
Abstract
This paper conducts a critical review of qualitative studies of the life experiences of people with health problems and proposes the notion of patient agency. It highlights that discontinuous continuity in life is the key category of life experiences around which individuals reveal agency. In particular, the paper first discovers multiple dimensions of life that individuals with illness engage in. It subsequently identifies four different manners in which discontinuous continuity in life is manifested along the multiple dimensions, such as single-dimensional rescaling, multi-dimensional shift, multi-dimensional embedding, and submission. These achievements and the remaining limitations in the medical sociology of patient agency are on a par with those in general sociological theories of individual agency. The paper proposes a set of future research agendas to expand these limits. This theory of patient agency is expected to renew approaches to how people lead their life in illness. It also suggests that patience should be a valid category of agency for general sociological imagination.
Introduction
In sociology, agency is generally defined as capacities for individuals to engage the social world (Emirbayer & Mische, 1998, p. 963) or the efficacy of human action (Sewell, 1992, p. 2). Accordingly, patient agency in this paper is defined as practices to lead a meaningful life in the world as a person who has health problems. Although few studies refer to agency directly among patients (Caiata-Zufferey, 2015; Redshaw, 2014), the medical sociological literature often addresses the capacities, self-efficacy, or practices of patients who lead their life meaningfully in the world. People with the sense of control, or the sense that one’s actions shape one’s life (Hitlin & Long, 2009), are healthier than those without the sense, due to the antecedent actual access to resources for health and the resultant responsible healthy behavior (Mirowsky & Ross, 2007; Oi & Alwin, 2017). Individual mastery over life, or mastering the circumstances of life, is conducive to mental health and general well-being (Charles et al., 1998; Pearlin et al., 2007). Patients empowered to reflect their views into medical treatments show better outcomes than their disempowered counterparts, thanks to the therapeutic effects of psychological empowerment (Broom, 2005; Radin, 2006) and the validity of the treatment interventions they recommend (Dew et al., 2014; Rapley, 2008; Shin & Shim, 2019).
Regardless of the consequences for health outcomes, agency in and of itself is significant to people in illness. The nursing literature recognizes that professional medical practices should be attuned to patients’ lifeworld and values that define their self as a meaningful individual (Kikuchi, 2005; Spichiger et al., 2005). It proposes to reconfigure intensive care as interventions enabling professionals to view illness and death as natural human passages and, subsequently, allowing patients time for engaging actively with these passages (Benner, 2004). The sociological literature adds that people with illness are socially expected to demonstrate their will to get well (Parsons, 1951; Radley, 1997) or some extent of control over their bodies (Kelly & Field, 1996) for them to be regarded as legitimate actors. In addition, building on the process of subjectivity-making inherent in power relations (Foucault, 1988[1982], 1991[1978]), studies demonstrate how patients reconstruct their subjectivities in illness, being surrounded by multiple power relations involving doctor–patient relations and family relations (Aujoulat et al., 2008; Mohammed et al., 2015). Finally, classic medical sociological studies place agency at the center of the life experiences of ill people. The liminal state of being ill and yet hoping without certainty to recover pushes individuals to question taken-for-granted life norms and to juggle with “the factors of existence (Turner, 1967, p. 106).” Accordingly, illness is a biographical event (esp. a disruption) rather than an isolated case amenable only to a doctor’s office (Bury, 1982). The regain of one’s biography and a sense of living (Frank, 1995), either through the recovery of health or the adaptations to illness, becomes the paramount issue. Health and illness implicate nothing but the presence and the absence of a sense of self in the world (Kagawa-Singer, 1993).
This view of illness as an inherent factor in agentic individual life practices becomes more explicit when illness is taken not as what people evade but what they learn to live with. Indeed, the literature on biographical continuity and reinforcement (Williams, 2000) demonstrates that individuals may feel that they are still leading a continuous life without disruption despite illness. Furthermore, some may even feel the continuity all the more due to illness. Homosexual French men who are infected with HIV (Carricaburu & Pierret, 1995), Javanese women who have contracted diabetes (Pitaloka & Hsieh, 2015), and old Americans who have lived through metastatic cancers as well as economic difficulties in the Great Depression (Killoran et al., 2002) all accept that difficulties from illness are not something that disrupts their life. Instead, these difficulties are taken as part of their life that they have had to live through as sexual minorities in bisexual-dominated France (Carricaburu & Pierret, 1995), as women in the male-dominated Java (Pitaloka & Hsieh, 2015), and as a poverty-experienced generation in the affluent U.S. (Killoran et al., 2002). To them, illness reinforces their sense of who they are and what they lead their life with.
