
Abstract
This study aimed to assess the attitudes of Cambodian women toward menopause and its associating factors. A cross-sectional study design was used to examine the attitudes of 181 Cambodian women ages 40–60 years toward menopause using the Attitude toward Menopause (ATM) scale. The mean total attitude score was determined as 84.54 ± 11.55 on a scale of 35–140, indicating that most participants had negative attitudes toward menopause. Perimenopausal women had more negative attitudes (80.02 ± 9.19) while postmenopausal women had more positive attitudes (86.63 ± 12.07) and was statistically significant (p = .006). Perimenopausal women perceived menopause as a health concerning medical issue requiring treatment, and something unpleasant in their lives. Older age and employment were the independent factors associated with positive attitudes to menopause. Tailored menopausal interventions and counseling for women in perimenopause, and younger and unemployed women regarding the symptoms of menopause should be considered as crucial for midlife Cambodian women.
Introduction
Globally, an increase in the population of menopausal women has made their health a major medical issue (Santoro et al., 2015). It is estimated that by the year 2025 the total count of postmenopausal women will rise to 1.1 billion worldwide (Shifren & Gass, 2014).Cambodia, like many other developing countries, has an increasing number of aging women. In 2013, the total number of women above 40 years of age was more than 2 million, almost 15% of Cambodia’s total population (National Institute of Statistics, 2013). A national study in Cambodia that considered a woman in menopause if she did not have a menstrual period for at least 6 months before the survey for any reason other than pregnancy or postpartum amenorrhea, reported that 11.5% of women aged 30–49 are menopausal in the country (National Institute of Statistics et al., 2015).
Menopause is not only a biological event but also psychosocial (Rubinstein, 2013). Many women perceive it as a welcome relief from menses and the risk of pregnancy while those who desire children consider it an unwelcome event (Ande et al., 2011). Almost all (96%) of the respondents in a American study agreed that women should see a doctor during menopause, and 81% of them perceived menopause to be one of the biggest changes in a woman’s life (Huffman et al., 2005). Attitudes, perceptions, and expectations are some of the psychosocial phenomena surrounding menopause. Both women in midlife and health professionals agree that attitudes toward menopause play a potential role in the experience of menopause, including its perceived severity (McGinnis et al., 2008). Though the occurrence of menopause involves the same physiological events for all women worldwide, it is assumed that attitudes to menopause differ by a range of cultural and social variables, which in turn may affect the menopausal experience and symptom reporting (Ayers et al., 2010). General characteristics, such as age, residence, education, parity, income, menopausal status, and marital status, also predict women’s attitudes toward menopause (Jassim & Al-Shboul, 2008; Noroozi et al., 2013). For instance, in Shiraz, the 34-item Attitude toward Menopause scale (ATM) returned a total attitude score of 102.7 ± 11.8 (of a possible 71–135), which reflects the positive attitudes of the participants toward menopause (Ghaderi et al., 2010). Whereas Korean women showed negative attitudes toward menopause, with a mean score of 60.00 ± 10.12 (of a possible 33–108) when measured with a modified, 27-item ATM tool (Kwak et al., 2014). In studies of Asian women conducted across nations, 87% of educated Pakistani women were found to have positive attitudes toward menopause (Memon et al., 2014). A study among Bengali postmenopausal women in India reported that those who have lived more years after menopause showed a signifying trend toward positive attitude on menopause (Dasgupta & Ray, 2017). Another study from Bahrain reported that premenopausal women displayed more negative attitudes toward menopause than peri- or postmenopausal women (Jassim & Al-Shboul, 2008). Similarly, in other studies, women of a better employment status, and widowed or divorced women were reported to have more positive attitudes toward menopause than their counterparts (Noroozi et al., 2013). Women with urban residence and higher per capita monthly expenditure expressed more positive attitude toward menopause in India (Dasgupta & Ray, 2013).
