
Abstract
Healthcare workers have been a vulnerable group during the pandemic. Even today, they continue to deal with the virus and its consequences. Such sustained stress over time has led to the development of mental health problems that may still be present in this population. These may be related to the coping strategies that are being implemented to manage this situation. This study aimed to examine the mental health of health professionals after the end of the acute phase of the pandemic and investigate which coping strategies predicted levels of stress, anxiety, depression, and burnout. A total of 285 healthcare workers were assessed. Descriptive and multiple regression analyses were performed. The result showed (a) levels of mild-to-moderate depressive symptomatology, moderate levels of stress and anxiety symptomatology, and a medium level of burnout; and (b) acceptance, behavioral disengagement, negation, substance use, and active coping as the strategies most implicated in this symptomatology. Interventions that help health professionals to develop adaptive coping strategies, thus avoiding or reducing the development of psychological symptoms, should be implemented.
The sociosanitary situation caused by COVID-19 has affected the mental health of the entire population to the point where it may have worsened compared with before the pandemic began (Daly et al., 2021; McGinty et al., 2020). Healthcare workers are a particularly vulnerable group. They have been placed in high-risk situations through continuous contact with the infected and they have had a high workload in situations of scarce resources; they have also been concerned about having contact with family members and they have lost patients, friends, and so on (Dong & Bouey, 2020). In fact, 70% and 25% of healthcare workers perceived medium and high risk of being infected, and the workplace response to COVID-19 was inadequate (Aram et al., 2022; Le et al., 2021). They experienced high levels of mental distress compared with the general population (Hassannia et al., 2021) .
Although the social and health situation has improved, the significant impact of the COVID-19 pandemic on the psychological well-being of healthcare workers (Hill et al., 2022), has been revealed in the form of fatigue, stress, anxiety, and depressive symptoms, among others (Kang et al., 2020). Li et al. (2021), in a meta-analysis involving 97,333 healthcare workers across 21 countries, found a high prevalence of moderate depression (21.7%) and anxiety (22.1%) in this population, a result that was consistent with other studies (e.g., Muller et al., 2020; Tan et al., 2023), founding that this symptomatology had significantly associated with the manifestation of physical symptoms as headache (Chew et al., 2020).
Equally, high stress levels (25.9%) were found, and a moderate/severe prevalence of burnout was experienced by healthcare workers (Luceño-Moreno et al., 2020, 2022; Tan et al., 2023). During the COVID-19 pandemic, a meta-analysis showed an incidence of burnout of 52% among all healthcare workers, including physicians and nurses (Ghahramani et al., 2021) or frontline workers and second-line employees (Macaron et al., 2023). Specifically, of the three components of burnout syndrome, low personal accomplishment was found in 31.18% of the people, followed by emotional exhaustion (22.06%) and depersonalization (8.72%) (Parandeh et al., 2022). These data confirmation that the impact of COVID pandemic was notable in this population.
Studies have shown that the management of stressful or traumatic situations depends on individual variables. Coping is a process of managing the external or internal demands that exceed the resources of the individual (Lazarus & Folkman, 1984). Some individuals adapt to situations functionally and others do not, and coping strategies are a key variable (Carver, 2011). Depending on the nature of the stressful situation and its consequences, particular coping strategies may be more effective than others. They may be adaptive, thereby limiting the impact of a stressful situation, or maladaptive, resulting in distress and negative psychological symptoms (Holahan & Moos, 1987).
Gan et al. (2004) found that the individuals implemented fewer active (problem-focused) strategies and more avoidable (emotion-focused) coping strategies in reaction to previous pandemics. Main et al. (2011) concluded that coping was a central mechanism against the adverse influence of stressors on perceived health. Negative coping was associated with stress, depression, and anxiety in general when COVID-19 emerged (e.g., Wang et al., 2020). Meanwhile positive thinking, active coping strategies for stress and social support were found to be positive predictors of a higher quality of psychological life and well-being and negative predictors of perceived stress, depression, and anxiety (Budimiret al., 2021). Some studies have concluded that healthy (i.e., positive) expressions of emotions or yoga/meditation can be adaptative strategies (e.g., Bhattacharjee & Acharya, 2020).
Studies examining these strategies in the daily work of health professionals have found that adaptative coping strategies are associated with fewer anxiety and depression symptoms and higher mental well-being, job success, and social cohesion (e.g., Mohr et al., 2014). A systematic review of the impact of disasters on the mental health of medical responders showed that poor social support and communication and maladaptive coping could be risk factors for the development of mental health problems among healthcare workers (Naushad et al., 2019).
