
Abstract
Some state health departments in the United States are in the process of increasing access to immediate postpartum long-acting reversible contraception (LARC), an evidence based approach to preventing unintended pregnancy. Changing state Medicaid policies for immediate postpartum LARC reimbursement has proven insufficient for overcoming access barriers, so states developed implementation strategies to conduct multiple, coordinated systems changes. This research was conducted to understand the roles of social networks in implementing a complex health systems change. In 2015 and 2018, semi-structured telephone interviews were conducted with state teams engaged in increasing access to immediate postpartum LARC. Transcriptions of interviews were coded based on the Consolidated Framework for Implementation Research and implementation strategies, then themes were refined through discussion. A web-based assessment in 2018 evaluated degree of implementation accomplishment. Teams found that increased formal or informal social engagement among members aided timeliness, resource coordination, accountability, and enthusiasm, and over the course of 2 years, reduced disruptions due to staff turnover. The composition of the team influenced the social ties it could draw upon. Preexisting relationships were the most common source of social networking. Bridging social ties connected state teams to novel information and instrumental aid used to seek funding, conduct consumer awareness activities, and train healthcare providers. Cultivating and maintaining relationships among agencies and organizations as part of routine operations enables them to be available for future implementation efforts. Multi-agency teams may benefit from prioritizing time for internal and external relationship-building to enhance implementation progress.
Keywords
Background
Learning communities are an increasingly used strategy to bring multiple groups together in order to share knowledge and increase the speed and effectiveness of public health implementation efforts (Okoroh et al., 2018). During implementation, growing and maintaining high-quality working relationships and social networks is vital to the sharing of information, collaborating to solve problems, and identifying potential allies and collaborators (Powell et al., 2015). Organizations networked with other organizations are more likely to acquire new knowledge (Tortoriello et al., 2012) and implement new practices faster (Damschroder et al., 2009). Within organizations, relationships between individuals contribute to effective implementation via clearer communication and social support (Damschroder et al., 2009). In turn, social support involves sharing skills, information, different perspectives, and tangible aid with each other, all of which can assist implementation progress (Heaney & Israel, 2008). Social support can potentially provide emotional support as well, which may buffer work stresses, promote work-related motivation and engagement, and discourage potentially disruptive employee turnover (Pomaki et al., 2010). While many implementation science frameworks and planning models suggest promoting social networking and strengthening relationships among stakeholders and between partnering agencies can aid implementation success (Foster-Fishman et al., 2001; Johnson et al., 2004; Powell et al., 2015), there is a paucity of research identifying the specific aspects of learning communities that support these social connections. There is also a need for in-depth research into how learning community members perceive and the extent to which they welcome relational capacity building efforts (Foster-Fishman et al., 2001). Further, research on whether social networks affect implementation progress or sustainability remains limited (Brown et al., 2012; Bunger et al., 2016; Palinkas et al., 2011).
In 2014, the Association of State and Territorial Health Officials (ASTHO), in partnership with the Centers for Disease Control and Prevention (CDC) and other federal and national agencies, launched the Immediate Postpartum Long-Acting Reversible Contraception (LARC) Learning Community (referred to hereafter as the Learning Community) to assist state health agencies with immediate postpartum LARC policy implementation (Kroelinger et al., 2015). Access to LARC immediately postpartum may prevent rapid repeat and unintended pregnancy (American College of Obstetricians and Gynecologists [ACOG], 2014) and is convenient for patients and their providers (Rodriguez et al., 2014). However, cost is a significant barrier to immediate postpartum LARC uptake (Moniz et al., 2015). Some insurers pay a single (“global”) fee for all labor-and-delivery care, which is not sufficient to cover LARC devices and insertion fees (Moniz et al., 2015). To overcome this barrier for those using public health insurance, states have changed Medicaid reimbursement policy to reimburse costs for immediate postpartum LARC (ACOG, 2018). The experiences of early-adopting states demonstrated that policy change alone was insufficient to improve widespread access to immediate postpartum LARC (Rodriguez et al., 2014) and that additional coordinated efforts were needed in areas such as provider training, device stocking, and consumer awareness, among others (Rankin et al., 2016), to facilitate implementation (Okoroh et al., 2018). Each state in the Learning Community created an implementation team consisting of representatives of state leadership, Medicaid medical directors, directors of maternal and child health or family planning programs, hospital administrators, and clinical providers. Therefore by design, state teams were multi-disciplinary and multi-agency.
The Learning Community took place between 2014 and 2018, and each year additional US jurisdictions joined. Assessments of implementation successes, challenges, and strategies used to increase access to contraception were conducted in 2015/2016 and 2018. This study uses data from the 13 states that participated in the Learning Community during the two assessment periods (2015/2016 and 2018) in order to identify factors that encourage social networking in a multi-agency collaboration. This research was also undertaken to report whether social networks within and external to organizations involved in the Learning Community affected their capacity to implement strategies to increase access to immediate postpartum LARC.
