
Abstract
This study explored the prevalence of depression, anxiety, and stress among healthcare workers (HCWs) in Kosovo. To shed light on the mental health of HCWs in Kosovo, the hypothesis that depression, stress, and anxiety levels will be elevated, particularly among those working in emergency departments, was tested. The study included 141 participants aged between 19 and 65 years, selected from both urban and rural areas of Kosovo using a semi-purposive sampling method. Participants completed the DASS-21 questionnaire. Participants’ demographic data were presented through descriptive analyses along with the prevalence rates of the DASS-21 indicators. These findings indicate a high prevalence of depression, anxiety, and stress among HCWs in Kosovo, especially among those employed in emergency departments.
Plain Language Summary
This study looks at the mental health of healthcare workers (HCWs) in Kosovo, focusing on depression, anxiety, and stress. The research included 141 healthcare workers, aged 19 to 65, from both cities and rural areas. They answered questions using a well-known survey called the DASS-21 to measure their mental health. The results showed that many healthcare workers experience high levels of stress, anxiety, and depression, especially those working in emergency departments. These findings highlight the need for better support for healthcare workers to help them manage their mental health and improve their well-being.
Introduction
Healthcare workers (HCWs) are exposed to high levels of stressors in the workplace, putting their health and well-being at risk. HCWs simultaneously perform delicate and complex tasks. Diagnosis, treatment, time pressure, staff shortages, inadequate equipment, and many patients are just a few of the challenges that HCWs face. Many studies have emphasized the widespread occurrence of mental health challenges among HCWs (Saragih et al., 2021), reporting a prevalence of 37% for stress (95% CI: 25–50%), 40% for anxiety (95% CI: 29–52%), and 27% for depression (95% CI: 29–45%). According to Lai et al. (2020), healthcare workers who are directly engaged in diagnosing, treating, and caring for COVID-19 patients faced an increased risk of developing symptoms such as stress, anxiety, and depression.
In Kosovo’s healthcare system, HCWs are categorized into primary, secondary, and tertiary care providers depending on the type of care (Ademi Osmani et al., 2017). Primary care workers are the first points of contact for individuals seeking to address their concerns. Primary care services include family medicine, internal medicine, pediatric care, and obstetrics and gynecology. This level of care does not require patients to be referred elsewhere. The next level is secondary care, in which specialists in dedicated clinics provide services. Secondary care clinics include cardiology, oncology, urology, pulmonology, and neurology clinics. Mental health care workers, although not necessarily requiring referrals, are also included in this level of care. The final level is tertiary care, in which highly specialized services are offered to treat referred patients. These services range from cardiovascular interventions to dialysis treatments (Gellman, 2020). Research on the impact of extensive work experience as either a risk or a protective factor for mental health has yielded mixed conclusions. According to Luo et al. (2020), less work experience correlates with an increased likelihood of mental health issues. On the other hand, Alnazly et al. (2021) observed that employees who had more than 20 years of experience reported higher levels of stress, anxiety, and depression during the COVID-19 pandemic than those with fewer years of experience. Research on the prevalence of mental health challenges among workers in Kosovo is limited (Arenliu Qosaj et al., 2022; Gallopeni et al., 2020). However, no study has addressed the prevalence of stress, anxiety, and depression among HCWs in Kosovo post-COVID-19 pandemic. The healthcare system in Kosovo faces significant structural, organizational, and resource challenges that directly impact the mental well-being of healthcare workers. During the COVID-19 pandemic, several studies have documented a high prevalence of stress, anxiety, and depression among healthcare professionals in Kosovo, thus highlighting a high level of psychological vulnerability in this sector. For example, Arenliu Qosaj et al. (2022) reported that 71.6% of healthcare workers experienced mild to severe mental health burdens, with factors such as lack of physical exercise, poor health status, and burnout predicting higher levels of depression, anxiety, and stress. Gallopeni et al. (2020) identified significant symptoms of anxiety and depression in this professional group, while Hyseni et al. (2023) highlighted the impact of coping strategies and mental health on burnout rates. These findings highlight the urgent need for sustainable and tailored interventions to support the mental health of healthcare staff in Kosovo, not only in times of crisis but also in the daily conditions of the system.
The mental health of healthcare workers (HCWs) has long been a subject of global research, with stress, anxiety, and depression consistently identified as prevalent occupational health concerns (Anger et al., 2024; Maunder et al., 2024). Theoretical frameworks, such as the biopsychosocial model of illness (Kusnanto et al., 2018), the Job Demands Resources (JD-R) model (Bakker & Demerouti, 2007), and the Conservation of Resources theory (Hobfoll, 1989) offer valuable insights into how work-related stressors, resource availability, and individual coping capacities interact to influence mental health outcomes. These models emphasize that mental well-being is shaped not only by psychological and social demands but also by structural and systemic factors in the work environment. This theoretical grounding underscores the necessity of examining these variables in diverse healthcare contexts, including under-researched regions such as Kosovo, where systemic challenges, such as limited infrastructure, high patient-to-staff ratios, and resource constraints, may exacerbate psychological strain among HCWs (Ademi Osmani et al., 2017). Understanding these dynamics within the local healthcare system is, therefore, essential for designing targeted evidence-based interventions that promote mental health and occupational well-being.
