
Abstract
Informal caregiving for dementia is common and often affects caregiver mental health. In addition to typical stressors faced by caregivers of persons with dementia (PWDs), rural caregivers often face additional stressors associated with living in more remote locations; unfortunately, this group is largely understudied. Ninety-three caregiver–PWD dyads completed measures of social support, perceived control, self-efficacy, burden, and cognitive functioning. Measures of PWD activities of daily living and mental functioning were also collected. These variables were hypothesized to predict caregiver self-reported symptoms of depression, anxiety, and stress. Contrary to predictions, only caregiving-related self-efficacy and caregiver burden predicted the caregiver’s mental health. Future interventions for improving rural caregiver self-reported mental health should target cognitions associated with caregiving self-efficacy and caregiver burden. Health care providers for rural families should focus on ways to reduce feelings of caregiver burden and provide caregivers with useful skills and tools for caregiving.
Almost 14% of individuals above 70 years have dementia (Plassman et al., 2007). Despite available formal caregiving options, many family members of people with dementia take on a more informal caregiving role. In 2004, more than 28 million family caregivers spent more than 30 billion hr caring for a family member with any condition, which could be roughly translated to more than US$300 billion market value (National Family Caregivers Association & Family Caregiver Alliance, 2006). Notably, 75% of care provided for individuals with Alzheimer’s disease alone is done so by informal caregivers (Schulz & Martire, 2004). In the present study, we focus on these informal caregivers of persons with dementia (PWDs), defined as caring for a family member or friend in an informal capacity (as opposed to a professional or paid capacity). Given the large number of informal caregivers, it is important to understand the associated mental health effects of caregiving.
There is a large amount of literature speaking to the physical and mental health effects of caregiving for family members with dementia. Evidence consistently shows that this role is associated with negative physical and mental health. Specifically, caregiving for individuals with dementia or Alzheimer’s disease is associated with anticipatory grief (Garand et al., 2012), clinical depression and anxiety (Schulz, O’Brien, Bookwala, & Fleissner, 1995), depressive disorders and symptoms (Kiecolt-Glaser, Dura, Speicher, Trask, & Glaser, 1991), and changes in processing speed (Caswell et al., 2003). Dementia caregiving is also associated with decreased immunity and more days sick with infectious diseases (Kiecolt-Glaser et al., 1991) and decreased health behaviors (e.g., less sleep; Connell, Janevic, & Gallant, 2001). Moreover, caregiving for individuals with dementia (vs. no dementia) is associated with increased physical and mental health difficulties, familial conflict, and caregiver strain (Ory, Hoffman, Yee, Tennstedt, & Schulz, 1999).
Despite the abundance of research on caregivers of PWDs, relatively little attention has been paid to caregivers in rural settings. In addition to the mental and physical effects, rural caregivers face additional challenges in caring for an individual with dementia or Alzheimer’s disease. Notably, rural caregivers indicate that their family member faces unmet service needs (Li, Kyrouac, McManus, Cranston, & Hughes, 2012) and limited availability and accessibility of services (O’Reilly & Strong, 1997b). In addition, they face potential stigma associated with dementia and fear the lack of privacy in a small community (Morgan, Semchuk, Stewart, & D’Arcy, 2002). In one report, researchers note that rural caregivers provide almost 50 hr of care a week (Kosberg, Kaufman, Burgio, Leeper, & Sun, 2007). Interestingly, gender differences appear in comparisons of urban and rural caregivers; male caregivers in rural environments exhibit poorer mental health as compared with their urban-dwelling counterparts; however, no differences emerge between female caregivers in the two locations (Tommis et al., 2007). Home care staff note that rural caregivers may be reluctant to use services in the area and may not request help until a crisis situation emerges (Morgan et al., 2002). Despite the drawbacks of being a caregiver of a PWD in a rural setting, rural caregivers do express somewhat high levels of social support (Kaufman, Kosberg, Leeper, & Tang, 2010). Social support in rural areas, despite its potential negative consequences (e.g., community members misunderstanding the dementia condition and criticizing the caregiver’s care decisions), does provide benefits, such as access to informal networks and less social isolation (O’Reilly & Strong, 1997a).
