
Abstract
Universal health insurance is widely believed to be a key strategy for improving health services. However, few studies have examined whether it increases the use of modern contraceptives. The purpose of the present research is to determine whether the policy of incorporating family planning services into the national health insurance policy in Indonesia (Jaminan Kesehatan Nasional [JKN], implemented in 2016) has led to an increase in the use of modern contraceptives. The data were obtained from the 2019 Government Performance and Accountability Survey (GPAS; Total = 46,220 married women aged 15–49 years). The findings show that women who are covered by the health insurance scheme for non-poor families (JKN non-PBI) are 19.12 times more likely to use modern contraceptives than women who are uninsured. Women who are covered by health insurance scheme for poor families (JKN PBI) are 17.04 times more likely to use modern contraceptives than those who are uninsured. These results are robust against predisposing, enabling and need factors associated with modern contraceptive uptake (i.e., education, family economic status, religion, knowledge of modern contraception, age at time of first marriage, perception of the ideal number of children, number of children born alive, and area of residence). The findings suggest that the government should expand health insurance benefits in order to increase the uptake of modern contraceptives, particularly among disadvantaged group within communities.
Introduction
Modern contraceptive methods are far more effective in preventing pregnancy than traditional methods (Heuveline & Hirschman, 2015). The United Nations (2020) reported that global modern contraceptive uptake has increased from 42% in 1990 to 49% in 2019. Although a relatively high proportion of women in Southeast Asia want to prevent pregnancies, modern contraceptive uptake in this region is below the world average, with only 47% of married women aged 15 to 49 years using modern contraceptives. Bearak et al. (2020) estimated that the unintended pregnancy rate in Southeast Asia declined by 21% between 1990 and 2019 and that the abortion rate during that same period increased by 21%. At the same time, the proportion of unintended pregnancies ending in abortion rose from 42% to 65% in the region (Bearak et al., 2020).
In Indonesia, modern contraceptive use was reported at 55% in 2019, while the maternal mortality rate remained high at 305 per 100,000 live births (BKKBN, 2019). The prevalence of modern contraceptive usage in the country declined from 59% in 2015 to 55% in 2019, with unmet needs for family planning at 12% in the same year (BKKBN, 2019). The highest percentages of unmet needs were reported in the eastern regions of Indonesia, particularly in Papua (21%), West Nusa Tenggara (17.1%), Maluku (16.8%), and Southeast Sulawesi (16.7%; BKKBN, 2019). Hence, ensuring access to modern contraceptives in this region is one of the government’s key strategies for reducing maternal mortality and advancing reproductive, maternal, and childhood health throughout the country.
One of the main obstacles to accessing modern contraceptives in most developing countries is financial (Fagan et al., 2017). To reduce the financial barrier, more inclusive health insurance policies with family planning services such as free modern contraceptives have been introduced in many countries, including Indonesia (Fagan et al., 2017). Since 2016, the Indonesian government has included family planning services in the JKN program. Without health insurance, individuals would pay approximately IDR 500,000 (USD 35.70) for an implant, IDR 6 to 7 million (USD 428.60) for MOW and MOP services, IDR 40,000 (USD 2.80) per injection, and IDR 400,000 (USD 28.60) for intrauterine device (IUD) services. Within the integration scheme, all of the abovementioned modern contraceptive services are available free of cost to all JKN members. In Indonesia, there are two types of membership in the health insurance system: JKN non-PBI, or contributing recipient membership, for citizens who are not considered poor and who thus pay for their insurance; and JKN PBI, or recipient membership, a scheme for poor families who are unable to pay and whose payments are thus covered by the government (Mboi, 2015).
Studies on the effect of health insurance on modern contraception services have yielded inconclusive results. In Turkey, Celik and Hotchkiss (2000) found that the odds of using modern contraceptives were higher for women who had health insurance than for those who were uninsured. However, Snyder et al. (2018) and Kavanaugh and Pliskin (2020) reported that the effect of health insurance on modern contraceptive use was strongly linked to a specific type of health insurance. By comparing women in the United States with private health insurance, Medicaid insurance, and no insurance, they found that those who received Medicaid obtained prenatal coverage later in pregnancy and had fewer medical visits than uninsured women. In China, Chen et al. (2017) also documented that the design of health insurance was linked to the use of maternal health services. Other studies have found no association between health insurance and modern contraceptive use (Ahmed & Mosley, 2002; Sheff et al., 2019). These inconsistent findings suggest a need for further investigation of the association between health insurance policies and modern contraceptive use within various contexts in order to better understand the mechanisms by which such policies are linked with the uptake of modern contraceptives.
Health insurance promotes the use of modern contraceptives via two channels. The first is the reduction of financial barriers to services. Reichhardt (2020) explains that family planning methods such as modern contraceptives are often expensive in the long term, though recurrent costs are relatively modest. Integrating modern contraceptive services into health insurance levels the costs of the services. Fagan et al. (2017) reported that individuals are more inclined to use health services that are pre-paid than those that are paid at the time of care. Moreover, Chen et al. (2017) highlighted that integrating family planning into health insurance may reduce financial barriers to other health services as their costs are spread across both users and non-users.