The international literature suggests that emergency service workers often face higher workloads, a more intense pace, and more frequent exposure to critical situations and trauma, which can significantly impact their mental well-being (Chirico et al., 2021). In Kosovo, there is limited data on studies that specifically address this comparison between emergency workers and other health professionals. The inclusion of this dimension in our study makes an important contribution to a better understanding of differences in occupational risks and identifying the need for interventions tailored to the type of health service.
Therefore, this study aimed to assess the prevalence of anxiety, stress, and depression among healthcare workers. This study specifically aimed to evaluate the prevalence of stress, anxiety, and depression within the healthcare workforce and to compare these mental health issues between those working in emergency departments and other healthcare professionals.
This study is crucial for healthcare workers’ well-being, patient safety, care quality, and the overall functioning of healthcare systems, as it provides valuable data to inform policies regarding interventions in the healthcare system, thereby enabling more professional delivery of health services. Interventions in workplaces that are more urgent in terms of need will directly affect workers in these environments, thereby enhancing the overall functionality of hospital services.
Theoretical Framework
The biopsychosocial (BPS) model is based on the general systems theory. Each system is structured with corresponding interdependent levels that function within a linear hierarchy (Fava & Sonino, 2008). The BPS model comprises of biological, psychological, and social systems. However, Engel does not explicitly delineate the boundaries between these systems or specify when one begins and the other ends; he emphasizes their interactivity (Engel, 1980). This model aims to explain a patient’s health condition, which may be caused by genetic disorders (biological factors), personality traits (psychological factors) or economic status (social factors). The mechanisms of coping with stress and depression and their associated health outcomes (Chuang et al., 2008; Di Benedetto et al., 2009). This underscores the significance of psychological factors in influencing the biological factors that are likely to be sustained by social factors.
Considering these systems and all the factors that interfere with HCWs’ work, we can identify the triggers that may eventually destabilize their well-being. Due to the nature of their work and continuous exposure to patients with various challenges, issues of mental health, and different biological predispositions as interdependent factors, HCWs are at a high risk of having biological factors that influence psychological factors, which are further sustained by social factors. Therefore, this study employed the BPS model to examine the mental health of the HCWs.
Literature Review
Prevalence of Stress
According to Lazarus and Folkman's transactional model of stress and coping, stress is understood as an emotional and physiological response that arises when perceived demands exceed an individual's available coping resources (Biggs et al., 2017). In occupational settings, stress may be triggered by both internal and external factors. Internal factors relate to how individuals perceive, appraise, and interpret situational demands, whereas external factors stem from workplace organization, workload intensity, managerial structures, and job-related insecurity (Panigrahi, 2016). More specifically, elements such as job insecurity, long working hours, lack of autonomy, and managerial style have been identified as significant contributors to elevated stress levels (Stansfeld & Candy, 2006). Although healthcare professionals often operate under substantial pressure, evidence shows that stress symptoms do not manifest uniformly across occupational groups, as the impact of stressors is shaped by individual, interpersonal, and organizational dynamics (Stansfeld & Candy, 2006). Nevertheless, the prevalence of stress among these workers has also increased. In a systematic review and meta-analysis, Al Maqbali et al. (2021) reported that the mean prevalence of stress among nurses during the COVID-19 pandemic was 44%. High levels of stress among healthcare workers (HCWs) can lead to reduced interest in patient care, increased negative attitudes towards the workplace, and emotional exhaustion. Over time, this may contribute to a higher likelihood of professional errors, suboptimal use or damage of equipment, and greater patient dissatisfaction, ultimately undermining the quality and safety of care. The COVID-19 pandemic has put immense pressure on health care workers worldwide. Lai et al. (2020) reported high levels of stress, anxiety, and depression among healthcare workers in China during the first few months of the pandemic. According to Moccia et al. (2020), frontline employees experience severe psychological distress. Increased workload, fear of viral infection, and high patient suffering and death have intensified existing challenges. The prevalence of stress has significantly increased during the global pandemic. The COVID-19 pandemic has caused a notable increase in stress across various countries. In Saudi Arabia, Serbia, India, Australia, China, Canada, and Iran, stress prevalence rates were found to be 38% (Al-Hanawi et al., 2020), 40% (Antonijevic et al., 2020), 33% (Chatterjee et al., 2020), 21% (Holton et al., 2020), 72% (Lai et al., 2020), 76% (Mrklas et al., 2020), and 84% (Pouralizadeh et al., 2020) respectively. A meta-analysis by Saragih et al. (2021) revealed that 35% of key personnel (KPs) experienced distress. Numerous studies have reported serious mental health findings throughout the pandemic, including those of health workers in Iran. Maleki et al. (2021). In Kosovo, during the COVID-19 pandemic, Ukëhaxhaj et al. (2022) reported that 32.4% of the population experienced moderate stress, while 11.3% faced severe stress levels. Meanwhile, According to Arenliu Qosaj (2022), the prevalence of stress is 21.9%, where 10% is mild, 11.6% moderate, 6% severe, and 4% extremely severe.