Methods
All states in the Learning Community were assessed at two time points.
Round 1: 2015/2016
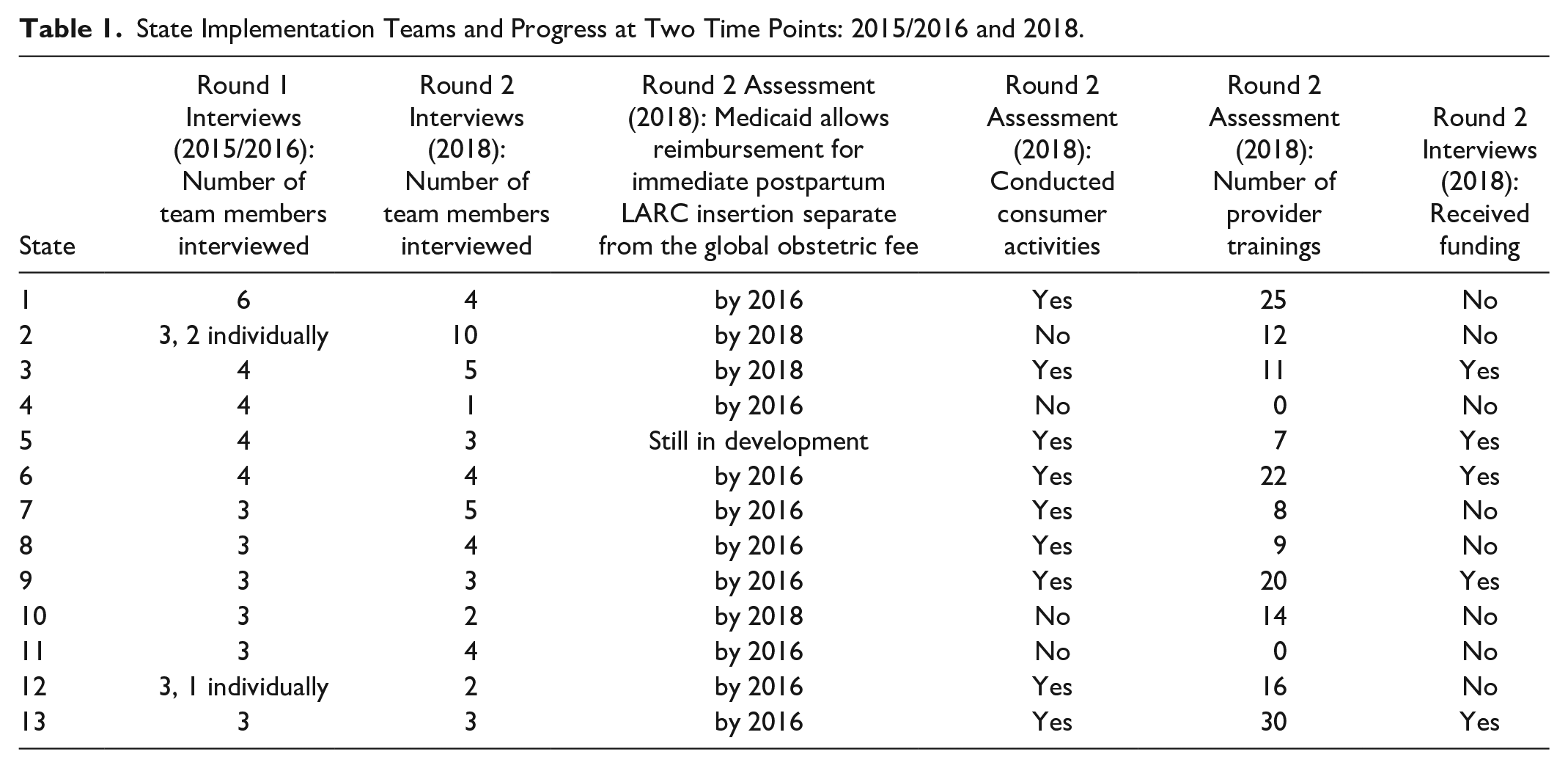
Semi-structured telephone interviews covering efforts to expand access to immediate postpartum LARC were conducted with members of all 13 state teams participating in the Learning Community (Figure 1) between November 2015 and March 2016 (Figure 2). Every team included at least one state health department staff member, plus state health officials, payer representatives (e.g., Medicaid), clinical providers, or other stakeholders. Team members were interviewed together when possible; between 3 and 6 team members joined each call (Table 1). In three cases, team members unavailable for the scheduled call were interviewed separately. In all, 16 1-hour interviews were conducted with 41 participants. The interviews are described in further detail in other publications (DeSisto et al., 2017, 2019; Kroelinger et al., 2019). The Consolidated Framework for Implementation Research (CFIR) was used as a framework for the interview guide and the initial coding scheme (Damschroder et al., 2009). CFIR synthesizes the concepts of several implementation science models into a single framework of factors influencing implementation, making it a useful framework for evaluating public health initiatives (Damschroder et al., 2009). The five major domains of CFIR are intervention characteristics, inner and outer settings, individuals involved, and implementation process. For this analysis, the inner setting was defined as the structural, political, and cultural climate of a state team, and the outer setting was defined as the economic, political, and social context in which the state team was operating. The initial coding scheme for the Round 1 interviews included the 39 constructs within the five CFIR domains, plus codes for “implementation strategy,” and whether something was identified as a facilitator or barrier to implementation progress. The construct “social networking” emerged as a theme, and was sub-coded by the type of supportive function: emotional (provision of empathy, trust, or caring), instrumental (tangible aid or services), informational (advice, suggestions, or information), and appraisal (constructive feedback and affirmation) (Heaney & Israel, 2008).
