
Abstract
Health professionals who come from different cultural backgrounds are required to interact competently and at the most acceptable communication level that meets the demands of the multicultural context in which English is the medium of communication. Lack of proper communication in such contexts can establish a hostile work environment. Thus, health programs should prepare students interactionally to operate within the work environment competently. A total of 42 nursing students in a Saudi university responded to a Discourse Completion Test. The data show that nursing students demonstrate a tendency to use direct refusal strategies, especially when refusing a request. The analysis also reveals problematic refusal semantic formulas used to address a higher-status person. Thus, diagnosing such communication issues can contribute to establishing a healthy work environment.
Introduction
Investigations of speech acts have played a vital role in exploring intercultural communication and identifying various social and cultural norms. The speech act concept was first introduced by Austin (1962), who explained the perception that a speaker’s words and/or sentence choices can involve an action; that is, by using speech acts, we can request, thank, apologize, complain, or refuse, among others, which are all part of our daily communication with people in any setting. Although speech acts exist in all languages, their linguistic forms and contextual occurrence are culture-specific (Brown & Levinson, 1987); accordingly, what might be appropriate and acceptable in one culture could be odd or unacceptable in another.
In this realm of research, many interlanguage pragmatic investigations have examined language learners’ use of speech acts and how the usage varies from that of native English speakers (Al-Mahrooqi & Al-Aghbari, 2016; Darweesh & Mehdi, 2016; Keshani & Heidari-Shahreza, 2017; Sharqawi & Anthony, 2019; Tanck, 2004). Refusals, which have been identified in the literature as one of the most challenging and inherently threatening speech acts because they require many face-saving strategies (Brown & Levinson, 1987), have been investigated in various languages, including Arabic (e.g., Abed, 2011; Al-Issa, 1998; Al-Mahrooqi & Al-Aghbari, 2016; Huwari & Al-Shboul, 2015). The findings have revealed the refusal semantic formulas commonly used by language learners (i.e., learners of English as a foreign/second language) and their appropriateness relative to those produced by native speakers of English. However, very few investigations have explored this speech act among health students (Li & Sun, 2015) and its potential impact on the work environment (i.e., the hospital setting).
Within health institutions, health professionals who come from different disciplines and, most importantly, different cultural backgrounds are required to work in teams and interact competently, not just at their specialty level but also at the most acceptable communication level that meets the demand of the multicultural context in which they work—hospitals (Iedema, 2007; Jones, 2013). Lack of proper communication in such sensitive context may create gaps where medical errors can occur and establish a hostile work environment. For example, various investigations examining junior nurses’ hospital training report on nurses’ experiences with unhealthy work environments. Thomas and Burk (2009) describe various stories in which nurses experienced horizontal violence and negative peer-to-peer behavior in the hospital setting. In one narrative, an intern expressed her discouragement because of the registered nurse’s refusal to answer a simple question: “I asked her if I could ask a quick question and she responded by saying, “No, not really,” without even looking up at me” (Thomas & Burk, 2009, p. 229). Examples like this reveal ineffective communication with suppressed negative feelings that, if ignored, can lead to a potential hostile work environment (Hinchberger, 2009). If perceived as impolite, refusals can lead to serious communication conflicts, especially when contextual factors, such as the interlocutor’s social status, gender, educational level, and so on, interfere. Accordingly, considering that English is the official medium of communication in hospitals, educational health programs are required to prepare health students (speakers of English as a second/foreign language) clinically and interactionally to competently operate within the work environment. Thus, one topic in need of further research is health students’ interactions, in particular the types of speech acts used by this population and the extent to which they reflect the students’ pragmatic competence and readiness for the multicultural contexts in which they will eventually work. This study explores the speech act of refusal as used by nursing students who speak English as a foreign language.