Positive attitudes help women live well with menopause while negative attitudes make their menopausal transition troublesome (Ayers et al., 2010; McGinnis et al., 2008); a positive attitude toward menopause is also closely associated with better quality of life for menopausal women (Li et al., 2016). Considering that such attitudes vary with culture, assessing Cambodian women’s attitudes toward menopause is a preliminary step for predicting the knowledge gap and may also aid in health talks and counseling within a cultural context. The life expectancy of a Cambodian female at birth is estimated to be 76.1 years by 2023 (National Institute of Statistics & World Health Organization, 2017). The high number of aging women and increasing life expectancy of women shows the need for careful planning by the healthcare system to meet their health needs. However, to our knowledge, studies regarding menopause are scarce or non-existing in Cambodia and no studies have been found that investigate the attitudes toward menopause of Cambodian women. This preliminary study aims to evaluate the attitudes of menopausal women toward menopause and associating factors in the Cambodian context. The findings of this study document women’s perceptions of menopause, which can further be used as facilitators of rational intervention for this group of women in Cambodia.
Theoretical Framework of the Study
The theoretical framework of this study was developed based on previous studies (e.g., Dasgupta & Ray, 2013; Jassim & Al-Shboul, 2008; Noroozi et al., 2013) and is presented in Figure 1. We expected the menopausal status, sociodemographic information (e.g., age, residence), lifestyle (e.g., physical exercise, smoking), and reproductive history (e.g., parity, abortion(s)) were individually associated with attitude toward menopause while controlling for each other.
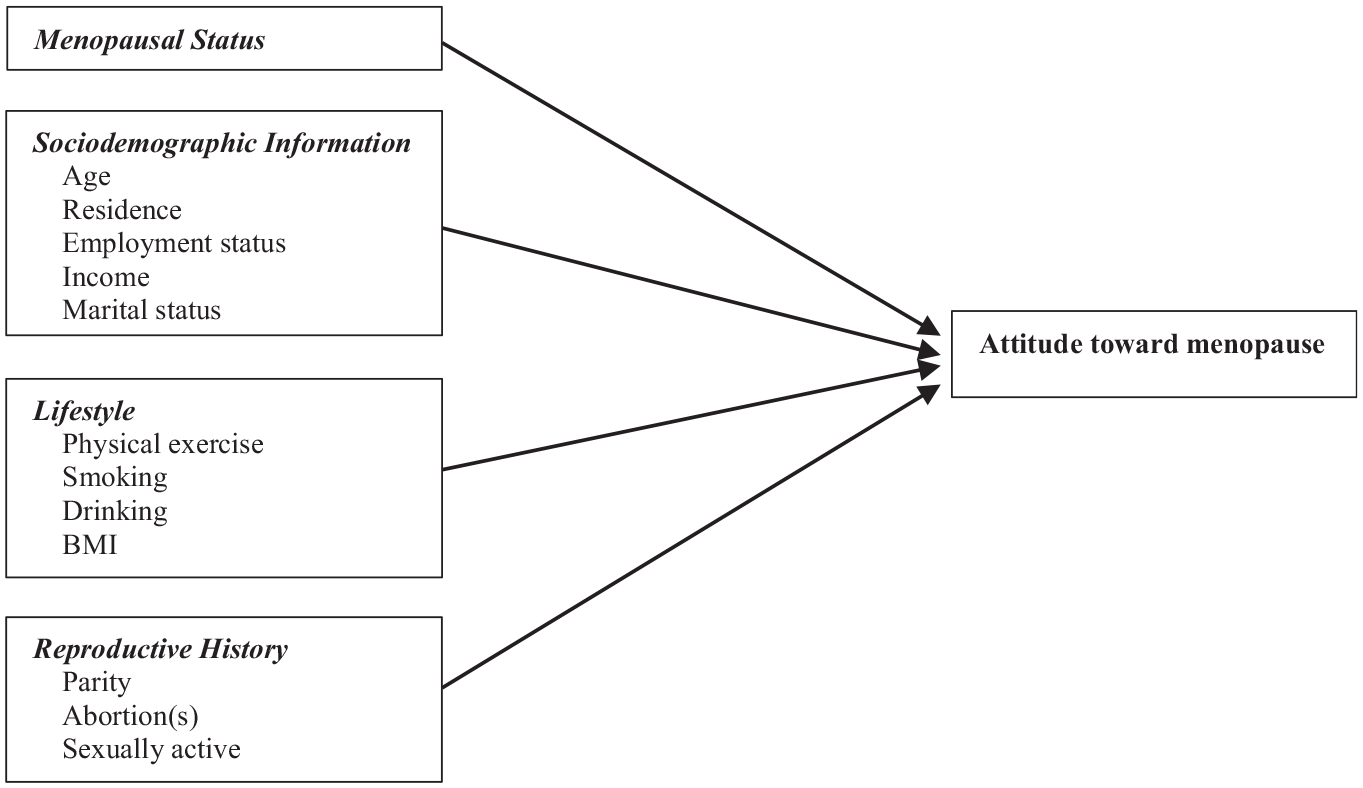
Theoretical framework of the study.
Methods
Participants and Recruitment
The participants of this cross-sectional study were 181 Cambodian women aged 40–60 years with the ability to answer the questionnaire with the assistance of an interviewer. Pregnant or breastfeeding women and women with medically induced menopause were excluded from the study. Convenience selection of three rural provinces (Kandal, Kampong Speu, and Kampong