
Abstract
This study investigated the social impact of COVID-19 on healthcare workers and their relationships with their families and relatives. Data were collected from a sample of 226 healthcare workers (HCWs) using an analytical cross-sectional design. The data extracted three factors: communication impairment, social avoidance, stigma, and personal deprivation and distress, rated as severe, moderate, and moderate, respectively. The results showed that HCWs’ social and personal lives were significantly affected, ranging from predominantly moderate to highly severe. The variability of the three factors coordinated with marital status and working hours showed a mixed pattern. Discontinued workgroups are more affected by communication impairments, social avoidance, and stigma, less emotional and personal deprivation. HCWs with lower levels of education suffer more severe impacts of working with COVID-19 patients than those with higher educational levels. The study highlights the social impact of working with the COVID-19 patients on healthcare workers and the need for more social support and institutional support.
Introduction
The coronavirus disease 2019 (COVID-19) outbreak has been described as the “biggest public health problem in a generation” (Plan International, 2020) and “a significant threat to humanity” (Gupta, 2020) that wreaks havoc on otherwise well-functioning health systems economies, and social networks (Rana et al., 2020). COVID-19 negatively impacts even those working on the frontlines of safeguarding societies and individuals. Working with infected patients exposes healthcare workers (HCWs) to the virus, putting them at high risk of contracting the disease or experiencing psychological discomforts, including bullying and harassment (Abolfotouh et al., 2020; AlAteeq et al., 2020; Bruns et al., 2020; Qiu, et al., 2020; Spoorthy et al., 2020; Yin et al., 2020).
Recent literature has extensively focused on the mental health impacts of COVID-19 on HCWs, (Alshekaili et al., 2020; Cai et al., 2020; Hamdan-Mansour et al., 2020; Kisely et al., 2020; Lai et al., 2020; Spoorthy et al., 2020; Yin et al., 2020; Wahed et al., 2020). According to Vindegaard and Benros (2020), research on the direct neuropsychiatric consequences and indirect effects of such diseases on mental health is critical to improving treatment, mental health care planning, and preventive measures during potential future pandemics. Nevertheless, the social and family lives of HCWs have been significantly interrupted and affected by the Pandemic, and this deserves appropriate attention (Al-Hanawi et al., 2020; De Laat et al., 2011).
Muller et al. (2020) evaluated 59 studies on staff working in diverse healthcare settings with varying levels of coronavirus severity and found that workers in contact with infected patients had higher levels of acute and posttraumatic psychological distress. Further, several studies (Conway et al., 2020; Kisely et al., 2020; Pappa et al., 2020; Wasim et al, 2020) have highlighted the dangers of morbidity and psychosocial repercussions on HCWs tasked with responding to COVID-19 in hospitals and related settings. According to a systematic review of 55 studies by Cabarkapa et al. (2020), HCWs show an increased risk of traumatic or stress-related disorders, depression, and anxiety. The biggest mental challenge was the fear of the unknown and the fear of becoming infected. Nurses and women appeared to be at greater risk. Vindegaard and Benros (2020) reported similar findings in their review.
The impact of COVID-19 on HCWs, concerning social aspects, is insufficiently researched even though we have seen that their social and family lives are significantly interrupted and affected by the Pandemic (Al-Hanawi et al., 2020; De Laat et al., 2011). According to Cabarkapa et al. (2020), family members and society’s perceived stigma heightened negative implications, predominantly stress and isolation. Xiao et al. (2020) argued that social support for medical staff had a significantly positive impact on self-efficacy and sleep quality and negatively impacted anxiety and stress. Noticeably, HCWs continued to work during the outbreak, devoting their time and effort to protecting the general public and adhering to their social and moral responsibilities (Cai et al., 2020; Jahrami et al., 2021). Regrettably, HCWs do not receive the necessary social support they need. Social and emotional support and empathy can surely help medical staff reduce anxiety levels.
