
Abstract
Inter-birth interval lengthening is a key component of fertility decline. Although South Africa fertility rate remains the lowest in sub-Saharan Africa, information on the effect of education on the interval between first- and second-birth across residential contexts is rarely documented. The study investigated the relationship between maternal education and second-birth interval (SbI) by residence among South African women. The study analyzed the 2016 South Africa Demographic and Health Survey data on 6,039 women aged 15 to 49 years who had reported at least one childbirth at the time of survey. Survival analysis methods were applied at 5% significance level. The SbI was significantly longer (p < 0.001) among urban (76 months) relative to rural (66 months) women. About a fifth of rural women and about a tenth of urban women had at most a primary education. Women who had a secondary education (aHR = 0.86; 95% CI [0.76, 0.96]) were 14% times more likely to delay second-birth compared to those who had at most a primary education in rural setting. Other determinants of SbI included region in rural; age at-first-birth and household wealth in urban; ethnicity, marital status at-first-birth and employment in both residential settings. The length of SbI remains long in both residential contexts, but longer in urban. Findings demonstrated rural-urban differentials in the relationship between maternal education and second birth interval, suggesting contextual impact. Fertility strategies targeted at strengthening health education for improved maternal and child health should be residential-context specific.
Keywords
Introduction
Fertility decline in most sub-Saharan African countries is remarkable over the last two to three decades. Compared to 1998, the current total fertility rate (TFR) amongst women declined from 6.3 to 4.2 in Malawi, 5.6 to 4.4 in Ethiopia, 4.6 to 3.9 in Ghana, 4.4 to 3.8 in Gabon, and 2.9 to 2.4 in South Africa (Population Reference Bureau, 2018; Tabutin & Schoumaker, 2004). Although South Africa fertility rate remains the lowest in sub-Saharan Africa, her observed fertility decline seems rather stalled, particularly in urban areas. Within the last two decades, TFR declined from 3.9 to 3.1 amongst women in rural but marginally increased from 2.3 to 2.4 amongst women in urban (NDoH, et al., 2019). Although literature suggested different patterns of sub-national fertility changes among sub-Saharan Africa countries (Lerch, 2017; White et al., 2008), urban pattern may have a strong impact on South Africa national fertility.
Amongst African countries, South Africa is the sixth most populous country with 2.6 children per woman and a median birth interval of 55.3 months (NDoH et al., 2019; Stats SA, 2018; United Nations, 2017). Rapid urban growth is a key feature of South Africa population. Urban population stood at about 68% which is marginally above global average and is estimated to be about 70% by 2030 (Stats SA, 2018; Atkinson, 2014). Previous studies have established that exploring fertility dynamics by residential contexts is key to unraveling demographic changes (Lerch, 2018; Shapiro & Tambashe, 2000; Towriss & Timaeus, 2018), most especially as it relates to urbanization in developing countries. Urban population, therefore, remains a platform through which the fertility changes could be investigated (Towriss & Timaeus, 2018).
Unarguably, there are needs for the examination of fertility transitions characterized by lengthening inter-birth intervals at sub-population levels. Studies have linked the postponement of all higher-order births, including the second birth as a driver of sub-Saharan fertility decline (Lerch, 2017; Moultrie, et al., 2012). Even though sub-optimal inter-birth intervals often have adverse consequences for maternal and child health outcomes (Ball, et al., 2014; Chen, et al., 2014; Mahfouz, et al., 2018; Molitoris, et al., 2019; Stevens, et al., 2018; Zhang, et al., 2017), the risk of second childbirth (and other higher-order births) can be curtailed compared to the risk of first birth. In contemporary South Africa, the transition from first to second birth is a critical segment in fertility change. With fertility preference of two children (Stats SA, 2015), having second childbirth is an event that most South African women look forward to. The present study therefore focused on second birth interval (SbI), defined as time elapsed between first and second childbirth.
Although with a varying direction of association between educational attainment and the tendency of having second childbirth, literature had long recognized education as a major socio-economic driver of fertility transition (Bartus, et al., 2013; Bongaarts, 2020; Klesment, et al., 2014). Education, particularly women’s education, has a considerable impact on fertility transition in contemporary demography due to many pathways between education and family behavior. Such pathways include better access to and use of health information, higher decision-making autonomy, better contraception and reproductive system knowledge, greater potential for earnings, and increasing opportunity cost of childbearing (Bongaarts, 2020; Impicciatore & Tomatis, 2020). In lieu of the aforementioned and the growth of education especially among women, exploring the influence of education on SbI while controlling for other correlates may clarify the role of education in fertility transitions in South Africa.
Like any other birth interval, SbI could impact on the maternal and child health (Ball et al., 2014; Chen et al., 2014; Stevens et al., 2018; Zhang et al., 2017). Mahfouz et al. (2018) submitted that: on the one hand, inter pregnancy interval less than 24 months is attributed to a high risk of preterm birth and low birth weight; on the other hand, an interval higher than 59 months is linked to high likelihood of having a stillbirth and pregnancy-induced hypertension. Likewise, other researchers (Grundy & Kravdal, 2014; Nisha, et al., 2019) have documented that a long birth interval (>59 months) is attributed to poor maternal and child health outcomes. Meanwhile, literature had estimated a median birth interval of 72 months for the late 1990s in South Africa (Moultrie et al., 2012; Towriss & Timaeus, 2018). Nearly two decades thereafter, fertility at replacement level is yet to be attained. The knowledge of the relationship between SbI and maternal education could scale-up interventions that may further lower fertility and, consequently, reduce the likelihood of negative maternal and child health outcomes.