Chhnang) and one urban area (Phnom Penh) was done for the data collection. A sample size of 105 was calculated through G*Power version 3.1.9.2, considering a maximum of five variables included in the multiple regression analysis, a level of significance of .05, and an effect size of .2. To ensure accuracy, a further 76 samples were added. This study protocol was approved by the Human Subjects Committee of “X” University, the Cambodia National Ethics Committee for Health Research, and the Ministry of Health, Cambodia.
Measures
Attitudes Toward Menopause (ATM)
Neugarten et al. (1963) developed the ATM scale to assess attitudes toward menopause. It consisted of 35 statements (16 positive items and 19 negative items) on menopause, and participants had to indicate their level of agreement or disagreement with each statement (Table 1). All items were scored on a 4-point Likert scale ranging from 1 (disagree strongly) to 4 (agree strongly). Negative items were scored inversely so that higher scores indicated more positive attitudes (Ghazanfarpour et al., 2015; Kısa et al., 2012). A total score, ranging from 35 (most negative) to 140 (most positive), was calculated by summing the scores of all the items. The cut-off point of the scale was the mean score, that is, 87.5 points. The hypothesis was that women who receive 87.5 points or higher have positive attitude (Erbil & Gumuşay, 2018). The Cronbach’s alpha of the ATM scale for American women has been reported to be .64 (Huffman et al., 2005), and .84 for Iranian women (Ghazanfarpour et al., 2015); the Cronbach’s alpha for the current sample was .80.
Attitude Toward Menopause Scale.

Note. Instructions: These statements are some things other women have said about menopause or change of life. Indicate your level of agreement or disagreement with each statement by circling (1) for agree strongly, (2) for agree to some extent, (3) for disagree somewhat, or (4) for disagree strongly. If none of the possible answers seem to fit exactly the way you feel, select the one that comes closest to the way you feel. Please circle only one number for each statement.
All items were scored on a 4-point Likert scale ranging from 1 (disagree strongly) to 4 (agree strongly). Negative items (highlighted in bold) were scored inversely so that higher scores indicated more positive attitudes.
