant, small positive correlation between health literacy and marital status (r = .185, p < .05), education level (r = .175, p < .05) and income (r = .186, p < .05). In other words, participants who were older, White, married, college educated, and had higher annual household income also had better health literacy. There were no significant correlations between participant demographics and patient activation. Please see Table 2 for all correlations amongst variables.
Spearman’s Correlations Amongst Variables.
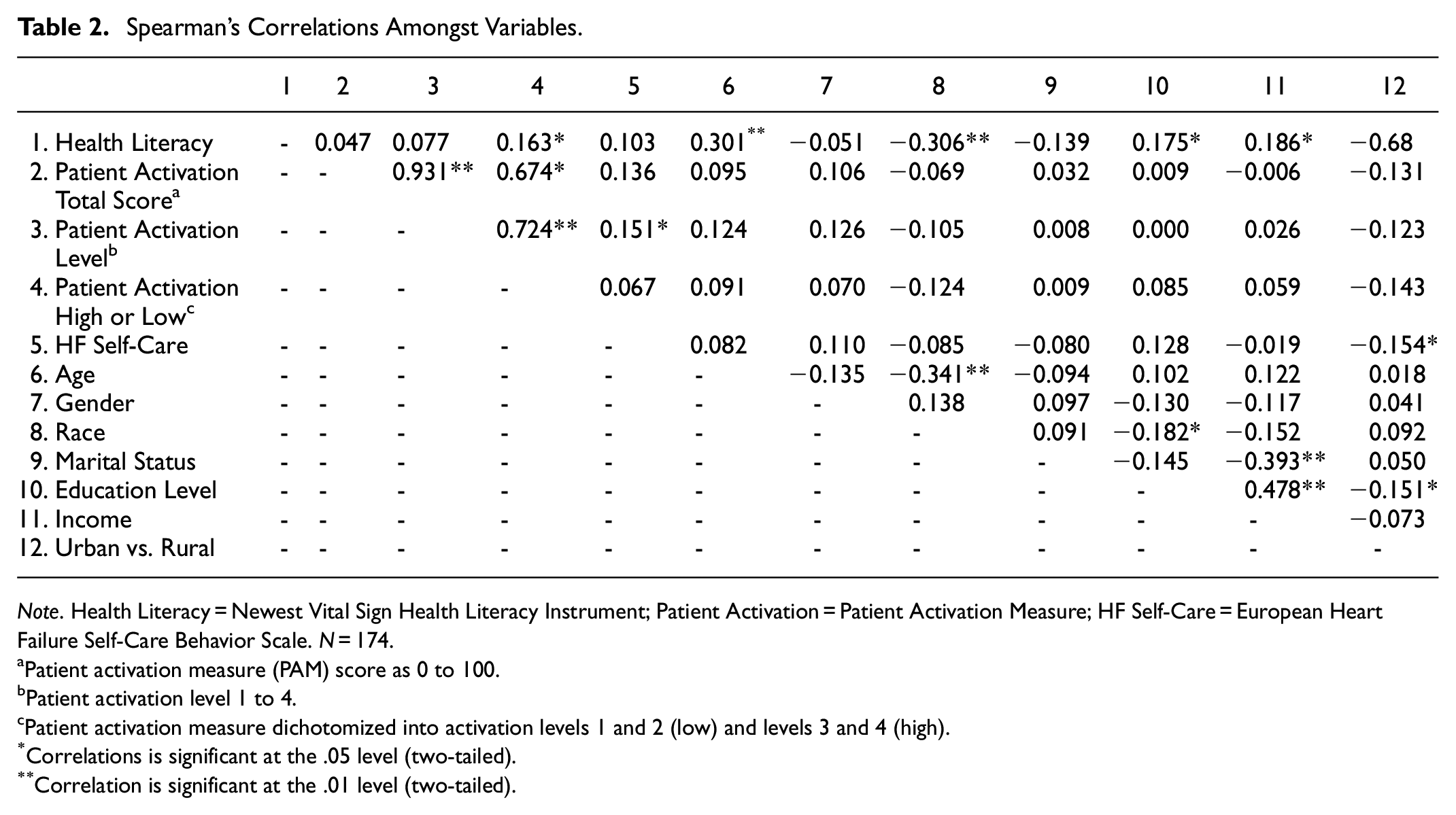
Note. Health Literacy = Newest Vital Sign Health Literacy Instrument; Patient Activation = Patient Activation Measure; HF Self-Care = European Heart Failure Self-Care Behavior Scale. N = 174.
