
Abstract
The aim of the paper was the validation of a psychosocial assessment tool for determining willingness to participate in child-centered safety promotion interventions, specifically in a low-income community in South Africa. A study was conducted as part of the initial validation to test the items and format the questionnaire. The instrument was then administered to Afrikaans speaking individuals in a community in the Western Cape. Iterative exploratory factor analysis was conducted at both the item and scale levels to select and reassign items and scales to determine the final composition of the questionnaire. The findings indicate that the instrument measures seven factors, namely incentives; priorities and community needs; perceived benefits; social approval; accessibility and values; altruistic capital; and community cohesion, which represents salient dimensions of the construct willingness to participate in interventions. The questionnaire and its subscales displayed acceptable to good reliability, with Cronbach’s α ranging from .55 to .80. Since willingness precedes actual participation, it is argued that insight into the factors that relate to willingness to participate provides an avenue for motivating actual participation.
Keywords
South Africa has high rates of violence and injury (Seedat et al., 2009) with children a particularly vulnerable group, exposed to violence and injury in the home, school, and broader community (Burton, 2006; Seedat et al., 2009). Those in impoverished settings experience the greatest burdens of violence and injury (Kaminer & Eagle, 2010). In such settings, reducing the injury risk of children and youth is a key public health challenge. Thus, early intervention is an important strategy for promoting the well-being of children, families and communities. Public health interventions may encompass a range of modalities, that involve mechanisms directed at the individual, family, community, societal, or physical environments. The interventions that refer to strategies or programs that engender knowledge, attitude or behavior change to improve the health status or safety among individuals or an entire community or population are of particular importance in community safety research (Taliep et al., 2017).
Safety promotion interventions, including those specifically focused on violence and injury prevention, remain fraught with complexities and challenges, and are also often delayed in their effects (Peden et al., 2008). Multiple factors account for the lack of efficaciousness and sustainability of interventions. One of them is the willingness of participants, or lack thereof, to engage or participate in interventions. Shaughnessy (2013) defines the construct willingness to participate as the predisposition to engage or act voluntarily in intervention programs or organized scientific inquiry (research). Moreover, the construct willingness to participate can be viewed as encompassing two corresponding elements namely, enablers of participation and inhibitors to participation (Ismail, 2018).
A dynamic and context-specific understanding of the psychosocial inhibitors to and enablers of child-centered safety promotion interventions is required to ensure their effectiveness (see Mendez et al., 2009; Stallinga et al., 2014; Swartz et al., 2006). The hypothesis is that participation in an intervention is expected to occur when intervention-related needs outweigh perceived intervention-related inhibitors (Ismail, 2018). However, if perceived inhibitor effects are cumulative, individuals may not participate in an intervention, even if the need exists for the intervention. There has been a growing body of research that highlights the role socio-cultural factors, environmental factors, personal factors, and others, may play in impeding or fostering intervention participation and retention (Ismail & Van Niekerk, 2020; Kafaar, 2015; Lesch et al., 2006; Orrell-Valente et al., 1999; Sahay et al., 2005; van Niekerk & Ismail, 2013).
Research findings have indicated the critical importance of participation for positive outcomes of interventions (Heinicke et al., 2001; Ramey et al., 1992). Despite this, evaluation studies have indicated that the lack of participation of individuals in interventions is problematic, with about 80% of prospective participants in communities declining to participate (Hopp et al., 2006; Subramanian et al., 2004). Lochman (2000) and Spoth and Redmond (2000) assert that low rates of participation often threaten the internal validity (namely, demonstrating intervention impact on specified outcomes under “ideal conditions”) and external validity (namely, generalizability, applicability, transferability, and extrapolation of the outcomes) of interventions, particularly when their effectiveness has previously been recognized. Therefore, if the external and internal validity of an intervention is compromised, the potential benefits of the implemented intervention may be affected. According to the World Health Organization (WHO, 2001), participation is a key predictor of health and well-being outcomes. The concept and assessment of both individual and community willingness to participate in an intervention affords an opportunity for meaningful reflection and amendments of intended interventions prior to implementation (Beebe et al., 2001; Edwards et al., 2000; Ogunrin et al., 2018; Stallinga et al., 2014).
The challenge, though, is to develop interventions and assessment instruments that are locally and contextually relevant. According to Nastasi and Hitchcock (2009), interventions have exhibited promising outcomes when utilizing culturally-sensitive measures. In South Africa, with its diverse cultural make-up, there is a growing recognition of the importance of culturally appropriate or relevant assessment measures.