Empirical evidence has indicated multifarious factors associated with inter-birth intervals including SbI. These have been identified as proximate (biological and behavioral factors) and distal (socio-demographic and -cultural factors) determinants (Bongaarts, 2015; Erfani & McQuillan, 2009; Finlay et al., 2018; Palamuleni, et al., 2007; Ramarao, et al., 2006; Yohannes, et al., 2017). According to Bongaarts (1978), four proximate factors: marriage, postpartum in-fecundability, contraception, and abortion were identified to define direct determinants through which all socio-economic and cultural factors operate to influence human fertility. Although Bongaarts (1978) model continues to be relevant, fertility behavior has changed substantially in the contemporary population (Bongaarts, 2015). For instance, exposure to sexual activity and childbearing take place not only within but also outside marriages in South Africa. Additionally, the usage of contraception has diminished the effects of conventional prolonged breastfeeding and postpartum abstinence on inter-birth intervals owing to increasing urbanization, cultural changes, and government policies (Baschieri, 2004; Kim, 2003). Some researchers, meanwhile, have claimed that socio-economic and -cultural factors could directly influence birth interval dynamics (Baschieri, 2004; Rindfuss, et al., 1987). Intuitively, these factors could suggest either to delay time to second birth or otherwise.
For instance, women may experience a longer birth interval after the birth of a son compared to the birth of a daughter (Baschieri, 2004; Mace & Sear, 1997; Rossi & Rouanet, 2015). In addition, literature has documented a significant influence of wealth status, religion, or survival of the first birth on the length of SbI (Bao, et al., 2017; Ramarao et al., 2006; Singh et al., 2012). Similarly, studies have reported the association between birth interval lengthening, including SbI and contraceptive use: the more improved access to contraception, the longer the birth interval (Towriss & Timaeus, 2018). Women’s age, work status, partner education, and marital status have also been documented as determinants of SbI (Ahammed, et al., 2019; Fiori, et al., 2014; Singh et al., 2012). Women education, particularly, is considered as the most important determinant of fertility change (Bongaarts, 2020).
Studies have suggested a strong association between maternal education and birth interval (Bongaarts, 2020; Klesment et al., 2014; Van Bavel, 2010); an increased educational attainment often suggests a reduced fertility. Women who had no formal or a lower education have been cited to have higher odds for having second childbirth compared with those who had a higher education (Ahammed et al., 2019; Fagbamigbe et al., 2020; Newman & McCulloch, 1984). Aside from this negative association, a positive or non-negative relationship between maternal education and the tendency of having second birth has been documented. For instance, women who attained a higher education have second births earlier than those with a lower education attainment in a study conducted among some European countries (Bartus et al., 2013; Klesment et al., 2014). We hypothesized that maternal education would significantly influence the SbI lengthening in South Africa. The knowledge of the South African fertility transition may be relevant and useful for other sub-Saharan Africa countries, especially with relatively high fertility rates.
This study investigated the relationship between maternal education and time interval from first to second birth by residence among women of reproductive age in South Africa. The goal was to identify both similarities and differences of the inter-relationship between women’s educational attainment and SbI for the two residential contexts. This could improve the knowledge of national fertility dynamics including the timing and extent of demographic dividends which is critical for national development policy. Consequently, the study addressed two questions. (i) For how long would a woman residing in rural or urban delay the second childbirth after her first birth? (ii) To what extent is the discrepancy in SbI among women who live in the same residential area due to their level of educational attainment?
Method
Study Design and Setting
A cross-sectional and nationally representative 2016 South Africa demographic and health survey (SADHS) data was used for this study (NDoH et al., 2019). The data contain self-reported information on sexual and reproductive health history of the sampled women in South Africa. South Africa is made up of nine provinces and each of these provinces was categorized as urban, traditional and farm areas, to enhance survey precision.
The multistage cluster sampling technique was used, and the master sampling frame containing enumeration areas (EAs) was adopted from the 2011 census frame of the Republic of South Africa. At the first stage, a stratification-based probability proportional-to-size sampling method was used to sample EAs (known as clusters) as the primary sampling unit. A systematic sampling thereafter was used to select residential dwelling units referred to as households at the second stage. Of 750 clusters sampled for the survey, 468 were from urban, 224 traditional, and 58 farm areas. For the purpose of this study, settlement/residence type is categorized as urban and rural (traditional and farm) areas. A total of 15,000 households were sampled from 750 clusters selected for the survey. A detailed sampling design and procedures has been reported (NDoH et al., 2019).
Study Population and Variables
A total of 6,039 (2,666—rural; 3,373—urban) women who had ever given birth were included in the study, having excluded women who had a multiple first births.
Outcome variable
The dependent variable of interest was time interval between first and second childbirth amongst women in South Africa. Women who did not have second childbirth as at the time of the survey were right-censored and were coded 0; otherwise, 1 in the analysis.