The second channel is the availability of additional funding for family planning service providers to spend on improving their services. In the Indonesian context, the implementation of the decentralization reform significantly reduced operational budgets for local family planning agencies because most local governments do not prioritize family planning in their development programs. Hence, integrating family planning into the national health insurance scheme strengthens the financial capacity of local family planning agencies to implement various programs encouraging citizens to use contraception. Yarger et al. (2017) suggested that the inclusion of family planning in universal health insurance schemes encourages family planning organizations to improve the quality and accessibility of their services, thus increasing citizens’ demand for contraception.
In Indonesia, a number of studies have investigated the effect of health insurance on contraceptive uptake. However, most of the research was either conducted before the incorporation of family planning services into the universal health insurance scheme or focused on a specific region, such as a province or district. Using Indonesian Social Economic Data from 2005, Samarakoon and Parinduri (2020) reported that Askeskin, or health insurance for the poor, encourages women to use contraceptives. Using Indonesian Social Economic Data from 2012 to 2016, Nasution et al. (2020) concluded that, until 2016, the implementation of the universal health insurance program did not increase the prevalence of contraceptive usage in Indonesia. In the district of Sleman, Sulistiawan et al. (2021) reported that out-of-pocket expenditures for contraceptive services were significantly associated with the type of health insurance owned and the types of contraceptive methods used. Accordingly, the present study examines the influence of the universal health insurance policy (JKN) following the integration of family planning services into the policy in 2016. The 2019 Government Performance and Accountability Survey (GPAS) of Indonesia enabled the analysis.
There is evidence that socio-demographic, reproductive, and obstetric characteristics, as well as previous experience with service usage, are linked to contraception use (Fagan et al., 2017; Tesfaye et al., 2018; Zhang et al., 2019). However, these characteristics must be examined in a systematic way in order to identify the most relevant barriers and facilitators to contemporary contraceptive usage. In this study, we used the Andersen and Newman Behavioral Model (ANBM) for health-care utilization for identifying predisposing, enabling and need factors that influence women’s decisions to use (or not use) modern contraceptives (Andersen & Newman, 2005). Predisposing factors are socio-cultural characteristics of an individual that exist prior to their health condition (i.e., age at first marriage, women’s knowledge about modern contraception, and women’s educational level). Enabling factors refer to the means or logistics required to obtain modern contraceptive services (i.e., place of residence, family income, and religious background), while need factors are the most immediate causes for health service use and reflect the individual’s perceived health status (i.e., ideal number of children).
In the next section, we detail the methods and variables measured in this study.
Methods
Study Design and Data
This is a cross-sectional data analysis based on the 2019 Indonesian Government Performance and Accountability Survey (GPAS), which was conducted from April to November 2019 by the Indonesian family planning agency (BKKBN) in collaboration with universities in 34 provinces and Indonesia’s Central Bureau of Statistics. Ethical clearance for this survey was granted by the BKKBN Ethical Committee Board (Number: 454/LB.02/H4/2019).
Respondents were selected based on stratified multistage random sampling (see Figure 1). A number of enumeration areas were systematically selected from 34 provinces and 514 districts. The enumeration areas were selected based on wealth index and urban/rural classification, which were determined by the Indonesia Central Bureau of Statistics based on the Indonesian Population Census 2015. As a result, 1,935 villages were designated as enumeration areas. In each village, a list of enumeration clusters was created, and 35 households were chosen from each cluster using a systematic random sampling method. This yielded a study sample of 67,725 households and 46,220 married women aged 15 to 49 years old (BKKBN, 2019).