Rationale
Currently, there is no standardized tool available to measure the willingness of community members from low-income settings to participate in child-centered safety promotion interventions. It would, therefore, be invaluable to develop an accessible and user-friendly tool for the South African and perhaps other similar populations, that assesses the level of community members’ willingness to engage or participate in safety interventions.
The development of a new instrument will address three shortcomings of existing willingness to participate measures: (a) the questionnaire will be the first known generic instrument developed that can be utilized for safety interventions; (b) the conceptualization of the construct willingness to participate with regards to safety promotion interventions will provide the groundwork for further research; and (c) the resultant questionnaire will aid researchers and intervention developers to ascertain not just overall levels of willingness to participate, but also specific psychosocial inhibitors and enablers that can be targeted to enhance intervention outcomes.
Such an instrument can play a critical role in assisting practitioners, researchers, and organizations enhance programmatic outcomes, and may contribute to the long-term sustainability and ownership of interventions in these communities. Considering the above-mentioned, the principal aim of the study is to evaluate the factor structure and internal reliability of a willingness to participate measure.
Conceptual and Theoretical Framework
Validation within the process of instrument development is of critical importance within a multicultural South African context to furnish an assessment tool that is culturally and linguistically relevant. The psychometric procedures within the current study were framed by Validation Theory (Rust & Golombok, 2009; Waltz et al., 2010).
Method
Study Setting and Design
Broadlands Park, also known as Tarentaal Plaas, is situated in the Helderberg Basin about 4 km outside of Strand in the Western Cape, South Africa. This is an under-resourced community consisting of low-cost government housing and backyard dwellings. The community has been in existence for 19 years, with community members previously located in nearby informal settlements and backyard shacks (Bulbulia & Van Niekerk, 2012). This community is predominantly an Afrikaans speaking community, and under South Africa’s previous racialized legislation would have been classified as a “colored” 1 community. Broadlands Park covers roughly 2.2 km2 radius (Statistics South Africa, 2011) and consists of 1,162 houses and 126 shacks, approximately 8,234 residents, comprising 5,534 adults and 2,700 children. The community has limited infrastructure, with 16% of the residents living in informal dwellings, and close to 30% of the adult population unemployed (The Unit for Religion and Development Research, 2001). The average income per household in Broadlands Park ranges from no income to R2124 per month (The Unit for Religion and Development Research, 2001). Most residents have not completed a secondary education, with the result only 6% of adults 20 years and older have no formal schooling. Those individuals who are employed are involved in either skilled, semi-skilled, or domestic work. Despite Broadlands Park being a designated member of the International Safe Communities Network in 2006, the community continues experiencing a high incidence of both intentional and unintentional injuries (The Unit for Religion and Development Research, 2001). Gangsterism, drug and alcohol abuse, and other psychosocial challenges are experienced in the community daily.
Sample
The assessment measure was administered to a sample of 375 community members (i.e., fieldworkers and household members). An attrition rate of 7.4% resulted in a final sample of 349. This resulted in a subject to variable ratio of 1:7 in the 46-item assessment tool developed.
The Instrument
A mixed-methods approach was utilized to develop the new measure, and included content validation, item generation, and initial validation processes (see Ismail, 2018; Ismail & Van Niekerk, 2020). A literature review was conducted as one of the data gathering tools to inform the conceptualization of the construct. In particular, the review scope focused on studies defining willingness to participate, theoretical frameworks of the construct, assessment of willingness to participate and studies related to inhibitors, and enablers of willingness to participate (Ismail, 2018). Subsequently, community engagement and individual interviews with community members related to inhibitors and enablers of willingness to participate were conducted. Nominal Group Technique discussions were conducted with various role-players in the relevant communities to inform the development of the instrument, while participatory methodologies were utilized to conceptualize the instrument in relation to psycho-social factors associated with intervention participation, with these categorized according to core dimensions (see Ismail, 2018; Ismail & Van Niekerk, 2020). A large pool of 64 items was constructed based on the indicators that were extrapolated from the literature, the data collected from the individual interviews and from the nominal group discussions (reflecting various inhibitors and enablers of willingness to participate). Psychosocial inhibitors and enablers included personal, relational and environmental factors as well as structural, physical, and social constraints. A detailed description of these inhibitors and enablers can be found in Ismail and Van Niekerk (2020). An expert in the field of test construction provided support throughout the item construction process. A Delphi method utilizing an expert panel reviewed items for relevance, difficulty, and ambiguity, with items subsequently amended or removed. In the final round panelists had to judge the content validity of the draft version of the questionnaire by rating items in terms of: how it related to the indicator; whether the response format was applicable or not; and whether items should be retained or removed. Item selection procedures were conducted on the English version of the instrument and these results were applied to the Afrikaans version (see Ismail, 2018; Ismail & Taliep, 2020). Figure 1 below provides an overview of the process, and the various phases in the development of the willingness to participate instrument.