Menopausal status
Menopausal status was determined by the Study of Women’s Health across the Nation (SWAN) guidelines (Avis et al., 2001): (a) premenopausal: women reporting menses in the previous 3 months without any irregularity; (b) early perimenopausal: women who have had menstrual bleeding in the previous 3 months but with increasing irregularity in cycle length over the past year; (c) late perimenopausal: women without menses in the previous 3 months but who had menses in the previous 12 months; and (d) postmenopausal: women without any menses in the previous 12 months (not due to any medication, pregnancy, or severe weight loss). Early and late perimenopausal groups were collectively categorized into a single perimenopausal group in our study due to the small number of samples in the two individual groups.
General characteristics
Data were gathered on demographic characteristics (e.g., age, residence, education level, employment, monthly personal income, marital status, BMI, physical exercise, smoking, drinking), reproductive history (e.g., menopausal status, parity, abortion, sexually active), and disease/infection-related health characteristics (e.g., perceived health and life state) based on the literature review. Perceived life and health status was rated on a Likert scale of 0–10. Information on height and weight was self-reported by the participants. The WHO guidelines for Asia and the Pacific were used to calculate body mass index (BMI), and was categorized as underweight (<18.5 kg/m2), normal (18.5–22.9 kg/m2), overweight (23.0–24.9 kg/m2), and obese (≥25.0 kg/m2) (World Health Organization [WHO], 2000).
Development of the Khmer version of measurements
A Khmer version of this tool had yet to be developed. Two professional translators specializing in the health field therefore created a Khmer translation using the back-translation technique (Chen & Boore, 2010). The consistency of the two versions was confirmed by a panel of experts (local women’s health doctors and nurses from a Phnom Penh hospital). Based on their reviews, minor modifications were made. For instance, to gain clarity “the change of life” was translated simply as “menopause.” The discussions and meetings between the authors and the panel of experts ended after the readability, language simplicity, and suitability of the Khmer version was confirmed. A pilot study was conducted on 30 women to assess its reliability; however, they were not included in the main study.
Data Collection
The in-person meetings were conducted by four local nursing students (all female) on a one-on-one basis following extensive training on the purpose of the study, the contents and administration of the questionnaire, and how to approach the participants and document their responses accurately. Permission was obtained from the respective village leaders before approaching the participants, and fully informed written consent was taken from all participants prior to the data collection; participation of the respondents was on a voluntary basis. The questionnaire was read to the participants in consideration of illiterate participants and to avoid error. Participants were assured of confidentiality and interviews were conducted in a private space of the women’s homes or an offset corner of a public space without any external disturbances. A total of 181 women completed the questionnaire, a response rate of 94%. At last, each participant was provided a small gift to express thanks and appreciation of their time. The data collection period was from July 27, 2017 to August 25, 2017.
Statistical Analysis
The general characteristics of the participants were analyzed using frequency and percentages. A p-value of .05 was considered statistically significant. The normality of the data was confirmed through graphical observation and formal tests. Using SPSS Version 20.0, the data were compared by the Kruskal-Wallis calculation. Parametric analysis of variance (ANOVA) with Duncan or t-test and multiple linear regression (Enter) analyses were performed to predict attitudes toward menopause. The ATM total scores was the dependent variable and only the significant variables in the ANOVA analysis (menopausal status, age, employment, physical exercise, abortions) were entered as the independent variables in the multiple regression analyses.
Econometric Model of the Multiple Linear Regression Analyses

Y denotes the dependent variable, the ATM total attitude scores, and the parameter β0 is an intercept and β1 ~β5 are the regression coefficients associated with X1 = menopausal status, X2 = age, X3 = employment status, X4 = physical exercise, and X5 = abortion(s), respectively. ε is the random error component reflecting the differences between the observed and fitted linear relationship.
