
Abstract
Older adults show a lack of knowledge about dementia, treatments, and management although they are fearful of developing dementia. The purpose of this study was to examine the effects of a 6-week intervention on knowledge, attitude, fear, and prevention behaviors concerning dementia among older adults who resided in community. The study used a pretest-posttest design with nonequivalent control group. A total of 40 participants completed the study. The intervention group showed a significant decrease in the fear of dementia scores compared to the control group after the intervention(p < .05). However, no significant differences were found between the groups with respect to knowledge, attitude toward dementia, and healthy prevention behaviors. The intervention may be effective in decreasing older adults’ negative emotions concerning dementia, particularly, fear. The assessment of the fear toward dementia may help identify individual causes and triggers and provide tailored interventions.
Introduction
Dementia is a clinical syndrome where cognitive abilities such as memory, language skills, judgment skills, motor skills, and performance functions are impaired, causing disruption to daily social life and professional performance. Alzheimer’s disease usually accounts for 60% to 80% of dementia, and cerebrovascular disease and Lewy body disease represent 5% to 10% cases each. Around 50% cases of dementia have more than one cause (Alzheimer’s Association, 2019). As the elderly population increases, dementia is expected to affect approximately 135 million people worldwide by 2050 (Prince et al., 2013). In South Korea, about 794,000 people aged 65 or above are estimated to be suffering from dementia in 2019, with a prevalence of 10.3% currently and an estimated 16.1% by 2050 (National Institute of Dementia, 2020a, 2020b). The prevalence is eight times higher among individuals aged 85 and older (33.7%) than among those aged 65 to 69 (4.2%). The annual medical expense for persons with severe dementia is more than twice that of those with mild cognitive impairment (National Institute of Dementia, 2020a). In particular, it is critical to improve the awareness, prevention and management of dementia among high-risk groups, such as senior citizens aged 75 years and above, having low income, and living alone (Kim et al., 2016).
Due to the negative perception surrounding dementia, however, individuals are reluctant to undergo a screening assessment. Among older adults who were recommended a second screening test for dementia according to the results of the first screening test, only 40% of them took the second test (Yoo et al., 2018). In South Korea, the registration rate for dementia management systems for people with dementia aged 60 or above was only 44.6% in 2018. Moreover, approximately 40% of people with dementia do not receive appropriate treatment (National Institute of Dementia, 2020a). Despite recent increases in dementia awareness, it is reported that the attitude toward dementia remains poor (Rosato et al., 2019; Seo et al., 2015). Only half the people think that they can deal with dementia (Luck et al., 2012; Seo et al., 2015). The majority of participants in the study of Rosato et al. (2019) responded that people with dementia need to be under a high level of control. These results indicate that many people still have negative attitudes toward dementia.
Dementia is one of the most feared diseases among older people. According to a recent survey, 17.5% of 4,033 adult respondents were most afraid of developing Alzheimer’s disease and related dementias—the percentage was higher than that of cancer, stroke, and diabetes (National Institute of Dementia, 2015). Studies show that the fear of dementia is greater among the elderly than other age groups and among women than men (Cantegreil-Kallen & Pin, 2012; Ryu & Park, 2019; Tang et al., 2017). Nevertheless, previous studies report that about 70% to 90% of older adults have never participated in a dementia education program (Chang et al., 2020; Seoul Metropolitan Institute of Dementia, 2018).
Older adults also show a lack of knowledge of the disease, treatments, and management (Lee et al., 2016; Seo et al., 2015). Furthermore, the elderly have little knowledge of the risk factors related to dementia (Yang et al., 2015). Heger et al. (2019) reported that more than half the respondents in their study did not know that unhealthy lifestyle may result in dementia. In addition, compared with younger people, older adults show a relatively low level of dementia knowledge (Seo et al., 2015). In a previous study by Lee et al. (2016), only about 60% of the respondents aged 65 and over could respond correctly to questions about dementia. Preventing and delaying cognitive decline is emphasized because there is no cure for dementia.