However, knowledge of coping strategies in healthcare workers in acutely stressful situations such as a pandemic is limited. Smallwood et al. (2021) found that the most widely reported strategies were exercise (44.9%), social connections (31.7%), and alcohol use (26.3%). Marcolongo et al. (2021) observed that some healthcare workers used acceptance, planning, and active coping. Finally, in a Turkish study, Cansız et al. (2021) concluded that accepting support, engaging in adaptive coping, and reducing self-distraction predicted lower anxiety symptoms.
In sum, the importance of coping strategies in managing stressful situations and their relationship with the mental health of the population, including healthcare personnel, has been widely demonstrated. However, to the best of our knowledge, research in this area during the COVID-19 pandemic and the post-pandemic period is limited. In light of the fact that the pandemic is ongoing and that health professionals continue to face it, the present study aimed to (a) analyze, after the end of the acute phase of the pandemic, the mental health (levels of stress, anxiety, depression, and burnout) of health professionals and (b) examine which coping strategies predicted levels of stress, anxiety, depression, and burnout. More knowledge regarding the coping strategies employed (including those that were more adaptive for the population in question) in this particular situation is needed if evidence-based interventions that mitigate psychological problems during present and future crises are to be developed.
Method
Participants and Procedure
A total of 285 healthcare workers were assessed. The sample comprised 249 women (86.9%) and 36 men (13.1%) with a mean age of 38.09 (11.56). The participants completed an online survey developed using Google Forms. A random sample of 35 national public health service hospitals was invited to share the survey link with their healthcare workers (physicians, nurses, and other service personnel) through institutional mail (four of them did not accept the proposal). Workers interested in participating voluntarily accessed the link and were not compensated for their participation.
The criteria for inclusion were that participants had to be health workers over the age of 18 years who had been working in hospitals during the pandemic (and at the time of interview). People with serious mental illness, who did not understand Spanish sufficiently, or who had difficulties completing the study online were excluded. The survey was conducted after the initial waves of the pandemic and after health personnel were completely immunized.
Participants were informed of the purpose of the study. This information and the consent form were presented on the first screen of the survey. All participants had to give their consent before continuing and completing the research protocol. The study conformed with the Declaration of Helsinki and received institutional review board approval at the Isabel I University (Spain).
Measures
Sociodemographic Variables
All participants were asked to provide information on age and sex.
Coping Strategies
Coping strategies were evaluated using the Spanish version of the brief COPE (COPE-28; Morán et al., 2010). This self-report comprises 28 items with a 4-point Likert scale from 1 (I haven’t been doing this at all) to 4 (I’ve been doing this a lot). Each of the 14 subscales comprises two items. These sub-scales are categorized into a second-order factor model (Meyer, 2001) that includes Adaptive coping strategies (use of emotional support, positive reframing, acceptance, religion, humor, active coping, planning, and use of instrumental support) and Maladaptive coping strategies (venting, negation, substance use, behavioral disengagement, self-distraction, and self-blame). In the sample, reliability (Cronbach’s alpha) was .60 for acceptance, .70 for venting and instrumental support, .72 for active coping, planning, and self-blame, .73 for positive reframing, .74 for self-distraction, .76 for behavioral disengagement, .77 for humor and negation, .78 for emotional support, 0.84 for religion, and .94 for substance use.
Depression, Anxiety, and Stress
Depression and anxiety symptomatology and stress were assessed using the Spanish version of Depression, Anxiety and Stress Scales (DASS-21; Bados et al., 2005). This self-report comprised 21 items that are evaluated with a 4-point Likert scale, from 0 (it has not happened to me) to 3 (it has happened to me a lot, or most of the time), to measure the severity/frequency with which the respondents have experienced each of the negative emotional symptoms during the previous week. In the present sample, Cronbach’s alpha was .93 for the depression sub-scale, .89 for the anxiety sub-scale, and .90 for the stress sub-scale.
Burnout
Burnout was assessed using the Spanish version of the Maslach Burnout Inventory (MBI; Seisdedos, 1997), a multidimensional inventory that assesses professionals’ feelings and attitudes toward their work and patients on a 7-point Likert scale ranging from 0 (never) to 6 (every day). This self-report consists of 22 items including three dimensions: emotional exhaustion, depersonalization, and personal accomplishment. In the present sample, Cronbach’s alpha was .93 for emotional exhaustion, .78 for depersonalization, and .78 for personal accomplishment.