Materials and Methods
The Discourse Completion Test Instrument
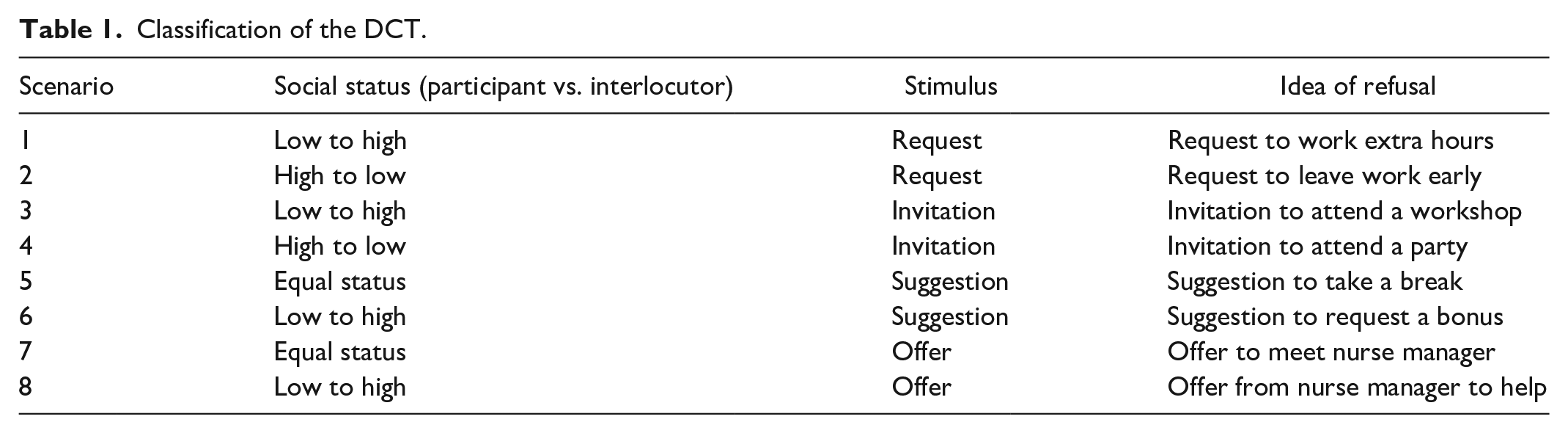
Similar to previous speech act investigations, the Discourse Completion Test (DCT) instrument, first used by Beebe et al. (1990), was employed to collect data in this study. The DCT was adjusted with content-enriched prompts (all in English) that mimic hospital-setting scenarios to suit the targeted audience (the appropriateness of the scenarios was confirmed with nursing faculty). The instrument (see Appendix) included eight scenarios to elicit refusals for requests, invitations, suggestions, and offers (two scenarios for each). Each scenario contained a short description of the scene followed by an incomplete dialogue in which the participants performed the refusal speech act in writing. Additionally, each scenario provided information about the role of the participant and the interlocutor (e.g., staff nurse, nurse manager [NM], etc.). The instrument was disseminated manually and via an online survey program (surveymonkey.com). Table 1 summarizes the eight scenarios according to the social status of the participant and the interlocutor (the controlled variable), the stimulus, and the idea of refusal.
Classification of the DCT.
Participants
Forty-two female college students in a Saudi health university responded to the DCT instrument. All students were majoring in nursing and studied English as a foreign language in school and in the preparatory year (English courses for three academic semesters) in college. Since the Saudi healthcare system hosts international healthcare professionals who work side by side with their Saudi counterparts; upon graduation, these Saudi nursing students are expected to work in Saudi hospitals where English is the medium of communication with equal coworkers and superiors who come from various cultural backgrounds including the United States, Europe, Philippines, India, and South Africa, to name but a few. Ethical approval was obtained from King Abdullah International Medical Research Center. Incomplete or inappropriate responses (e.g., responding with an approval instead of a refusal) were discarded; a total of 304 responses were collected.
Results
Beebe et al. (1990) classification scheme was used to code the data. As the first to examine refusal strategies, these authors classified refusals into three main categories: (1) direct refusals in which the speaker refuses in a direct, blunt manner using expressions such as “No” or “I can’t”; (2) indirect refusal in which the speaker puts some effort into the refusal and uses strategies (e.g., statements of apologies or regrets, excuses, alternatives, etc.) to soften the refusal expression and reduce its impact on the listener; and (3) adjuncts to refusals in which the speaker uses utterances, such as statements of positive feeling or opinion, to avoid producing any refusal response, that is, to soften the impact on the listener.
Table 2 shows the overall semantic formulas used to structure refusals in this dataset. The analysis revealed that the semantic formulas follow the three broad categories of refusal strategies proposed by Beebe et al. (1990): direct, indirect, and adjuncts to refusals. Emojis or images used to express emotions (Merriam-Webster, n.d.), emerged as a semantic formula in this dataset and were classified as “adjuncts to refusals” because they were mostly used with willingness, with statements of positive opinion or feeling, and with statements of empathy (Table 3).