Independent variables
The main independent variables were maternal education (at-most primary = 0, secondary = 1; higher = 2) and place of residence (urban = 1 or rural = 2). Also, an interaction between maternal education and place of residence variable was generated (at-most primary/rural = 0, at-most primary/urban = 1, secondary/rural = 2, secondary/urban = 3, higher/rural = 4, and higher/urban = 5). Other independent variables considered for the study were region/province, ethnicity, wealth index, age at first-birth, marital status at first-birth, employment status, contraceptive use, first-birth sex, first-birth survival, and desire for more children. The detailed description of these variables is presented in Table 1 and included demographic, socio-economic, cultural, and bio-behavioral factors.
Definitions of Independent Variables.

Data Analysis
As the main goal of the study is to investigate the influence of maternal education on time interval of first to second childbirth, survival analysis methods were used for the analysis. The “true survival time” for women who have had second-birth was the SbI. The “censored time” for the women yet to have second birth was time since the first-birth and interview date. The Kaplan-Meier survival method was used to describe the women’s time interval to second-birth while the log-rank test was employed to examine the association between SbI and the explanatory variables. Also, the Mann-Whitney test was applied to examine the rural-urban differences in average survival time. Semi parametric-based extended Cox hazard regression was thereafter used to explore maternal education effect on SbI, having confirmed violation of proportional hazard assumption. The model is expressed as follows (Akinyemi, et al., 2020):

where bj is the jth coefficient of the predictor variable Xj; h0(t) is the baseline hazard function and h(t)/h0(t)—hazard ratio (HR); γj is the jth overall effect of Xj(t) = Xj × gj(t) (time dependent predictor(s)) such that its positive value indicates the HR increases with increasing time; otherwise, it decreases; p1—number of predictors, independent of time; p2—number of predictor(s) which interact with time; and g(t) = t (in which estimated HRs increase or decrease exponentially as t increases). A detailed description of Cox proportional hazard model including the extended Cox hazard model’s time function, gj(t) is presented in Supplemental Appendix 1.
The coefficient bj indicates the changes in the expected duration of SbI for every unit change in the jth predictor. The exponentials of the coefficients suggest the likelihood of having a second-birth; thus, HR > 1 indicates higher likelihood, HR < 1 lower likelihood, and HR = 1 equal likelihood.
The crude cox proportional hazard model was used to explore the association between maternal education and SbI in both rural and urban settings, including the interaction between the two key variables. All significant variables (p < .15) premised on the log-rank test were thereafter included in the extended Cox regression model using a-two model approach while controlling for other predictors as well as accounting for multicollinearity in each of the settings. In model 1, maternal education and variables to define other socio-demographic characteristics were included; model 2 is the full model with the exclusion of partner’s education due to collinearity with marital status at first birth. However, only the full model tagged model 3 was considered for the pooled data. The adjusted HRs (aHRs) including their 95% confidence intervals (CIs) and/or p-values were reported. Importantly, provisions were made for intracluster correlation and the data was weighted to adjust for differences in population sizes of each province in South Africa. All analyses were conducted at 5% level of significance using Stata 14.
Ethical Approval
The South African Medical Research Council (SAMRC) Ethics Committee and the ICF Institutional Review Board reviewed and approved the survey protocol, instruments, and material prior to the collection of data. Refer to SADHS 2019 report for the details of the ethical approvals for the parent study (NDoH et al., 2019). The Demographic and Health Surveys Program, ICT International, USA also permitted the usage of the dataset for the present analysis.
Results
Participants’ Characteristics
The average (±SD) ages of the rural and urban women were 33.1 (±8.6) and 34.0 (±8.5) years, respectively. While women aged <20 years at first birth constituted the highest percentage of rural (51.1%) and urban (44.4%) women studied, those of aged ≥25 years constituted the least (Table 2). About three-quarters of the women had secondary education, while about one-fifth never used contraceptives in both rural and urban settings. Nearly all the women’s first childbirth survived in both the rural (96.1%) and urban (96.6%) areas.
Distribution of Women’s Characteristics and Their Association With the Median Time to Second Birth According to Rural and Urban Settings.