Methodology process steps: Overview of phases and objectives of the study.
The newly developed Willingness to Participate Questionnaire (WTPQ) consisted of 58 items. Twelve of these items were used to obtain demographic information from participants relating to their age, relationship status, living situation, education, employment, and income. The remaining 46 items (44 items met inclusion criteria, 1 item was recommended to be removed but was retained for the validation phase, and 1 item was added on recommendation by the Delphi Panel Review) measured willingness to participate. The 12 demographic items were standard demographic questions in assessment tools and were thus not subjected to the same validation process as the 46 items measuring willingness to participate (see Figure 1). The WTPQ was intended to be a self-report measure with closed-ended responses. The first draft of the questionnaire comprised only the one Likert scale, that is, “very willing,” “somewhat willing,” “would not affect my decision either way,” “somewhat unwilling,” and “very unwilling.” However, this response format constrained how statements had to be phrased and eventually answered by the participants. Based on the consultation with the experts, alternate response formats were included ranging from: somewhat willing to very unwilling; disagree to strongly agree; and rarely to always.
Data Collection Procedure
The study received ethics approval from the Department of Psychology’s ethics committee at the University of South Africa. Participants for this phase of the study were recruited from November 2016 to March 2017. Participants were recruited from Broadlands Park. Initially, all Broadlands Park households were mapped from Google maps and all addresses captured into an excel file. The households mapped comprised of 1,014 addresses, and did not include backyard dwellings. Thereafter, the mapped households were split into five zones (see Figure 2, Broadlands Park Map) prior to randomization.

Broadlands Park subdivided into color-coded zones.
The Broadlands Park civic association approved the study and made themselves available if assistance was required. Subsequently, community members in Broadlands Park were identified and invited to apply for five vacancies as data collectors in the current study. Potential applicants went through an interview and selection process, and once successful were given training on interpersonal skills, conflict resolution management, communication skills and how to administer the questionnaire. The successful data collectors consisted of 2 females and 3 males, and each was assigned with administering 75 questionnaires. Four of the data collectors were from the area, while one data collector was from outside the area. During the initial training, data collectors were given a map of the area subdivided into zones (see Figure 2) allocated to them for easy reference as well as a list of addresses for them to invite potential participants.
Figure 2 provides a visual representation (map) of Broadlands Park and the subdivided zones for data collection that were provided to the data collectors as part of their information pack.
Data collectors then invited randomly selected participants from the households selected on an individual basis, outlining the research aims, expectations for involvement and ethical issues related to participation. Data collectors were briefed before the recruitment process. If the potential participant turned down the opportunity to participate, data collectors were advised to thank the individual for their time and continue to the next address on their list. The data collectors were also advised that if at any time they felt unsafe they should immediately terminate data collection for the day and leave the area.
Once invitations were successful, data collectors provided the first author with a list of 400 prospective participants’ names, addresses, and contact numbers. Subsequently, the first author called prospective participants to confirm interest, briefed prospective participants and invited them to enroll on the study. Of the 400 prospective participants, only 375 agreed to participate in the study. The data collectors thereafter provided these 375 participants with a consent form, an information sheet and contact details. The first author was available to answer all questions participants had about the study as well as provide feedback once the study had been completed.
Once the consent form was signed, the data collectors collected the sheets and either administered the questionnaire at the same visit or scheduled an appointment to administer the questionnaire at a more convenient time. The data collectors administered the questionnaire to the participants at their homes.
The completed consent forms and questionnaires from the data collectors were collected on a bi-weekly basis. During these collection meetings, the first author would check up on how the process was going as well as conduct quality checks to ensure the consent forms and questionnaires were completed correctly. A WhatsApp group was created with the data collectors and was specifically developed for communication daily. The data collectors could also utilize this platform of communication in case they had urgent matters to discuss or raise certain concerns or questions with me.