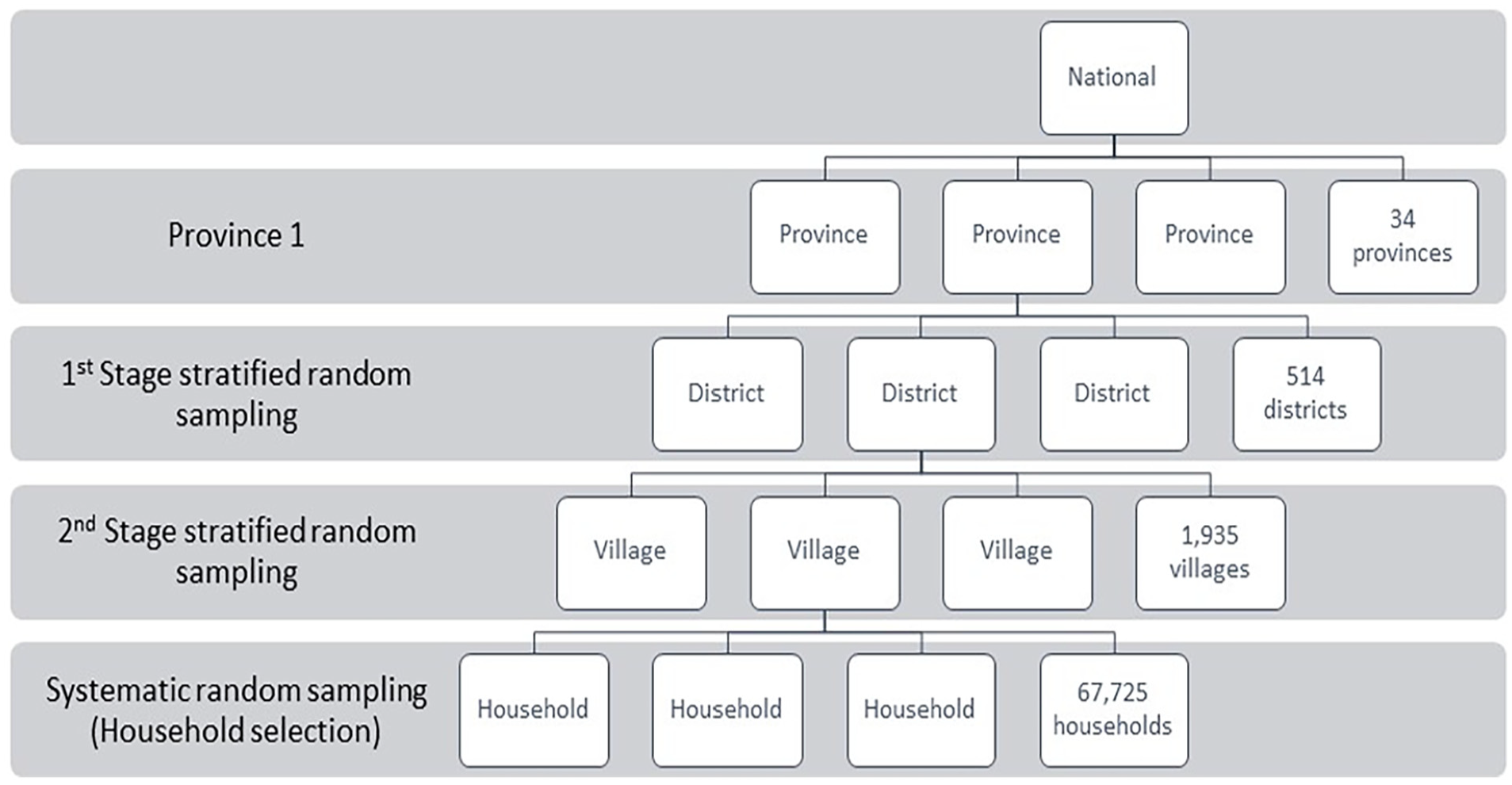
GPAS 2019 stratified random sampling procedures.
Before collecting field data, a pilot survey was conducted to assess the extent to which respondents understood the survey questions, as well as to better understand the mechanism of household listing strategies. Pre-testing and trials were carried out in March 2019 in Depok Sub-District, Depok City, West Java. Interviewers went door-to-door in the selected cluster (BKKBN, 2019). The results of the pilot survey indicated that all respondents could easily understand the questions. Overall, the survey took 30 to 40 minutes to complete.
Variables Measured
The dependent variable is modern contraceptive use. In the survey, each respondent was asked whether she was currently using family planning/contraception methods. If the answer was yes, the interviewer then asked her which family planning/contraceptive method(s) she was currently using.
The interviewer carefully read the possible responses to the respondents: (1) female sterilization (such as tubal ligation, laparotomy, or voluntary surgical contraception for women), (2) male sterilization (such as vasectomy or voluntary surgical contraception for men), (3) the contraceptive pill (oral contraceptives), (4) intrauterine contraceptive device, (5) contraceptive injection (Depo-Provera), (6) implants (Norplant), (7) female condom, (8) male condom (such as prophylactic and rubber), (9) diaphragm, (10) contraceptive foam, (11) contraceptive jelly, (12) lactational amenorrhea method, (13) standard days method, (14) periodic abstinence (such as rhythm and calendar method), (15) withdrawal (coitus interruptus), and (16) other traditional methods.
Yes or no answers were provided and the interviewer was to tick the boxes in accordance with the respondent’s responses. A dummy variable was created to measure modern contraceptive use (0 if respondents reported not using modern contraceptive, 1 if respondents reported using one of the family planning/contraceptive methods numbered 1 to 12 above).
The main independent variable in this study is ownership of health insurance. We categorized health insurance ownership into four categories: uninsured (code = 0, as the reference group), JKN PBI (code = 1), JKN non-PBI (code = 2), and covered by other health insurance (code = 3). Respondents were asked whether or not the family planning/contraceptive methods they used were covered by health insurance. If the answer was yes, the interviewer then asked the type of health insurance that was paying for the services (i.e., JKN PBI, JKN non-PBI, and other types of health insurance).
Based on the Andersen and Newman Behavioral Model (ANBM) framework (Andersen & Newman, 2005), we included some predisposing factors collected in the survey (i.e., age of respondent, age at first marriage, women’s knowledge of modern contraceptives, and women’s educational level), enabling factors (i.e., area of residence, family income, and religious background), and need factors (i.e., ideal number of children) as explanatory variables to control the relationship between health insurance ownership and modern contraceptive use. We categorized age into six categories: 15 to 19 years, 20 to 24 years, 25 to 29 years, 30 to 34 years, 35 to 39 years, 40 to 44 years, and 45 to -49 years (as the reference group).
Knowledge of modern family planning is a key determinant in changing attitudes and practices concerning modern contraceptive uptake among women (Lopez et al., 2013). We coded knowledge of modern contraceptives into two categories: 1 if respondents reported knowledge of eight modern contraceptive methods (male sterilization, female sterilization, contraceptive injection, contraceptive pills, implant, condom, intrauterine contraceptive device (IUD), and lactational amenorrhea method) and 0 if respondents reported not knowing these eight modern contraceptive methods.