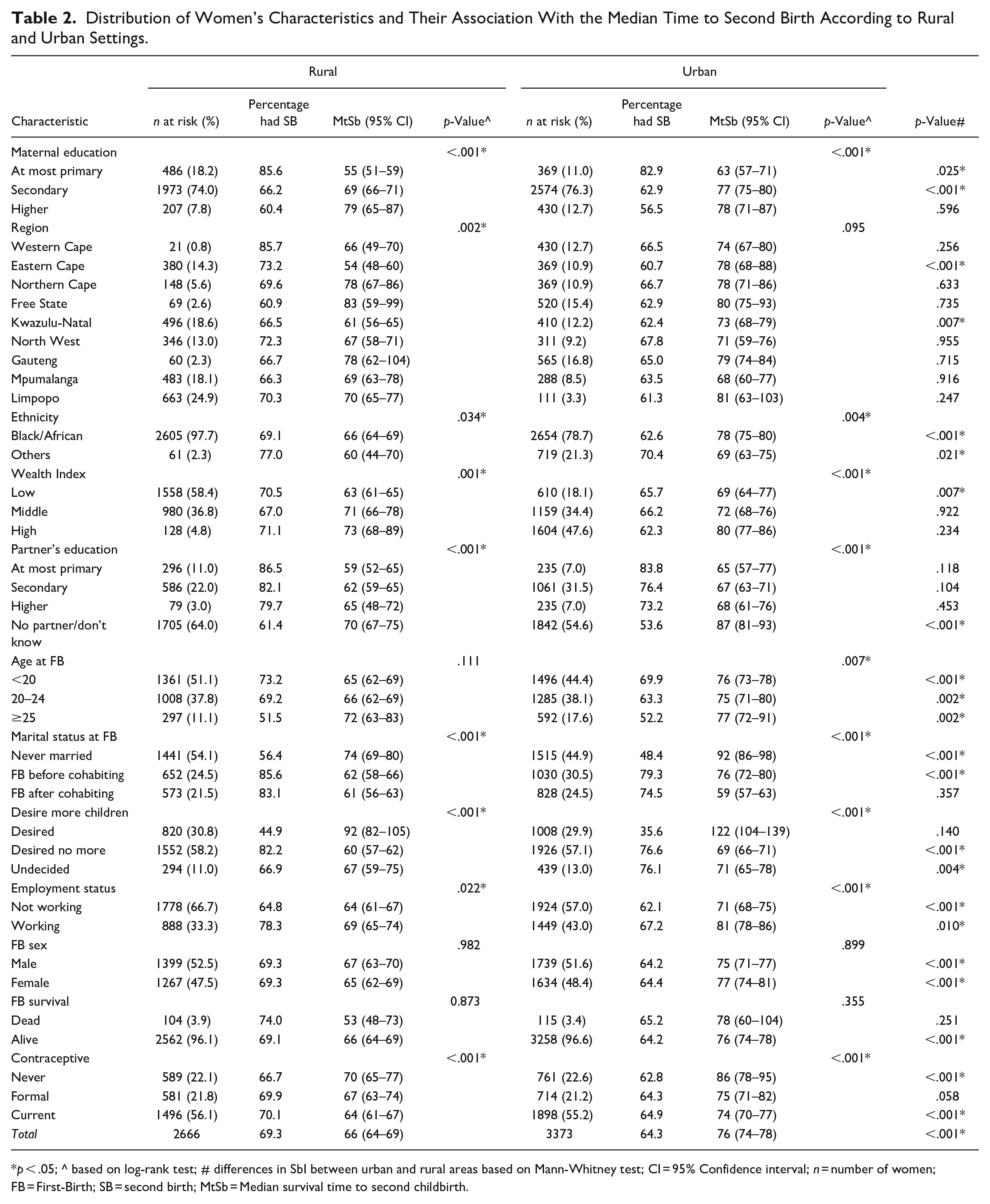
p < .05; ^ based on log-rank test; # differences in SbI between urban and rural areas based on Mann-Whitney test; CI = 95% Confidence interval; n = number of women; FB = First-Birth; SB = second birth; MtSb = Median survival time to second childbirth.
Of 6,039 women analyzed, 4,015 (66.5%) had had second births—1,847 (69.3%) in rural and 2,168 (64.3%) in urban—prior to the date of the interview. Black/African was the most common race of both the rural (97.7%) and the urban (78.7%) women; however, women of other (White, Colored, and Indian/Asian) race had the majority of second births in both the rural (77.0%) and urban (70.4%) settings. The percentage of women who had second birth decreased as the women’s age at first birth and their educational attainment increased, in both settings. While 85.6% of rural and 82.9% of urban women who had at most a primary education had second-birth, only 60.4% of rural and 56.5% of urban women who had a higher education had second-birth. Most women who neither decided nor desired another child had had second-birth. One-third of the rural women reported that they were currently working compared to 43.0% of urban women. Compared to 44.9% of urban women, more than half of rural women were never married. The median survival time to second birth (MtSb) was 66 (95% CI [64.0, 69.0]) and 76 (95% CI [74.0, 78.0]) months amongst rural and urban women, respectively (Table 2). This finding is also shown in Figure 1, a probability plot showing the risk and cumulative survival curve of having a second birth.