Given these variegated findings, the current task in this critical review is not to adjudicate on whether illness brings disruption, continuity, or reinforcement to individual lives (Balmer et al., 2015; Sanders et al., 2015; Saunders, 2017; Trusson et al., 2016). Instead of upholding one out of these conflicting experiences, the task lies in synthesizing these findings into a holistic conceptual model that attends to how individuals with illness continue leading their life that is nonetheless laden with substantial disruptions and discontinuities. In particular, the current review purports to elaborate from existing studies what continues and what discontinues in the life experiences surrounding illness and to reveal various manners in which discontinuity and continuity play out together. Qualitative studies of patient experiences have largely emphasized either discontinuity/disruption or continuity/reinforcement but not both. This review purports alternatively to provide a holistic model that properly describes this ambivalence of patient experiences.
Comparable interests have existed in the literature, if formulated differently and not fully pursued yet. The disability literature has long set it as a crucial task to examine the unceasing “ability of the individual (with illness) to perform such social roles as worker, family member, citizen, or friend (Levine, 1987, p. 4)” and to explain how people manage their life well despite adverse health problems (i.e., “disability paradox”) or sometimes because of these health problems (Albrecht & Devlieger, 1999; Weinberg, 1988). Likewise, key moments in a life with illness are suggested to be examined as an ill person’s efforts for “restitution” (e.g., courage and humor pursuing to go back to the old normal life), “quest” (e.g., efforts to meet suffering head on and accept illness), and “chaos” (e.g., troubles, anger, grief, and depression; Frank, 1995, pp. 75, 97, 115). The leading scholarly inquiry on biographical disruption in illness simultaneously calls for an investigation of ill people’s strategic health management to minimize the impact of illness on their biography (Bury, 1982).
Sympathizing with these early efforts, the current review engages existing qualitative studies about the life experiences of people living with illness and disability, ultimately proposing discontinuous continuity to be the key category of life experiences for patient agency. It highlights two main findings from the literature along with their limitations. Firstly, studies demonstrate that people with health problems experience a loss in agency on a certain dimension of life (e.g., a physical, psychological, or social-relational dimension) and yet they continue their lead in life as they appreciate the still remaining, if shrunk, agency on the same dimension (Albrecht & Devlieger, 1999; Ginter & Braun, 2016; Sanders et al., 2015). In other words, people with illness experience a loss of agency in their reduced bodily practices of control over their life and yet they still reveal agency via the remaining practices of bodily control (Hallowell, 1999; Henshall et al., 2016; Scott et al., 2005). This is how people with illness secure continuity in their lead in life despite the ruptures from illness. It is, however, the limitation of these studies that they are focused on a single base of agency and unsusceptible to its multiple bases (Howard et al., 2010; la Cour & Hvidt, 2010; Sered & Agigian, 2008). These achievements and limitations will be elaborated in the discussion of patient agency as single-dimensional rescaling.
Secondly, other studies report instead that people with illness reveal agency as they live on multiple dimensions of life simultaneously. For example, an ill person attempts to actively lead its life not only on a physical dimension (e.g., efforts for reconstructing a bodily being) but on a social-relational dimension (e.g., efforts for making relations with family and friends; Kagawa-Singer, 1993). This multiplicity provides opportunities for people to secure continuity in life amid the difficulties and discontinuities from illness. However, these studies are deficient on two fronts. The studies register many empirical reports of various bases of agency and, quite often, incongruent manifestations between them, like the presence of agency on one base and its absence on another. On these occasions, the studies themselves (Broom & Tovey, 2008; Killoran et al., 2002; Sulik, 2009; Trusson et al., 2016) hurriedly conclude either for the presence or the absence of agency (but not both); either for continuity or discontinuity in life (but not discontinuous continuity nor continuous discontinuity); either for biographical reinforcement or disruption (but not both); either for the control-seeking life or the submission-taking life (but not both). Other studies avoid this limitation by not posing a conclusion for either this or that (Albrecht & Devlieger, 1999; Burke et al., 2011; Ginter & Braun, 2016; Henshall et al., 2016; Kaiser, 2008; Mohammed et al., 2015; Redshaw, 2014). Instead, they remain loyal to describing and only tolerating the often conflicting and incongruent life experiences of ill people. They fall short of explaining what social and individual conditions make these surprising incongruences present. The resort to the social context-free psychological models, like a temporal model of identity goals (Charmaz, 1995; Morse & Mitcham, 1998; Morse & Obrien, 1995), is the only exception. These achievements and limitations will be elaborated in the discussion of patient agency as multi-dimensional shift, embedding, and submission.
As a critical review, this paper proposes a conceptual “launch pad” for future research to expand these limits by embarking on empirical “tests” (Grant & Booth, 2009, pp. 96–97). Future research needs to investigate context-specific manifestations of multiple dimensions of life on which ill people reveal their agency and the ways in which these multiple dimensions coexist and interact with one another. In doing so, future research is expected to illuminate the patterns in which the multiplication of the bases of life becomes a critical mechanism by which ill people reveal patient agency. It will finally be able to adjudicate on the prediction that it is by this multiplication that individual agency reveals itself not only in control of but in submission to the circumstances of life.