State Implementation Teams and Progress at Two Time Points: 2015/2016 and 2018.

Locations participating in the ASTHO Immediate Postpartum LARC Learning Community in the United States.
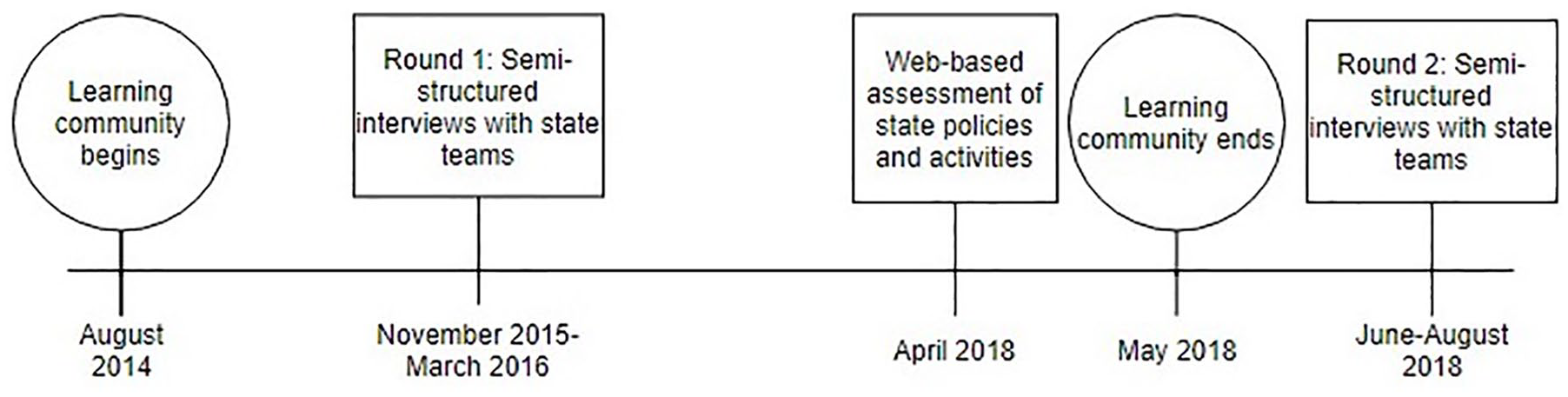
Learning community implementation and assessment timeline.
Round 2: 2018
In April 2018, all state teams participated in a web-based, quantitative assessment in REDCap electronic data capture tools (Harris et al., 2009, 2019) hosted by University of Illinois at Chicago that included questions about implementation strategies and activities and Medicaid policies (Figure 2). From the start of the Learning Community, nine “focus areas” were used to classify the strategies states identified as needed to increase access to contraception: increasing healthcare provider awareness and training; securing adequate funding for contraception policies and programs; addressing administrative, stocking, and other logistical barriers to accessing the full range of contraceptive methods; conducting consumer awareness; establishing partnerships across agencies, payers, and other stakeholder organizations; delivering comprehensive services to a range of service locations; conducting quality assurance and evaluating access to contraception; and addressing persistent access challenges and barriers to specific populations (Association of State and Territorial Health Officials [ASTHO], 2017; DeSisto et al., 2019). Teams created their own implementation action plans that included strategies from at least one of these focus areas, and the assessment was organized around those focus areas. States used a broad range of strategies to increase access to contraception, but most states included activities based in the focus areas of healthcare provider awareness and training; reimbursement and financial sustainability; and consumer awareness (DeSisto et al., 2021). Therefore, measurements of efforts in those three focus areas were used to gauge implementation progress after 2 years between states. To measure healthcare provider awareness and training, the number of healthcare provider trainings regarding contraception conducted from 2016 to 2018 were counted and categorized. The focus area of reimbursement and financial sustainability was measured by whether there were state Medicaid policies to reimburse for immediate postpartum LARC insertion separate from the global obstetric fee. States were considered to have conducted “consumer-related activities” if they reported that they either “reached out to consumers of reproductive age to obtain their perspectives on or experiences with your state’s contraceptive initiatives,” or if they “engaged in any activities to increase consumer awareness about the full range of contraception, and/or LARC.” Since social networking relates directly to the focus area of stakeholder partnerships, this was also measured via the question “Since October 2016, has your team engaged with any of the following stakeholders (please include members on your [name of state] Learning Community core team)? Please rate the level of commitment to your jurisdiction’s contraceptive access efforts for each.” The level of stakeholder engagement in a state was measured by the number of different stakeholder organizations rated as at least minimally engaged on the assessment.