Studies have widely documented that more educated women postpone marriage and childbearing and are more likely to utilize modern contraceptives (Larsson & Stanfors, 2014). In this study, respondent level of formal education was classified into three categories: lower (elementary school or less, code = 1, as the reference group), moderate (junior secondary education, code = 2), and higher (high school or more, code = 3).
The importance of family income for contraceptive uptake has been widely documented in the literature (Celik & Hotchkiss, 2000). In this study, family income was measured by ten ladders of income which then we categorized into tertiles (Celik & Hotchkiss, 2000): low-income status (third tertile, code = 1, as the reference group), middle-income status (second tertile, code = 2), and high-income status (first tertile, code = 3).
The role of religion in contraceptive uptake is an issue of significant debate in the literature, suggesting that religion cannot independently predict modern contraceptive use (Beson et al., 2018). We classified respondent religion into six groups: Muslim (as the reference group), Catholic, other Christian, Hindu, Buddhist, and other religions.
The literature indicates that women who want more children are less likely to use contraceptives (Withers, et al., 2015). In this study, we used two measures: respondent’s desired number of children and number of children born to date. In the survey, respondents were asked the specific number of children they would have if they could go back to the time when they did not have any children and could choose exactly the number of children they would have in their entire lives. We categorized respondents’ answers into two categories: 0 if respondents answered two or fewer and 1 if respondents answered more than two children. For the number of children born to date, we classified responses into two categories: 0 if the respondent had two or fewer live born children and 1 if the respondent had more than two live born children.
Statistical Analyses
The analysis was performed using Stata version 17.0. Descriptive statistics were used to present the socio-demographic characteristics of respondents as well as type of contraception used and health insurance ownership. Multivariate logistic regression was performed to test the association between type of health insurance ownership and modern contraceptive use. In the first model, we estimated only the association of type of health insurance ownership and modern contraception use. In the second model, we included all explanatory variables (predisposing, enabling, and need factors) to control for the relationship between each type of health insurance and modern contraceptive use. We used odds ratio (OR) with a p < .05 and a 95% confidence interval to determine statistical significance. Unadjusted and adjusted odds ratios were determined in order to investigate the effect of each type of health insurance on the probability of modern contraceptive use. National population weights associated with sampling design were utilized to address the bias that might occur due to the sampling design employed in the survey.
Results
Respondents’ Characteristics
Table 1 presents the respondents’ characteristics. Rural areas had a higher proportion of modern contraceptive users than urban areas (55% for rural and 45% for urban). Middle-income families were also more likely to use modern contraception than lower- and higher-income families (48.8% for middle income, 26.6% for higher income, and 24.7% for low income). The proportion of modern contraceptive users increased with age, with the age group 35 to 39 years having the highest proportion (60.2%). Of the respondents who used modern contraceptives, 37.4% had a higher level of education, 35.7% had a moderate level of education, and 26.8% had a lower level of education. The majority of respondents were Muslims who used modern contraception (92.1%). The proportion of women using modern contraceptives was higher among unemployed women than among employed women (64.9% and 35.1%, respectively).
Respondents’ Socio-Demographic Characteristics Based on Their Use of Modern Contraceptives.

Only a small percentage of respondents with health insurance used modern contraceptives (4.3% for JKN PBI, 1.7% for JKN non-PBI, and 0.2% for other insurances). Respondents who reported knowing about eight modern contraceptive methods used contraception more frequently (81.5%). Respondents who were 15 to 24 years old at the time of their first marriage used modern contraceptive more frequently than others (39.3% for 15–19 years and 39.9% for 20–24 years). Modern contraceptives were being used by 64.4% of women who said they wanted fewer than two children. Among women with two or fewer live born children, 65.8% used modern contraceptives.