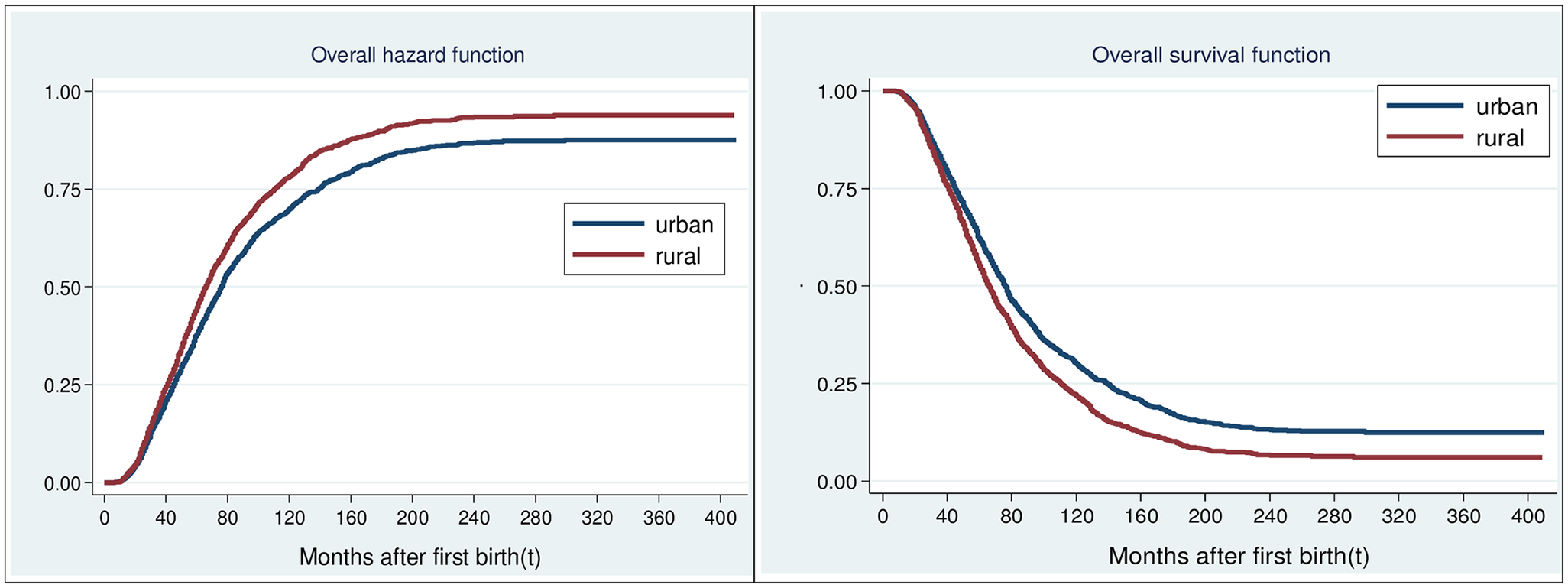
Overall survival and hazard function of second birth interval by residence. The probability plot showing the cumulative survival curve and the hazard of having a second childbirth.
Urban-Rural Differences in the Pattern of Second Birth Interval
The findings show a shorter MtSb among women who attained at most a primary education compared to those who had a secondary or higher education, irrespective of their residential abode. Urban women who had at most primary (urban—63 [57, 71] vs rural—55 [51, 59] months, p = .025) or secondary (urban—77 [75, 80] vs rural—69 [66, 71] months, p < .001) education had a significant longer MtSb compared to their rural counterparts (Table 2). Figure 2 corroborates this finding; it shows the probabilities of having second birth by maternal education and its interplay with place of residence.
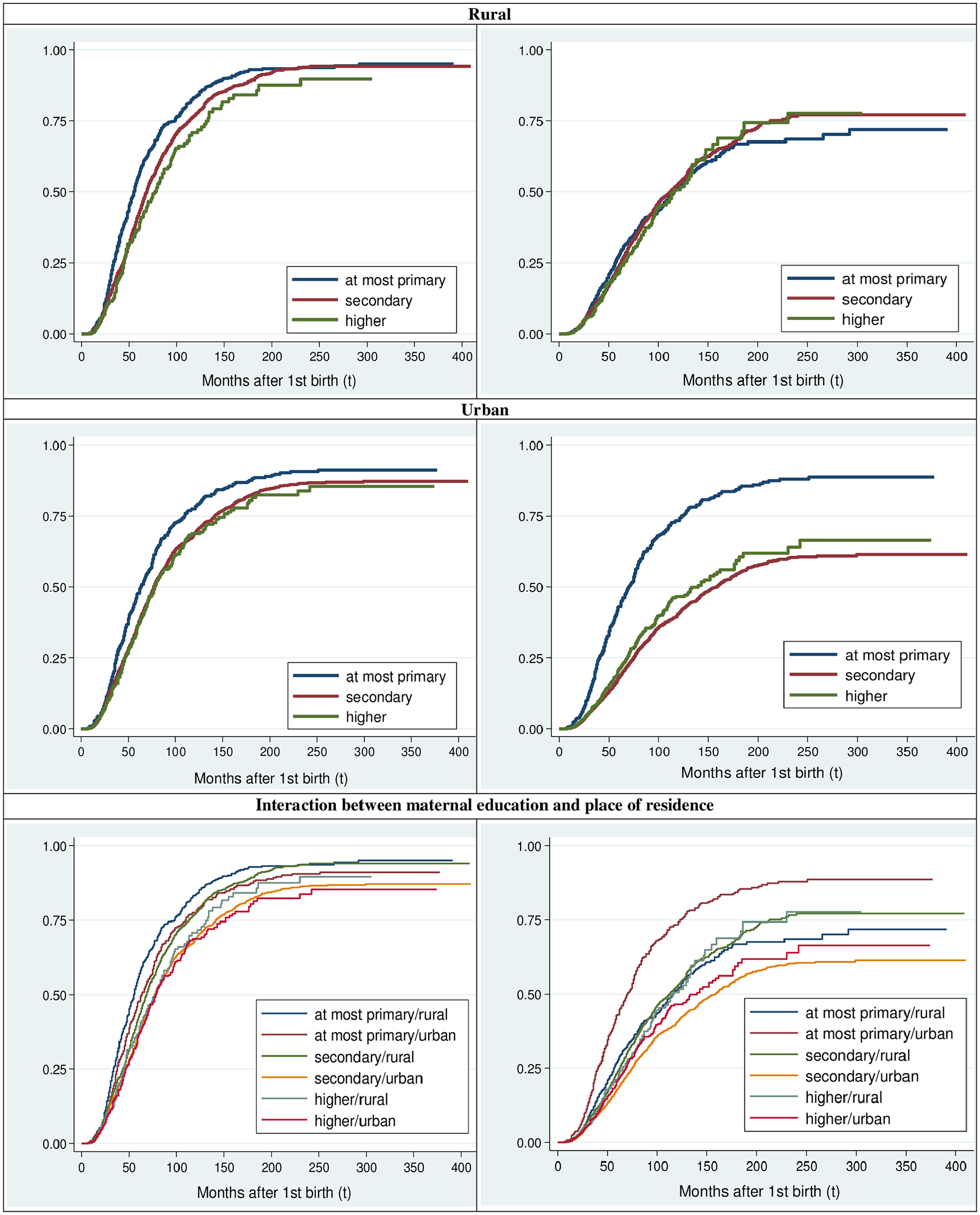
Hazard function of time to second birth by maternal education (left-panel, unadjusted; right-panel, adjusted) in rural and urban residence.