Much of the research on caregivers in rural settings is qualitative, which is a necessary first step to understanding the problems faced by this population. However, more work is necessary to more fully understand the relationship among demographic variables, reported caregiver burden and social support, patient’s dementia, and caregiver mental health, as previous research suggests that rural and urban caregiving is qualitatively different. In the present descriptive study, we will examine predictors of caregiver mental health (self-reported anxiety, stress, and depression) in a sample of rural dementia caregivers. This next step affords service providers more information about potential points of intervention for this group of individuals.
To our knowledge, this is the first examination of mental health predictors in rural dementia caregivers. In the present study, cognitive functioning, social support, caregiver burden, perceived control over one’s life, self-efficacy in caregiving, and demographic variables (i.e., age and gender), in addition to the care-recipient’s level of dementia and ability to complete activities of daily living (ADLs), will be explored as possible predictors of self-reported caregiver mental health.
Research supports the hypothesis that many of these factors will predict dementia caregivers’ mental health symptoms. Greater social support is related to lower levels of depression (Lopez, Romero-Moreno, Márquez-González, & Losada, 2012; Williams, 2005), and a caregiver’s burden is negatively related to his or her mental health (Garand, Dew, Eazor, DeKosky, & Reynolds Iii, 2005; García-Alberca et al., 2012). Demographic variables are also related to caregiver mental health, including age (Covinsky et al., 2003; Neundorfer, 1991; Sparks, Farran, Donner, & Keane-Hagerty, 1998) and gender (Covinsky et al., 2003; Mahoney, Regan, Katona, & Livingston, 2005). Moreover, across elderly caregiving studies (i.e., not restricted to dementia caregiving), spouses report greater depressive symptoms than do caregiving children (Pinquart & Sörensen, 2011). The PWD’s ability to perform ADLs also predicts caregiver anxiety (Mahoney et al., 2005), as well as the PWD’s level of dementia (Sparks et al., 1998). Self-efficacy, an individual’s belief that he or she has control over the events in his or her life, is related to how much stress one believes he or she can handle and has to do with how he or she encounters challenges (Bandura, 2000). Conceptually similar, caregiver self-efficacy is a caregiver’s self-report of his or her ability to engage individuals with dementia in meaningful activities, respond to the individual’s needs, and deal with caregiving difficulties. Increased caregiving self-efficacy is associated with lower levels of depression (Gilliam & Steffen, 2006) and mediates the relationship between care-recipient behavioral problems and caregiver depression (Sherwood et al., 2007). A greater sense of caregiving-specific self-efficacy may also be related to lower levels of depression, anxiety, and anger (Steffen, McKibbin, Zeiss, Gallagher-Thompson, & Bandura, 2002). Although the cited research is by no means exhaustive, it does support the hypothesis that there is a relationship between a caregiver’s social support, burden, self-efficacy, and demographic characteristics and his or her mental health. However, previous research has largely neglected caregivers in rural settings.
To our knowledge, this is the first exploration of whether processing speed predicts mental health in caregivers. Although previous research suggests that individuals’ chronic stressors (such as chronic health conditions) predict changes in cognition (for review, see Marin et al., 2011) and that caregiving status predicts cognitive functioning (although this effect disappears when distress is entered into the regression; Caswell et al., 2003), we will include caregiver processing speed as a predictor of mental health.
Hypotheses
Better rural caregiver mental health (fewer self-reported symptoms of stress, depression, and anxiety) will be predicted by greater levels of caregiver social support, perceived control, and self-efficacy; lower levels of caregiver burden; and better cognitive functioning. Moreover, demographic variables, such as being female and younger age, will be related to better caregiver mental health. Finally, lower levels of dementia and greater ability to perform ADLs in/by the care-recipient will be associated with better caregiver mental health.
Method 1
Participants
Individuals interested in receiving an intervention for caregiver burden responded to local media advertisements or learned about the intervention from community resources (e.g., local Alzheimer’s Association chapter). Each of the 93 participating families consisted of one primary caregiver (defined by the participating family) and one PWD (this is loosely defined, as not all PWDs had received a formal diagnosis). Seventy-five percent of the families reported receiving a diagnosis of dementia (see Table 1 for the dementia breakdown). Families lived in rural areas of central Virginia.
Characteristics of Participants.

Note. MMSE = Mini Mental Status Examination.