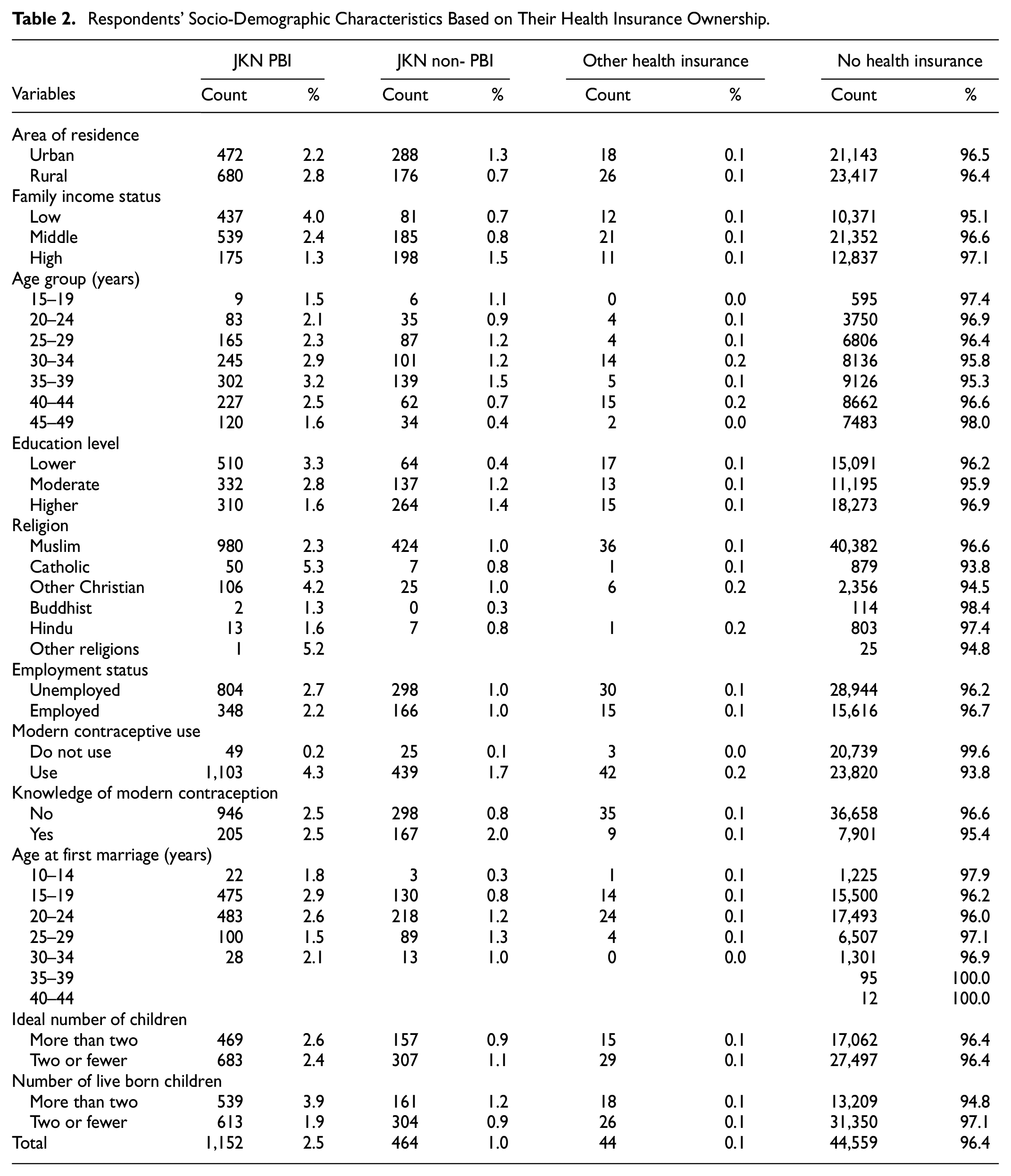
Table 2 describes the socio-demographic characteristics of respondents based on health insurance ownership. Only 3.4% of women had health insurance. JKN PBI was available to 69.4% of the women with health insurance. There is no discernible difference between urban and rural dwellers with respect to health insurance ownership. Women from low-income families had nearly three times more access to JKN PBI than women from high-income families. Women from higher-income families had roughly twice as much access to JKN non-PBI. There is no discernible difference in JKN non-PBI ownership between low- and middle-income families. Women aged 35 to 39 years had the most access to health insurance among those covered by JKN PBI and non-PBI. Women with lower levels of education had roughly twice as much access to JKN PBI as men. There is no substantial difference in health insurance ownership between employed and unemployed women. Among those covered by JKN PBI, women who used modern contraception were significantly more likely to use their insurance than those who were not using modern contraception (4.3% compared to 0.2%). However, among women covered by JKN PBI, those who were using modern contraceptives had about three times more access to insurance than those who were not using modern contraceptives. Among those covered by JKN PBI, women between the ages of 15 and 19 years and those between the ages of 20 and 24 years had the greatest access to health insurance. Women with more than two children had roughly twice the access to JKN PBI and non-PBI as women with two or fewer children.
Respondents’ Socio-Demographic Characteristics Based on Their Health Insurance Ownership.
Multivariate Logistic Regression Results
Table 3 depicts the odds ratio estimate of modern contraceptive use among 46,220 women. Model 1 shows the results of logistic regression before inclusion of predisposing, enabling, and need factors. All health insurance types were significantly associated with modern contraceptive use. Respondents who were covered by JKN non-PBI were 27.72 times more likely to use modern contraception use than uninsured respondents. Respondents covered by JKN PBI were 26.61 times more likely to use modern contraception than uninsured respondents. Respondents covered by other types of health insurance were 13.74 times more likely to use modern contraception than those who were uninsured.
Odds Ratio Logistic Regression Results.