Results
The general characteristics of the participants are shown in Table 2. The study included 43 women (23.8%) in the premenopausal group, 45 (24.9%) in the perimenopausal group, and 93 (51.4%) in the postmenopausal group. Among all, 34.8% were from Phnom Penh and 65.2% were from the provinces. Less than one-third (29.8%) had above primary education, and 86.2% were employed, with 64.1% of them earning less than or equal to US$100 monthly. Most participants were married (62.4%), had normal BMI (39.8%), and do not practice physical exercise (61.9%). Only 12.2% self-reported as current drinkers while 2.8% reported as current smokers. More than half (60.8%) had anywhere from one to four children and 38.7% of the women had experienced at least one abortion. At the time of the study, almost half (49.7%) of the women reported as sexually active. A visual analog scale (0[lowest] to 10[highest]) rated participants’ satisfaction with their own health as a mean of 5.49 ± 1.45 (SD) and toward life as a mean of 5.42 ± 1.39 (SD).
Demographic Characteristics by Menopausal Status (N = 181).

Table 3 shows the Kruskal–Wallis test comparing the means of the attitudes toward menopause items across menopausal status. Perimenopausal women, compared with women of any other status, had statistically more negative attitudes toward menopause for many negative items, such “A woman should see a doctor during menopause” (p < .001), “Menopause is one of the biggest changes that happens in a woman’s life” (p = .027), and “Menopause is an unpleasant experience for a woman” (p = .021). On the other hand, postmenopausal women had statistically stronger positive attitudes toward menopause for many positive items, such as “Women are generally calmer and happier after the change of life (after menopause) than before” (p = .008), “Women generally feel better after menopause than they did for years” (p < .001), “A woman has a broader outlook on life after the change of life (after menopause)” (p = .015), and “Many women think menopause is the best thing that ever happened to them” (p = .001).
Mean Attitude Toward Menopause by Menopausal Status.
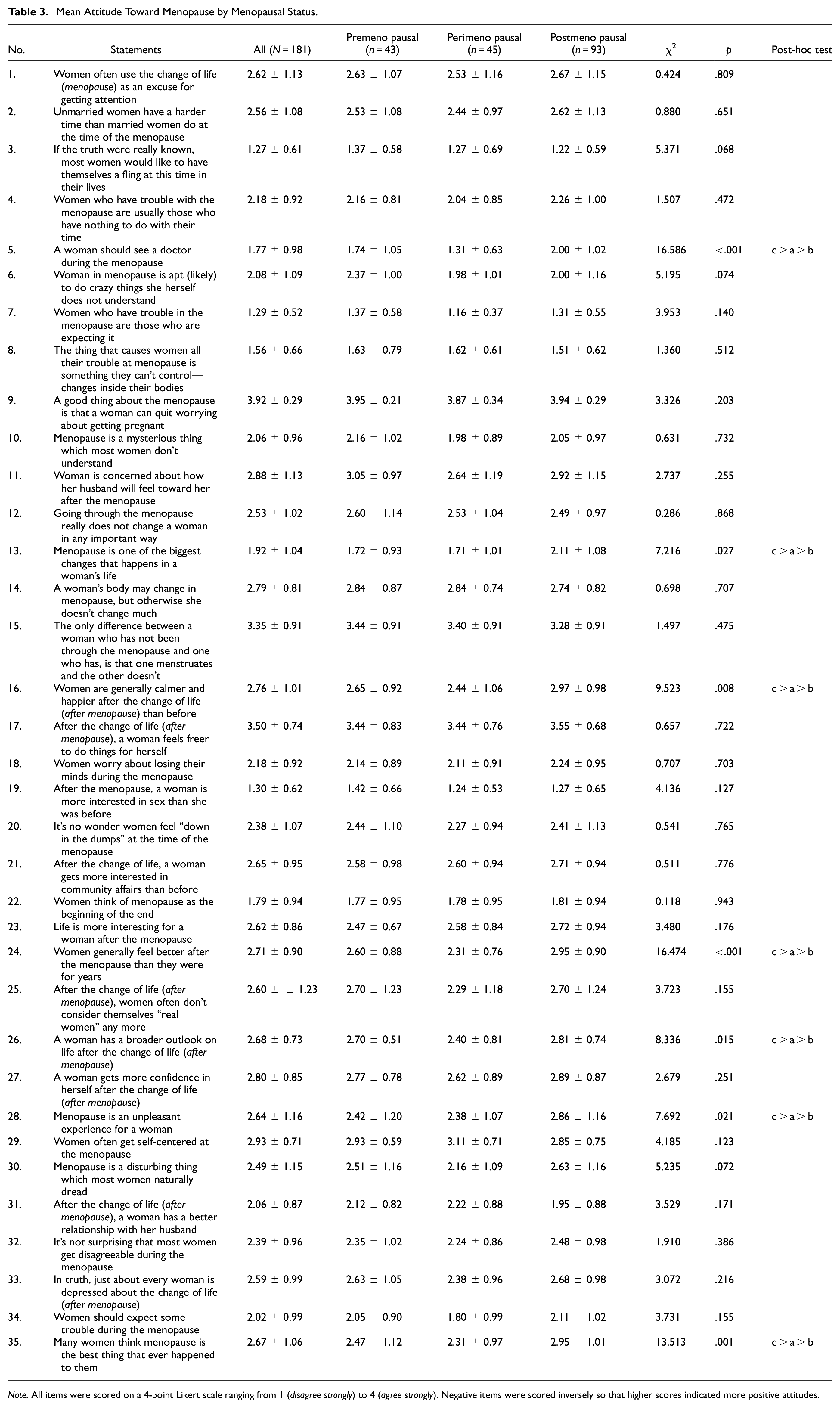