Prevalence of Anxiety
Healthcare services are associated with challenges that make the work of healthcare workers more challenging. Difficulties such as inadequate staff, insufficient resources, and long working hours may negatively affect the productivity, work, and health of healthcare workers themselves (Gao et al., 2012). When the health of KP itself is mentioned, the literature indicates that both the physical and mental health of KP should be researched by different authors to understand the prevalence of disorders present in these employees before and during the COVID-19 pandemic. Anxiety is one such disorder (Chen et al., 2022; Osasona & Oderinde, 2023; Shamsan et al., 2022). Ahmed & Alkhamis (2009) described anxiety as a state that encompasses physiological and psychological aspects, including cognitive, somatic, emotional, and behavioral elements. According to a report by the World Health Organization (2017), the global prevalence of anxiety disorders is 3.6%, with anxiety symptoms reported in 38% of rimary care nurses (PNs) in China, as found by Ding et al. (2014).
Anxiety affects quality of life in NPHS (Maunder et al., 2024) and relationships with colleagues or patients (Ruitenburg et al., 2012; Sun et al., 2012). The factors that cause anxiety in these workers are workplace stress (DiGiacomo & Adamson, 2001; Sun et al., 2012), high commitment, long hours, time pressure (Mark & Smith, 2012), younger age, and female (Mosolova et al., 2021). Anxiety disorders are associated with negative consequences such as a lack of functional capacity, substance abuse, and addiction. In contrast, other factors related to anxiety disorders are social, family, financial, interpersonal, and professional (Pereira-Lima et al., 2019). Yang et al. (2017) investigated the influence of sociodemographic factors on anxiety among doctors, pharmacists, and nurses. About one-third of the participants indicated that they experienced extremely severe anxiety, whereas general anxiety levels were found to be moderate. The authors found no correlation with sociodemographic factors such as faith, race, age, sex, hours of sleep, experience, and results. However, other authors have reported characteristics related to the level of anxiety, such as sex, age, type of workplace, and the number of cases managed with COVID-19: being a woman, being under the age of 30, working in specialized hospitals, and managing a higher number of COVID-19 cases were predisposed to the prevalence of anxiety (Shamsan et al., 2022). Chen et al. (2022) conducted a meta-analysis and found that anxiety is more prevalent among women, married people, parents, and nurses.
A study conducted in Nepal aimed to analyze mental health problems because of the COVID-19 pandemic, including depression, anxiety and stress among frontline junior resident doctors, as according to the authors these doctors are some of the healthcare professionals who are sensitive to mental health concerns. This study concluded that anxiety was the most common in the sample (50%), with a moderate level of anxiety being the most pronounced. These conclusions are supported by those of other studies (Chew et al., 2020; González-Sanguino et al., 2020; Huang et al., 2020; Luo et al., 2020). Studies have shown serious mental health issues during the pandemic. Motahedi et al. (2021) conducted a cross-sectional study to assess the level of anxiety and depression among healthcare workers in a COVID-19 referral hospital in Iran, including clinical, administrative, and cleaning staff. The results showed that the mean anxiety score were 6.64 (SD = 4.86) and depression 18.21 (SD = 10.59), with a direct and significant relationship between them (p < .001). Depending on coping with episodes of anxiety, stress, and depression, many CPs continue to work and practice their profession; however, after experiencing such episodes, others show harsher negative consequences, such as suicidal thoughts, endangered well-being in the long term, and a lack of sleep (Joshi et al., 2021; Kiliç et al., 2021; Mattila et al., 2021). Continuous work without identifying the needs of NPSH while experiencing anxiety can result in psychiatric illnesses, burnout, job dissatisfaction, and job resignation (Alharthy et al., 2017). High levels of anxiety, depression, and stress are associated with denial of problems, non-acceptance, escape from stress, and increased use of alcohol and drugs in patients with NPSH. The high-profile mental health problems continuously identified by studies also affect the reduction in the efficiency of cognitive functions, the reduction in quality of work, and the relationships that NPHS have with their patients (Maharaj et al., 2019).