By and large, findings showed a significant longer average length of SbI among urban women relative to their rural counterparts (p < .001). Even when disaggregated by the categories of other characteristics considered, significant rural-urban differences in SbI were evident. For instance, the rural-urban differences in MtSb were observed among women who never married (rural—95% CI 74 [69, 80] vs. urban—95% CI 92 [86, 98] months, p ≤ .001), who were from low-wealthier households (rural—95% CI 63 [61, 65] vs. urban—95% CI 69 [64, 77] months, p = .007) or lived in Eastern Cape province (rural—95% CI 54 [48, 60] vs. urban—95% CI 78 [68, 88] months, p < 0.001). Meanwhile, nearly all the considered characteristics had significant (p < 0.15) differences in their respective survival curves category except for first-birth sex and survival of the first child in both settings (Table 2).
Influence of Maternal Education on Time to Second Childbirth by Rural-Urban Residence
Tables 3a and 3b respectively present unadjusted and adjusted hazard ratios of the influence of maternal education on second birth interval in both rural and urban contexts.
Unadjusted Hazard Ratios of Second Birth Interval by Maternal Education Among Rural and Urban Women.

HR = hazard ratio; 95% CI = Confidence interval; Ref = reference category; LL = log-likelihood; AIC = Akaike information criterion.
Adjusted Hazard Ratio of the Relationship Between Maternal Education and SbI According to Rural-Urban Residence and Their Pooled Sample.

aHR = adjusted hazard ratio; CI = 95% confidence interval; Ref = reference category; LL = log-likelihood; AIC = Akaike information criterion; n = number of observations; partners education variable was excluded in models 2 and 3 due to collinearity with marital status at first birth.
p < .001. bp < .01. cp < .05.
Rural women who had a secondary (HR = 0.79; 95% CI [0.71, 0.88]) and a higher (HR = 0.67; 95% CI [0.55, 0.82]) education respectively were 21% and 33% more likely to lengthen SbI relative to their rural counterparts who had at most a primary education. Similarly, women who had a post primary level of education (secondary—HR = 0.78; 95% CI [0.69, 0.88]; higher—HR = 0.74; 95% CI [0.63, 0.88]) were about 22% to 25% times more likely to delay second birth compared to those who had at most a primary education in urban setting. Relative to rural women who had at most a primary education, women who had at most a primary and lived in urban including those who had a post primary education irrespective of their residential abode were about 20% to 40% significantly more likely to delay second-birth (Table 3a).
These associations remained relatively alike when other socio-demographic factors were controlled for in rural or urban context. Relative to women who had at most a primary education, the risk of having second-birth was significantly lower among rural residents who had a post primary education (secondary—aHR = 0. 68, 95% CI [0.70, 0.82]; higher—aHR = 0. 62, 95% CI [0.62, 0.93]). A similar but reduced-lower likelihood of having second-birth was observed among urban women who had a post primary education (secondary—aHR = 0. 79, 95% CI [0.69, 0.90]; higher—aHR = 0. 80, 95% CI [0.66, 0.98]; model 1). For model 2, when all other significant variables were controlled for, women who had a secondary education were 14% more likely to delay second-birth in rural setting; however, maternal education was not significantly associated with SbI among urban women. For model 3, compared to rural residents who had at most a primary education, women who had a secondary education (rural—aHR = 0.87; 95% CI [0.77, 0.97]; urban—aHR = 0.79; 95% CI [0.69, 0.89]) or a higher education (urban—aHR = 0.82; 95% CI [0.86, 0.98]) were more likely to delay second-birth (Table 3b).
Other significant predictors of SbI were ethnicity, employment status, marital status at first-birth and desire for more children for both urban and rural residents. While factors such as wealth index and age at first-birth had significant relationships with SbI among women residing in urban areas, ethnicity was a peculiar factor associated with SbI among rural residents. Of these, age at first-birth of urban and women’s region of rural residents had time-varying effects on SbI. The chance of having second-birth increased with increasing age at first-birth. Urban women aged ≥25 years at first birth were 29% times more likely to shorten SbI at baseline; however, the likelihood declined by 1% at every unit increase in survival time relative to teenage mothers at first-birth. Whereas among rural residents, Eastern Cape and Kwazulu-Natal women respectively had about two times the likelihood of having second-birth at baseline, but declined by 1% for every increase in unit of time compared with their Limpopo counterparts.