For education, 12 years is equivalent to a high school degree.
No participants reported being Hawaiian or Other Pacific Islander, Asian or Asian American, Arabic/Middle Eastern or Native American or Alaska Native.
Measures
Measures completed by the caregiver
Demographic questionnaire
In addition to typical demographic information, the questionnaire included items regarding the relationship between the caregiver and PWD, the number of years the caregiver has been caregiving for this family member, and whether or not there is a professional caregiver present, as well. Five families did not report demographic information (see Table 1 for participant characteristics).
Depression Anxiety and Stress Scale–21-item version (DASS-21)
This measure assesses self-reported depression, anxiety, and stress symptoms over the past 7 days. Scores on the full scale range from 0 to 126 (scored according to questionnaire guidelines), and scores on the individual scales range from 0 to 42; higher scores reflect higher endorsement of symptoms. Note that this questionnaire measures the physiological symptoms of anxiety (e.g., “I felt I was close to panic”), symptoms of stress (e.g., “I tended to overreact to situations”), and depressive symptoms (e.g., “I felt that I had nothing to look forward to”). Psychometric properties for the DASS-21 (Lovibond & Lovibond, 1995) in a sample of older adults seeking treatment for worry in a primary health care setting suggest adequate internal consistency and correlates with widely used measures for similar constructs (Gloster et al., 2008). In the current sample, the full scale exhibits high internal consistency, Cronbach’s α = .93.
Multidimensional Scale of Perceived Social Support
This 12-item questionnaire (Zimet, Dahlem, Zimet, & Farley, 1988) contains questions regarding the participant’s perceived social support from three domains: significant other, family, and friends. Individuals rate the degree to which they agree or disagree with statements about how supported he or she feels by others. Scores range from 1 to 7 (mean of item responses); higher scores reflect greater social support in each of the domains. Cronbach’s α = .93 in the current sample.
Zarit Burden Index–22-item version (ZBI)
This 22-item (Zarit, Reever, & Bach-Peterson, 1980) questionnaire contains questions regarding a caregiver’s feeling of burden related to caregiving. Scores range from 0 to 88 (sum of item responses). Higher scores reflect greater feelings of burden; little or no burden is reflected by scores of 0 to 21, mild to moderate burden by scores of 21 to 40, moderate to severe burden by scores of 41 to 60, and severe burden by scores of 61 to 88. Cronbach’s α = .91 in the current sample.
Perceived control
This 12-item (Lachman & Weaver, 1998) questionnaire consists of questions regarding an individual’s sense of perceived control over his or her life. Personal Mastery (e.g., “I can do just about anything I really set my mind to”) and Perceived Constraint (e.g., “I often feel helpless in dealing with the problems of life”) subscales are used to create a perceived control score with higher scores reflecting a greater sense of perceived control overall and a higher standing in each subscale. Possible scores range from 1 to 7 (mean of item responses). In the current sample, Cronbach’s α = .79.
Caregiver Self-Efficacy Tool–20-item version
This 20-item questionnaire (Braddock, 2008; modified for the current study) consists of questions from the original 34-item questionnaire. This assesses the caregiver’s efficacy and self-efficacy in how he or she is able to work with the PWD on activities provided by the intervention (e.g., “At this time, I am confident that I am able to understand my family member’s interests and hobbies”). Scores can range from 20 to 100 (sum of item responses); higher scores reflect self-efficacy with respect to caregiving in the caregiver. Cronbach’s α = .94 in the current sample.
Digit Symbol-Coding subtest of the Wechsler Adult Intelligence Scale–III (WAIS-III). 2
The Digit Symbol-Coding subtest (Wechsler, 1997) measures cognitive processing speed by asking participants to copy symbols of corresponding numbers into boxes as quickly as possible in 2 min. Possible scores can range from 0 to 133 (sum of correct symbols).
Alzheimer’s Disease Cooperative Study (ADCS)—ADL Inventory–Severe Impairment Version (ADCS-ADL-SIV)
This 19-item interview (Galasko et al., 1997) includes questions for the caregiver of the PWD concerning the PWD’s abilities to perform ADLs over the past 4 weeks. Caregivers are asked to describe the actions of the PWD observed in domains such as eating functions, personal care functions, and his or her ability to use items around the home. Using a structured interview, scores of 0 to 54 (sum of item responses) were obtained with higher scores reflecting greater ability to perform ADLs. This interview has adequate test–retest reliability (with a significant correlation of .93 from baseline to 1-month follow-up; Galasko et al., 2005). Note that this form was used with permission from the National Institute on Aging (NIA) Alzheimer’s Disease Cooperative Study (NIA Grant AG10483).