Prevalence of Depression
Depression is another important mental health concern in the healthcare workforce, with potential consequences for both individual well-being and the quality of patient care. Several recent studies have examined the prevalence of depression among healthcare professionals, highlighting its complexities. A study conducted in France by Fond et al. (2022) aimed to determine the rate of clinical depression in a sample of healthcare workers during the post-COVID-19 period. Using structural equation modeling, we recruited 10,325 participants from various national healthcare institutions. The findings indicated that 30.2% of the respondents met the potential diagnostic criteria for clinical depression, highlighting the significant prevalence of this problem among healthcare workers. In addition, the study also identified some of the factors that contribute to depression, emphasizing the important influence of professional factors, including professional burnout (“burnout”), constant harassment in the workplace, and a lack of decision-making freedom, as well as individual factors, especially recurrent major depression. In another publication, a meta-analysis and systematic review by Abraham et al. (2021) focused on healthcare workers in the Eastern Mediterranean Region synthesized data from 108 studies in 12 countries and found that being a woman, working long hours, and poor sleep quality were identified as depression risk factors. The meta-analysis, which included 77 studies, found that 33.03% of healthcare workers in the Eastern Mediterranean Region experienced depression, with emergency healthcare workers exhibiting notably higher rates. Angerer et al. (2017) explored the influence of night shift work on the risk of depression. This systematic review included 11 longitudinal studies that demonstrated various associations between night-shift work and depression. Although studies within health professions did not reveal a consistent link between these variables, research on non-health care professionals indicated a higher risk of depression associated with several years of night-shift work. Another systematic review and comprehensive meta-analysis conducted by Marvaldi et al. (2021) assessed the mental health status of health care workers during the COVID-19 pandemic. This review included 70 studies involving over 100,000 participants and consequently showed a significant prevalence of depression (31.1%) among healthcare workers. The study conducted by Deng et al. (2021) also provided important findings. Similar findings regarding depression during the pandemic have been observed among healthcare workers in Iran (Motahedi et al., 2021). During the COVID-19 pandemic in China, the prevalence of depression and anxiety among the general population and healthcare workers was assessed. These findings indicate higher levels of depression and anxiety among healthcare workers than the general public, with healthcare workers experiencing prevalence rates of 31% for depression and 40% for anxiety. A comparative analysis showed that healthcare workers had higher rates of depression (40%) and anxiety (38%) than the public before the peak of the pandemic (depression, 33%; anxiety, 24%). After the peak of the pandemic, the prevalence of these issues among healthcare workers declined, whereas it increased among the general public.
Risk Factors for the Development of Stress, Anxiety, and Depression in Healthcare Workers
Studies conducted before and during the COVID-19 pandemic have identified several risk factors for depression, stress, and anxiety among healthcare workers. Consistently, high workloads and challenging job roles have been recognized as major sources of stress (Terry, 2020). Additionally, inadequate organizational support and resources exacerbate mental health challenges for healthcare professionals (Johnson et al., 2018). Exposure to traumatic events, a widespread concern in healthcare settings, is associated with high stress and anxiety (d’Ettorre & Pellicani, 2017). The unique circumstances of the COVID-19 pandemic have intensified risk factors. For example, studies during the pandemic have highlighted the additional burden faced by frontline workers, who experience higher levels of worry, depression, and anxiety than their counterparts (Thu Pham et al., 2023). Shift work during the pandemic and direct care of patients with COVID-19 have also emerged as significant risk factors for mental health issues among healthcare workers (Thu Pham et al., 2023). In addition, pre-existing mental health conditions such as a history of anxiety or depression may increase vulnerability to negative mental health outcomes (Pappa et al., 2020).
Consequences of Stress, Anxiety, and Depression in Healthcare Workers
Depending on how they cope with episodes of anxiety, stress, and depression, PNs continue to work and practice their profession, but others, after experiencing such episodes, show more severe negative consequences, such as suicidal thoughts, endangered well-being in the long-term future, and lack of sleep (Mattila et al., 2021). Continuous work without identifying the needs of PWD while experiencing anxiety can result in psychiatric illnesses, burnout, job dissatisfaction, and job resignation (Alharthy et al. 2017). High levels of anxiety, depression, and stress are associated with denial of problems, non-acceptance, escape from stress, and increased alcohol and drug among KPK (Budzyriska & Morys, 2023). These mental health problems also reduce the efficiency of cognitive function, reduce the quality of work, and affect the relationships that NPs have with their patients (Maharaj et al., 2019).
Present Study
Previous research has extensively documented the prevalence of stress, anxiety, and depression among healthcare workers worldwide, as well as the occupational and contextual factors influencing these mental health outcomes (Arenliu Qosaj et al., 2022; Chirico et al., 2021; Gallopeni et al., 2020). However, there is a lack of empirical data addressing these issues within the specific context of Kosovo, particularly when comparing emergency department staff to other healthcare professionals. Understanding the prevalence and patterns of these conditions in the local context is crucial for developing targeted interventions and policy responses.
Building on the gaps identified in the literature, this study aims to address the following research questions:
What is the prevalence of stress among healthcare workers?
What is the prevalence of anxiety among healthcare workers?
What is the prevalence of depression among healthcare workers?
What are the differences in the prevalence rates of depression, anxiety, and stress among healthcare workers in emergency departments and other healthcare professionals?