Semantic Formulas of Refusal Strategies Used by Nursing Students.

Frequencies of the Strategies Used by Speakers.

To better understand the structure of refusals, the rest of this section examines the semantic formulas of refusal as they were used in the four scenarios: request, invitation, suggestion, and offer. Although some of the refusals were produced with grammatical errors, mostly tense errors, they are still accepted and deliver the refusal meaning. In this dataset, direct refusal strategies were the most used (53.6%) across all scenarios when producing refusals, but mostly when refusing a request. In both status scenarios (Scenarios 1 and 2), most students in this dataset used the semantic formula “flat no” followed by “statement of regret,” “negation of proposition,” “excuse/reason/explanation,” and/or “lack of empathy.” For example, in making a refusal to a low-status person (Scenario 2), students refused the staff nurse’s request to leave work early with a direct “flat no” followed by “negation of proposition” and/or “excuse/reason/explanation” (e.g., No, you can’t/No, as you can see we’re too busy so you have to stay/You can’t, no/No, you can’t I need you/No, there is a lot of work). In a similar manner, when refusing the nurse manager’s request to work overtime (Scenario 1), the data showed that students used direct refusals, but this time with the supplement of “excuse/reason/explanation” and/or “statement of regret” (e.g., No, sorry, I can’t because I’m tired and I can’t work anymore/No, sorry, because my shift is already finish/No, I need to go, sorry). In Scenario 2, students’ use of “excuse/reason/explanation” was meant to support or justify their direct refusals because their focus was on the responsibility in the given scenario rather than on softening the impact of the refusal for the interlocutor. The lack of the use of “statements of regret” with a lower-status interlocutor may indicate that the students have exercised some power, as they acted as the more senior person in this specific scenario. In refusing to a higher-status person, however, although students used direct refusals, it seems that they were status conscious and made attempts to reduce the illocutionary force on the interlocutor using “statements of regret” as well as providing a reason or an explanation. This falls in line with Al-Kahtani (2005), who found that Saudis tend to give more excuses and explanations in refusals compared to US native speakers of English. The use of a “statement of regret” is also a common refusal strategy among Arabic speakers who often use it whenever they reject a request (e.g., Al-Issa, 1998).
The data also revealed incidents where students used direct refusals with the “lack of empathy” semantic formula (Morkus, 2009). For example, refusals such as No, I can’t because it is not my business; No, I am finished my work; and No, sorry, it’s not my business, if used in a real-life scenario could lead to a potential conflict as the interaction here is with a higher-status person. Students’ use of direct refusals in this setting may be in line with previous investigations that found that the use of direct refusals reflects speakers’ L2 proficiency and the lack of knowledge of the L2 language pragmatics (Takahashi & Beebe, 1993).
Direct strategy was also a preference when refusing an offer. In this dataset, two refusal semantic formulas emerged: (1) “flat no” followed by “gratitude” (e.g., No, thank you), which were used by many students to reject an equal-status offer (Scenario 7); and (2) “flat no” followed by “gratitude” and “excuse/reason/explanation” (e.g., No thanks, I prefer to do it myself/No thank you it’s ok no need/No thanks but I changed my mind); these were used to reject an offer from a higher-status person (Scenario 8). Most of the reasons given by students in this scenario indicated their preference for performing the given action in the scenario (e.g., I’d prefer to do it myself/I can do it myself/I can do it without help). Though all were direct refusals, students’ choice of refusal formula reflects their awareness of their difference in social status with the interlocutor; thus, in the latter formula, they have put some effort into softening the refusal by providing a reason or an excuse that prevented their acceptance. However, again, some examples in the dataset revealed the possible lack of L2 pragmatic competence when refusing an offer to an equal-status person (e.g., No this no one business/I mind my business), as well as to a higher- status person (e.g., Not anyone business, I like it this way/I like it this way, thanks).