During the Pandemic, healthcare workers were vilified, and people avoided them in their communities because they were regarded as carriers of the viral infection. According to Taylor et al. (2020), more than a quarter of non-HCWs adults (1,716 from the United States and 1,835 from Canada) believed that the liberties of HCWs should be significantly restricted, including isolating themselves from their communities and families; more than a third responded that they avoided HCWs for fear of infection. Another study by Mostafa and Mostafa (2020) on 509 physicians working directly or indirectly in COVID-19 care routes in Egypt found that most HCWs experienced stigma related to COVID-19. Further, factors like young age, lower qualifications, and working in quarantine hospitals were independently associated with stigmatization related to COVID-19, with 25.3% of study participants experiencing severe stigma and higher scores on the negative self-image scale. Bagcchi (2020) reported several cases of stigmatization of healthcare workers, COVID-19 patients, and survivors worldwide during the Pandemic. For example, doctors rode bicycles in Mexico after being denied public transportation and subject to physical assaults.
Similarly, healthcare workers in Malawi were reportedly denied access to public transportation, insulted on the street, and evicted from rental apartments. Media reports in India stated that doctors and medical staff caring for COVID-19 patients faced significant social ostracism, including being asked to vacate their rented homes and facing attacks (Bagcchi, 2020). Several studies showed that anxiety, stress, and self-efficacy are mediating variables associated with social support and sleep quality; social support reduces anxiety and stress and improves self-efficacy (Amin, 2020; Chen et al., 2020; Xiao et al., 2020).
Gunawan et al. (2020) reported that their communities rejected nurses and medical doctors in Indonesia and Thailand because they were considered a means of viral transmission. As Ramaci et al. (2020) argued, social stigma in the health context is negatively associated with people or a group with a common specific disease. Thus, social stigma is more evident, especially when dealing with a highly contagious disease like COVID-19, and it is common for HCWs who serve such patients. Unfortunately, the stigma goes beyond death. For example, one female physician was denied burial rights in her neighborhood in Egypt; the Egyptian Prime Minister condemned this action, as it contradicts and violates all religious teachings and human rights (BBC, 2020).
Purpose and Objectives
The current study examined the social and family impacts of serving COVID-19 patients on HCWs in Saudi hospitals and healthcare facilities.
Methodology
An analytical cross-sectional design was used to assess the impact of the COVID-19 epidemic on healthcare workers who served in hospitals and medical centers designated for such patients and suspected infections. The study focused on the first health cluster in the Eastern Province of Saudi Arabia and included 12 hospitals and 188 primary healthcare centers.
The questionnaire was distributed electronically to the sector’s HCWs, including physicians, nurses, allied health personnel, and administrative staff. HCWs who were active in providing care for COVID-19 confirmed and suspected cases and agreed to respond to the survey were included in the study. Out of the 600 HCWs contacted electronically, 226 completed the questionnaire, with a response rate of approximately 38%.
The characteristics of the study are listed in Table 1 sample. Around two-thirds were women, and a very high percentage were married. All samples had post-secondary education, with a very high percentage indicating a continuous work assignment, implying that they spent considerable time away from their families, with relatively fewer HCWs working intermittently.
Characteristics of the Sample.

The Psychometric Properties of the Instrument
This paper highlights the social impact of a larger study on the psychosocial impacts of COVID-19 on HCWs in the Eastern Region of Saudi Arabia. Therefore, the questionnaire was based on exploratory discussions with several HCWs and their colleagues. This section initially consisted of 17 items, 12 of which correlated at least (three or more) with one other item. In five items, the commonality was less than 0.30, so they were removed because they did not contribute to a simple factor structure. One item had cross-loading over 0.4, and it loaded to a higher item. The Kaiser-Meyer-Olkin sampling adequacy measurement was 0.851, which was greater than that of the generally prescribed value of 0.6, and Bartlett’s test of sphericity was significant (at χ2 (66) = 1,305.868, p < .05).
Moreover, all diagonals of the anti-image correlation matrix exceeded .5. All commonalities were above 0.30 (Table 2), confirming that each item shared some common variance with other items. Given these overall indicators, only 12 items were retained for the factor analysis (Hatcher, 1994; Hill, 2011).