Methods
Participants
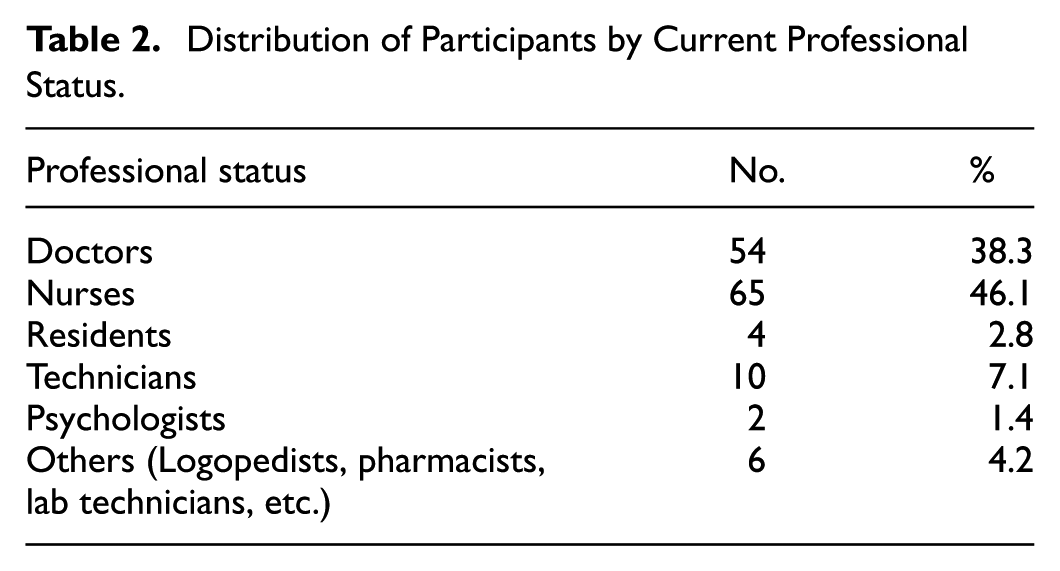
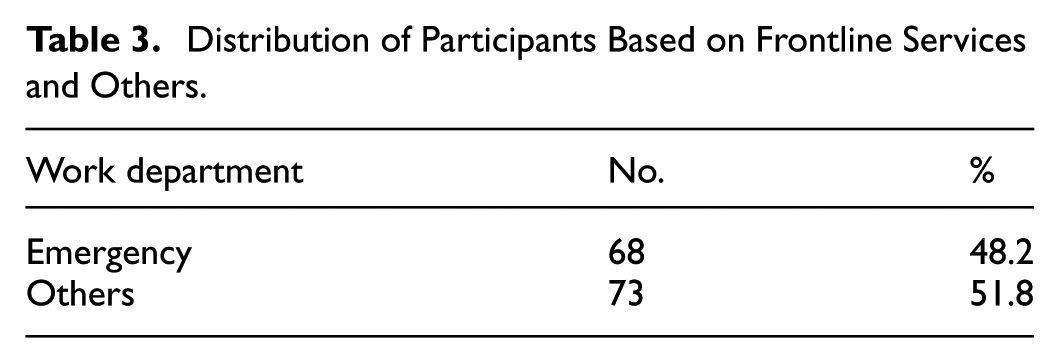
Sample consisted of 141 healthcare workers in Kosovo aged 19 to 65 years (M = 38.5, SD = 12.14). Of these, 67.4% were women and 32.6% were men. Of the total participants, 80.9% lived in urban settlements, and 19.1% lived in rural settlements. Their level of education was higher, with more than half of the sample in bachelor’s degree studies (51.1%), continuing with specialization (30.5%), postgraduate doctoral studies (10.6%), 3.5% of them had started university studies but had not completed them, and 4.3% of them had secondary education. Their experience ranged from less than 5 years (28.4%) to 5 years (11.3%), 5 to 10 years (18.4%), 10 to 15 years (15.6%), 15 to 20 years (9.9%), and >20 years (16.3%). The dominant professional status of the participants was 46.1% of the role of the nurse as a healthcare worker; 38.3% presented the role of the doctor to continue, with a lower presence of other professionals, such as pharmacists, physiotherapists, cardiologists, psychologists, and others. 48.2 Of the participants, 48.2% were identified as part of the emergency services, while the rest (51.8%) were reported to be workers in other healthcare departments (e.g., neurology, rheumatology, radiology, internal medicine). Our study included
Instrument
The instrument used for data collection was the DASS-21 (Lovibond & Lovibond, 1995). This scale has a total of 21 items, and various studies have shown high reliability values for this scale; its special feature is that it measures symptoms of three emotional states and that it has managed to be administered in different countries and cultures of the world. Participants were asked to respond based on their experiences over the past week using a scale from 0 (not at all applicable) to 3 (very much applicable or most of the time). The internal consistency of the scale in the Albanian version had a Cronbach’s alpha of .94. The measuring scale included seven items for measuring stress, where a model item of this dimension would be: “I had difficulty calming down because something had bothered me,” seven items for measuring anxiety, where a model item of this dimension would be: “I had difficulty breathing (e.g., breathing very fast or feeling like I can’t breathe properly even without physical activities),” while for measuring depression fit the items of the dimension, a model item would be: “I was not able to experience any positive feeling” that I have nothing to be happy about.”