Materials and Methods
Out of a variety of review types, this review conceives of itself as a critical review (Grant & Booth, 2009). According to the typology, inconsistent findings among qualitative studies of illness experiences invite either a critical review or a qualitative systematic review (i.e., qualitative evidence synthesis). Despite the similarity that both aim to develop a new theory (i.e., narratives, themes, and concepts) via conceptual innovation among reports of on-the-ground experiences, the latter is motivated by the practice-oriented needs to produce synthetic recommendations about “barriers and facilitators to the delivery and uptake of (health care) services” (Grant & Booth, 2009, p. 100). On the contrary, a critical review purports to “resolve competing schools of thought” and “provide a ‘launch pad’ for a new phase of conceptual development and subsequent ‘testing’” (Grant & Booth, 2009, p. 93); “while such a critical review aggregates the literature on a topic, the interpretative elements are necessarily subjective and the resulting product is the starting point for further evaluation, not an endpoint in itself” (Grant & Booth, 2009, p. 97).
Such a critical review features methodological characteristics in the SALSA framework (Grant & Booth, 2009, pp. 93–97): regarding search (“S”), it does not typically demonstrate the systematicity of other more structured approaches and, instead, purposively seeks to identify most significant studies in the field; for appraisal (“AL”), it attempts to evaluate studies according to their conceptual contribution to the field with no formal quality assessment; it produces a narrative and conceptual synthesis (“S”); its ultimate analysis (“A”) seeks to identify conceptual contribution to derive its own new theory.
Therefore, this review is based on a finite number of qualitative medical sociological studies that are significant in the field. This review began constructing a body of materials to be reviewed, by including studies about how people continue leading their life amid health problems that are published in leading medical sociological journals, such as Sociology of Health and Illness, Journal of Health and Social Behavior, Social Science and Medicine, Qualitative Health Research, and Health Sociology Review. It focused on medical “sociological” journals, since the subject matter of agency is most productively addressed in the sociological tradition (Glaeser, 2016; Joas & Beckert, 2006). It collected studies that address at least one of the key concepts such as agency, actorhood, selfhood, personhood, subjectivity, sense of control, and empowerment. This set of keywords itself was inspired by sociological theories of action and agency.
While perusing the initial set of studies, more excitingly, this review came to build an additional set of key concepts that these studies newly drew attention to, such as healing, self-healing, self-curing, biographical disruption, biographical continuity, suffering, sickening, ailing, and preserving. It was a rewarding process of expanding narratives and concepts for experiences of patient agency. By applying these concepts, more studies were added to the initial set of studies. In addition, when archived studies cite specific papers that are relevant and published outside the medical sociological journals, this review included these cited studies as well. As a result, it included a total of 41 studies in the following review (see Table 1 for details). In all, this process of building a corpus involved several circuitous and repetitive rounds of sociological theory-based keyword-building, paper-archiving, critical reading, keyword-expanding, and critical analysis.
Forty-One Studies Reviewed in the Order of Their Appearance along with Sub-Themes.

In proposing a resultant typology of discontinuous continuity in life, this review followed the principles of qualitative content analysis (Schreier, 2012); it conducted open coding on conceptual themes until the saturation point when no new theme for discontinuous continuity is found in the studies. In the process, it implemented incremental abstraction of lower-level concepts into higher-level concepts. Once critical reading hits the saturation point, it put the hitherto evolving coding frame to closure where discontinuous continuity in life is finally organized in four different themes with nine constituent sub-themes (Figure 1).