Pattern Matrix, Loadings, Eigenvalue, and Communalities for Social Scale.

Note. Factor loadings <0.4 are suppressed.
Extraction method: Principal axis factoring; Rotation method: Promax with Kaiser normalization.
A description scale was used to assign levels for the mean values obtained. The following formula was used to assign the means levels:
Accordingly, the three levels of severity are 1.00 to 2.33 low, 2.34 to 3.67 moderate, and 3.68 to 5.00 high.
The Severity of social impact is based on the formula: Category length = (highest weight-lowest weight/number of categories = 5 − 1/3 = 1.33; thus, low (1.00–2.33), moderate (2.34–3.67), high (3.68–5.00). This was based on the duration of the impacts from the highest (always) to the (never) incidence.
The internal consistency of the social scale (17 items) using Cronbach’s alpha showed a value of .904; this high score reflects high reliability, which is an acceptable value (Santos, 1999). The internal consistency of the refined scale was 0.866, and the internal consistency for each subscale was acceptable at 0.823 for FACT1 (five items), 0.862 for FACT2 (four items), and 0.844 for FACT3 (three items). Eliminating more items did not yield any substantial increase in the alpha for any of the main or sub-scales. Overall, these analyses indicated three distinct factors (FACT1, 2, 3) underlying the sample responses and were internally consistent (De Laat et al., 2011).
Factorability of the scale
During the data screening and preliminary analysis, the following issues were addressed for further analysis (Tabachnik & Fidell, 2013):, missing data, outliers among cases, and normality of variables. The percentage of the missing values in the data was around (6.2%). Results of Little’s MCAR test (Little, 1988) on whether values were missing completely at random (MCAR) were insignificant (χ2 (59) = 73.340, p = .099), suggesting that values were missing entirely at the chance.
Data were evaluated for univariate and multivariate outliers by examining Mahalanobis distance for each participant. Univariate or multivariate outliers were 31 cases with 13% considered acceptable.
Principal axis factoring (PAF) analysis was used instead of principal component analysis (PCA) because PCA assumes no error (Brenner, 2019). The initial eigenvalues revealed that the first three factors explained ~44%, 11%, and 7% of the variance, respectively. The fourth, fifth, and sixth factors had eigenvalues greater than 1, and each factor explained ~6%, 5%, and 4% of the variance, respectively. Solutions for the fourth, fifth, and sixth factors were examined using the Varimax and Promax rotations of the factor loading matrix. The three-factor solution, which explained ~62% of the variance, was preferred because of (a) its previous theoretical support, (b) the leveling of eigenvalues on the Scree plot after three factors (Figure 1), and (c) a lack of primary loadings and the difficulty in interpreting the fourth and subsequent factors. The three-factor Varimax and Promax solutions were nearly identical. As a result, both solutions were tested in subsequent analyses before settling on a Promax rotation as the final solution (Hatcher, 1994).

CFA scree plot.
A PAF analysis was conducted using Promax rotations for the final stage, with three factors accounting for 62% of the variance. The Promax rotation provided the best-defined factor structure. All items had primary loadings over 0.4 (Table 3).
Descriptive Statistics for Social Scale (N = 195).

Results
Table 4 shows the original social impact scale comprised of the 17 items and presents the sample distribution on all scale items before extracting the factors.
Descriptive Statistics of the Social Impact Scale Items.

In general, the distribution demonstrates varying degrees of severity of the impact of COVID-19 on HCWs’ social and family lives and interpersonal interactions. The severity ranges from moderate to high, with only one item/variable having a low impact. The higher social impacts were seen in the inability to participate with family and relatives on social and religious occasions, fear of transmitting the infection to the family, no physical contact with spouse, children, and parents; a state of panic in family and work-life; and weakened or no communication with friends. All other items/variables exhibited moderate impact. The only item with a low degree of severity was “I do not like to go home because of family problems,” indicating that there were no family problems initially. However, the detailed results showed that around 15% of respondents have problems (always or usually), with around one-fourth facing problems sometimes.