Procedures and Data Analysis
This study employed a quantitative survey method to assess the prevalence of stress, anxiety, and depression in healthcare workers. Data were collected using the DASS-21 questionnaire (Lovibond & Lovibond, 1995), administered both online and in person over a three-week period, with an average completion time of 3 to 5 min. The survey gathered demographic details such as age, residence, job position, and work experience to provide a comprehensive analysis.
Descriptive statistics were used to summarize the participants’ demographic data and the prevalence of stress, anxiety, and depression. The Shapiro-Wilk test was applied to assess the distribution of the data, which indicated a non-normal distribution of the data for the main outcome variables. Consequently, the non-parametric Mann–Whitney U test was used to compare the levels of depression, anxiety, and stress between the two independent groups (emergency care workers and workers from other departments). This test was chosen because of its suitability for data that did not follow a normal distribution and for independent groups.
Ethical Considerations
Participation in the study was voluntary. Before completing the questionnaire, the participants were presented with a consent form indicating that confidentiality would be maintained, there would be no possibility of identification, and that the data would be used only for the purposes of this study. This study was approved by the relevant Ethics Committee of a public university and was authorized by a major University Clinical Center.
Written and verbal consent was obtained from all participants prior to their involvement in the study to ensure ethical compliance and respect for their autonomy. Confidentiality and anonymity will be protected, and data will be stored securely, accessible only to the research team.
Results
Based on the data collected to describe the demographic aspects of the research in more detail, Table 1 presents the data in question. The distribution of participants in professional status is shown in Table 2, whereas the distribution of participants in emergency healthcare workers and other departments is shown in Table 3.
Demographic Data.

Note. Sample size = 141, SD = Standard Deviation.
Distribution of Participants by Current Professional Status.
Distribution of Participants Based on Frontline Services and Others.
The reported prevalence of depression among healthcare workers was as follows: 39.7% were classified as having a normal level of depression, 16.3% experienced mild depression, 27% had moderate depression, 7.8% had severe depression, and 9.2% were at had very severe depression (see Table 4). For the 141 healthcare worker participants, the prevalence of anxiety was reported to be 35.5% at the normal level, 6.4% at a mild level of anxiety, 19.9% at a moderate level, 12.1% at a severe level of anxiety, and 26.2% at the participants reported a very severe level of anxiety (Table 4). The results regarding the prevalence of stress levels among healthcare workers were reported to start from 14.9% at a mild level of stress, to continue with 13.5% at a moderate level, 12.1% at a severe level, and 7.1% at a level of severe stress; correspondingly, more than half of the participants (52.5 %) reported normal levels of stress (Table 4).
Prevalence of Depression, Anxiety, and Stress Among Healthcare Workers.

Different levels of depression, stress, and anxiety in healthcare workers have been reported in frontline workers (emergency) and others. Among participants, 29.4% of emergency workers reported normal levels of depression, 11.8% reported mild, 30.9% reported moderate, 10.3% reported severe, and 17.6% reported very severe depression. In contrast, other healthcare workers showed a different distribution of depression levels. The study found that 49.3% of participants exhibited normal levels of depression, while 20.5% experienced mild depression, 23.3% had moderate depression, 5.5% were classified as having severe depression, and 1.4% fell into the very severe depression category (Table 5).
Prevalence of Depression, Anxiety, and Stress in Groups.

Note. No = Number of employees; Pr = Prevalence.
Emergency workers reported a higher prevalence of anxiety at a very severe level (42.6%) than other workers with lower levels of severe anxiety (11%). Other workers reported greater levels of anxiety, with 8.2% experiencing mild anxiety, 26% moderate anxiety, and 17.8% severe anxiety, compared to emergency workers who reported 4.4%, 13.2%, and 5.9% for mild, moderate, and severe anxiety, respectively (Table 5).
The prevalence of stress at very severe, moderate, and light levels was higher among emergency workers (severe level, 11.8%; moderate and light levels, 17.6% each) than among other workers at the corresponding levels (very severe, 2.7%; moderate, 9.6%; and mild, 12.3%). Opposite results were reported for severity, with other workers reporting higher levels of severe stress (13.7%) than emergency workers (10.3%; Table 5).
After analyses for normality distribution, according to which the results reported deviation from the normality distribution, the Mann-Whitney U analysis was used to compare the levels of depression, anxiety, and stress among the PNs in emergency departments versus those in other departments. The analysis revealed significant differences between healthcare workers in emergency departments and those in other areas for each variable (depression, anxiety, and stress). A negative Z-value suggested that emergency department staff generally ranked lower, indicating higher levels of depression, anxiety, and stress. The significance values for depression (p = .000), anxiety (p = .027), and stress (p = .022) confirm that these differences are unlikely to be due to chance (Table 6).