Indirect strategy was the second most frequent (30.6%) refusal strategy used by nursing students in this setting. The data show students’ preferences using indirect refusals for rejecting an invitation to both high- and low-social-status individuals (Scenarios 3 and 4, respectively). The two most frequent refusal formulas were “wish” followed by “excuse/reason/explanation” and/or “regret” (e.g., I wish I could, but I didn’t bring a gift [−p]; I wished that, but I have a lot of work sorry [+p]), and a “statement of regret” followed by “negation of proposition” and/or “excuse/reason/explanation” (e.g., I’m really sorry, I can’t I have a meeting on the same time/Sorry I can’t[−p]; Sorry tomorrow I’ve some work/I’m very sorry I have something to do [+p]). The use of “statement of regret” followed by an “excuse” here follows the refusal strategy reported by native English speakers in similar situations; however, excuses and/or explanations given in this dataset (across all scenarios) were vague, unlike the detailed excuses reported by native speakers (Al-Kahtani, 2005; Tanck, 2004).
Responding to the suggestion scenario, the data also revealed several other alarming refusals that students produced in response to a higher-status person (Scenario 6). For example, refusal samples, such as I don’t care about salary, and it’s not benefit for you; why are you asking?/This is my work no need for a bonus mind your work/I’m not here for money/I know how to manage my time/I don’t see that as a good thing to do; they will pay me more if they say that it would be ok, have emerged as problematic refusals considering that the interaction is with a higher-status person, such as a nurse manager. Similar strategies emerged in other investigations on refusal and were classified as a “reprimand” (e.g., Al-Issa, 1998) in which the speaker expresses disagreement with the interlocutor and reprimands them. Again, similar to the “lack of empathy” refusal strategy, this strategy needs to be addressed because, if used in an authentic setting, it may lead to a potential conflict in a heavily hierarchical system (Thomas & Burk, 2009).
Initiating the refusals with the “wish” and “statement of regret” semantic formulas was specific to the invitation scenario in this setting which indicates students’ awareness of the sensitivity of turning down an invitation rather than a request. Additionally, various investigations indicated that “regret” is a common strategy used by Arabic speakers with which they demonstrate their inability to accept an invitation (Al-Issa, 1998; Al-Shalawi, 1997). In this dataset, the “regret” statement in its different forms (e.g., Sorry, I’m sorry, I’m very sorry, etc.), whenever it is used across the scenarios, has been placed in various positions, that is, at the beginning, middle, and end of the refusals.
Indirect strategy was also a preference when rejecting a suggestion from both equal- and high-social-status colleagues in this setting (Scenarios 5 and 6, respectively). The semantic formulas used for this scenario varied, but three formulas emerged as being frequently used: (1) “indefinite reply” (e.g., I don’t know. [−p]/I’ll see about that [+p]); (2) “conditions for acceptance” (e.g., I should finish my work, then I take a break. [−p])/If I need, I will ask for it[+p]); and (3) “agreement” followed by “excuse/reason/explanation” (e.g., It’s a good idea, but I prefer to finish my work first [−p]).
Adjuncts to refusals strategy was the least (15.8%) commonly used in this dataset. Interestingly, the strategy has emerged across all scenarios but mostly in refusing an invitation. Two semantic formulas to initiate the refusals were used: (1) “statement of positive opinion/feeling” followed by “emoji,” “negation of proposition,” and/or “excuse/reason/explanation” (e.g., Wow, it will be fun ☺ but I can’t I have to finish my work/Oh happy birthday ☺, but I have work) and (2) “statements of regret” followed by “emoji,” “negation of proposition,” and/or “excuse/reason/explanation” (e.g., Sorry I can’t ☹/I’m sorry I have other plans ☺/Sorry tomorrow I have some work ☹). The use of the emoji has emerged as a new strategy in this study and was not reported in any previous investigations on elicited refusals. A possible explanation could be that these characters have been used to express involvement with the interlocuter and to minimize any possible threat to their positive face considering the interlocuter’s gentle invitation.
Conclusions and Implications
This study explored how nursing students, speakers of English as a foreign language, structure the speech act of refusal. In line with Beebe et al.’s (1990) taxonomy, refusals in this setting fell into 3 broad categories: direct, indirect, and adjuncts to refusals. Similar to previous investigations among learners of English as a foreign language, nursing students in this setting leaned toward using direct refusal strategies, especially when refusing a request (Abu Humeid & Altai, 2013; Al-Mahrooqi & Al-Aghbari, 2016; Çiftçi, 2016). Semantic formulas, including the use of “lack of empathy” and “reprimand” to address a higher-status person, emerged as problematic refusals that, if used in real settings, may lead to communication breakdown, as they impose a threat to the interlocutor. Further investigations need to explore the likely occurrence of similar strategies in authentic interactions and their impact on communication and, thus, the workplace environment. Moreover, as this study was limited to female nursing students, further research is recommended to explore refusal strategies across genders as well as in naturally occurring discourse.