Note. All items were scored on a 4-point Likert scale ranging from 1 (disagree strongly) to 4 (agree strongly). Negative items were scored inversely so that higher scores indicated more positive attitudes.
Table 4 shows the total attitude scores by participant characteristics. The mean and standard deviation of the total attitude score was 84.54 ± 11.55 (range 35–140, with 140 the most positive). The total attitude score was significantly (p = .006) higher for postmenopausal women (86.63 ± 12.07) than premenopausal women (84.72 ± 11.53), followed by perimenopausal women (80.02 ± 9.19). The total attitude score was higher (p = .051) in women who exercised 1–4 days a week (88.59 ± 9.23) versus those who do not (84.49 ± 11.85). In univariate analysis, significantly more positive attitudes were seen for women of the age group 51–60 (86.64 ± 11.84, p = .003), employed women (85.35 ± 11.33, p = .017), and women with no history of abortion (86.05 ± 11.12, p = .027). No statistically significant associations were observed with other variables investigated in the study.
Total Attitude Scores by Participant Characteristics.

After adjusting for confounding factors, multivariate regression analysis determined that perimenopausal transition was significantly associated with overall attitude toward menopause. Perimenopausal women showed significantly negative attitudes than did women in premenopause (β = −0.212, p = .017) (Table 5). The independent factors responsible for the variance in attitude were age and employment status. It was observed that older women, of age 51–60, showed significantly stronger positive attitudes (β = 0.211, p = .031) than younger ones. Employed women were more likely to have more a positive attitude (β = 0.186, p = .009) than those who were unemployed. Other factors did not have any effect on attitude.
Factors Altering the Attitude Toward Menopause.

Note. Confounding variables (only the significant ones in ANOVA) age, employment status, exercise, and abortion(s) were controlled.
Discussion
A woman’s attitude toward menopause alters her menopausal experience. Understanding women’s perceptions of menopause will be of benefit to healthcare providers. The paucity of research on such attitudes among Cambodian women prompted this cross-sectional study.