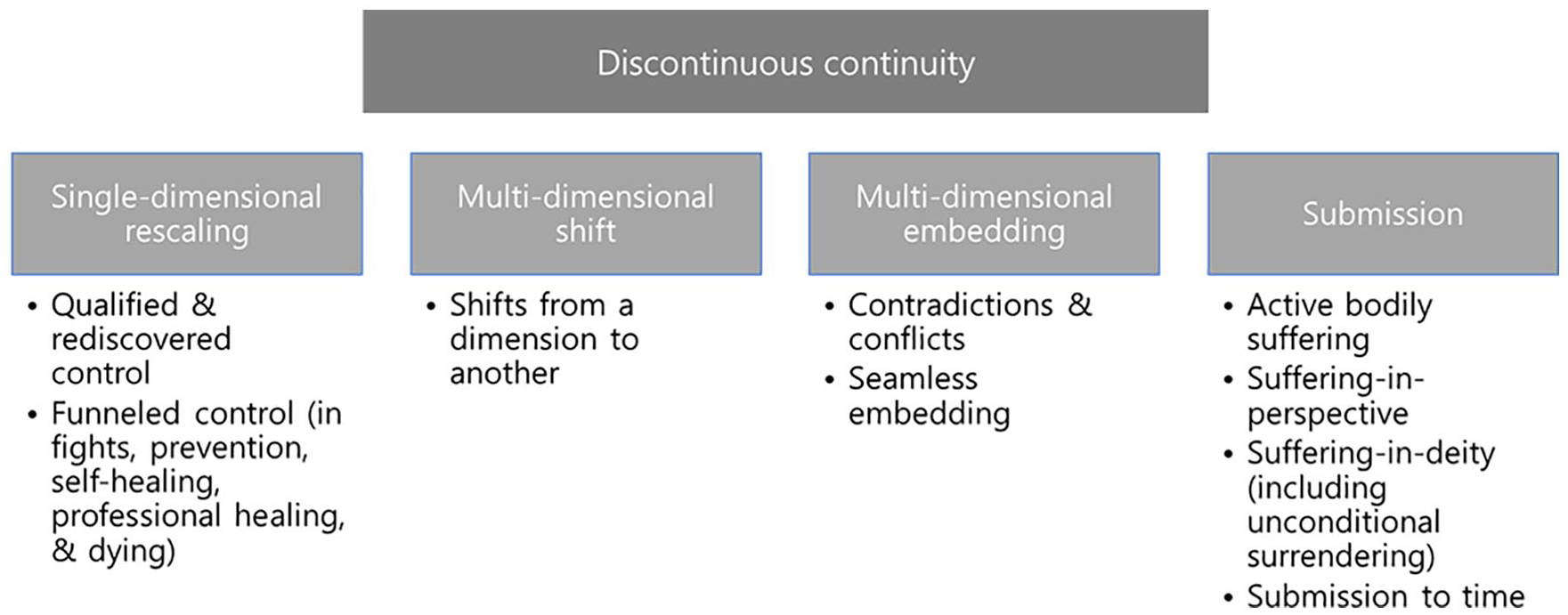
Patient agency in discontinuous continuity.
Results: Manifestations of Discontinuous Continuity
Existing studies report various ways in which people with illness reveal agency amid adversities. This review conceptualizes them as practices of patient agency and categorize them into four different types that compose discontinuous continuity in life: single-dimensional rescaling, multi-dimensional shift, multi-dimensional embedding, and submission.
Rescaling in the Control Over a Single Dimension of Life
The bodily aspect of life is an essential element that constitutes agency. For example, the loss of body parts (e.g., breasts) from surgery makes women discouraged, and a regain in the physical appearance makes them feel good about themselves (Kaiser, 2008). In addition, those living with breast cancer do not easily label themselves survivors due to the persistent fear of cancer recurrence and a potential loss in physical health (Kaiser, 2008). Likewise, the regain of physical appearance (e.g., hair, breasts) during cancer treatments is closely tied to Palestinian women’s coming to terms with their life in illness (Hammoudeh et al., 2016). At the same time, some bodily restraints from illness do not necessarily deter individuals from appreciating other bodily components of life and having a sense of continuous life on them. The bodily dimension of life is taken as an immediate source for people to reveal their agency by redefining, rescaling, and refocusing on the meaning of the dimension in their life. This review locates the first instances of discontinuous continuity in these practices of single-dimensional rescaling.
Firstly, people reveal their agency by confirming and yet redefining the significance and meaning of the bodily aspect of life that is affected by illness (i.e., agency in a qualified and yet rediscovered control). Although compromised, people with physical disability remain satisfied with the quality of life, based on the remaining control over bodily movements (Albrecht & Devlieger, 1999). British with chronic low back pain renew the view of their life and take it as still flowing amid the disability on the basis of their remaining enjoyment of physical activities (e.g., their picking up of walking instead of running, and swimming instead of tennis; Sanders et al., 2015). Australian parents of the kids who are hospitalized for congenital health defects locate the agency and personhood of the kids in their sustained bodily movements (Redshaw, 2014). Swedish women with recurrent breast cancer incorporate their persistent illness within their sense of continuing life and make sense of their living by letting go of what is lost physically and carrying on with what remains physically (Sarenmalm et al., 2009). The remaining control over life stands out in non-physical areas, as well. The Swedish women with cancer base their life on the remaining time, routines, or social relations and still make senses of their living, when they have clearly lost some in each of these life aspects (Sarenmalm et al., 2009).