Measure completed by the caregiver and PWD
Mini Mental Status Examination (MMSE)
In this brief dementia screener, individuals are asked a series of questions regarding orientation (e.g., date and location), short-term memory, and working memory. Scores on the MMSE (Folstein, Folstein, & McHugh, 1975) range from 0 to 30 with higher scores reflecting greater cognitive functioning. Although both age and education can affect mean scores on the MMSE (Crum, Anthony, Bassett, & Folstein, 1993), in the present intervention, a score of 30 reflects no dementia, scores 26 to 29 reflect questionable dementia, scores of 21 to 25 reflect mild dementia, scores of 11 to 20 reflect moderate dementia, and scores of 0 to 10 reflect severe dementia (Perneczky et al., 2006). In line with Crum et al.’s (1993) scoring guidelines, both the serial sevens question (subtracting seven from 100 and so on) and spelling WORLD backward were administered, and the set that yielded the higher score was used for scoring.
Procedure
Consent procedure
To ensure that all individuals comprehended the purpose of the intervention research study, as the first step in the consent procedure, the researcher (a) informed the caregiver and PWD of the goals of the study, (b) assessed whether or not the PWD understood the purpose and goals of the study, and (c) determined which consent forms were necessary for each family. If the PWD comprehended the purpose and goals, the researcher administered an informed assent agreement to the PWD and a “guardian informed consent” agreement to the caregiver so that he or she could sign for the PWD. The caregiver was asked to sign a caregiver informed consent agreement. It should be noted that some of the PWDs were unable to sign the assent form. In this case of last resort, the PWD could provide oral assent to participate, and both the caregiver and the home visitor would sign and date the assent form. The home visitor was also asked to provide a detailed rationale for not obtaining written assent.
Questionnaire administration
All families participated in their homes; both the PWD and caregiver were present. Following informed consent, caregivers completed the demographic, DASS-21, social support, ZBI, perceived control, and caregiver self-efficacy questionnaires independently. Researchers administered the digit symbol questionnaire, ADL, and MMSE according to established measure guidelines. Note that during oral administration (ADL and MMSE), the caregiver and PWD were separated when possible to ensure measurement validity (i.e., so one would not overhear the other’s answers).
Results
Analytic Plan
To assess the predictors of caregiver mental health (as assessed by the DASS-21), a hierarchical linear regression was conducted. Prior to running the regression analysis, assumptions were checked. Notably, caregiver age and caregiver mental health were not normally distributed; these variables were transformed using a square root transformation and were normally distributed following the transformation. All other assumptions (multivariate normality, linearity, normally distributed errors) were checked and met (see Table 2 for descriptive information for the measures before transformation).
Descriptive Information for Measures.