Authors have suggested that women with positive attitudes better manage menopausal symptoms than those with negative attitudes (Ayers et al., 2010; Kwak et al., 2014). In the present study, it was found that Cambodian women had negative attitudes toward menopause as measured by the ATM scale (84.54 ± 11.55, range 35–140). This result is consistent with previous applications of the same scale in countries like Korea (60.00 ± 10.12, range 33–108) (Kwak et al., 2014) and Turkey (34.70 ± 8.56, range 0–80) (Kısa et al., 2012). The reason for the negative attitudes among Turkish women was their concern about sexuality after menopause; in particular, a majority of premenopausal respondents in that study agreed that women are often concerned that they will no longer have sexual intercourse after menopause (Kisa et al., 2012). Similarly, perimenopausal women in our study agreed more often with negative items, such as that one should see a doctor during menopause (p ≤ .001), that menopause is one of the biggest changes that happens in one’s life (p = .027), and that menopause is an unpleasant experience for a woman (p ≤ .021). This signifies that Cambodian women were concerned about menopause such that they felt it as a medical problem requiring treatment and something unpleasant in their lives. Educating midlife women about the normal parameters of the menopause experience, addressing any symptoms with possible treatments, and informing women that menopause can be a pleasant experience and does not necessarily call for medical consultation are interventions nurses and health workers can apply to help them reduce fear and increase confidence to deal with menopause in perimenopausal women. Further investigation of the concerns and reasons behind the negative attitudes of Cambodian women toward menopause with in-depth qualitative research is sorely needed to assist these women adopt positive attitudes that will ultimately help them have successful menopausal transitions.
Among each menopausal status, there were differences in how women reported their attitudes about menopause. Perimenopausal women had the lowest total ATM score, which implies that they tended to be less positive in attitude toward menopause, while postmenopausal women had the highest total ATM score and were more positive in their attitude toward menopause. This is consistent with other studies suggesting that those who have already gone through this bodily change become less susceptible to false stereotypes and find it less troublesome (Huffman et al., 2005; Jassim & Al-Shboul, 2008) while peri-menopausal women tend to express more anxiety and distress about menopausal symptoms than postmenopausal women, possibly due to uncertainty or lack of knowledge about physiologic and symptomatic events that occur during the menopausal transition or potentially due to going through irregular menstrual cycles and the climacteric symptoms (Dasgupta & Ray, 2013, 2017). The participants’ strong agreement with the positive items of the present study suggest that postmenopausal women see the benefits of menopause in their later life. They were seen as having expanded identities and happier experiences. The status of women gets elevated after reaching menopause or after living more years of menopause as evidenced by the studies in Asia (Dasgupta & Ray, 2013, 2017). Midlife Cambodian women, who are about to face or are facing menopause should be guided and encouraged by the health personnel to focus on positive perceptions of menopause, because how a woman’s life is affected by menopause depends in large part on how she views it (McGinnis et al., 2008).
Consistent with many other studies, older women in the present study displayed more positive attitudes than comparatively younger women in both univariate and multiple regression analyses. McGinnis et al., 2008 studied that women who do not experience menopausal symptoms intensely have a more positive attitude toward menopause. Though the present study did not aim to relate the experience of menopausal symptoms with attitudes toward menopause, there could be a possibility that the perimenopausal participants owing to their menopausal symptoms (especially, vasomotor symptoms) expressed more negative attitude. Also, young women have a tendency to connect menopause with aging, fear of the unknown, and fear of losing their femininity (Rubinstein & Foster, 2013). On the other hand, older women are more likely to have gone through the transition and are less worried about menopause. The fears and myths are alleviated as they experience menopause, which encourages a more positive attitude (Rubinstein & Foster, 2013). This finding also supports our earlier assertion that premenopausal women should be guided to develop positive attitudes toward menopause, by reducing their fears and clarifying their perceived uncertainties about menopause.