Patient activation measure (PAM) score as 0 to 100.
Patient activation level 1 to 4.
Patient activation measure dichotomized into activation levels 1 and 2 (low) and levels 3 and 4 (high).
Correlations is significant at the .05 level (two-tailed).
Correlation is significant at the .01 level (two-tailed).
Multivariate analysis was performed to explore the relationships among HF self-care, patient activation, and health literacy (See Table 2). Results showed no significant relationship between HF self-care adherence and health literacy scores. There was a small, positive correlation between health literacy and dichotomized high/low activation levels (r = .163; p < .05), indicating that the higher the health literacy the higher the activation level. Neither patient activation scores (0–100) nor patient activation levels (level 1–4) were significantly associated with health literacy. There were no significant correlations between patient activation as a continuous score (0–100) and other study variables. There was a small, positive correlation between HF self-care and the patient activation levels only (level 1–4; r = .151; p < .05). However, when a simple linear regression was conducted, patient activation level was not a significant predictor of self-care adherence (B = 0.173, p = .064). Table 3 summarizes the results of the regression analyses.
Regression Analysis Summary for Predicting HF Self-Care.

Discussion
This study aimed to examine the relationships among patient activation, health literacy, and self-care adherence among 174 adults with HF. Contrary to our expectations, patient activation and health literacy were not significant predictors of self-care adherence in adults with HF. Patient activation level (level 1–4) was only mildly positively correlated with HF self-care adherence. Health literacy had no significant influence on HF self-care adherence in this sample, and there was only a weak positive correlation between health literacy and patient activation when the levels were grouped as low or high.
The relationships between demographic variables and HF self-care adherence, patient activation, and health literacy were also examined. Our study sample was ethnically and racially representative of the HF population, with almost half (48.5%) of study participants being persons of color. The study sample was also relatively evenly distributed by males and females. There were no significant differences in HF self-care adherence by race, age, gender, marital status, annual household income, or level of education in this study sample. Greater heart failure self-care was mildly associated with living in an urban area, which may be due to better access to care (Loccoh et al., 2022). There were no significant associations between demographic characteristics and patient activation. Health literacy, however, was significantly lower among persons of color and those who were unmarried, under the age of 65 years, and whose household income was less than $50,000 annually.
The finding that patient activation may not be a reliable predictor of HF self-care is an important finding, because there is a growing interest in involving patient activation in interventions aimed at improving HF self-care adherence and overall HF outcomes (Lin et al., 2020). Our finding is inconsistent with previous investigators who demonstrated that highly activated HF patients are more likely to adhere to self-care behaviors. One possible explanation may be differences in study sample characteristics. For example, two investigations reporting a significant influence of patient activation on HF self-care were among rural HF patients (Do et al., 2015; Young et al., 2017). Most of the participants in this study were urban residents, and there was a small association between better self-care and urban living. Although Masterson-Creber et al. (2017) demonstrated that higher patient activation predicted better self-care among 96 urban HF patients, the study participants were hospitalized and may have had different clinical characteristics than our study sample, such as more advanced HF. More research is needed to further explore the association between patient activation and HF self-care adherence and to find out if urban-rural living or clinical characteristics are factors in the relationship between patient activation and HF self-care.
It is plausible that the weak correlation between patient activation levels and HF self-care adherence demonstrated in this current study may help to explain the inconsistent effects of patient activation interventions on HF self-care behaviors. For example, in one study, among 84 HF patients who were randomized to an individualized, patient activation intervention or usual care, there was a significant increase in patient activation scores in the intervention group but no significant improvement in self-care adherence (Shively et al., 2013). In a study by Young et al. (2016), there was no difference in HF self-care between the patient activation intervention group and the control group in 100 HF patients discharged from the hospital. In fact, the intervention group had a higher hospital readmission rate (Young et al., 2016). A study with a sample size of 475 HF patients had better results, although there was only a small effect size between the intervention and control groups (Meng et al., 2016). Overall, more research is needed to confirm the usefulness of patient activation measures for evaluating changes in HF self-care behaviors.