The use of emojis emerged as a new positive, polite refusal strategy that was used to support refusals. This finding indicates the importance of non-verbal communication in delivering refusals as it works on softening the impact of refusal and establishes a sense of involvement with the interlocutor. It also refutes the possibility of any intentional vulgarity by the participants using direct refusal strategies. In Arabic cultures, people normally consider the interlocutor’s feelings, which explains the heavy use of “reason/excuse/explanation” sematic formulas across the four scenarios. These findings were similar to Al-Eryani’s (2007) observations in which Yemeni Arab learners of English as a foreign language offered reasons and explanations to soften their direct refusals. The tendency to use direct refusal strategies, however, may reflect students’ language proficiency, which limited their choices of indirect strategy usage. Another possible rationale could be related to the lack of awareness of how to perform this speech act in L2.
To conclude, it is important to note that, in hospital settings, though not addressed, nurse interns are expected to follow an appropriate communicative style and to exhibit high linguistic awareness. Thus, with the increasing number of internationally educated health professionals who work collaboratively in multicultural settings in which English is the medium of communication, investigations of this type are vital. Health-related investigations have identified hierarchy, disruptive behavior, personality differences, personal values and expectations, and other factors as common barriers to interprofessional communication and collaboration in hospitals (Jones, 2013; O’Daniel & Rosenstein, 2008; Rosenstein & O’Daniel, 2008). Consequently, examining speech acts (specifically, cross-cultural speech acts) is essential to raising pragmatic awareness, which helps minimize intercultural miscommunication (Takahashi & Beebe, 1993). This should help in diagnosing and treating any potential communication issues among health students that can later contribute to establishing a healthy work environment. Since students in this study demonstrated occasional awareness of social status, nursing training curricula for L2 English can foster this by training them how to appropriately employ politeness strategies to alleviate threatening acts as well as consider contextual factors, such as social status, gender, and others, when performing them. For example, teaching students the refusal semantic formulas, their usage, and their cultural appropriateness can raise awareness of L2 sociopragmatic and pragmalinguistic competence. Additionally, similar DCT scenarios can be used to supplement teaching materials and help students compare and contrast their refusal production and predict its impact on the interlocutors as well as the work environment. In general, like any other language skill, the use of appropriate speech acts is an ability that can be acquired. Nativeness is not the goal here; rather, it is raising L2 pragmatic awareness, which can save nursing students from situations in which they might be perceived negatively by others or be subject to stereotyping in the workplace due to their unintentional violation of cultural norms.
Footnotes
Appendix
Please read the following scenarios. After each scenario you are required to supply a response in the blank after “YOU.” You are required to supply
You are working in a night shift at a hospital. At the end of your shift, the Nurse Manager, who is the head of the in-patient ward, asks you to work for an extra hour.
You are a Nurse Manager in a hospital. A staff nurse has some important work to do. He/she asks you to release him/her early in the afternoon, but you yourself have a lot of pending work that needs his/her presence.
You are a nurse in a hospital and the Head Nurse invites you to attend a workshop that he/she is presenting.
You are a Head Nurse in a hospital. A staff nurse invites to you to his/her daughter’s birthday party.
You work as a staff nurse in a hospital. The workload is very high, and you are getting stressed. Your nurse friend suggests that you apply for a long break.
You are a staff nurse in a hospital and the Nurse Manager suggests to you to request a salary raise (a bonus).
You are a staff nurse and have little free time as you have just started your own work. You were supposed to meet with the head of the ward to finish some paperwork. You generally do all your work yourself and without the help of others. Your nurse friend offers to meet the ward manager on your behalf and sort things out.
You are a staff nurse in a hospital. You thought of changing the time of your shift from night to morning, and you talked to your team about your intentions. However, you later changed your mind and wanted to keep the shift time as is. The Nurse Manager heard about it and offered to help you change the shift time. But now, you really don’t want to change the shift time.
Acknowledgements
The author extends her thanks and appreciation to all the participants (nursing students) who generously participated in this study.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.