In both univariate and multiple regression analyses, it was seen that employed women had more positive attitudes than their counterparts. Employment influences the psychological condition of women, and has been considered a stress buffer for some women who are approaching menopause (Lee et al., 2010; Yanikkerem et al., 2012). Employed women seem to have more exposure to self-realization outside their home (Lee et al., 2010). All of these factors have been reported to contribute to favorable experiences of menopausal symptoms (Yanikkerem et al., 2012). In Cambodia, the proportion of women in formal sector-employment is lower than that of men, with 53.3% of the total female population engaged in family work in 2013 (National Institute of Statistics, 2013). This large portion of women are not exposed to self-realization opportunities outside their home. Creating more opportunities of employment for Cambodian women is necessary, and would aid them not only in their financial independence but also in self-realization and in improving their attitudes toward menopause and life more broadly.
In the present study, physical activity was significantly related to the total attitude score in bivariate analysis, but the relationship was not retained in the multiple regression analysis. Mostly, the influence of physical activity has been seen as positive for menopausal women. Elavsky in 2009 recommended physical activity for women to manage menopause, stating that it has long-term benefits for women undergoing the menopausal transition (Elavsky, 2009). One study claimed that women with higher levels of physical activity tended to have more positive attitudes (Li et al., 2016). However, another study claimed that physically active women are more likely to have negative attitudes toward menopause (Morrison et al., 2010). This difference in the studies’ results might be because of variation in the quality, kinds, and duration of physical activity, or the tools used to measure the level of physical activity of the respondents. Uniformity in these measures could give a reliable relation between physical activity and attitude toward menopause.
The diversity of attitudes across different parts of the world suggests that social and cultural factors play a role in shaping people’s attitudes toward menopause. Hence, for the management of menopause, a holistic approach to health, with physical, mental, psychological, social, and cultural aspects, should be taken when developing appropriate interventions (Afridi, 2017). Nurses can play a preventive role by evaluating women’s perceptions. Moreover, health counselors need to encourage women to share their fears, and remind them that the personal experience of menopause varies from person to person: personal plans for coping with the menopausal experience should be constructed with the collaboration of health personnel. Tailored pre-, peri-, and postmenopausal educational interventions depending related to the status and symptoms of menopause should be regarded as crucial for Cambodian midlife women. Menopausal clinics in health centers could be an effective option. Education has been studied as an important predictor of women’s positive attitudes toward menopause elsewhere (Kısa et al., 2012; Memon et al., 2014); however, it is not statistically significant in our study. The reason for this could be the low variation in education level (more than 70% had primary and below level education) or the use of only two education categories. Further study is recommended to explore attitude’s relationship with education among women with varied level of education so that its role can be made clear.
This study is subjected to the typical limitations of a cross-sectional study; it does not allow for the potentially casual relation of variables. Also, though the research assistants thoroughly explained the difficult terms and sentences in the questionnaire, it is not possible to evaluate the participants’ understanding. However, the Khmer version of the tool was adequate as proven by the high values of the Cronbach’s alpha coefficient, and knowledgeable research assistants were assigned to collect the data. Also, the study could have been further enriched with the correlational analysis between menopause symptoms and menopausal attitude. Moreover, self-reported answers might be exaggerated; participants’ answers could be influenced by social desirability or embarrassment and could be socially acceptable rather being truthful.
Conclusion
This preliminary study examined Cambodian women’s attitudes toward menopause, revealing that their general attitude was negative. Women in perimenopause, and younger and unemployed women reported more negative attitudes toward menopause. Promoting positive attitudes toward menopause is necessary so that Cambodian women can be lead through menopausal stage with less suffering and help them to maintain a sound mind and body. Other factors related to attitude were menopausal status, age, and employment status hence the health promotion activities for middle-aged women should be flexible and varying to serve women in a variety of situations. Since there are significant differences at the individual and cultural level in the experience of menopause, this study affirms the importance of offering a different viewpoint of menopause, from a cross-section of Cambodian society. Further study is warranted to assess the casual relationship between attitudes and symptoms. Qualitative studies should be designed to explore in depth the culturally sensitive insights, perceptions, and perspectives of this population toward menopause.
Footnotes
Acknowledgements
The authors would like to thank all the women who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.