Between June and August 2018, all teams participated in semi-structured hour long telephone interviews focused on implementation strategies that they had reported in the 2018 assessment and their overall experiences in trying to increase access to contraception (Figure 2). No individual interviews were conducted. In all, 50 implementation team members participated (Table 1). The initial coding scheme for the Round 2 interviews were the nine focus areas of the Learning Community, as well as codes for any other implementation strategies, facilitators, and barriers. These interviews included the question, “Has your team explored any source of funding, either new or existing, for activities to increase access to contraception across the state, such as provider training, outreach, or other activities?” with further probes if so. Teams that were successful in obtaining or leveraging funds were considered to have received funding. Teams were also asked, “Have there been any participant changes to your team since joining the Learning Community?” and if so, were probed whether and how this impacted their ability to move their work toward their goals forward. Teams that reported a negative impact to their progress due to lack of consistent membership on the team were considered to have experienced slowed progress due to staff turnover.
For both sets of interviews, codes were iteratively developed and applied until no further emergent themes could be identified, at which point topical saturation was considered to have been reached. To refine the identified themes, the team searched for cases that were inconsistent with or contradicted existing themes and considered alternative explanations (Table 1). Both sets of telephone interviews were audio-recorded and transcribed by a third-party vendor. Two to three research assistants independently coded each interview in Dedoose (version 7.0.23, Los Angeles, CA), meeting to discuss and come to consensus on codes. Participants gave verbal consent to interviews and recording. This project received an exemption from the University of Illinois at Chicago Institutional Review Board. All reported names are randomly generated pseudonyms.
Results
Social networking emerged as a salient theme in the Round 1 interviews and was explored to gain a deeper understanding of how social networks are encouraged and influence teams’ implementation efforts. Following CFIR typology, social networking that took place between members of a state team was considered to take place in the “inner setting,” distinct from the social networking that linked the state team with external people and organizations, considered the “outer setting.”
Inner Setting
Bonding within teams
Teams that had formally established responsibilities, a clear leadership structure, or frequent contact were more often aware of each other’s activities, resources, and skillsets. In the absence of formal responsibilities or leaders, teams with frequent informal communication and team bonding were more aware of other team member’s activities, and thereby avoided redundant or wasted effort. Teams were considered bonded if they reported a formal leader or structure, and/or if they had opportunities for informal bonding within the team via existing bonds (generally accomplished by working on prior projects together), or having multiple opportunities for face-to-face communication, most commonly through routine meetings or working in close physical proximity. Participants associated working physically near teammates with more frequent and personally meaningful interactions. Face-to-face communication was a recurrent theme in terms of creating strong working relationships and a shared understanding of priorities and values. In many cases, team members had working relationships before the Learning Community brought them together (Table 2). Not only did teams with preexisting collaborations have established familiarity and trust, many of their formal and informal communications around immediate postpartum LARC policy implementation took place during meetings for those preexisting groups. Members of bonded teams commonly reported working toward shared goals. They also provided mutual social support, and often publicly thanked each other, heralding the importance of each other’s work to team efforts (Table 2). The following interchange between team members from different departments in a bonded team exemplifies this:
Social Networking in the Inner Setting of Implementation Teams in 2015/2016 and Impact of Turnover by 2018.

We really depend on [Kevin’s department] to help with the education aspect of this.
We gladly do it, Maria. [Laughter]
You guys have been great. I know.
After a similar exchange in a different team that bonded primarily through physical proximity and informal contacts, one member said “I appreciate the support from everyone. It’s nice to be part of the team, not just chugging away on our own and feeling a little bit helpless.” Social connections helped create and maintain enthusiasm for the project, in turn spurring implementation efforts forward. These bonded teams often created a collective social network by leveraging internal and external social ties.