Data collection occurred over 2 months with a total of 349 completed questionnaires. All participants of the pilot test received a R50 ($3.41) grocery voucher for participating and as part-compensation for their time spent in the study. Data collectors were also compensated for their time and effort put into the collection of the data.
Data Analysis
The 349 questionnaires were captured in a data file to prepare the data for analysis. The questionnaires were captured in the Microsoft Office Excel Program. The raw data were then cleaned and coded and sent to an external evaluator to verify whether items were captured correctly or erroneously. All the questionnaires were filed according to the data collectors and zones within which the questionnaire was administered. This allowed for easy access to check if suspected errors were discovered. Once the external evaluator verified the data, the data was checked once again by the lead author and converted into an SPSS file to prepare for analysis.
Factor analysis
The method used for evaluating the factor structure of the draft version of the WTPQ was the statistical technique of exploratory factors analysis (EFA) at item-level using the Statistical Program for the Social Sciences (SPSS, version 24.0) package. The motivation behind utilizing EFA is to identify a latent subset of characteristics or factors that underlie a specific domain (Schaap & Vermeulen, 2008). EFA is considered appropriate when the objective is to determine the initial factor structure (dimensions) of a new measure when the factor structure is unknown or cannot be theoretically hypothesized (Dimitrov, 2012).
A preliminary exploratory factor analysis was conducted with the final item pool to identify the underlying latent constructs existing in the draft version of the measure. A common factor analysis method of extraction was employed. Since an a priori factor structure was not employed, the use of a scree-plot and the EFAs eigenvalues to determine how many factors to retain, was included. An oblique rotation was decided upon, as it produces correlated factors facilitating easy interpretation (Hair et al., 2010). An oblique rotation was employed because the literature suggests that one is likely to discover a relationship between factors (Cummins, 2000).
An examination of the Pattern Matrix table was the next step. To consider the relative contribution of each item to a factor, a strict critical value of 0.30 was employed (refer to Hair et al., 2010). Items that loaded on more than one factor was regarded as poor items, and at least three items should load on a factor for it to be considered a stable factor.
Determining preliminary internal reliability
The reliability of an assessment tool refers to the extent to which it consistently and accurately measures a construct. The concept of reliability is grounded in two fundamental considerations: (1) do items in a single measure actually assess a single construct? and (2) do measures assessing a single construct produce consistent estimates of that construct across multiple measurements? (Hair et al., 2010).
To investigate the reliability of the preliminary assessment measure, the internal consistency of each subscale, as well as the entire measure, was evaluated. This allowed for the consistency of responses of all items in the measure to be assessed. Internal consistency reliability for the preliminary assessment measure was explored utilizing the Cronbach’s alpha to ascertain the number of items and their strength of inter-correlations. For the present study, reliability co-efficient above .70 was regarded as displaying good reliability (Nunnally, 1978).
The item-level analyses considered the item discrimination of each item and were computed using inter-item correlations. Item discrimination refers to the degree to which an item can differentiate among participants (DeVellis, 2012). The item-total correlation value is a reflection of how well items measure what they are intended to measure. Correlations that exceed .70 suggest item redundancy, while correlations less than .20 suggest the item is measuring an entirely different construct (Streiner & Norman, 2008). A critical value of .30 was utilized to evaluate the items. Items below .30 were removed from the scale as it indicated that the item did not correlate well with the overall score (Hair et al., 2010).
Results
It was important to conduct frequency checks on the data to screen for missing values, prior to conducting the factor analysis. The frequency tabulations indicated that the amount of missing data was negligible at 0.03% overall. Field (2009) purports that excluding cases listwise if it does not result in a massive loss of data is the best option. Since the missing data was negligible at 0.03% it was decided to exclude cases listwise. The variable-to-participant ratio (1:7) was sufficient and would not affect the number of cases processed during factor analysis.
Compliance With Specific Assumptions
A normal distribution curve indicated that the data sampled is slightly skewed to the right, but still falls within a normal distribution curve. The sample size of 349 was considered adequate for factor analysis. Furthermore, the subject-to-variable ratio of 1:7 falls within the recommended criteria for conducting exploratory factor analysis (Tabachnick & Fidell, 2007). The KMO statistic (0.79), the anti-image diagonal (above 0.5 for all variables) and the Bartlett’s test of sphericity (χ2 (1,035) = 4,536.969, p < .00) provided evidence that there were sufficient inter-correlations and common variance between variables, and that the current data set met the assumption of factorability of the data and was appropriate to conduct a factor analysis on this data.