Mann–Whitney U Analysis.

Discussion
The main aim of this study was to assess the prevalence of depression, anxiety, and stress among health workers in the public sector of Kosovo, with a particular focus on identifying the differences between those working in emergency departments and their colleagues in other health services. In this way, the study aimed to provide evidence-based evidence that can guide the development of interventions and work policies tailored to the specific needs of these professional groups. The findings showed that 60.3% of participants reported mild to very severe symptoms of depression, 64.5% reported symptoms of anxiety, and 31.6% reported mild to severe symptoms of stress. These rates are significantly high and consistent with the findings of international studies documenting increased levels of psychological distress among health workers working in conditions with high demands and limited resources (d’Ettorre & Pellicani, 2017; Johnson et al., 2018; Terry, 2020). In comparison with the findings of the study by Arenliu Qosaj et al. (2022), who also reported worrying levels of prevalence of the factors, the study findings suggest the continued vulnerability of this group, particularly for those working on the frontlines in emergency services, and reinforce the need for consistent monitoring and mental health support strategies tailored to the public health sector. The post-pandemic period in Kosovo may have been particularly challenging due to the accumulation of clinical overload from care delays, ongoing staff shortages (e.g., movement of personnel to the private sector or abroad), increased work intensity and more complex clinical cases, and a systematic lack of psychological support in the workplace. These chronic factors may explain why anxiety and depression appear higher now than in the early stages of the pandemic (Arenliu-Qosaj), while, while acute immediate stress dominated, long-term effects have become more evident in the results of the current study. It is also expected that acute stress was higher in the early stages of the pandemic, while anxiety/depression may remain/increase subsequently as a result of prolonged work stressors and social/economic insecurities (Maleki et al., 2021).
Furthermore, the study by Gallopeni et al. (2020), despite the differences in measurement, shows a percentage that is also significantly different, where 91.1% of participants reported the presence of mild to severe depressive symptoms and 91.7% reported symptoms of anxiety (Gallopeni et al., 2020). These rates, along with the current study’s rates of depression, anxiety, and stress, are not significantly different from those reported in Pakistan (Sandesh et al., 2020), Singapore (50%; Chew et al., 2020), and various European countries (Hummel et al., 2021). However, studies assessing the mental health of healthcare professionals after the pandemic, although few in number, point to poor mental health in healthcare workers (Grünheid & Hazem, 2023) since the pandemic COVID-19 was declared to be past only, thus not yet reflected in detailed studies of mental health in this population. These findings align with the study’s expectation that this group would exhibit a high prevalence of depression, anxiety, and stress. Additionally, the thesis is supported by the observed differences in these mental health dimensions between healthcare workers in emergency departments and those who do not. The current findings indicate notable differences in the levels of depression (p = .000; p < .005), anxiety (p = .022; p < .005), and stress (p = .027; p < .005), with statistically significant results seeking closer attention. These differences align with findings from comparable studies conducted globally, which show a concerning prevalence of mental health issues among this subgroup, particularly when compared to other healthcare worker groups (Hendrickson et al., 2022; Kumar et al., 2021; Wong et al., 2021; empirical insights drawn, including prevalence and predicted and reported discrepancies between those employed in emergency departments and those in other departments, using evidence from various studies and reports, can be attributed to the stressors of high job demands and challenging work roles (Terry, 2020), insufficient organizational support and limited resources in healthcare settings (Johnson et al., 2018), exposure to traumatic events (d’Ettorre & Pellicani, 2017), health emergencies, such as that of COVID-19 (Thu Pham et al., 2023) or pre-existing mental health conditions (Pappa et al., 2020). The results of the present study are consistent with those of previous research addressing the mental health difficulties encountered by healthcare professionals worldwide. These elevated prevalence rates highlight the urgent need to implement supportive mental health interventions specifically designed to meet the unique needs of health care workers.
This study makes an important contribution to the scientific literature not only by reporting the alarming prevalence rates of depression, anxiety, and stress among healthcare workers in Kosovo but also by highlighting a distinctive dimension: the significant differences between those working in emergency services and their counterparts in other healthcare sectors. These results not only confirm international findings on the high psychological risk of this professional group, but also provide empirically based data from the local context, where social, economic, and institutional factors in the post–COVID-19 period play a specific role. By including a focused analysis of differences by type of healthcare service, this study advances a deeper understanding of stress sources and the varying need for intervention, offering a clear basis for the development of tailored policies and support programs for healthcare workers in Kosovo. This includes addressing job demands, increasing physical and psychological safety, ensuring the availability of easily accessible mental health resources within healthcare institutions, and conducting further research on the individual mental health needs of these groups.