Teams without pre-existing relationships or consistent contact were less aware of the overall team’s efforts. One participant of a team without a leader or scheduled team meetings said, “We really needed to coalesce as a team. We have not done that.” In another unbonded team, one member said, “I definitely feel a little left out of the loop by those guys. Either that or they’re just not doing anything at all.” Unbonded teams experienced more difficulty sharing the resources each team member had to offer. A member of one of these teams recounted asking another team member for a particular piece of information for months, but in response received information unrelated to the original request. Without formal or informal engagement, team members had only their own resources to call upon. Further, members of unbonded teams did not tend to perceive shared priorities or goals. One participant talked at length about her own work goals, then asked her teammates whether they had goals of their own. She was not only unaware of what the other team members were doing day to day, but what those day to day activities were driving toward.
Diverse team composition
State teams that joined the Learning Community were encouraged to include a variety of disciplines and professional roles, with a special emphasis on representatives from state health departments and collaborating intra-state organizations (Kroelinger et al., 2015). Although this diversity decreases the likelihood that all team members have pre-existing relationships, it enables them to draw upon a wider array of expertise. One team discussed the utility of including a representative from family practice, since they provide many of the women’s health services in that rural state (Table 3). In another team, gathering data from Medicaid claims to evaluate implementation was complex enough to require coordination between multiple subject matter experts (Table 3). Additionally, teams representing multiple organizations or disciplines benefited from the ability to call upon more diverse social ties, facilitating responses to barriers across multiple domains.
Round 1 Interview Quotations Illustrating Roles of Social Networking in Implementation Efforts.

Interlocking networks
Individuals with concurrent roles on multiple organizational boards or committees may be said to “interlock” the organizations (Granovetter, 1983). Most state teams had members with interlocking working relationships (Table 2), which served multiple purposes, such as introducing members to each other and enabling coordination of strategies and vision. As one participant in a bonded team put it, “It’s also helpful to kind of get on the same page so that different organizations aren’t going down different paths.” Interlocking also provided informational support, as in this example where a member in a bonded team drew upon other concurrent state work to inform immediate postpartum LARC efforts: “I sit on another committee around [infant health in the state], and they’re doing some pilot work. . .could be at least a useful or interesting model to consider.” State teams described instances in which interlocking assisted in gaining access to instrumental resources, as when a person secured a stockpile of devices for a hospital system through a residency program she was involved in. Interlocking networks also assisted in creating a shared appreciation of the importance of policy change among leadership (Table 3).
Outer Setting
Existing social networks utilized for new purposes
The vast majority of teams had pre-existing relationships and agreements with external organizations and were able to draw upon them for support in immediate postpartum LARC policy implementation (Table 4). Teams found that past work with these organizations enabled more stable partnerships in the present. Existing coalitions and consortiums were mentioned repeatedly as a method of engaging others and advancing the work, especially when they prioritized immediate postpartum LARC access in their portfolio of projects (Table 3). One participant from an unbonded team with a pre-existing social network said, “The great thing about the [healthcare] coalition is I get everyone at one table. . . I don’t have to do very much work to find my stakeholders. They’re already there and they are really supportive of this work.”
Social Networking and Implementation Progress in the Outer Setting at Two Time Points: 2015/2016 and 2018.

Of their consortium in another state, a member of a bonded team with pre-existing social ties remarked, “It’s for us not only helpful that we have an existing infrastructure, but very helpful that this is prioritized at the top of that sustained infrastructure.” Implementation or communication problems sometimes arose in the absence of preexisting relationships. One member of an unbonded team without external connections said, “We’ve tried to partner with [private insurers] for some stuff, and it’s just not been real successful. A lot of the administration has changed at those insurance companies.”
Those teams with pre-existing working relationships considered them critical to their implementation efforts.
External ties as bridges to new social networks
In addition to using preexisting social ties, teams also sought new ties (Table 3). Participating in the Learning Community served as an opportunity for teams to make new external connections (DeSisto et al., 2017). In some cases, a single person served as a crucial bridge to a previously unconnected social cluster (Table 3), creating connective social networking structures. Often a single social tie facilitated connections to other states, to the Learning Community, or to other potential partners. Team members repeatedly said things like, “I’ve reached out to [bridging social tie] and he helped me reach out to a couple other states.” By contrast, the problem with relying on a single relational tie to a larger social network is illustrated by this quote, “We’ve reached out to [him] three times. . . It’s just been a dead end. Absolutely zero response.” When a single person was the sole link to new information or connections, and that person was busy or unable to assist, communication and meetings were delayed or entirely prevented.