Analysis
First, the assumptions of normality and homoscedasticity were confirmed, and descriptive statistics and Pearson correlation coefficients were calculated for each continuous variable. Correlations between variables did not indicate any associations greater than .90, a Durbin−Watson statistic greater than 4, or other problems associated with multicollinearity and/or homoscedasticity. The Student’s t test was used to analyze significant mean differences between men and women on all variables so this variable could be controlled for in subsequent analyses when necessary.
Next, a multiple regression analysis was performed for each variable (stress, anxiety, depression, and burnout). In Step 1, sex was entered as a control variable; Age was not used as a control variable since this variable did not show a statistically significant correlation with coping strategies and had a very low correlation with the symptomatology. Coping strategies were introduced in Step 2. Statistical analyses were conducted using the SPSS (Windows version 22.0, SPSS Inc., Chicago, IL).
Results
Table 1 shows the means, standard deviations, and correlations between the study variables. It is worth noting that the mean for depression was 6.25 (SD = 5.51), with 7 being the cut-off point for moderate depression. The mean for anxiety was 5.27 (SD = 4.95), with 5 being the cut-off point for moderate anxiety. The mean for stress was 9.60 (SD = 5.13), with 10 being the cut-off point for moderate stress.
Means, Standard Deviations, and Correlations of Study Variables.

Significant at the .01 level.
The mean of emotional exhaustion was 24.98 (SD = 13.25), with 19 being the cut-off point for moderate scores. The depersonalization mean was 6.70 (SD = 6.44), with 7+ being the cut-off point for moderate scores. Finally, the mean for personal accomplishment was 36.91 (SD = 6.98); the cut-off point for moderate scores was less than 39 and for low accomplishment, less than 33.
Table 2 shows the differences in symptomatology between sexes in each group (women vs. men). Depression, anxiety, and stress averages were significantly higher in females than in males. Women reported higher levels of emotional exhaustion than men.
Differences Between Sex in the Symptomatology Reported.
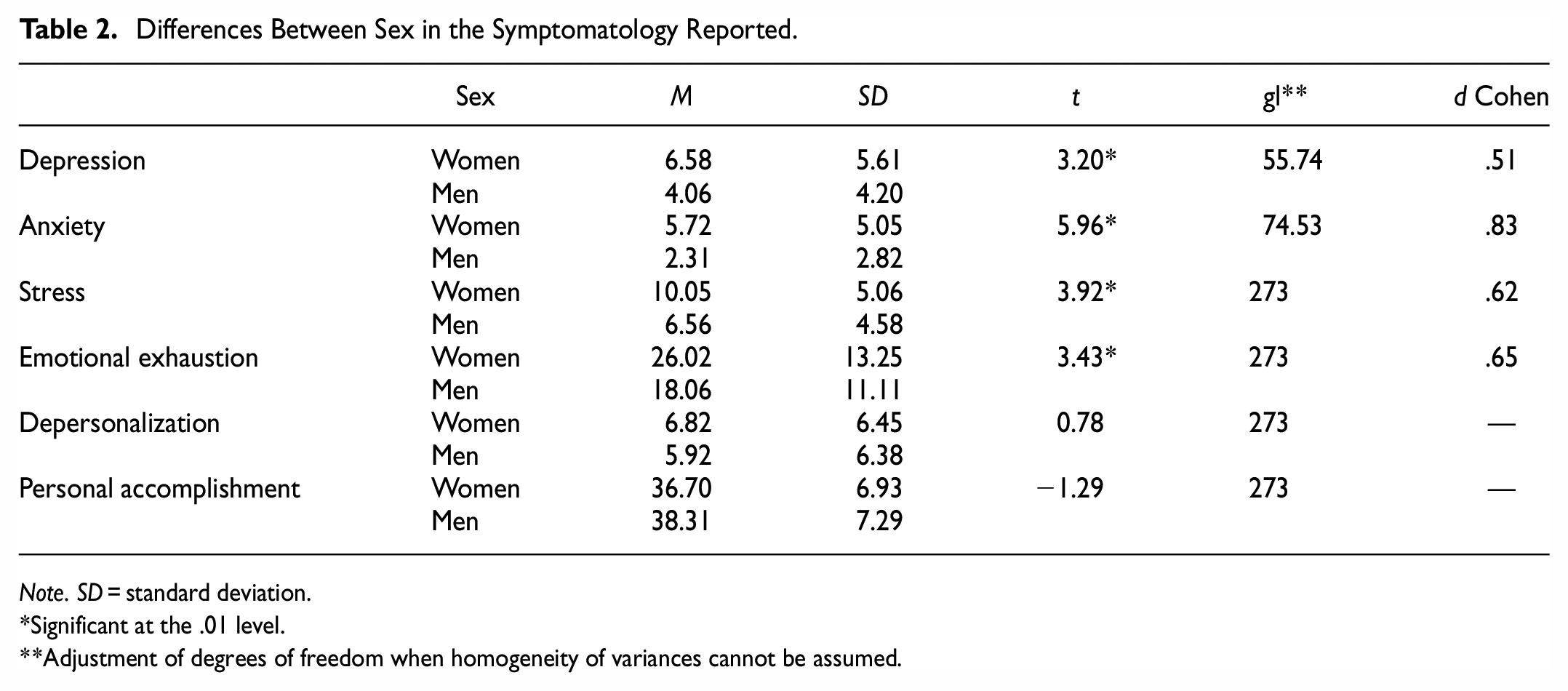
Note. SD = standard deviation.