The development and implementation of an effective education program for older adults living in communities are vital for lessening the fear of dementia, increasing dementia knowledge, improving attitudes toward the disorder, and promoting prevention behaviors against dementia (Lee et al., 2016; Lüdecke et al., 2016; Park et al., 2017; Roberts et al., 2014). Dementia prevention programs help relieve older adults’ depressive moods and enhance their quality of life (Sun et al., 2017). A multi-component integrated program including exercise, multimedia, and activities can be effective for the elderly because they prefer to engage in activities and listen to or watch audio-visual content rather than read written information (Parker et al., 2011). Some studies have reported that video-assisted education can enhance older adults’ confidence in dealing with specific diseases and stimulate their interest to adopt and modify their health-promoting behaviors (Du & Hu, 2016; Manor et al., 2013; Paragas & Barcelo, 2019; Wischer et al., 2018). Thus, it is important to examine the effects of a multi-component integrated dementia prevention program on the knowledge, attitudes, fears, and prevention behaviors regarding dementia among healthy older adults.
Methods
The study used a pretest-posttest design with nonequivalent control group, examining the effects of the 6-week multi-component integrated dementia prevention program among cognitively healthy older adults. The effects on knowledge, attitude, fear, and prevention behaviors concerning dementia were measured via survey questionnaires at the baseline as well as at the completion of the intervention.
Upon the approval from institutional review board, study participants were recruited from a senior citizen center in Seoul, Korea. The potential participants who regularly visited and spent the time at the center were initially contacted through center staff who included nurses or social workers. All participants met the following eligibility criteria: (a) 65 years and older in age; (b) no cognitive deficits with a score lower than eight on the Short-form Samsung Dementia Questionnaire (S-SDQ) (Choi et al., 1999); (c) no dementia prevention program taken in the past 6 months. Older adults with acute illnesses or major hearing or sight deficits were excluded.
Using G*Power 3 program (Faul et al., 2007). the sample size of this study was estimated based on the previous study of a dementia education program (Kang et al., 2013). A sample size per group needed for the effect size of 0.8 with a power of 80% and a significance level of .05 was 21. A total of 45 participants completed consent and participated in the study. Then, they were conveniently assigned to either experimental group or control group. For example, participants were assigned to control group if they were unable to participate in the intervention due to schedule conflicts. Three participants were disqualified because of incomplete questionnaire. In addition, two were excluded due to their poor attendance in the intervention. Finally, a total of 40 participants completed the study. Of the participants, 20 completed the intervention while those in the control group received usual care at the senior citizen center.
Intervention
A multi-component integrated intervention for dementia awareness and prevention was offered once a week for 6 weeks. The intervention sessions were held in a seminar room at the senior center, and each session lasted 60 minutes. The intervention included exercises, lectures and cognitively stimulating activities. The contents and materials constituting the intervention were chosen based on the literature review. They have been adapted and modified from the National Dementia Center’s resources (Shin et al., 2017).
Every session began with a 10-minute physical exercise accompanied by music favored by and familiar to the participants in the experimental group. Physical exercise was included to reduce physical inactivity—a high risk factor for dementia—and to educate the participants about the same (Alty et al., 2020).
Then, each session incorporated different contents. Session 1 and 6 had 40 minutes of lectures; through lectures, the participants were given knowledge about dementia, and they learned about the definition and types of dementia as well as the symptoms, risk factors, and healthy behaviors for preventing dementia.
Sessions 2, 3, 4, and 5 focused on 40 minutes of cognitively stimulating activities as part of promoting dementia prevention behaviors. The participants in the experimental group participated in the activities such as making Christmas ornaments using origami, learning a new language—English, watching video clips, and drawing. The activities have been shown to be an effective tool for cognitive stimulation and used as a non-pharmacological treatment older adults and people with dementia (Cepeda & Ruiz, 2019; Pike, 2013).
The participants had to memorize steps and use their hands and fingers to make origami figures. After watching a movie clip in which an elderly woman travels to the United States after studying English, they learned and practiced short phrases in English such as “Nice to meet you,” “Thank you,” “You are welcome,” and so on. Previous research shows that learning a new language has a positive effect on enhancing cognitive functions among older adults (Klimova, 2018).
The participants also watched other video clips from television documentaries about people who overcame their fear of dementia and were living positively to prevent dementia. The clips focused on reducing stigmatization and discrimination associated with dementia. After the participants watched the video clips, they were asked to express their feelings and perceptions regarding dementia by drawing pictures. Video clips were used as a means to improve their attitude toward dementia and reduce the fear of dementia through vicarious learning experience (Manz & Sims, 1981).
As a wrap-up, every session ended with a 10-minute discussion and Q&A. It provided them an opportunity to clarify what they had learned and ensure their accurate understanding of dementia via the Q&A session at the end of the intervention (Table 1).