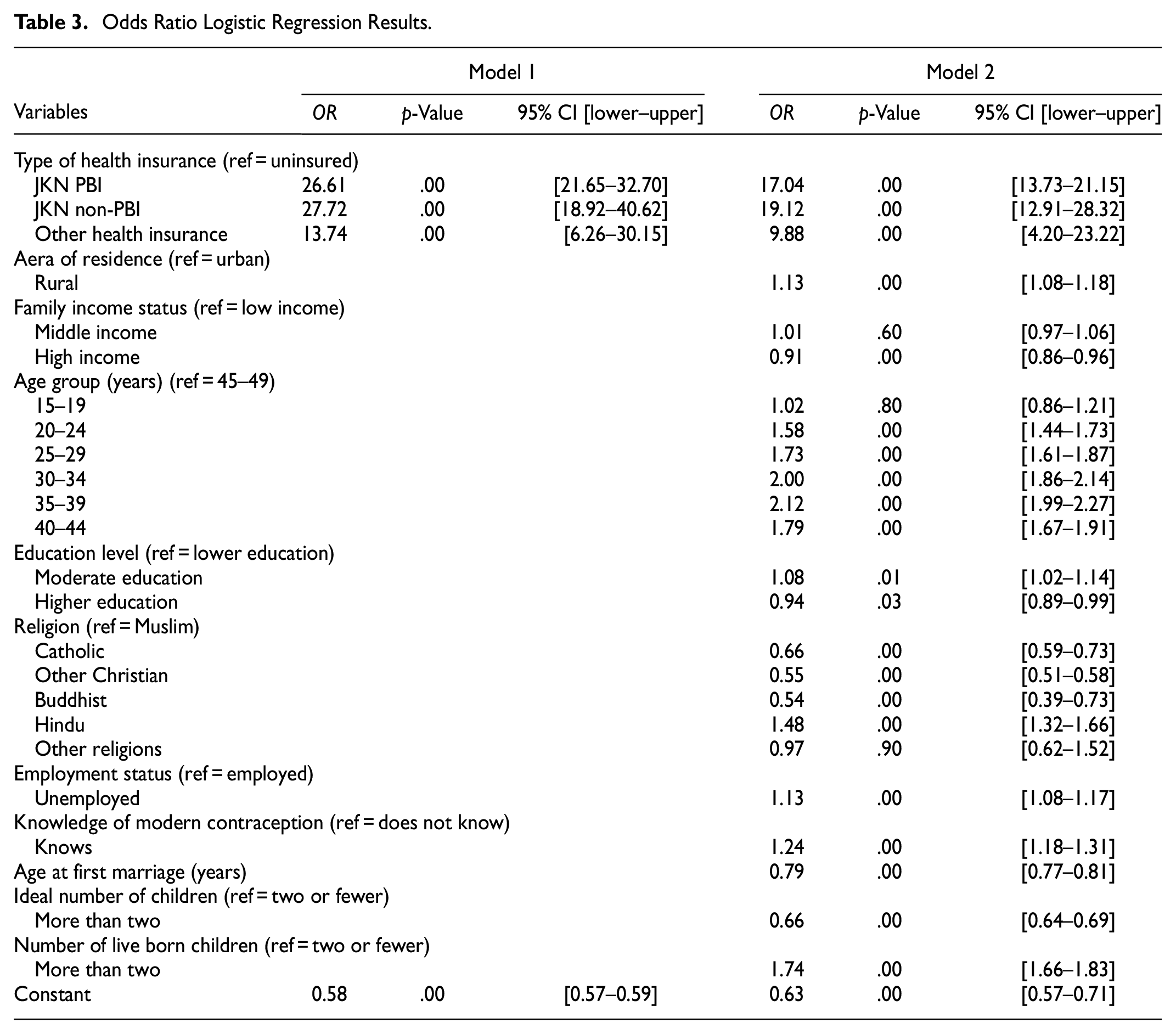
Model 2 shows estimated results of logistic regression after inclusion of predisposing, enabling, and need factors associated with contraception use. All types of health insurance continue to be strongly linked to use of modern contraceptives. Respondents covered by JKN non-PBI were 19.12 times more likely to use modern contraceptives than uninsured respondents. Accordingly, respondents covered by JKN PBI were 17.04 times more likely to use modern contraception than respondents who were uninsured. Those who had any other type of health insurance were 9.88 times more likely to use modern contraception than those with no health insurance.
The prevalence of modern contraceptive use among rural married women was 1.13 times that of urban married women. Women from wealthier families were less likely to use modern contraceptives than women from poorer families (OR = 0.91, p = .00). No significant association was found between the relationship of middle-income families and uptake of modern contraceptives. Women’s age was significantly associated with modern contraceptive use. The highest odds of using modern contraceptives were found in women aged 35 to 39 years (OR = 2.12, p = .00).
Interestingly, women with a higher educational level were less likely to use modern contraceptives than women with a lower educational level (OR = 0.94, p = .03). However, women with a moderate level of education were more likely than women with a lower level of education to use modern contraceptives (OR = 1.08, p = .01). Hindus were more likely to use modern contraceptives than Muslims (OR = 1.48, p = .000). However, Catholics, Other Christians, and Buddhists were less likely to use modern contraceptive than Muslims. Unemployed women were more likely to use modern contraceptives than employed women (OR = 1.13, p = .00). Respondents with awareness of the eight above-mentioned modern contraceptive methods were more likely to use modern contraceptives than those without this awareness (OR = 1.24, p = .00). Age at first marriage had a negative relationship with modern contraceptive use. Women who reported having more than two children and an ideal number of children greater than two were more likely to use modern contraception (OR = 0.66, p = .00 and OR = 1.74, p = .00 respectively).