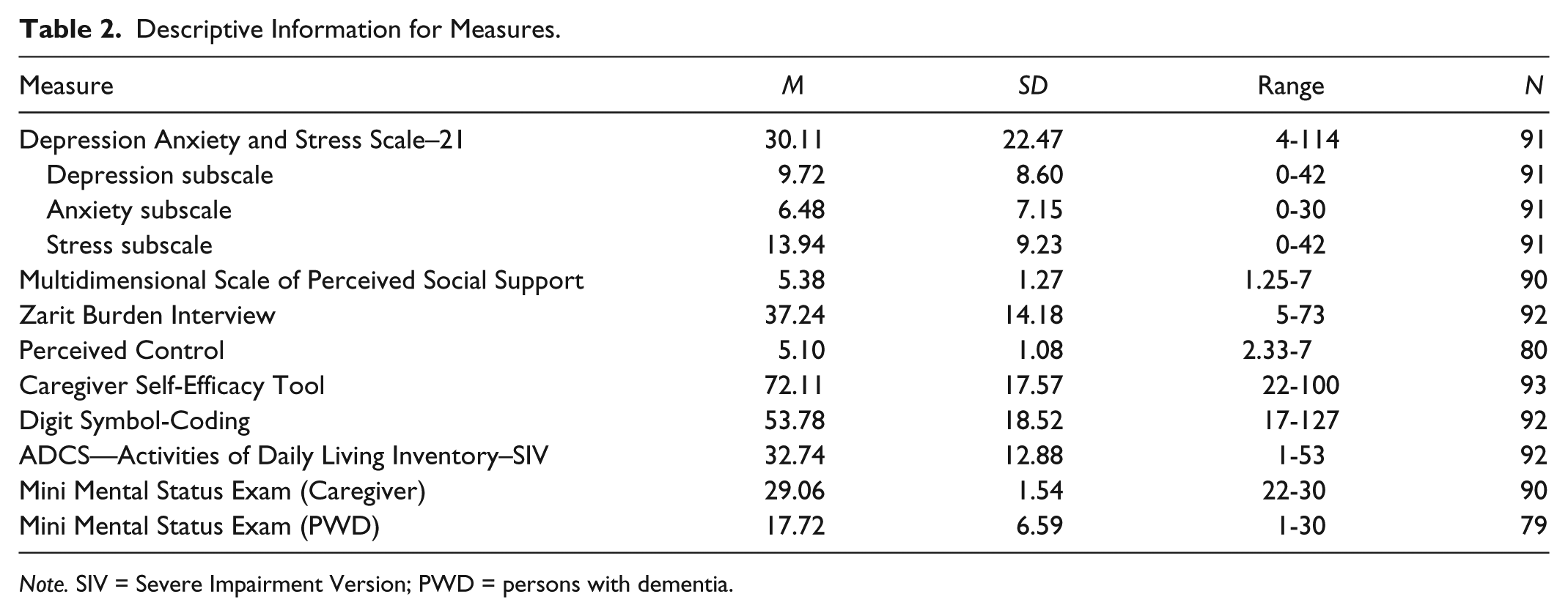
Note. SIV = Severe Impairment Version; PWD = persons with dementia.
Predicting Caregiver Mental Health
To assess how well caregiver social support, perceived control, caregiving self-efficacy, caregiver burden, and PWD’s cognitive functioning (on the MMSE) and ADL predict caregiver mental health, when controlling for the caregiver’s age and gender, a hierarchical linear regression was computed. When age and gender were entered, they did not significantly predict caregiver mental health, F(2, 57) = .51, p = .605, R2 = .02. However, when caregiver social support, perceived control, caregiving self-efficacy, caregiver burden, and PWD’s cognitive functioning and ADL were entered into the model, they significantly improved the prediction, ΔR2 = .55, ΔF(6, 51) = 10.62, p < .001. All variables entered together significantly predicted caregiver mental health, F(8, 51) = 8.22, p < .001. Together, these variables accounted for 56.3% of the variance in caregiver mental health.
Contrary to predictions, only caregiver self-efficacy, β = −.38, t(51) = −3.35, p = .001, and caregiver burden, β = .44, t(51) = 3.83, p < .001, were significant predictors of caregiver mental health. Caregiver age, t(51) = −0.82, p = .419, gender, t(51) = 0.22, p = .823, social support, t(51) = −1.74, p = .089, perceived control, t(51) = −0.33, p = .746, the PWD’s cognitive functioning, t(51) = −1.52, p = .135, and the PWD’s ADL, t(51) = 1.35, p = .184, did not significantly predict the caregiver’s mental health.
Taken together, the results suggest that greater caregiver self-efficacy in caregiving ability is related to better (i.e., lower scores) caregiver mental health. Moreover, better caregiver mental health is related to less caregiver burden. Surprisingly, caregiver age, gender, social support, perceived control, and the PWD’s cognitive functioning and ADL did not significantly predict the caregiver’s mental health.
Follow-up analyses
Following the results of the multiple linear regression, exploratory correlational analyses were conducted to examine the relationship among caregiver self-efficacy, caregiver burden, and mental health domains (see Table 3 for correlation coefficients). Results suggest that caregiver self-efficacy is negatively correlated with caregiver depression, anxiety, and stress, such that as the caregiver’s self-efficacy in caregiving increases, depression, anxiety, and stress decrease. Moreover, caregiver burden is positively correlated with caregiver depression, anxiety, and stress, such that increasing feelings of burden are associated with greater reported depression, anxiety, and stress symptoms. Overall, caregiver burden is more strongly correlated with mental health variables than caregiver self-efficacy.