Dementia Prevention Program—Weekly Topic and Program.

Instruments
Demographic data including age, gender, living status, marital status, job status, economic status, and level of education were collected. All the measures were used in this study after obtaining permission from the original author and the author who translated the measure.
The Dementia Knowledge Scale (Cho, 1999) was used to measure the knowledge of dementia. The scale includes 15 items related to causes of dementia (five items), system and resources (three items), symptoms of dementia (four items), and treatments and prevention of dementia (three items). Each correct answer received one point, whereas both a wrong answer and a “I don’t know” answer received no points. The total scores range from 0 to 15, with higher scores indicating a higher level of dementia knowledge.
The Attitude toward Dementia Scale (Cho, 1999) was utilized to measure the attitude toward dementia. The instrument includes nine items with a Likert scale from 1 to 5. The total scores range from 9 to 45. Higher scores indicate a more positive attitudes toward dementia.
The fear of dementia was assessed using the Korean version of the Fear of Alzheimer’s Disease Scale (K-FADS) which was originally developed by French et al. (2012). This scale is composed of three sections and includes a total of 30 items related to general fear of dementia (17 items), fear of physical symptoms (eight items), and tragic attitude toward dementia (five items). The reliability and validity of the Korean version has been reported in previous studies (Cho, 1999; Moon et al., 2014). Each item is scored 1 to 5 for a total scores range of 30 to 150. Higher scores mean lower levels of fear of dementia (French et al., 2012).
Dementia prevention behaviors refer to the actions taken in advance with the intention of preventing or delaying the onset and impact of dementia by an individual (Wittenberg et al., 2017; Yu, 2011). The measurement tool for dementia prevention behaviors (Lee et al., 2009) consisted of 12 items with a Likert scale from 1 to 3. While a total scores range is 12 to 36, higher scores indicate better performance in dementia prevention behaviors (Lee et al., 2009).
The Short form of the Samsung Dementia Questionnaire (S-SDQ) was used to assess the participants’ cognitive level for determining their eligibility to participate in the study. The 15-item instrument was developed by Choi et al. (1999). Each item uses a Likert-scale from 0 to 2. The total scores range is 0 to 30. Lower scores represent better cognitive levels. The reliability and validity of the instrument has previously been reported (Cho, 1999; Choi et al., 1999; French et al., 2012; Moon et al., 2014).
Data Analysis
Descriptive analysis included means, standard deviations, and percentages. In the homogeneity test, there was no significant difference between two groups in regard to the demographic characteristics of participants. In addition, based on the Shapiro–Wilk test, the outcome variables of fear of dementia, attitude toward dementia and dementia were normally distributed. The chi-squared test, independent t-test, or Mann–Whitney U test were used to compare the baseline scores between the groups. The differences in the scores from baseline to post-intervention were calculated. The Wilcoxon signed-ranked test and Mann–Whitney U test were utilized to compare the scores within and between experimental group and control group. The p value of .05 was used for statistical significance. The SPSS/WIN 23.0 software was used in all analyses.
Results
The mean age of the study participants was 76.93 years. Half the participants lived alone. None reported a high level of economic status. Their education ranged from no education to university education or above. The general characteristics of the participants were presented in Table 2.
General Characteristics of Participants of the Two Groups.