Black/African women (aHR = 0.87; 95% CI [0.77, 0.99]) had a 13% lower tendency to shorten SbI compared to women of other race living in urban setting. However, Black women had a 31% lower risk of welcoming a second-birth among rural residents. Women who had their first births after cohabiting had about 44% higher risks of having a shortened SbI among rural residents, but 79% among urban residents, than those who never married. Relatively, women who were working had about 15% lower likelihood of having a second-birth irrespective of their place of residence (rural—aHR = 0.87; 95% CI [0.79, 0.96]; urban—aHR = 0.83; 95% CI [0.76, 0.91]). Urban women who were from wealthier households had a 18% reduced risk of having a second-birth, but not for rural residents. Although women who formerly or currently used contraceptives had a lower nonsignificant likelihood of having a second-birth at baseline, the likelihood significantly increased by 0.5% for every unit increase in survival time for both settings (Table 3b).
Discussion
The present study investigated the influence of maternal education on first to second childbirth interval by residence amongst women in South Africa using 2016 SADHS nationally representative data. The proportion of the women who had a second-birth was lower in urban compared to rural. Even though a lengthened SbI compared to the optimal inter-birth interval of 3 to 5 years (World Health Organization, 2007) was observed in both settings, it was significantly longer in urban. The SbI is longer among the women studied compared to the median birth interval of 55 and 56 months (though confined to non-first births in the 5 years prior to the survey year) respectively among rural and urban sub-populations in South Africa (NDoH et al., 2019).
These results suggest a considerable difference in SbI between South Africa women residing in rural and urban areas. Urban women, essentially, have a higher tendency to increase SbI than those in rural. Similar result has been reported in other studies (Ahammed et al., 2019; Yohannes, et al., 2011) that women from rural areas were more likely to have a second birth relative to their urban counterparts. The observed differential may be attributed to the heightened costs of childbearing in urban relative to rural settings (Lerch, 2018). Besides, the difference could be due to disparities in the women’s residence-specific socio-economic and demographic characteristics. For instance, a higher percentage of rural women were unemployed, from low-wealthier households, lived in Eastern Cape and Kwazulu-Natal provinces or had at most a primary education compared to their urban counterparts in this study. This comparative differential of the rural and urban SbI’s lengthening demonstrates the impact of urbanization on fertility transition.
The role of non-optimal inter-birth intervals as a critical risk factor of poor maternal and child health outcomes is negatively related to maternal education (Molitoris et al., 2019). Saliently, the study suggests that rural women who had a secondary education were more likely than those who had at most a primary education to have a longer SbI. This finding remained rather similar after controlling for other correlates among rural residents; this may suggest that maternal education influence on SbI is relatively independent of a collective effect of other correlates among rural women. On the other hand, the effect of maternal education on SbI substantially changed while controlling for other variables. This indicates that maternal education alone may not have contributed to the relative lengthened SbI among urban women. This differential aligns with earlier literature (Ahammed et al., 2019; Kim, 2003; Klesment et al., 2014). Educational attainment affords women the opportunity of non-childbearing activities access. Unlike in urban, the rural’s SbI pattern is not surprising for educated women are more likely to postpone marriage, use contraceptives and desire no more children (Olatoregun, et al., 2014). This could partly be explained from the point of view that an increased in educational attainment promotes women’s social and economic status. Addressing poor maternal and childbirth outcomes due to non-optimal birth interval would therefore require women empowerment through education, especially in rural setting.
After adjusting for the effect of other variables, ethnicity, employment status, marital status at first-birth and desire for more children significantly impacted on SbI in both residential contexts. Generally, a poor level of education could induce unemployment, poor wealth status and consequently impact on SbI. Being employed is a significant factor of SbI in that employed women were less likely to have a second birth in both the rural and urban settings. This is in line with the existing theory that wage employment or career generally has a delaying impact on women’s fertility transition (Benzies et al., 2006). The result, however, disagrees with a previous study (Levin et al., 2016) which opined that employed women were more likely to have a second childbirth.
Black/African women were less prone to having a second childbirth either in rural or urban relative to other ethnicities. Of note, rural and urban Black/Africans respectively were about 31% and 13% times more likely to delay a second-birth. This suggests urban Black/Africans proceed sooner to have a second childbirth relative to their rural counterparts. This could partly be explained by ample apartheid government policies that favored Whites -most of whom lived in urban-fertility in South Africa (Palamuleni et al., 2007).
A high percentage of women who had a second-birth may suggest that most women had already attained their desired fertility, for nearly 60% of the women desired no additional child(ren). Hence, the early second-birth and subsequently, the shortened SbI among women who neither decided nor desired to have more children as observed in both settings. Other likely reason may be ascribed to the increased in proportion of women with an unmet need for contraception in the last two decades, as documented in the 2019 SADHS report (NDoH et al., 2019). Another plausible explanation could be that a high proportion of teenage mothers who may be unwilling to raise another child, due to economic and psychological effect of having the first child before marriage, may rescind the decision afterwards. Perhaps, this contracts the belief that a culture of early sexual intercourse has a higher tendency of producing many children linked with shortened birth intervals (Fitaw, et al., 2003). Policies aimed at addressing non-use of contraceptives, contraceptive discontinuation and failure, and by extension, the unwanted births are therefore required.