External ties as sources of informational support
Evaluating implementation progress through surveys or medical or payer claims takes time and resources. Teams reported that tracking immediate postpartum LARC access though informal social ties with health care providers and hospital administrators was faster and required less resources. These networks also helped identify barriers to progress. One participant in a bonded team with a pre-existing external social network recounted, “we were hearing from them, the OBs, that these devices were so expensive. The way we were paying for it was as part of the [bundled labor and delivery reimbursement rate]. Hospital administration wouldn’t even order the LARCs. . .That effectively made them unavailable.” Someone from another team (unbonded, without a pre-existing external social network, that relied upon creating new social ties) cited the usefulness of the perspective given by these connections, saying, “You kinda get a real good understanding of the obstacles and challenges that each group is facing within that hospital system.”
Communication with teams in the Learning Community from other states provided opportunities to compare efforts and outcomes as well as share resources and detailed information about implementation strategies. For teams early in the implementation process, talking in-depth with other state teams helped solve current and anticipate future problems (Table 3). Teams that were further along in the process found these conversations helped them stay focused, accountable, and gave them opportunities to reflect on and evaluate their work.
External ties as sources of instrumental aid
Connections with non-profit organizations primarily resulted in instrumental support for patient outreach, provider training, LARC device funding, or device donations. One internally bonded and externally networked team secured years of funding in part due to a single social connection that bridged previously unconnected networks (Figure 3 diagrams the formation of links between social clusters). In that instance, a private foundation approached a family practice doctor because they were interested in reducing the high teen pregnancy rate in the county. The doctor connected the foundation to a member of the state team, who he previously partnered with in private practice. After a presentation by that team member, the foundation agreed to help the state team, and also convinced two other foundations to provide additional funding. Another team leveraged the tie between a state political leader and a non-profit CEO to secure provider training on LARC insertion, provided by the nonprofit. When a new social tie connected the team to instrumental support, the team always institutionalized the new relationship through formal contracts.
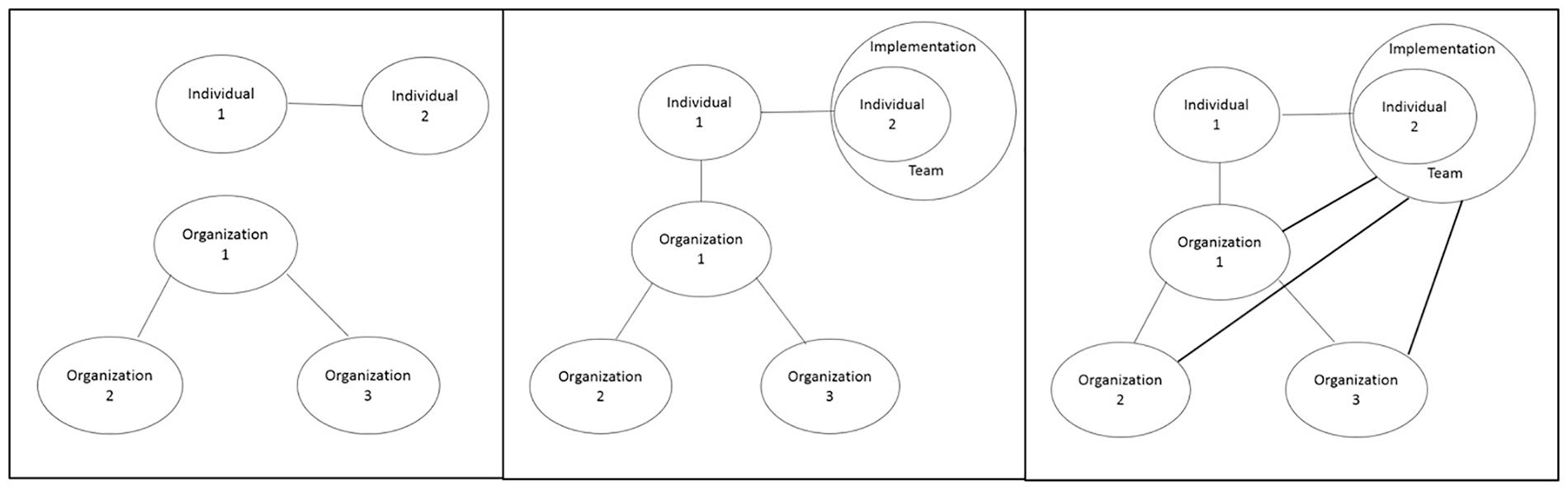
From Round 1 interview, unconnected social clusters before state team created (left), after first bridging tie between clusters (center) and after subsequent social ties and formalizing of relationships (right).