Results of the Exploratory Factor Analysis
The results from the eigenvalues and scree-plot did not produce a clear and unambiguous interpretation, with nine factors displaying eigenvalues greater than 1, and the point of inflection on the scree-plot occurring at either Factor 2, indicating a 1-factor solution or Factor 8, indicating a 7-factor solution. Thus, inspection of the items and their loadings on each factor to select the number of stable factors to retain was utilized. Table 1 below provides an overview of the common variance explained for the factors extracted during the first round of factor analysis.
Total Variance Explained for the First 20 Factors.

Note: The blue shade indicates the eigenvalue of the factors.
Factor loadings that were 0.30 and above were considered significant (Hair et al., 2010). A factor also required a minimum of three significant loadings to be considered a stable factor.
The initial factor analysis yielded a 7-factor solution. Based on the aforementioned criteria seven factors were extracted, each having a minimum of three items loading on a factor. The subsequent EFA was conducted on all 46 items based on the 7-factor solution that emerged from the initial EFA. This round of EFA identified 12 items that failed to significantly load on any factor (items 13, 15, 28, 30, 32, 33, 34, 37, 40, 41, 42, and 43). These items were removed before conducting a final round of EFA (see Table 2 below).
Factor Loadings for the EFA With Direct Oblimin Rotation Pattern Matrix With a Stipulated 7-Factor Solution.
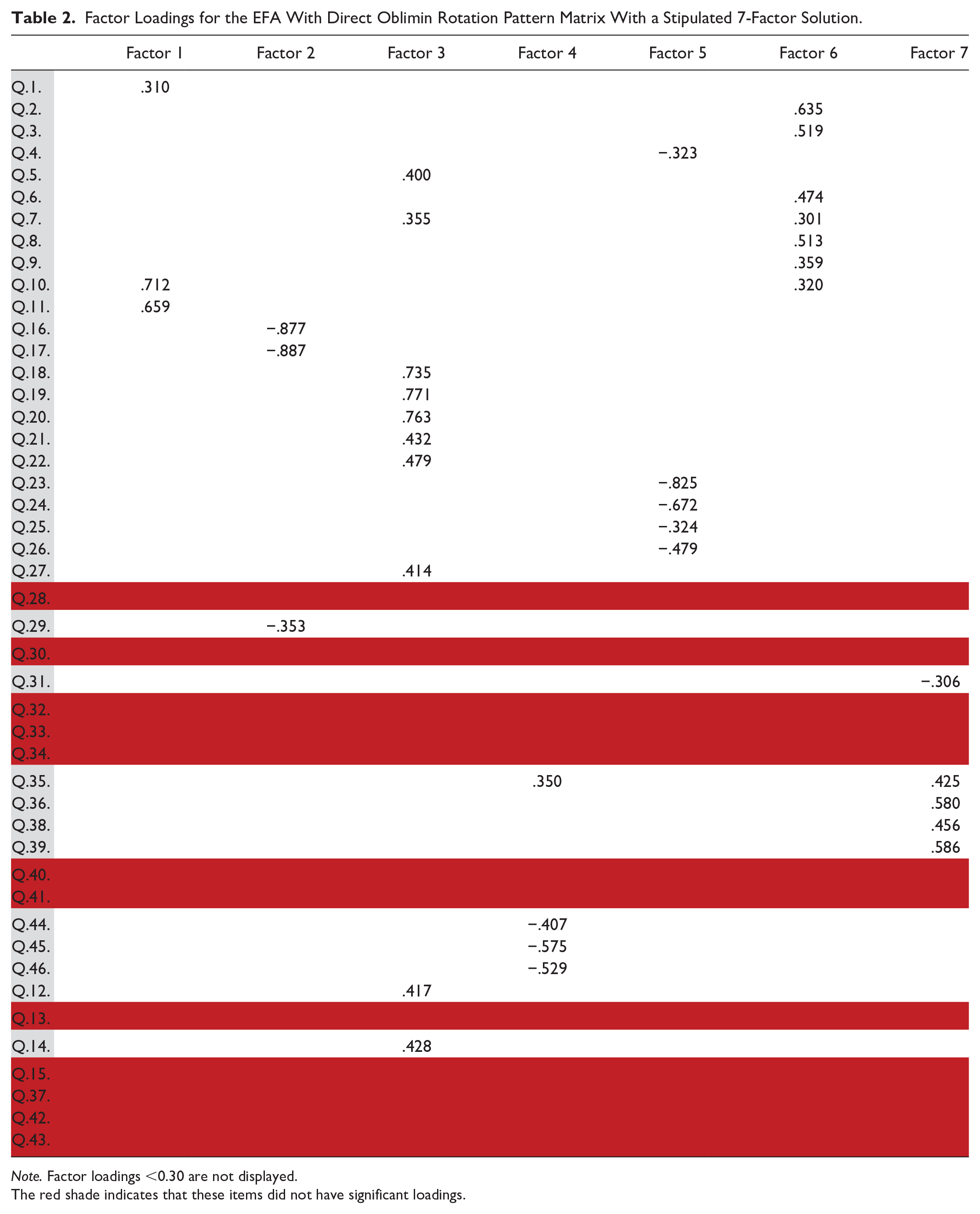
Note. Factor loadings <0.30 are not displayed.