Discussion
In 2016, the Indonesian government began including family planning services in the JKN scheme. The integration of family planning services into the system was intended to address financial barriers to modern contraceptive services under the decentralized family planning system. Accordingly, the objective of the current study is to examine whether the policy aim was achieved. Considering some predisposing, enabling and need factors, we discovered that JKN ownership, both PBI and non-PBI, was associated with modern contraceptive uptake 3 years after implementation of the policy. Women who were covered by JKN non-PBI were 19.12 times more likely to use modern contraceptives than uninsured women. Women covered by JKN PBI were 17.04 times more likely to use modern contraceptives than uninsured women. Women with health insurance were 9.88 times more likely to use modern contraception than women with no health insurance. Our descriptive analyses also show substantial differences in modern contraceptive use among women with health insurance, particularly those with the JKN PBI scheme, which is designed to help low-income families.
Our key findings confirm prior studies which reported the benefits of health insurance on family planning uptake (Reichhardt, 2020; Fagan et al., 2017; Chen et al., 2017; Yarger et al., 2017). Prior research has found that health insurance ownership lowers financial barriers to family planning and increases access to it in Rwanda, Ghana, and Turkey. In Turkey, Celik and Hotchkiss (2000) reported that integrated modern contraceptive services within national health insurance substantially reduced out-of-pocket costs, which in turn increased the uptake of modern contraceptives among women. In Rwanda, Bucagu et al. (2012) confirmed the benefit of integrated family planning services in health insurance to sustain the use of modern contraceptives. Similarly, our study found that JKN PBI in Indonesia substantially increases modern contraceptive use among women from poor families.
Among predisposing factors, women’s age was associated with modern contraceptive uptake. Women in the 30 to 34 years and 35 to 39 years age groups had the highest odds of using modern contraceptives. These findings confirm prior studies showing that the practice of using modern contraceptives was more common among women in the 30 to 39 years age group compared with older than 30 to 39 years age groups (Thorvaldsen & Islam, 2012). The explanation for this could be that as women get older, they are more likely to already have the number of children they desire or to want to spread out their children’s births. Another possible explanation is that most women in the approaching menopausal stage have less sexual activity and are therefore less likely to use contraceptives (Lasong et al., 2020).
Age at first marriage was negatively associated with modern contraceptive uptake: older age at marriage was accompanied by a decrease in the use of modern contraceptives. This association gives a clear picture of decreasing odds with an increase in age at marriage which posits that when women marry later, there is a smaller chance that they will use modern contraceptives. One possible explanation is that women in Indonesia who postpone marriage are less likely to avoid pregnancies because their “delay,” which is not culturally expected, reduces the relative length of the childbearing phase. Using the Indonesian Demographic Health Survey (IDHS) 2017, Mahmud et al. (2021) also documented similar findings suggesting that when women marry at an older age, naturally, they will pursue their reproductive desire in a shortened reproductive period.
Studies have widely documented that more educated women postpone marriage and childbearing and are more likely to utilize modern contraceptives (Larsson & Stanfors, 2014). In contrast with these studies, we discovered that women with lower levels of education were more likely to use modern contraception than those with higher levels of education. One possible explanation for these findings is the increased access to JKN PBI of women from lower-income families. Another explanation is that women with a higher level of formal education have more knowledge and information about the side effects of modern contraception and thus prefer to use alternative family planning methods that are safer than modern contraception, for example, natural and non-hormonal methods of birth control which generally have a lower risk of side effects than hormonal contraception methods (Freundl et al., 2010). Nevertheless, our findings corroborate studies in Benin, Zimbabwe, and Bangladesh (Emina et al., 2014; Hossain et al., 2018). A study in Benin reported an inverse U-shaped curve relationship of formal education and modern contraception use, while in a study in Zimbabwe found that an increase in the proportion of women with secondary or more education does not correlate with modern contraception use (Emina et al., 2014). In Bangladesh, Hossain et al. (2018) found that the prevalence of modern contraceptive use was determined by access to free family planning services, not by women’s levels of formal education.
Rather than formal education, we found knowledge of modern contraceptives to be positively associated with the uptake of modern contraceptives in Indonesia. The odds of modern contraceptive uptake increase along with the number of modern contraceptive methods known by women. These findings confirm prior studies positing that knowledge about contraceptives is an important determinant of contraceptive use. Using 2019 GPAS data, Sari et al. (2021) found that knowledge of modern contraceptives was amongst the most important determinants of modern contraceptive uptake in West Java province. In Ethiopia, Lopez et al. (2021) documented that knowledge of long-term contraceptive methods was the main predictor of long-term contraceptive use. The authors highlighted that knowledge of modern family planning is a key determinant of changing attitudes and practices concerning modern contraceptive uptake among women.
Among enabling factors examined in this study, we found that urban residence and higher family income were negatively associated with modern contraceptive uptake. In contrast with prior studies in Nigeria, the Philippines, and Ghana (Celik & Hotchkiss, 2000), the prevalence of modern contraceptive use among women in rural areas was 1.16 times higher than among those living in urban areas. This evidence could point to improved family planning services as a result of the integration of family planning services into the universal health insurance scheme. For example, Mahmud et al. (2021) documented free mobile family planning service initiatives across local governments following the integration of the services into the JKN scheme. Many disadvantaged women in rural areas can now easily access various family planning services because of the availability of mobile family planning services. As stated in our descriptive findings, the prevalence of modern contraceptive use in rural areas was higher than in urban areas.