External ties as sources of emotional support
Simply talking to people external to the state team who were working toward the same goal was referred to as energizing and inspiring. As one participant from an unbonded team put it, “when I’m ready to just throw my hands up and say, ‘I can’t do this anymore,’ then I go to [health collaborative meeting]. . .It does get me re-inspired.” Discovering that other Learning Community states experienced similar problems allowed teams to exchange emotional and appraisal support (Table 3). One member in a bonded team explained, “I also appreciate kind of the commiseration. Not everything’s perfect. I think that it is really nice to be a part of the community where you actually hear other people’s struggles as well. . . and hopefully it will help speed up the corrective actions that we can take because we can learn from others.” Another participant of an unbonded team noted that seeing “we’re not the worst off” was helpful, but also “the stories of people who have had more success are inspirational and instructive.” Teams also shared implementation successes from other states to inspire and engage their own stakeholders. A bonded team member expounded, We were inspired by [state’s] effort to make policy changes and start this program. Really, we copied what [state] was doing. We relied on them. We gained momentum. . .Once I presented it to leadership here they were excited. . . We got everybody excited here at the agency about doing this and we got it done.
Implementation Progress
Web-based assessments and the Round 2 telephone interviews with the implementation teams conducted in 2018 provided insights into how their social networks had developed over time and influenced implementation efforts. Staff turnover within implementation teams was a commonly cited barrier to goal achievement in the Learning Community (DeSisto et al., 2021). Eleven of the 13 teams experienced turnover between the 2015/2016 and 2018 interviews in their core implementation team. Interestingly, teams that were bonded in 2015/2016 tended to report that by 2018 they had experienced less disruption due to transitions within the team: in 2018, 33.3% (n = 3) of the bonded teams reported staff turnover was a barrier to implementation, whereas 75.0% (n = 3) of the unbonded teams felt that staff turnover slowed their progress (Table 2). Someone from a team that was socially bonded in 2015/2016 reported in 2018: “it’s been great to work with such a great team that have such a long history and experience and good trust and respect.” People who joined teams that were bonded in 2015/2016 described being able to “hit the ground running,” saying that “[staff transitions] didn’t slow us down like it could have. I think in other instances where we’ve had teams change over, we haven’t had that great of success as we’ve had this time.” By contrast, someone in an unbonded implementation team that had lacked formal team structure or frequent contact between team members in 2015/2016 reflected in 2018, “Everyone who’s worked on the LARC project has left. . .we do joke that the LARC initiative is the strongest predictor of who’s going to leave, whether you know it or not. Because it’s one person after another. . .” This directly led to delays: “every time someone came and went, the project would get dropped for a while. . . I think it’s really made a big difference because there’s no other reason, really, to say why it’s 2018, a couple years later, and we still don’t have [this goal accomplished].”
States reported at least minimally engaging 8 to 19 different stakeholders in their work to increase contraceptive access in their jurisdiction. Based on the bimodal distribution of the data, a state was considered to have “high stakeholder engagement” if teams listed at least 10 different organization types. The degree of social networking in the outer setting that implementation teams could leverage in 2015/2016 was associated with higher ratings of engagement with stakeholders such as community health workers, provider associations, minority health associations, and non-profit organizations in 2018 (Table 4). All but one team that reported high levels of stakeholder engagement in 2018 included team members already capable of leveraging pre-existing ties with external stakeholders in 2015/2016. Level of stakeholder engagement in 2018 was influenced by many factors unmodifiable by the implementation team, including the political climate and amount of resources available to stakeholder organizations. However, it is notable that the three teams without known social ties that could be used to create formalized connections in 2015/2016 all described difficulties in 2018 such as, “we’ve tried to engage the [health organizations] around the state. . .we’ve been unsuccessful. . .Identifying the key players, I think is sometimes what’s difficult for us.”
By 2018, all but one of the thirteen participating states had accomplished Medicaid policy change for immediate postpartum LARC insertion (Table 1). Bonded state teams with higher levels of stakeholder engagement tended to have conducted activities to increase consumer awareness of contraception in their area (83.3%, n = 5), compared with other states (66.7%, n = 4). Further, more socially networked teams conducted a higher number of healthcare provider trainings (mean: 18.8) than states that reported lacking necessary external stakeholders (mean: 4.8). Although team members frequently referenced the importance of social ties in identifying potential funding sources, there was no clear relationship between social networks in 2015/2016 and successfully securing funding for implementation activities by 2018. Summarizing their work over the past years, one member of an internally bonded and externally networked team said in 2018, “it’s really the partners, the communication between the partners. . .Each area has an area of expertise that we’re able to pull and draw from . . . there’s the private funders, the foundations that have also been assisting in those efforts and organizations throughout the state. I think those two items have probably been some of the greatest success and reasons for success.”