Three factors were extracted from the data describing the social impact of COVID-19 on HCW family relationships, including communication barriers, social avoidance, emotional deprivation, and personal suffering.
Communication Barriers and Interaction Problems
Factor 1 includes communication problems: SOC1—Being away more frequently from family and home, SOC2—Difficulties and weakness of communication with family, SOC3—Difficulties and weakness of communicating with family (parents), SOC7—Not kissing my spouse, children, and parents, and SOC17—Weakness or no communication with friends. By being involved in efforts to combat the COVID-19 epidemic, HCWs could not communicate with their immediate family (spouse and children), extended family (parents and relatives), and friends. Considering the importance of family and kin ties in an oriental society that sanctions social relations and responsibilities, the overall score of severity for Factor 1 is high. Thus, communication has a significant social impact of COVID-19 on HCWs assigned to respond to the epidemic. This is understandable considering their overwhelming work and the lack of free time to communicate with their families and social networks.
Social Avoidance and Stigma
Factor 2 represents unexpected reactions from family, relatives, and friends and can be called tension with family, resulting in social avoidance and stigma. This factor includes: SOC8—Family and relatives’ reluctance to extend help, SOC9—Family fears me going home because I work with corona patients, SOC11—My family tries to evade my visits, and SOC12—The nature of the coronavirus epidemic created tension in our family. These items indicate that families were abandoning those members who serve COVID-19 patients. The overall severity score of this factor was moderate.
Emotional and Personal Sufferings
Factor 3 encompasses the personal suffering of HCWs, with items including: SOC13—I would not like to go home because of family problems, SOC14—I suffer from loss of and lack of privacy, and SOC15—Deprivation or difficulties in fulfilling the emotional needs of the spouse. Factors 1 and 2 paved the way for Factor 3, representing emotional and personal suffering. As explained earlier, HCWs experience a lack of and inability to communicate with their families, relatives, and friends. Simultaneously, there is a thread of family tension and avoidance of the members who work in healthcare settings serving COVID-19 patients. The cumulative effects of these experiences could be reflected in the personal and emotional well-being of HCWs. The overall severity score for Factor 3 was moderate (Table 5).
Factor Loadings, Communality, Means, Standard Deviations for the Items Comprising VAR1, VAR2, and VAR3 and Social Impact Severity.
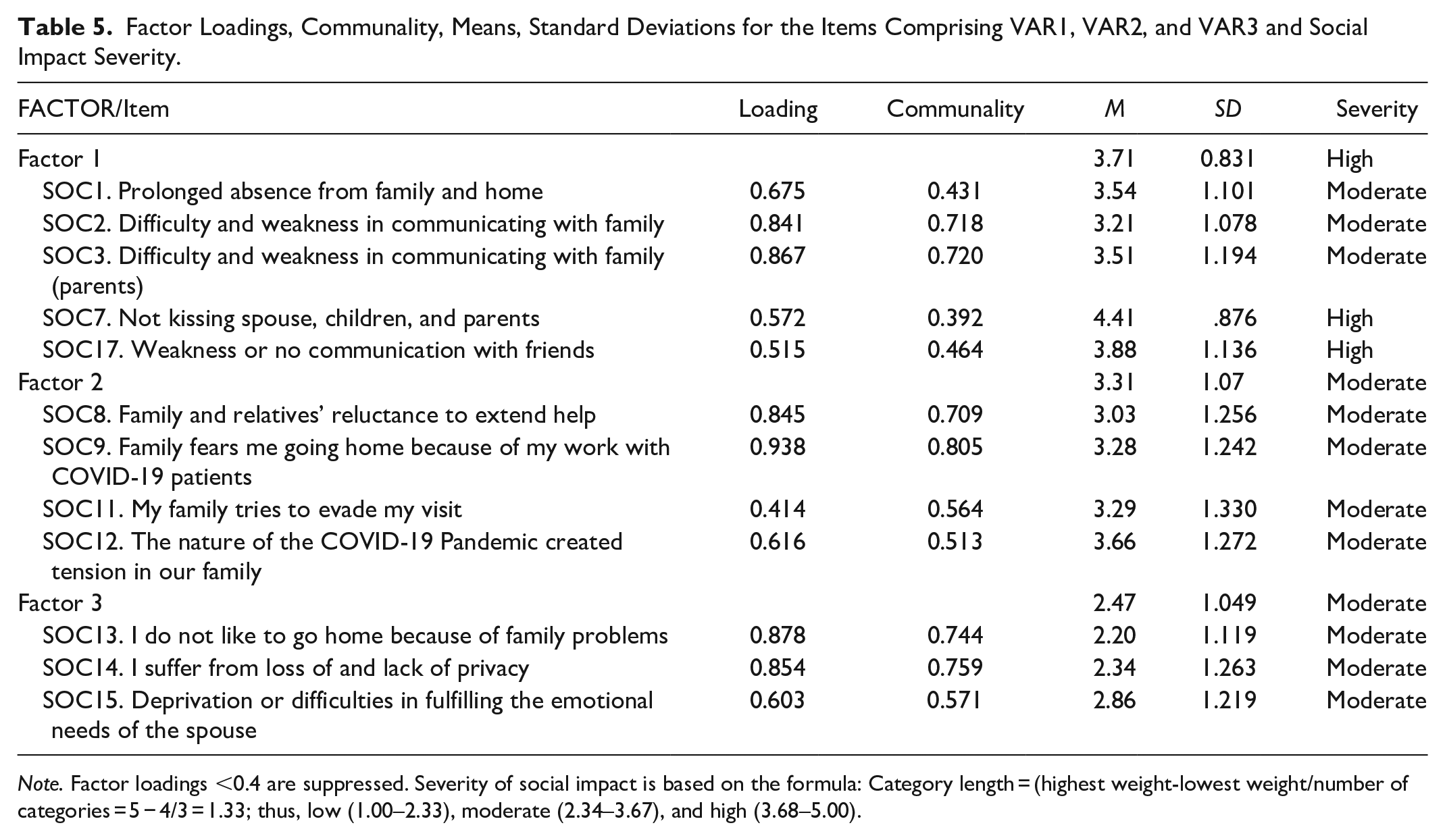
Note. Factor loadings <0.4 are suppressed. Severity of social impact is based on the formula: Category length = (highest weight-lowest weight/number of categories = 5 − 4/3 = 1.33; thus, low (1.00–2.33), moderate (2.34–3.67), and high (3.68–5.00).