Secondly, people with bodily restraints often reveal agency all the more in efforts to overcome these very restraints head on and heed to nothing else in their life (i.e., agency in a funneled control in fights, prevention, self-healing, professional healing, and dying). American single women who are on breast cancer treatments base their life solely on the remaining physical health and their effort to regain the lost health, so that they voluntarily exit from existing intimate relations with a partner and give no concern to building new relations other than working on their own body (Ginter & Braun, 2016). This kind of agency is most drastically revealed by individuals who identify themselves with fighters against illness. Fighting against illness makes women with breast cancer feel positive about themselves regardless of the results (Kaiser, 2008). Americans who have lived for 20-some years with metastatic cancers view themselves as heroic battle fighters against illness (Killoran et al., 2002). An online self-help community of Norwegian women with breast cancer fight heroically through cancer treatments and, thus, continue working toward self-realization (Sandaunet, 2008). Parents of the kids with congenital health defects locate the personhood of the kids in the fact that these kids take medical treatments actively (Redshaw, 2014). A teenage girl with bodily disfigurements from multiple cancer treatments aspires to be healed as a human being by asking for the medical professionals’ acknowledgement of her own capacity and right to communicate with them regarding medical treatments (Speraw, 2009).
People reveal agency in their active involvement in and control of preventive health practices or healing processes, if not a fight against illness. British women whose family members have breast cancer take risk-managing measures proactively, such as genetic tests and preventive surgery, according to the sense of obligation to themselves for being legitimate individuals (Hallowell, 1999). Similar findings of agency in the active preventive measures are reported in other countries (Caiata-Zufferey, 2015; Petersen, 1998; Scott et al., 2005). In addition, British survivors of cancers engage in self-healing practices, such as diets, alternative medicines, and religious involvements, and find it essential to their life to gain a sense of control through these self-healing practices (Henshall et al., 2016). Americans with cancers experience the liberating and emancipating feeling that they are actively doing something every day from their voluntary use of alternative medicines other than the conventional medical treatments that doctors recommend (Broom & Tovey, 2008). When this sense of agency is valued in society, medical service users rely on these alternative medical resources as a status-generating asset and differentiate themselves who can wield self-healing agency from others who cannot afford those resources (Fries, 2013).
These control-seeking efforts sometimes take a scientific and professional outlook. American women with breast cancer for years reveal their sense of self through their increased sense of control and empowerment over breast cancer, by actively learning doctors’ techno-scientific language, reading medical journals, and predicting their future life in medical terms (Sulik, 2009). Canadians with cancers exhibit their self and subjectivity by desperately seeking to heal themselves and trying to become intelligent individuals (Mohammed et al., 2015). British women with breast cancer attempt to overcome the fear of cancer recurrence by actively engaging in regular tests, hyper-vigilance, and self-surveillance (Trusson et al., 2016). Canadian women with breast cancer get a sense of control over their life by actively participating in deciding whether they take adjuvant treatments (e.g., radiotherapies and chemotherapies after surgery) and, subsequently, by taking an interventionist approach in which they exhaust whatever treatment options available (Charles et al., 1998). The control-seeking is not only evident in healing but dying. Americans with advanced cancers become animated when they have a say in arranging hospice and how/where to die (Volker & Wu, 2011).
Shifts From a Dimension of Life to Another
Though significant, the physical aspect of self is not the only dimension on which ill people place their lives. A review of conceptual works stresses the multiple dimensions of existential meaning-making in relation to health and illness, such as secular, spiritual, and religious dimensions, although it does not specify what specific practices comprise each dimension (la Cour & Hvidt, 2010). Correspondingly, it is found among BRCA 1/2 mutation-carrying Canadian women that their self is defined in several terms, such as physical health, appearance, emotions, and relations (Howard et al., 2010); depending on which term they value, they attempt to preserve their self with different decisions about whether or not to take the preventive measures to reduce breast or ovarian cancer, such as regular screening, mastectomy, and oophorectomy. Likewise, practitioners of alternative medicines in Boston view the life experiences of people with breast cancer as “holistic sickening” in the sense that these people experience their life holistically on physical, spiritual, psychological, and social-relational dimensions (Sered & Agigian, 2008, p. 616).
Given this multiplicity, individuals reveal agency and secure continuity in their life by shifting the base of their living from one dimension to another. This review conceptualizes it as patient agency in discontinuous continuity via multi-dimensional shifting. For example, people with disabilities come to develop new layers to their sense of living, such as mind and spirit, when the bodily layer is damaged due to illness and disability (Albrecht & Devlieger, 1999); some seem to shift their base of life from body to mind/spirit relatively quickly, while others do so only with difficulty depending presumably on the severity of disability and their belief in the spiritual component of life. This manner of agentic practices is distinguishable from those of the people who place their life upon body, mind, and spirit in a relatively “balanced” and coterminous manner (Albrecht & Devlieger, 1999, p. 986). For another example, women who have lost breasts from cancer surgery focus on the personality gain in place of the physical loss and come to embrace their life (Kaiser, 2008).