Correlations Among Mental Health Variables, Caregiver Burden, and Caregiver Self-Efficacy.

Note. DASS = Depression Anxiety and Stress Scale.
p < .01. **p < .001.
In addition, a post hoc power analysis was conducted using G*Power software (Faul, Erdfelder, Lang, & Buchner, 2007). Our sample (93 participants) was adequately powered at .95 (α = .05) for a two-tailed t test, and medium effect size, for eight predictors in a multiple linear regression.
Discussion
To our knowledge, this is the first assessment of multiple predictors on the mental health of caregivers of PWDs in a rural setting. Contrary to predictions, caregiver age, gender, social support, perceived control, and the PWD’s cognitive functioning and ADL did not significantly predict the caregiver’s current mental health (as assessed on a self-report depression, anxiety, and stress symptom measure). Consistent with predictions, however, caregiver self-efficacy and burden did predict caregiver mental health. Exploratory analyses revealed medium-sized correlations between caregiver self-efficacy and depression, anxiety, and stress. Moderately large correlations emerged between caregiver burden and the components of mental health. Taken together, these results suggest the importance of rural caregiver’s experienced burden and feelings of self-efficacy while caregiving for a loved one with dementia.
The present study failed to support previous dementia caregiving findings with regard to the relationships between mental health and social support (Lopez et al., 2012; Williams, 2005), age (Covinsky et al., 2003; Neundorfer, 1991; Sparks et al., 1998), gender (Covinsky et al., 2003; Mahoney et al., 2005), and relationship (Pinquart & Sörensen, 2011). Previous research has also found support for a relationship between caregiver mental health and the PWD’s reported ADL (Mahoney et al., 2005) and level of dementia (Sparks et al., 1998). In the present sample of rural caregivers, these factors do not appear to play a significant role in predicting their overall mental health when caregiving.
Prior work—replicated in the present study—has found that the burden of caregivers of Alzheimer’s disease patients (García-Alberca et al., 2012) and individuals with mild cognitive impairment (Garand et al., 2005) is related to caregiver mental health. This suggests that the relationship between mental health and burden is fairly robust, even across mild and more severe forms of dementia caregiving. Caregiver quality of life is also strongly tied to reported levels of caregiver burden (Heggie et al., 2011). Burden has also been found to mediate the relationship between a patient’s disturbing behavior and a lack of caregiver social support on depression in dementia caregivers (Clyburn, Stones, Hadjistavropoulos, & Tuokko, 2000). These relatively robust findings across studies make it clear that caregiver burden is one area that could be targeted by interventions to greatly improve caregiver’s mental health. Caregiver self-efficacy was also found to predict mental health in our rural dementia caregivers. This result also is in line with prior work in this area; self-efficacy is associated with lower levels of depression (Gilliam & Steffen, 2006; Romero-Moreno, Márquez-González, Mausbach, & Losada, 2012) and mediates the relationship between patient behavioral problems and caregiver depression (Sherwood et al., 2007). Importantly, researchers have found that the combination of self-efficacy and spirituality in caregivers is associated with better mental health (Lopez et al., 2012).
Individuals with greater self-efficacy are hypothesized to be able to take on challenges, rather than avoid them, and are less vulnerable to anxiety and depression (Bandura, 2000). To measure caregiving self-efficacy in the current study, caregivers were asked about their confidence in engaging the PWD in activities around the home, coping with added responsibilities around the home as a caregiver, and effectively responding to the frustration associated with caregiving. Caregivers’ greater feelings of caregiving self-efficacy were associated with better mental health (i.e., fewer self-reported symptoms of anxiety, depression, and stress). It is perhaps the case that self-efficacy provides a certain resiliency in caregivers of individuals with dementia. What is surprising, however, is that perceived control (a concept very similar to self-efficacy) did not significantly predict caregiver mental health. The caregivers may not have understood this measure, as it was the measure most commonly left incomplete in the packets. Thus, the questions may not have been a valid measure of perceived control in this sample. What is likely, though, is that there is something unique about self-efficacy specific to caregiving skills—and not more general feelings of control in one’s life—that is related to mental health in this sample of rural caregivers.