Variability Among Subgroups
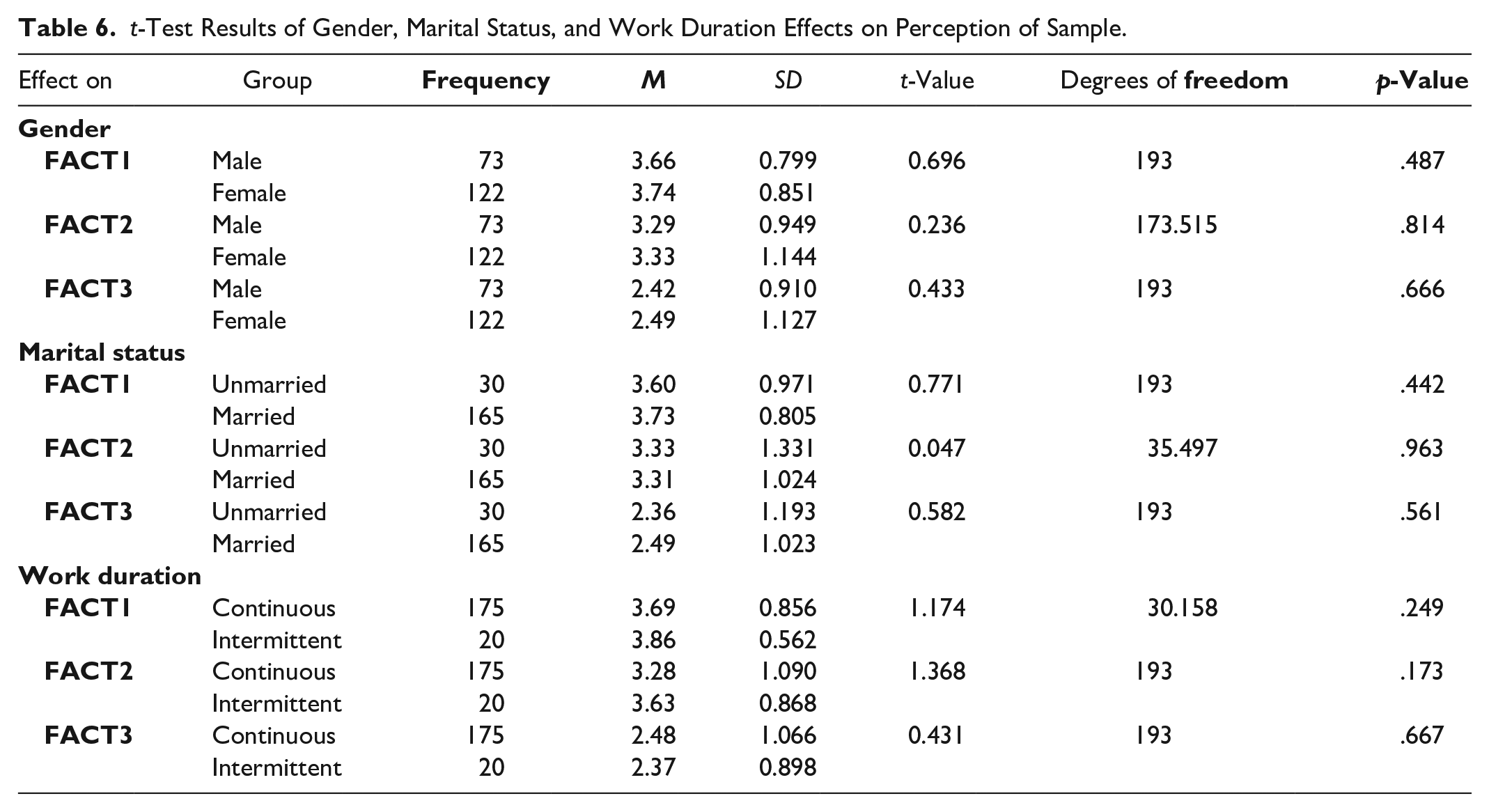
Factor variability was tested among the sample subgroups using the t-test and one-way analysis of variance. Analysis results detected no significant differences among the three subgroups (i.e., gender, marital status, and work duration) among the three factors. However, minor differences were observed. For example, females showed higher means and variability than males for the three factors (Kim et al., 2020). The variability of the three factors showed a mixed pattern. For example, married people showed more severe impacts on Factor 1 (communication barriers) and Factor 3 (personal and emotional deprivation), with less impact on Factor 2 (social stigma and isolation). The levels of impact on work duration were more severe in the group that worked intermittently on Factors 1 and 2, with less impact on Factor 2. These mixed results require further studies with different and probably larger samples (Tables 6–8).
t-Test Results of Gender, Marital Status, and Work Duration Effects on Perception of Sample.
One-Way ANOVA to Select Groups With the Three Factors.

p ≤ .05.
Scheffe Post Hoc Results of Education Level Effect on Perceptions of Sample.

Mean differences are statistically significant at .05 level such that the difference is in favor of the category with the greater mean.