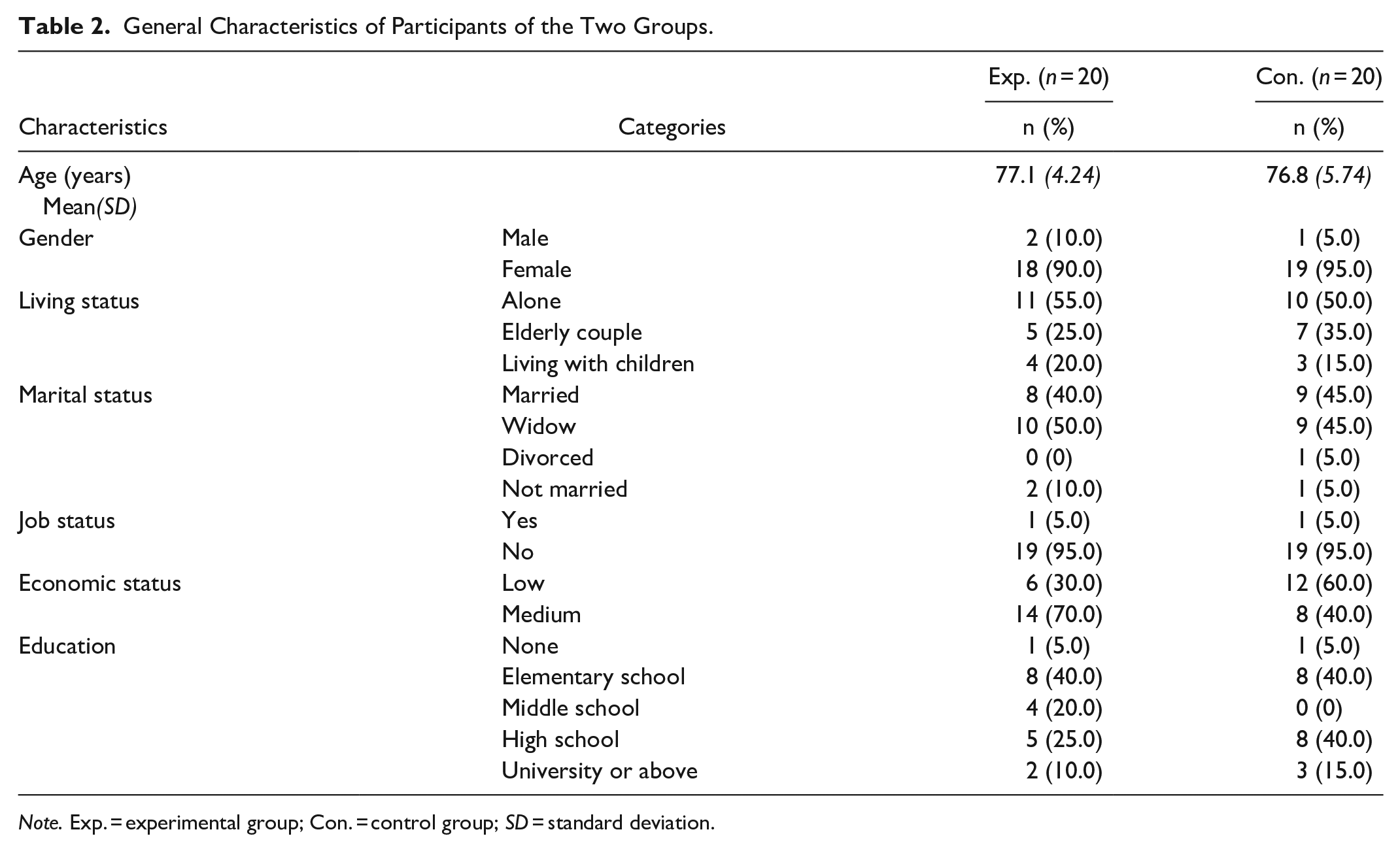
Note. Exp. = experimental group; Con. = control group; SD = standard deviation.
In regard to the changes in the scores of dementia knowledge from baseline to post-intervention, there was an increase from 9.05 to 10.70 in experimental group, whereas little change was in control group. However, the difference in the changes between the groups was not significant statistically (p = .103).
There was a decrease in the scores of the attitude toward dementia from baseline (20.65) to post-intervention (19.10) in experimental group. Yet, the attitude scores of baseline and post-intervention were nearly the same in control group. There was no statistically significant difference in the changes between the groups (p = .285).
As for the fear of dementia, a significant difference was found between the groups (p < .029). The K-FADS score in the experimental group was decreased from 103.85 at baseline to 93.75 after the intervention. However, the fear of dementia was rather increased in control group.
The dementia prevention behavior in experimental group was improved after the intervention while it remained nearly the same in control group. There was no statistically significant difference between the groups concerning the changes in the scores of dementia prevention behaviors before and after the intervention (p = .231). Table 3 presents the changes in the scores of outcome variables between two groups.
Differences in Outcome Variables Between the Two Groups.

Significance level: p < .05.
Discussion
This study was conducted to develop an integrated dementia awareness and prevention program to provide dementia preventive education and activities (i.e., physical exercise along with music, lectures, videos and movies, art and craft, and language learning) and to examine the program’s effects. The program was designed to not only reduce the fear of dementia but also improve dementia knowledge, attitude toward dementia, and dementia prevention behaviors.