Limitations
There were a number of limitations in the current study that should be noted. First, participating families all responded to local advertisements for a caregiver intervention by a local Alzheimer’s disease group. All families had to be willing to allow researchers to come into the home across a few months to administer measures and interact with the caregiver and PWD. Thus, the present sample may not be representative of every rural family with an individual with dementia. Second, religion and spirituality were not assessed in the current study; thus, a potentially important aspect of coping or support was not included in our model. Caregivers of PWDs have reported that religious coping is helpful when coping with caregiving (Stolley, Buckwalter, & Koenig, 1999). Research on religious coping in rural caregivers has primarily focused on ethnic and racial differences. Results suggest that African Americans endorse greater religious coping than Caucasian individuals (from cities: Haley et al., 2004; and rural areas: Kosberg et al., 2007). Despite our sample being largely Caucasian, religion and religious coping may play a role in caregiver’s understanding of the caregiving role, and thus may have affected the present results.
Importantly, results from the present analyses should be interpreted in light of the fact that the self-efficacy measure has yet to be rigorously tested or validated. Although previous work has utilized the longer form of the measure (Braddock, 2008), the measure was shortened for the present study and has not been validated in either form. Despite this, the measure demonstrated excellent internal consistency in the present sample and was found to significantly predict caregiver mental health. In addition, participating caregivers seem to have found the measure approachable, as they all completed it. However, future work must test the reliability and validity of the measure, especially in larger samples.
Future Directions and Conclusions
The present study was the first to our knowledge to examine caregiver age, gender, perceived social support, perceived control, burden, caregiver self-efficacy, and the PWD’s cognitive functioning and ADL as predictors of rural caregivers’ mental health. Contrary to predictions, only caregiver burden and caregiver-related self-efficacy were significant predictors of symptoms of depression, anxiety, and stress. Importantly, these two predictors accounted for more than half of the variance in caregiver mental health, suggesting the relative importance of these two components on mental health. Future research should investigate interventions targeting caregiver-specific burden and self-efficacy, seeking to reduce the perceived burden by rural caregivers and increase the relative control that caregivers have over their situation. Specifically, interventions could teach caregivers how to cope with increased responsibilities around the home, dealing with difficult PWD behavior, and how to effectively engage the PWD in meaningful activities around the home. Given the results of the present study, interventions that successfully target these areas may reduce mental health problems in rural caregivers, who deal with unique issues when it comes to caregiving.
In addition to the difficulty of caregiving for an individual with dementia or Alzheimer’s disease, rural caregivers must effectively cope with the added stressors of rural caregiving. Largely forgotten by targeted interventions, rural caregivers face the added challenges of lack of privacy and increased stigma in small communities (Morgan et al., 2002) and limited availabilities of services (O’Reilly & Strong, 1997b). The present findings are somewhat positive in that two factors that can be targeted by interventions, namely, caregiver burden and self-efficacy, were shown to be predictive of caregiver mental health. Many variables that would be impossible to target in interventions, such as caregiver age and gender, did not significantly predict mental health. Moreover, it may be possible to target burden and self-efficacy via telephone or Internet, which would overcome some of the difficulties associated with rural caregiving.
Informal rural caregivers, often with little or no choice due to limited resources, have made a difficult decision to care for a loved one with dementia or Alzheimer’s disease. Moreover, these individuals have the added difficulties associated with caregiving in rural areas. In the present study, reduced caregiver burden and increased caregiving-related self-efficacy are related to decreased caregiver mental health (i.e., self-reported symptoms of depression, anxiety, and stress). These results are promising in that they provide a potential next step in creating targeted interventions for reducing caregiver mental health issues.
Footnotes
Acknowledgements
The authors thank the home visitors who made data collection throughout this study possible: Nancy Soule, Valerie Diamond, and Larry Stillwell. Finally, they thank the research assistants in the Dodson Cognition Lab at the University of Virginia for their assistance with data entry.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was supported by the Virginia Department for Aging and Rehabilitative Services [90AI0046 to the Alzheimer’s Association, Central and Western Virginia Chapter for the CONNECTIONS intervention].