A one-way analysis of variance test was used to compare the groups (education level, income level, and healthcare worker specialty) on the three factors. Only one comparison showed significant differences, on education level. In Factors 1 and 2. Scheffe’s post hoc results of education level showed that HCWs holding a diploma experienced more severe social impacts on Factors 1 and 2 compared to the higher education levels (bachelor and graduate degree). HCWs with diplomas differed from those holding graduate degrees on Factor 2 (avoidance and stigma) and Factor 3 (personal deprivation and emotional deprivation). It is expected that those workers were at the bottom of the professional ladder, burdened with heavier workloads, and likely less compensated. In healthcare settings, professional stratification exists, with the physician placed at the top, physicians further experience internal stratification based on their areas of specialization and experience. HCWs with bachelor’s degrees differed significantly on Factor 2 from those holding graduate degrees. These results may indicate that HCWs with lower levels of education suffer more severe impacts of working with COVID-19 patients than those with higher educational levels.
Discussion
The study results show that, in general, HCWs experience marital or family problems. This may indicate that their daily work, regardless of COVID-19, is overwhelming and may interfere or even interrupt their family lives and deteriorate further with the Pandemic. The analysis revealed a significant concern that HCWs experience problems communicating with their families and relatives. Communication barriers form a significant social impact of COVID-19 on HCWs assigned to respond to the epidemic. This is understandable considering their overwhelming work and lack of free time to communicate with their families and social networks. However, the importance of social support and communication cannot be ignored. Reddy and Gupta (2020) emphasized the importance of effective communication for HCWs in dealing with patients and others.
In addition, to the communication barriers, the family’s fear of contracting the infections from HCWs who work with COVID-19 patients created tension and panic. Thus, families were not welcoming their HCWs members (e.g., husband, wife, sons, and daughters) to come home for a break and even forcing them to quarantine themselves in isolated units in their own homes. These results align with Ramaci et al. (2020), who indicated that uncertainty, stigmatization, and potentially exposure to their families to infection were prominent themes for HCWs during the crisis. Healthcare professionals, particularly those caring for people with confirmed or suspected COVID-19, are at risk of infection and mental health issues, and may also be concerned about spreading the virus to their families, friends, or coworkers (Xiang et al., 2020). Early in the pandemic outbreak, the World Health Organization (2020) warned that some healthcare workers might experience avoidance by their families or communities owing to the stigma or fear of contracting the disease. The WHO (2020) suggested that healthcare workers stay connected with loved ones through digital methods to mitigate the negative impact on their family relationships. Healthcare institutions should offer psychosocial support to HCWs and respond to work stress and pressures they encounter in their service to coronavirus patients and their families.
Limitations
An online questionnaire was sent to approximately 600 healthcare workers in a cluster of hospitals and health centers. About 226 participants completed the questionnaires. Consequently, the findings of this study may be interpreted cautiously. Despite this limitation, the study revealed interesting findings on the social impact of COVID-19 on healthcare workers.
Conclusions
Although COVID-19 interrupted the lives and work of billions of people, HCWs were hit the most. In order to examine the impact on HCWs, we studied the behavior patterns of workers in eastern Saudi Arabia’s cluster of hospitals, clinics, and transitional compounds designated to such cases. HCWs worked full-time; some even worked around the clock to respond to the Pandemic in that region. As a result, HCWs were compelled to live apart from their families and communities for an extended time. The high demands of such work created a harmful impact on the lives and well-being of HCWs and their families. The impact of COVID-19 on the social aspects of such relationships is discussed in this article. The general findings of the data show that the social and personal lives of HCWs were remarkably impacted to varying degrees, from mainly moderate to high severity. The data revealed three factors, including communication barriers, avoidance and stigma, and personal deprivation and suffering.
Footnotes
Acknowledgements
Special thanks to Shari Yores for editing the manuscript and to Muhammad Alhur for helping with statistical analysis. We are greatly indebted to the healthcare workers in the fifth Health Cluster in the Eastern Province of Saudi Arabi for their kindness in responding to our questionnaire.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for the present study was obtained from the concerned department at the health cluster, allocated as an emergency response to the COVID-19 pandemic. In addition, the nature of the study was explained to the participants as well as the requirement for their consent. They were informed that their participations were voluntary, they could withdraw from the study at any time, and the anonymity and confidentiality of the data were assured. Only those who agreed to the ethical requirements and informed consent participated in the study.