The disability literature attests to multi-dimensional shifting with more nuance. Young South African burn survivors who live with bodily disfigurements (Lau & van Niekerk, 2011), people living with extreme bodily pains (Morse & Mitcham, 1998), and people with bodily impairments (Charmaz, 1995; Morse & Obrien, 1995) diversify the bases of subjectivity and the foundations for the positive meanings of life so that they come to define life as being based on mind and spirit instead of body. In their efforts to continue leading the life, some people take only the disembodied self in spirit/mind and reject the embodied (and disfigured) self. These people shift the site of a meaningful life from the physical ground to the non-physical one. This practice is qualitatively different from that of those who accept both physical and psychological/spiritual aspects of self with a sense of coherence or contradiction (Lau & van Niekerk, 2011). Sometimes shifting takes place in the other direction. People diagnosed with dementia shift the base of their continued self from the damaged cognitive aspect to their bodily existence with other people and to their spiritual relation with (i.e., faith in) God (Bryden, 2018); they do so with more or less difficulty.
Embedding in the Multiple Dimensions of Life
The practices of shifting are often not easy and sometimes irrelevant to some people. These individuals instead take the multiple dimensions altogether and base their life on this multiplicity. In doing so, individuals carve out alternative moments to reveal agency. This review conceptualizes them as patient agency in discontinuous continuity via multi-dimensional embedding.
Embedding takes several forms. Firstly, ill people reveal agency in nothing but their encounters with the contradictions and conflicts between different dimensions of life (i.e., multi-dimensional contradictions and conflicts). People with bodily impairments and pains identify their self with the perceived conflicts among the bodily, spiritual, and cognitive elements of life (Charmaz, 1995; Lau & van Niekerk, 2011; Morse & Mitcham, 1998; Morse & Obrien, 1995); these people exist where these conflicts are. A teenage girl with bodily disfigurements from cancer treatments stresses that bodily scars give her a sense of living and being healed as a human with two contradictory meanings (Speraw, 2009). She takes bodily scars with pride (i.e., the scars attesting to her non-bodily self that survives all the difficult treatments) as well as trauma (i.e., her existence in bodily impairments). This episode reflects the general dilemmas that are associated with an endeavor to practice agency to its full extent, both bodily and non-bodily. Implied in the episode is that this girl bases her being not only on the bodily aspect, which enacts her scar-based trauma, but also on the non-bodily aspect which breeds her pride in life despite the scars. While she appreciates her non-bodily being, it is her inevitable confrontation with the bodily scars that heightens the non-bodily sense of being to a deeper level. For another example, British with chronic low back pain construct their flowing biographies incessantly via dynamic negotiations between the physical self (i.e., the self with bodily pain) and the social self (i.e., social roles; Sanders et al., 2015). These people do not simply give up all their social roles due to the illness or simply keep performing their roles without being restricted by the illness.
Sometimes the negotiation between different foundations of self unfolds without any confusion, conflict, or contradiction and appears as seamless embedding next to one another (Lau & van Niekerk, 2011; Sanders et al., 2015; i.e., seamless embedding). Once accepting the multiple bases of life, individuals become agentic in combining the bases in different ways. For example, people with cancers base a sense of self on social-relational functioning (as family members and workers) as well as physical functioning, so that they can hold a stable sense of self based on the former when the self on the latter fluctuates (Kagawa-Singer, 1993). Danish women on the sickness absence from work due to mental problems define their life not as a onetime instance of leaving job (at the onset of illness) and returning to work (after recovery), but as a prolonged process of “healing a (vulnerable) self” in multiple life aspects concurrently (Nielsen et al., 2012, p. 302). For these women, a sense of self does not only lie in work but in health. Therefore, they keep working (and not stop working), if for fewer hours, all the while they invest enough time in healing. This way of living is viewed by themselves as a “stronger” and “empowered” life (and not a “handicapped” life; Nielsen et al., 2012, p. 308). For another example, Canadians who lead their professional work life while diagnosed with bone cancer redefine their life as composed multi-vocally of vocational work, identity work, and illness work (Parsons et al., 2008). This unique redefinition highlights not only the ever-present centrality of work in their life, in that the illness-healing process is categorized as illness work; it also demonstrates the weightiness of health in life and, more importantly, the relocation of (vocational) work as being only one of many (and not the only) possible works (involving health) in life.
A special case of this seamless embedding of multiple dimensions of life is located at the intersection of medicine and religion. Among individuals with breast cancer in the Middle East, their religious faith and the acceptance of the divine will as a cause of illness and health do not lead these women to passively accept their fate nor prevent them from seeking professional medical help (Al-Azri et al., 2013; Hamdy, 2009; Hammoudeh et al., 2016). Instead, these women actively reconstruct their subjectivity both on the religious front and the secular-scientific front at once.