It is important to consider that HF self-care is a group of health-promoting activities aimed at managing HF symptoms (i.e., weighing daily, eating a low salt diet, taking medications as prescribed) rather than a single activity. Each self-care activity is a unique behavioral phenomenon, involving different skills, stimuli, and decisions. If each HF self-care activity was evaluated individually, it is possible that patient activation may influence one behavior more than another. For example, multiple investigators report that adherence to medications, which is a HF self-care activity, is significantly influenced by patient activation (Graffigna et al., 2017; Parchman et al., 2010). How activation influences each self-care behavior individually is still unclear and is an area that should be explored.
The weak positive correlation between health literacy and patient activation demonstrated in this study is consistent with previous studies that indicate that health literacy and patient activation are separate concepts and not strongly correlated (J. Hibbard, 2017; Sheikh et al., 2016). Of note, the significant correlation between patient activation and health literacy in this study was only demonstrated when patient activation was dichotomized into low and high groups. Similar to our findings, a study of 151 adults with HF demonstrated that activated patients were more likely to perform self-care activities regardless of their health literacy status (Jacobson et al., 2018). The current study serves to confirm that increasing health literacy may not impact patient activation and increasing patient activation may not impact health literacy.
The current study did not demonstrate an association between health literacy and HF self-care adherence. Likewise, previous research findings are inconclusive regarding an association between health literacy and adherence to HF self-care (Chen et al., 2011; Como, 2018; Erünal & Mert, 2020). For example, a study by Erünal and Mert (2020) demonstrated that better health literacy was significantly associated with better HF self-care. Conversely, Jacobson et al. (2018) found no relationship between degree of health literacy and self-care behaviors. One explanation may be that there are varying definitions and measures of health literacy (Cajita et al., 2016).
There may be other mechanisms linking health literacy to self-care decisions, such as psychological or social characteristics (Jaarsma et al., 2017; Kuhn et al., 2021; Meraz, 2020; Meraz et al., 2023; Riegel et al., 2022). Of note, previous studies have reported (Cajita et al., 2016) that health literacy is lower among younger persons of color and those who were socioeconomically disadvantaged (Delgado & Ruppar, 2017; Muvuka et al., 2020). Cognitive function and age may also be factors that determine whether health literacy has an impact on self-care adherence (Cajita et al., 2016). Although health literacy may benefit the overall health of HF patients (Cajita et al., 2016), it may not be a key factor in improving self-care adherence. More research is needed to fully understand the role of health literacy in HF self-care adherence decisions.
Limitations
This study used self-report instruments, which are subject to reporting bias, such as inaccurate recollection of behaviors and socially desirable responses. The survey was administered online, limiting the generalizability to those with access to technology and those who are comfortable with an online survey. Confirmation of study eligibility was also self-report, which means participants may have provided responses that were not accurate. Future research should replicate the study using a longitudinal study design to confirm associations between patient activation, health literacy, and self-care adherence. Furthermore, there were no open-ended questions in this study. Adding a qualitative component to the study may help researchers better understand the relationship between health literacy, patient activation, and HF self-care.
Implications
This study has implications for practice and ensuing research studies. This study observed that HF self-care adherence was poor. Thus, developing clinical and educational strategies with the goal of improving patients’ self-care adherence is recommended. Our results imply, however, that attempts to improve self-care adherence in patients with HF should not focus solely on levels of patient activation or health literacy. Despite numerous investigations on HF self-care, practitioners are still challenged to understand patient’s self-care adherence decisions and effective interventions. Future research should continue to explore modifiable factors that motivate decisions for self-care adherence. Lastly, although the current study sample was fairly distributed by income, race, and gender, future research should also consider the influence of other social determinants of health such as economic stability, culture, and access to care.
Conclusion
This study examined the relationships among measures of patient activation, health literacy, and HF self-care adherence in racially and ethnically diverse sample of adults with HF. There was no predictable relationship between patient activation, health literacy and HF self-care adherence. There was only a small, positive correlation between patient activation level and HF self-care adherence. More research is needed to elucidate the influence of patient activation and health literacy on HF self-care behaviors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by Baylor University IRB # 1577400-1