This study contributes to the growing body of research on the mental health of healthcare workers by providing context-specific data from Kosovo, a country in which empirical evidence in this area remains scarce. By focusing on the prevalence of depression, anxiety, and stress among healthcare workers, particularly those working in emergency departments, this study highlights a vulnerable group within the healthcare system that requires targeted attention. The use of the DASS-21 instrument and the inclusion of participants from both urban and rural areas provided a broader understanding of the mental health challenges faced by healthcare workers in transitional healthcare settings. These findings provide a valuable basis for future research and inform public health strategies aimed at supporting the psychological well-being of medical staff in under-researched contexts.
The findings of this study can be more fully understood in light of the Biopsychosocial Model (BPS), which provides an integrated approach to explaining the factors that influence the mental health of healthcare workers. The biological component is reflected in the higher levels of stress, anxiety, and depression symptoms in emergency service workers who face constant exposure to physical fatigue and immediate risks. The psychological aspect is evidenced by a high level of emotional symptoms, especially in professionals with less experience or without structured psychological support. Social factors such as the lack of institutional support structures and unequal burden sharing in the Kosovo healthcare system also contribute to the deterioration of workers’ well-being. This integration highlights the need for integrated interventions that address not only individual symptoms, but also systemic conditions that contribute to professional burnout (Kusnanto et al., 2018).
Limitations
Despite these significant empirical findings, this study has several limitations specific to its design and context. First, the relatively small sample size considerably limits the statistical power and representativeness of the findings. In addition, the use of a cross-sectional survey conducted within a restricted two-month timeframe meant that the observed associations between workplace setting and mental health indicators (depression, anxiety, and stress) could not establish temporal or causal relationships. A longitudinal follow-up of the same participants would allow tracking of changes over time and better identification of cause–effect dynamics.
Second, the recruitment strategy was limited to public healthcare institutions in Kosovo, which while appropriate for the study’s aims, may not capture the experiences of healthcare professionals in private or mixed systems. This limits the generalizability of the results beyond similar public health care contexts. Third, data collection relied on a self-administered questionnaire (DASS-21), which, although widely validated and previously standardized in Kosovo (Arenliu Qosaj et al., 2022), captures self-reported symptoms and is subject to recall bias and social desirability effects. Additionally, using a single measurement tool may not fully reflect the complexity of mental health status, particularly in high-stress occupational groups.
Finally, this study did not assess coping mechanisms, access to psychological support, or workplace resource availability, all of which may moderate or exacerbate mental health challenges. Future research incorporating these factors and using a mixed-methods approach could provide a more comprehensive and nuanced understanding of health care workers’ mental health in post-pandemic Kosovo.
Practical Recommendations and Future Directions
Based on the findings of this study, concrete recommendations can help improve the mental well-being of healthcare workers in Kosovo and provide clear directions for future research.
Given that emergency service workers have reported significantly higher levels of depression, anxiety, and stress, health institutions should develop programs specifically dedicated to this group. These programs could include rotating schedules to reduce workload, stress management training, and regular protocols for discussion and processing after critical situations (Anger et al., 2024; Maunder et al., 2024). Another necessary measure is the integration of mental health services in the workplace. Incorporating periodic screenings, for example every 6 months, with validated instruments such as the DASS-21, providing psychological counseling within institutions, and creating confidential channels for reporting mental health concerns would help in the early identification of risk and timely intervention. Institutional leaders should also undertake policies that strengthen the physical and psychological safety of employees, including providing the necessary protective equipment and equitable division of workloads between departments. Studies suggest that fostering a creative work environment can contribute to increasing job satisfaction and overall well-being of healthcare staff (Gholami et al., 2025).
Another key element is the development of mandatory training modules for all health care workers to identify and manage symptoms of stress, anxiety, and depression, including practical self-care strategies. Finally, given the significant differences between subgroups of healthcare professionals, future research should focus on identifying specific risk and protective factors for each group (e.g., nurses, doctors, and technical workers). Longitudinal studies would help to understand changes in mental health after the pandemic and during periods of health crisis (Anger et al., 2024).
These recommendations, grounded directly in the study’s results, have the potential to foster a healthier work environment, enhancing not only employee well-being but also the overall quality of healthcare services.
Footnotes
Consent to Participate
Informed consent was obtained from all participants involved in the study.
Author Contributions
Liridona Jemini Gashi: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Validation; Supervision; Visualization; Writing—original draft; Writing—review & editing; Dardana Fetahu: Conceptualization; Data curation; Formal analysis; Investigation; Project administration; Validation; Visualization; Writing—review & editing; Arta Rexhepi: Conceptualization; Data curation; Formal analysis; Validation; Visualization; Writing—original draft; Resources; Diona Visoka: Conceptualization; Data curation; Formal analysis; Validation; Visualization; Writing—original draft; Resources; Veronë Perçuku: Conceptualization; Data curation; Formal analysis; Validation; Visualization; Writing—original draft; Resources.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee on Research, Faculty of Philosophy.