The improvement of family planning services following the integration of family planning services into the JKN scheme may also explain the linkage between family income and modern contraception use in our study. We found that women from higher-income families were less likely to use modern contraception than women from lower-income families. This may reflect the increased access to low-cost and/or free contraception that was made possible with the integration of family planning services into the JKN scheme. Another possible explanation is that women from higher-income families prioritize other factors, such as user control over one’s method or sexual acceptability, over effectiveness when deciding on the best choice of contraceptive method. Kavanaugh and Jerman (2018) found similar trends of negative association between economic status and contraceptive uptake in the United States, suggesting broader access to affordable and/or free contraception through various initiatives of family planning programs in the country.
Religion also influences contraceptive uptake in Indonesia. The odds of modern contraceptive uptake are higher among Hindus than Muslims. However, Christians, Catholics, and Buddhists are less likely to use modern contraceptives than Muslims. The role of religion in contraceptive uptake is an issue of significant debate in the literature (Beson et al., 2018; Wusu, 2015). This suggests that religion is not an independent predictor of modern contraceptive use. For example, a study in Nigeria documented that Muslim woman were more likely to never have used or not to be using modern contraceptives than Catholic and Protestant women. This may be explained by the larger proportion of women who are less educated, unemployed, and income poor in Muslim communities than in Catholic and Protestant communities in the country (Wusu, 2015). In the Indonesian contexts, Withers and Browner (2012) reported that the role of religious leaders and local customs determined the difference in modern contraceptive uptake among women of various religions.
Both need factors examined in this study showed significant associations with modern contraceptive use. Women whose ideal number of children was more than two had lower odds of using modern contraceptives than those who desired two or fewer children. These findings confirm prior studies in Indonesia which reported that women who wanted more children were less likely to use contraceptives than those who wanted fewer children, suggesting that women desiring to have a larger number of children tend not to use modern contraceptives (Withers et al., 2010). With regard to the number of live born children, our study shows that women with more than two live born children were more likely to use modern contraceptives than those with two or fewer children. This finding also confirms existing studies showing that the number of living children was linked to contraceptive use and that, as the number of living children grows, so does the likelihood of using contraception (Withers et al., 2010). For example, a study in Ethiopia reported that women who had two to three children were nearly three times more likely to seek modern contraception than women who had only one child. This may be because the more children a woman has, the more likely she is to desire to space or limit the number of children, and the more likely she is to use contraception (Kebede et al., 2019).
This study entails certain limitations. First, there may have been some recall bias in the data due to retroactive reporting of modern contraception uptake (Smith et al., 2018). Second, because contraception is a sensitive topic, respondents may have replied to the questions in a way that they believed would project a positive picture of themselves, exposing the results to social desirability bias. Third, because of the study’s cross-sectional design, the analysis can only provide evidence of statistical association and cannot infer cause-effect relationships. The interpretation of the study’s findings is complicated by concerns about reverse causality and selection bias. Further study using longitudinal panel data based on better measurement of modern contraceptive uptake is recommended to address these issues.
Despite its limitations, this study’s findings provide policymakers with valuable insights into how to improve modern contraceptive uptake in the setting of universal health care. First, when family planning is incorporated in the benefits of health insurance package, these synergies can improve the uptake of family planning services. Including family planning in the benefits of the health insurance package removes financial barriers and strengthens the infrastructure for service delivery, allowing these gains to be amplified. Changes in the delivery of family planning services induced by the careful design of health insurance systems can result in advances in understanding and social norms around family planning over time, speeding its acceptability and adoption. Second, the findings show that the prevalence of health insurance ownership in Indonesia remains very low. In order to broaden the benefits of universal health insurance for modern contraception uptake, the government should create various initiatives to encourage women and families to become involved in the program. For example, the government could provide a health insurance premium that is affordable for the general public; alternatively, premiums could be calculated based on income brackets. The findings of the study has also identified certain groups within which women are less likely to have health insurance, including low-income families living in urban areas.
Conclusion
Our study concludes that the incorporation of family planning services in the Indonesian Health Insurance Program (JKN scheme) is likely to increase the uptake of modern contraceptives. To broaden the benefits of the JKN scheme for modern contraceptive uptake, the government should develop a variety of initiatives to encourage women and families to participate in the national health insurance program.
Footnotes
Author Contributions
SS, EP, ME, AT, AR, and DP: prepared study design, collect data, conduct data analyses, and wrote the main manuscript. SS revised the manuscript. All authors reviewed the manuscript. All authors have contributed equally.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Universitas Brawijaya via Hibah Penguatan Pusat Studi 2022 Granted to Portsmouth Brawijaya Center for Global Health, Population and Policy Number 1666.1/UN.01/UB/2022. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Institutional Review Board Statement
The ethical clearance for this survey was granted from the BKKBN ethical committee boards number: 454/LB.02/H4/2019.
Informed Consent Statement
Informed consent was obtained by BKKBN from all subjects involved in the study. Written informed consent has been obtained from BKKBN to publish this paper.
Data Availability Statement
The raw data of GPAS 2019 were used in this study with permission from the Indonesia Family Planning Board or BKKBN. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.