In the process of developing an effective program for promoting dementia prevention behavior, this study tried to include the influencing factors identified in previous studies. Older adults often have limited knowledge of the causes and risk factors related to dementia and are in need of practical information about prevention behaviors (Rosenberg et al., 2020). In a survey with 1661 people aged from 51 to 70 years (Marcum et al., 2019), understanding dementia was revealed as a major component in preventing dementia. One-third respondents in the study reported they were not confident in how to decrease personal dementia risk. It was understood that to induce any desirable behavior, the provision of relevant information, that is, sufficient knowledge is an essential precedent. Despite the importance of dementia knowledge, knowledge does not always result into prevention behaviors (Yamane et al., 2021). Ajzen and Fishbein (1977) explained that attitude is an important variable that forms the intention to take a certain action and that it is a major variable that determines behavior along with knowledge. Family history and previous experiences of dementia affect not only one’s knowledge of and attitude toward dementia but also confidence in possibility of prevention (Rosenberg et al., 2020). Previous studies indicated that sufficient knowledge and positive attitude are necessary to reduce negative behaviors, suggesting that knowledge and attitudes influence behaviors (Wu et al., 2022). Fear, uncertainty and concerns over dementia is influenced by an individual’s knowledge, opinions and experiences of dementia. According to the previous study in older adults living in communities, there was a significant difference in the fear of dementia depending on whether they received education on dementia (Kim & Kim, 2020). It was also noted that the greater the fear of dementia, the poorer the performance concerning dementia prevention behavior (Kim & Kim, 2020). Thus, the integrated dementia awareness and prevention program for older adults in this study has included components pertaining to each factor.
Evidence shows that preventive behaviors in lifestyle such as physical exercises and cognitive activities may have protective effects and reduce risks of dementia (Heger et al., 2019). A previous systematic review indicated that integrated multi-component interventions are more effective than those with a single component (Bruderer-Hofstetter et al., 2018). In particular, the video-assisted the use of multimedia such as video clips in this study may have been effective in decreasing negative emotions such as fear toward dementia among the elderly. Recent research provides strong evidence that the use of media in health education is beneficial among older adults (Belchior, 2007; Haines et al., 2009). It is shown that the utilization of technological tools and multi-media are useful for older individuals, in increasing adherence and improving their engagement in the activities of interventions (Coley et al., 2019).
The findings of this study suggest that a 6-week integrated intervention can reduce the participants’ fear of dementia. However, the intervention in this study did not have any effect on dementia knowledge, attitude toward dementia, and dementia prevention behaviors. Similarly, no significant change in dementia knowledge and attitude toward dementia was found in a previous study of an integrative medicine program for dementia prevention in older adults at a public health center (Ahn & Hyun, 2019). Yet, although it was not significant, an improvement was found in the levels of dementia knowledge and prevention behavior after the older adults’ participation in the program. It may be necessary to tailor interventions in order to be effective based on the needs of older adults such as individuals with low health literacy or who live alone (Poppe et al., 2020). Mobile apps can also be used for increasing access to information and educational resources related to dementia without the restriction of time and place (Chelberg et al., 2021). In addition, it may be difficult to change knowledge, attitude, and prevention behaviors concerning dementia in the short term. Evidence shows a significant improvement when longer interventions are implemented (Je et al., 2019). Better results may be yielded when the frequency and duration of intervention is increased in a follow-up study.
The limitations of this study include convenience sampling. Randomized clinical trials and longitudinal studies with a large sample size are recommended to examine the effects of a dementia awareness and prevention intervention. In addition, the demographic and cultural characteristics of the participants may have influenced the results. It is necessary to examine the interventions in various samples in order to generalize the findings. Further investigation is also needed not only to gain a better insight into the relationships between knowledge, attitude, fear, and prevention behaviors but also design and implement effective interventions for older adults in community.
In summary, the prevention of dementia with early diagnosis is critical. This study may help increase the understanding about older adults’ fear of dementia which is a barrier and prevents from practicing dementia prevention behaviors. The fear of dementia needs to be further assessed while identifying particular causes and triggers. Based on the assessments, tailored interventions can be developed to effectively lessen the fear of dementia. Continuous multi-faceted interventions are critical to increase the level of awareness and prevention of dementia among older adults living in communities.
IRB protocol approval numbers:
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Research Resettlement Fund for the new faculty of Seoul National University.