Significant at the .01 level.
Adjustment of degrees of freedom when homogeneity of variances cannot be assumed.
Table 3 presents the results of multiple regression analyses predicting symptomatology (stress, anxiety, depression, and burnout). As Model 1 shows, coping strategies (acceptance, positive reframing, behavioral disengagement, and negation) contributed significantly to the prediction of depressive symptoms (r2 change = 0.347; p < .001). Thirty-five percent of the variance in depression may be explained by the coping strategies (mostly acceptance and positive reframing, which were negatively correlated with depression, and behavioral disengagement and negation, which were positively related to more depression). Model 2 shows that 23% of the variance in anxiety can be explained by behavioral disengagement and negation, which were positively correlated with more anxiety. Model 3 shows that 23% of the variance in stress can be explained by acceptance, behavioral disengagement, and negation, with behavioral disengagement and negation being positive correlated with more stress and acceptance negatively correlated with stress.
Results of Multiple Regression Analyses on the Prediction of Symptomology (Depression, Anxiety, Stress, and Burnout).

Note. VIF = Variance Inflation Factor (multicollinearity).
Significant at the 0.01 level.
Model 4 shows that 34% of the variance in emotional exhaustion can be explained by acceptance, substance use and behavioral disengagement, which was positively correlated with more emotional exhaustion, as well as drug use; acceptance is negatively correlated with emotional exhaustion. Model 5 shows that 36% of the variance in depersonalization can be explained by active coping, substance use, and behavioral disengagement, which was positively correlated with more depersonalization as well as drug use; active coping was negatively correlated with depersonalization. Finally, Model 6 shows that 30% of the variation in personal accomplishment can be explained by active coping, acceptance, and behavioral disengagement, which was negatively correlated with personal accomplishment; acceptance and active coping were positively correlated with personal accomplishment (a positive outcome, i.e., the more accomplishment, the less burnout).
Discussion
As previous studies have shown (e.g., Hassannia et al., 2021), the health crisis caused by COVID-19 has had a significant impact on the mental health of healthcare workers. Coping strategies aimed at managing this crisis may have been related to its psychological consequences (Main et al., 2011). The present study aimed to analyze its impact (in terms of levels of stress, anxiety, depression, and burnout) and how the coping strategies implemented by those concerned were related to symptomatology.
The sample presented a level of mild-moderate depressive symptomatology and moderate levels of stress and anxiety symptomatology, with the women self-reporting greater stress than men. These findings are in line with previous studies (Carmassi et al., 2022; İlhan & Küpeli, 2022; Lai et al., 2020; Sobregrau et al., 2022). Cheung et al. (2022), in a meta-analysis of the immediate psychological impact of SARS and COVID-19, found that the prevalence of anxiety was 37.8% and depression 39.8%. For the general population, the figures were 29% for anxiety and 21.9% for depression.
The results of the present study indicate that symptoms could be present months after the first waves of infection. Dong et al. (2021) found that around one third of health workers in China suffered anxiety, depression, and stress during the early stages of the pandemic. The authors predicted that the long-term impact would continue to be observed, and their findings confirmed this. Likewise, the sample of the present study revealed a medium level of burnout, with a moderate level of emotional exhaustion, depersonalization, and personal accomplishment, thus aligning with previous studies both of the first peak of COVID-19 (Conti et al., 2021) and the post-pandemic period (Zhou et al., 2022). This may be due to a lack of adequate psychological interventions (Chirico et al., 2020; Drissi et al., 2021). The health workers have been exposed to high and sustained stress, which is still present today, not only because of the high demands of their work but also because COVID-19 has not been vanquished. This highlights the importance of treating present symptomatology and helping healthcare workers to cope adequately with future situations.