Discussion
State teams working toward expansion of immediate postpartum LARC access used social networking as an implementation strategy. This analysis highlights factors that encourage or enable social networking during an implementation effort, and how social networks may facilitate implementation. The structural characteristics of social networks, and the mechanisms by which social ties were created, varied between the inner and outer setting. Within the inner setting of the state team, the social network was dense (meaning many of the possible relational ties were present, per Granovetter, 1983) and the ties within the team were generally organically created and maintained by collaboration on prior or concurrent projects. Physical proximity of work locations, regularly scheduled meetings, and formally assigned roles and responsibilities encouraged denser networks and team bonding. In the outer setting, teams relied on bridging social ties that connected them to new social clusters, such that social networks in the outer setting were less dense, more geographically dispersed, and intentional effort was commonly expended to create and maintain them.
The experiences of these 13 teams demonstrate the variety of advantages to the implementation process garnered by cultivating and leveraging working relationships. Relationships within teams immediately assisted with cohesion and coordination of efforts, which in turn reduced the disruptive impact of staff turnover as the implementation process continued over time. Consistent with the integrated model for building collaborative capacity (Foster-Fishman et al., 2001), the diverse skills, roles and organizations of team members enhanced not just the knowledge and skills of the team, but also the collective social networks the implementation team could draw upon in order to successfully address strategic areas such as consumer awareness or healthcare provider training.
As seen in other contexts, the history of relationships between organizations affected their ongoing working relationships (Chertoff et al., 2018; Dunlop et al., 2016; Thompson et al., 2002). Social networking with organizations or coalitions in the outer setting predominantly provided instrumental support (such as funding, training, and marketing) and knowledge of providers’ early implementation concerns and barriers. Additionally, teams intentionally sought out new social ties in the outer setting for informational and appraisal support, incidentally also receiving emotional support. Congruent with the aspect of the “strength of weak ties” theory that posits that bridging social ties connect people to new information (Granovetter, 1983), these new social relationships were sources of information or tangible aid otherwise unknown to the team.
Most participating teams were both internally bonded and externally connected. A few had strong ties within their team but lacked useful social connections outside of it, or vice versa. No team considered having many working relationships as a problem, but several teams reported being hindered by having too few, and 2 years later these teams struggled engaging necessary external stakeholders.
This study has several limitations and strengths. The health and payment systems and resources available varied widely between teams. Some teams began work to access to immediate postpartum LARC years before others. This variance complicates comparisons between teams, but enhances the generalizability of the findings. Team members were usually interviewed together, creating an opportunity to observe their interactions and communication styles, but possibly restraining individuals from discussing negative aspects of their work together. Interviewing via telephone enabled repeated interviews with all state teams but prevented interviewers from noting body language or non-verbal communication. Interviewing only the state teams meant that only their views of the social networks were investigated. How the teams’ partner facilities, clinicians, patients, leadership and stakeholders viewed their relationships remains unknown. However, because every team in the Learning Community was interviewed, networking across state teams was potentially fully available for study. Social networking was an emergent theme in an evaluation not designed to assess social relationships, so interviews may have missed pertinent insights. This does mean that the social networking examples and insights were verbalized entirely because participants themselves considered them important and pertinent to their implementation process. Finally, these findings are based on multiple assessments of implementation teams over more than 2 years. This allows for triangulation of findings, potentially reducing biases from either survey or web-assessment data alone, and most importantly enables assessment of whether social networking precedes and affects implementation accomplishments.
Conclusion
Increasing access to immediate postpartum LARC can be a complex, multi-agency effort. Within a systems changing implementation project such as this, efforts to build social networks serve a variety of functions. Internal team cohesion appeared to optimize collaboration, reduce disruptive staff turnover, and enable the creation of an external collective social network. External social networks provided information and infrastructure for implementation activities, tangible aid and services, and progress appraisal. Creating or strengthening external relationships aided teams in identifying and effectively communicating with necessary stakeholders such as private payers, reproductive justice groups, or organizations with the resources to provide immediate postpartum LARC-related trainings for health care providers. The implications of this study are not limited to immediate postpartum LARC policy implementation. Social networking could be used in other multi-agency, multi-system collaborations, or implementation efforts requiring complex and coordinated changes. Routinely cultivating and maintaining formal and informal relationships between agencies and organizations enables availability for future implementation efforts. Multi-agency teams may benefit from prioritizing time for internal and external relationship-building to enhance implementation efforts.
Footnotes
Acknowledgements
The authors wish to thank Drs. David A. Goodman and Charlan D. Kroelinger, as well as all of the ASTHO Immediate Postpartum LARC Learning Community state teams, for contributing their time and expertise.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the Association of State and Territorial Health Officials.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This evaluation was considered exempt by the University of Illinois at Chicago Institutional Review Board. All participants gave verbal consent and were aware participation was voluntary.