Furthermore, marital status had a significant impact on SbI in that women in a relationship (married or cohabiting) were more likely to have a second birth relative to never-married women in both settings. This finding aligns with earlier literature (Fagbamigbe et al., 2020). The plausible explanation could be that married women are at a greater risk of exposure to sexual activity and pregnancy that could lead to accelerated second childbirth. More so, about half of the South African women who had at least a child were never married; this could lead to lengthened SbI as having a second child might be delayed until marriage.
However, the results of a few predictors of SbI that are peculiar to each of the residences imply some contextual impacts. Among urban women, age at first-birth significantly influenced SbI as older women were more likely to welcome a second childbirth. The reason could partly be due to the non-attainment of desired parity (De Jonge et al., 2014; Mcguire & Stephenson, 2015). The implication of this may be associated with the fact that women who have not attained their preferred family size are more likely to long for a second childbirth (Yohannes et al., 2011). This corroborates findings from other sub-Saharan countries like Ethiopia, Uganda, and Zimbabwe (Hailu & Gulte, 2016; Mcguire & Stephenson, 2015) which claimed older women were more likely to welcome second childbirth.
Similarly, increasing household wealth lengthened SbI in urban areas. This suggests that time elapsed between first and second-birth is significantly influenced by the availability of financial/material resources. This finding corroborates the claim of other empirical studies (Hailu & Gulte, 2016; Yohannes et al., 2011). A plausible explanation could be attributed to the accessibility to health care services and information relating to the implication of shorter inter-birth intervals on women and child health, which may motivate the women to delay a second-birth. This buttresses the importance of women empowerment through education and employment as a means of improving economic status which may affect SbI.
In rural area, on the other hand, women who lived in the provinces of Eastern Cape or Kwazulu-Natal had a significantly shorter SbI compared with their Limpopo counterparts, though the effect subsequently declined over time. The finding of significant fertility changes in the two provinces is corroborated by an earlier study (Chersich et al., 2017).
Contraception used to delay childbirth has been reported in literature as a positive predictor of lengthened inter-birth intervals (Towriss & Timaeus, 2018). However, this study demonstrated a nonsignificant opposing association between contraception and SbI in the two settings. While the use of contraceptive is protective against shortened SbI among rural women, contraceptive use among urban women portend to shorten SbI. The nonsignificant result may be linked to the fact that nearly 80% of the women used contraceptive in both settings. Although, such contraception may be discontinued. According to NDoH et al. (2019), the rate of contraceptive use discontinuation is 29% within 1 year after commencement.
Meanwhile, this study is not without limitations. First, the study design is cross-sectional. The analyzed variables can only provide evidence of a statistical relationship but not a causal relationship between the variables and time to second birth. Second, there may be a possibility of recall bias as the survey entailed self-reported data without any means of verification. Also, the usage of secondary data limited our potential to sufficiently assess the influence of some characteristics like breastfeeding practices, abortion rate, and first birth interval length as drivers of second birth interval. Nonetheless, the study has been strengthened using the most recent large nationally representative dataset. Besides, the strength of the work includes provision of information on how maternal education impacted on SbI in both rural and urban residential settings, which is rarely documented.
Conclusion
Knowledge of the SbI is not only critical at directing the subsequent childbearing experiences but also at improving maternal and child health. The information is valuable and important to policy and decision makers in making informed decisions on the direction of future fertility patterns at sub-national population levels. A longer SbI was observed among urban women relative to their rural counterparts, though a longer duration of SbI compared to the optimal birth interval length is evident in both settings. The findings demonstrate residence context-specific differential in maternal education effect on SbI among South African women. Increasing maternal education is negatively associated with SbI in rural; however, education may not have distinctively influenced the relative lengthened SbI among urban women. Other considerable predictors—ethnicity, marital status at first-birth, desire for more children, and employment status—have been identified to impact on SbI in both settings. While being older at first-birth could shorten the SbI among urban women; rural women living in Eastern Cape or Kwazulu-Natal province may welcome a second childbirth early. The SbI’s differential between the residential contexts should be addressed by strengthening the health education systems. These may have a far-reaching impact on women’s socioeconomic empowerment and adherence to the optimal inter-birth interval, and consequently an improved maternal and child health.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440221079920 – Supplemental material for Influence of Maternal Education on Second Childbirth Interval Among Women in South Africa: Rural-Urban Differential Using Survival Analysis
Supplemental material, sj-docx-1-sgo-10.1177_21582440221079920 for Influence of Maternal Education on Second Childbirth Interval Among Women in South Africa: Rural-Urban Differential Using Survival Analysis by Rotimi Felix Afolabi and Martin Enock Palamuleni in SAGE Open
Footnotes
Acknowledgements
We acknowledge the National Demographic and Health Survey’s supervisory bodies in South Africa for granting us access to the data used for our study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.