In accordance with Chen et al. (2022), the present study shows that coping strategies predicted the symptoms presented by healthcare workers. In particular, the results suggest that acceptance, behavioral disengagement, negation, substance use, and active coping are most implicated in symptomatology (i.e., depression, anxiety, stress, and burnout).
Specifically, the results indicate that acceptance predict the level of depression, stress, or burnout (i.e., emotional exhaustion and personal accomplishment). However, it is essential to consider that the reliability of this COPE subscale (Morán et al., 2010) could have been higher in the study sample; hence the results concerning acceptance could be inconclusive. Nevertheless, in line with research on the general population (e.g., Feliu-Soler et al., 2018; Twohig & Levin, 2017), it appears that a willingness to confront undesirable experiences full-on and recognize them can help in their management, thus reducing symptoms (Hayes et al., 2011) and encouraging a sense of personal accomplishment. A recent systematic review (Rudaz et al., 2017) showed that acceptance and mindfulness training improved the mental health of health workers, reducing their levels of stress and burnout.
The present study also found that active coping, namely, initiating direct action and increasing one’s own efforts to eliminate or reduce the stressor, was associated with depersonalization and personal accomplishment (because the most active health professionals are those who presented less typical symptoms of burnout). This contradicts the findings of studies conducted during the pandemic, where such a strategy was inversely correlated with anxiety (Lara et al., 2021), possibly because it reduced the peak of anxiety that resulted from the acute situation but was not sustained over time (since stress or depression can be either acute or chronic; Hammen et al., 2009).
By contrast, behavioral disengagement (a maladaptive strategy) was shown to be related to all the symptomatology under examination. It predicted greater anxiety, depression, and burnout (i.e., emotional exhaustion, depersonalization, and personal accomplishment as an indirect association). Greenglass et al. (2022) found that the tendency to limit attempts to deal with a stressor, including giving up on goals with which the stressor interferes, was related to anxiety during the first wave of the pandemic, while Fukase et al. (2021) demonstrated that behavioral disengagement was also associated with the likelihood of depression. Moreover, this strategy has been associated with burnout, though not in health personnel; in particular, it has been found to predict neglect (Montero-Marin et al., 2014).
Another strategy is negation, which predicted psychological distress, specifically depression, anxiety, and stress symptoms. Also, in police officers, it has been found that negation is a maladaptive coping strategy (Acquadro et al., 2015). Negation may cause the person to avoid or limit the possibility of coming into contact with negative personal experiences, thus perpetuating the negative emotion, though it may not be associated with burnout. Herbert et al. (2013) concluded that negation in an emotional context can have mixed results, depending on what is implied logically by the negation; it may also have positive effects because it may rest of the negated concept. Perhaps, negating the situation helps healthcare workers to reduce its effects on their work; it may not predict emotional exhaustion or depersonalization but it may also not allow for personal accomplishment.
Finally, substance use was associated with emotional exhaustion and depersonalization, which is congruent with the findings of other COVID-19-era studies that concluded that more frequent use of drugs correlated with higher levels of burnout (e.g., Mercado et al., 2022). As was explained above, this can be a way of reducing negative personal experiences that, while reducing discomfort in the short term, increases fatigue in the medium and long term.
The present study has several limitations that should be born in mind when interpreting and generalizing from the results. First, the sample comprised a disparate number of men and women, and this study did not differentiate between type of healthcare workers; future researchers might consider including more males and analyze the differences between professionals. Second, as it was a cross-sectional study and relied on self-report, it was not possible to establish causal relationships between the variables. Despite these limitations, the study has identified symptoms that were presented by healthcare workers months after the start of the COVID-19 pandemic. In addition, it has shown how their coping strategies may have been adaptive or maladaptive. Studying pandemic coping behavior is very important for two main reasons: first, it can help those who help so that they can have coping mechanisms that decrease their well-being or quality of life or, even more significantly, generate disorders; and second, because the mental health of healthcare workers affects the care they provide to their patients; for instance, poor mental health may increase the rate of medical errors (Jyothindran et al., 2020). Thus, helping these professionals to develop strategies such as acceptance or active coping, and avoiding negation, behavioral disengagement, and the use of substances to mitigate the stressor, may not only improve their well-being and quality of life but also the care they give their patients. In this line, incipient results suggest that some psychological interventions could have reduced depression, anxiety, and stress during the COVID-19 pandemic (Varela et al., 2023). In particular, online CBT, which teaches strategies to deal with stressful situations, has proved effective in treating and preventing many stress-related disorders (e.g., Bureau et al., 2021; Weiner et al., 2020). More research is needed to apply these interventions to the medium and long-term effects of the pandemic.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.