Submission
When health problems hamper the control over the circumstances of life, ill people reveal agency by way of their effortful submission to these supra-individual circumstances, whether they be secular or sacred; material or spiritual. This review conceptualizes it as patient agency in discontinuous continuity via submission. Agency in submission takes several forms.
Firstly, agency in submission takes the form of submission to bodily suffering, or active bodily suffering. Canadians who are on colon and rectal cancer treatments take their suffering from chemotherapies not simply as side effects but the evidence that they are still living and being effectively treated (Bell, 2009). To this extent, suffering does not only mean agony; it means an existential foundation for them. Parents of the kids with congenital defects certify the agency of the kids with their difficult and yet indelible journey to endure all the medical interventions and to be “active in their being” and suffering (Redshaw, 2014, p. 132). In addition, the kids are active in their loving and thanking the parents. More fundamentally, agency resides in their being able to receive parents’ love amid all their bodily suffering. In the legal literature, likewise, the ability to feel pain constitutes a foundation of human agency (Berg, 2007). The nursing literature confirms that humanity lies in the individuals who are granted the capacity to weep and suffer and that medicine, if it aims for humane caring, needs to institute time and space for it (Benner, 2004).
Secondly, ill people reveal agency in submission by incorporating their suffering of health problems as part of many other difficulties that are characteristic of their whole life (i.e., submission to suffering-in-perspective). Americans with breast cancer liken their life not with surviving the cancer but with living with it and accept it as part of many difficulties in life (Kaiser, 2008). Ironically, this incorporation of suffering in the perspective of a whole life makes these women not reluctant to label themselves survivors who do not outlive the cancer but lead their own life despite the fear of cancer recurrence. Filipino immigrant women in the U.S. who are on breast cancer treatments do not take the notion of survivorship wholeheartedly and they instead view their living in illness as “passing through” many usual adversities and trials in migrating life (Burke et al., 2011, p. 189). Suffering and their acceptance of it are constant elements with which they have led the life. Thus, submission becomes only a matter of life. British who attend a diabetic renal clinic reveal stoicism and endurance as a way of presenting themselves in relation to illness, which is not active control-seeking or passive defeatism (King et al., 2002).
Thirdly, the incorporation of suffering into agency via suffering-in-perspective can be further enmeshed with religion, where submission to suffering is revealed as a willful act qualified within divine powers (i.e., suffering-in-deity). Thai women with breast cancer subscribe to the Buddhist teaching that life is filled with suffering and difficulties not limited to breast cancer. This religious norm-driven submission to suffering enables these women to live (with cancer) without too much stress (Liamputtong & Suwankhong, 2015). Americans who live for 20-some years with metastatic cancers frame their long living with cancers as being unremarkable and typical in their life journey that runs through economic hardships and various other difficulties (Killoran et al., 2002). The study finds that the submission to God helps these Americans to incorporate suffering as part of their life and view their taking it as their willful act. Javanese Indonesian women with diabetes take their life with illness as normal life experiences, in their active and persistent efforts to adapt their meanings of life to bodily sufferings that are taken as part of many difficulties in life (Pitaloka & Hsieh, 2015). For them, the life principles lie in submission, suffering, and passive autonomy under divine powers. They take the submission of life to God’s will as a process of being an empowered individual and reaching emotional and spiritual maturity.
At the same time, suffering-in-deity involves ill people’s unconditional surrendering to divine powers. Whereas Americans with advanced cancers value their control over how to treat cancers and how to die, they also find themselves able to keep on going once they turn over to God their whole life and the outcomes of cancer treatments, including whether to be healed or to die (Volker & Wu, 2011). Some Canadians with cancers shape their self and construct their subjectivity by submitting themselves to spiritual powers and accepting the intractability of the cancers, at the same time as they seek desperately for medical-technological cures (Mohammed et al., 2015). Palestinian women with breast cancer come to terms with their life by submitting illness and recovery to the will of God (Hammoudeh et al., 2016). Likewise, Thai women with breast cancer gain a sense of living by leaving their illness and health to Buddha (Liamputtong & Suwankhong, 2015). British survivors of cancers rely on spiritual and religious practices and some find it important to their life to gain calm and peace through these practices (Henshall et al., 2016). People diagnosed with dementia sense their continuous self and agency in their building relationship with God and in their desire for being despite the cognitive defects (Bryden, 2018; Swinton, 2007). These studies do not simply implicate some individuals who become able to live thanks to their submission to God; they implicate more distinctively other individuals who live ultimately to submit to God.
Lastly, submission is sometimes practiced more moderately in relation to time rather than divinities (i.e., submission to time). People with cancers portray their living with illness as “a journey” or the “living on borrowed time” (Broom & Tovey, 2008, p. 1657). British women with breast cancer actively plan for the future life and, at the same time, they acknowledge that they may not be allowed to live that future (Trusson et al., 2016). French men who get infected with HIV via homosexual relations base a sense of identity and continuity in life on “a wait in all its glory” that is an active wait for a miracle cure for re-living and, at the same time, a wait for dying (Carricaburu & Pierret, 1995, p. 76).
Discussion
This review proposes several directions for future research. Sociological studies of health and illness have long been interested in revealing how people with health problems continue leading their life. By reformulating this interest ingeniously within a general sociological inquiry of agency, this paper has reviewed the existing qualitative studies of illness experiences under the notion of patient agency. It has conceptualized four different manifestations of patient agency which shed brighter lights on the lives that people with illness go through. It proposes that agency is constructed and revealed in these specific practices of securing continuity in life despite all the discontinuities and disruptions stemming from illness (i.e., discontinuous continuity).
It is exciting to see that the achievements of these medical sociological works are on a par with the various conceptions about individual agency in general sociological theories. The very emergent notion of discontinuous continuity as the nature of patient agency in this paper resonates with the Bourdieusian description of habitus-based human action, that is, “transformations with continuity and regularity” (Bourdieu, 1977, p. 82), “regulated improvisation,” and improvised regularity (Bourdieu, 1977, pp. 78–79). The multi-dimensional composition of patient agency (i.e., shifting and embedding in multiple bases of life) is reminiscent of the rich meanings that are layered upon one another in individual action in economic transactions (Granovetter, 1985) and political mobilization (Padgett & Ansell, 1993). The notion of human agency lying both in active and passive intentionality, and both in control of and submission to one’s circumstances (Joas, 1996) finds its specifications in patient agency revealed in unidimensional rescaling and submission in this paper. To this extent, the notion of patient agency is not only a specific invitation to the agency matters among patients; it is also a general suggestion that the nature of human agency at large can be examined among patients and their patience in life. To be sure, there is strong support for this general suggestion. It is known that patience is one of the crucial elements in governmentality even among rulers (Foucault, 1991[1978], p. 96); as for the ruled, it is recognized that the relevant social skills for political challengers vis-à-vis incumbents lie in those which “keep their hopes of challenging (the incumbents) alive,” if challengers cannot immediately change the current rule by the incumbents (Fligstein, 2001, p. 117).
In this perspective, it is not simply coincidental that one of the future tasks of general theories of individual agency overlaps with what medical sociology of patient agency needs to do in the future. When individual agency is revealed in relation to multiple frames (i.e., habit, imagination, and judgment; Emirbayer & Mische, 1998), a toolkit of multiple cultures (Swidler, 1986), multiple structures (Sewell, 1992), or multiple institutions (Friedland, 2013), the ultimate investigation into the nature of agency lies in describing how these multiple practices of agency are combined together into patterns. The medical sociological literature of patient agency shares the same future task in more specific forms.
Firstly, it will be revealing to specify when people with illness reveal their agency on the basis of a single dimension of life and when they reveal it on the basis of multiple dimensions. In doing so, it will be also rewarding to explicitly compare the multiple dimensions that emerge in an empirical context (e.g., among women with breast cancer) and those that emerge in another (e.g., among men with prostate cancer). Secondly, it remains intriguing whether there are differences in the extent to which people with illness enjoy their life, depending on the various ways for them to reveal agency. It is very probable that a person who bases its agency only on a bodily dimension will experience a different sense of leading one’s life than another person who bases it on multiple dimensions involving both bodily and non-bodily ones. Likewise, it needs to be answered whether there is a difference between a person who leads the life on a set of multiple dimensions and another person who does so on another set of multiple dimensions. Thirdly, when people reveal their agency on multiple dimensions, it is implied that the agency on a dimension does not necessarily get along with the agency on another dimension. Thus, it seems to be worthwhile to take a survey of different manners in which these multiple dimensions get more or less organized with one another among different individuals or social groups. Fourthly, the multi-dimensional compositions of patient agency are often found to coexist with patient agency in submission, whereas the literature is short of any theorization of the coexistence. It seems to be promising to further investigate how multi-dimensionality and submission are related to each other.
Conclusion
Sociology has long addressed what constitutes human agency. Drawing on this perspective, this review identifies a coherent research interest among medical sociological studies of patient experiences (i.e., what people in illness lead their life with). It subsequently formulates a synthetic model of agency among people in illness, or patient agency. The model highlights that ill people practice their agency in four different manners: single-dimensional rescaling, multi-dimensional shift, embedding, and submission. It also highlights nine constituent sub-themes. Drawing on this holistic model, future research will not only be able to understand contradictory aspects of patient experiences simultaneously; from a general sociological perspective, it will also illuminate the extent to which the nature of human agency resides in patience (i.e., patience as agency).
Footnotes
Acknowledgements
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2020S1A5A2A01043365).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2020S1A5A2A01043365).