The red shade indicates that these items did not have significant loadings.
In this round of the iterative EFA process the same parameters were specified and only one item failed to significantly load on any factor (item 1). Item one was removed for the final 33 item scale (see Table 3). As is evident, this round of factor analysis produced the same factor structure as the previous round of factor analysis. The model explains 39.9% of the common variance between items.
Factor Loadings for the EFA With Direct Oblimin Rotation Pattern Matrix of the Third Round After All Seven None Loading Items Have Been Removed.

Note. Factor loadings <0.30 are not displayed.
The red shade indicates that these items did not have significant loadings.
Thus, a 7-factor solution was extracted, each having a minimum of three items except factor 5. Factor 1 consisted of 5 items (item 4, 23, 24, 25, and 26), Factor 2 consisted of 3 items (item 16, 17, and 29), Factor 3 consisted of 10 items (item 5, 7, 12, 14, 18, 19, 20, 21, 22, and 27), Factor 4 consisted of 3 items (item 44, 45, and 46), Factor 5 consisted of 2 items (item 10 and 11), Factor 6 consisted of 5 items (items 2, 3, 6, 8, and 9) and Factor 7 consisted of 5 items (item 31, 35, 36, 38, and 39). These items were considered the final items in the overall scale and the extracted factors represented the subscales.
Factor Structure and Labeling the Factors of the WTPQ
The final version of the questionnaire following the factor analysis comprised of 33 items and 7 subscales. The factor number and the label assigned, the item number in the questionnaire and a brief description of the question is presented in Table 4. Items that loaded significantly on Factor 1 were related to perceived benefits and this factor is therefore named accordingly. Factor 2 is labeled incentives as the items that loaded on this subscale all related to attributes of incentives for participation in interventions such as food and cash vouchers. Factor 3 is labeled priorities and community needs as the items that loaded on this subscale referred to, either priorities faced by community members both in their personal capacity and as an active community member, or to participants concern over their community and how interventions needed to be contextually relevant. Items that loaded significantly on Factor 4 were all related to community connectedness, and as a result, we labeled the factor lack of community cohesion. The two items that loaded on Factor 5 dealt with approval sought from peer relationships so this factor is labeled peer approval. Even though the criteria for selecting stable factors were three or more items loading on a factor, we decided to retain the two-item factor. A single factor can have two items loading, if there are conceptual and or practical motivation supporting the retention of these two items. We labeled Factor 6 accessibility and value as the items related to convenience, user-friendliness, availability and value participants attach to child-centered interventions. Lastly, the items on the last factor referred to the unselfishness and generosity of individual community members and their sense of belonging, and so, we named the factor altruistic capital.
Description of Items and Factors.

The seven subscales or factors epitomize salient dimensions of the construct willingness to participate of community members exposed to child-centered violence and injury prevention and safety promotion interventions being implemented in their communities. The questionnaire has consequently been called the Willingness to Participate Questionnaire (WTPQ).
Assessing the Internal Consistency Reliability of the WTPQ
The internal consistency reliability of the WTPQ, and the internal consistency of each subscale, was evaluated. This allowed for the assessment of the consistency of responses of all items in the measure. The internal consistency of each of the subscales were assessed by means of calculating the Cronbach’s alpha. Cronbach’s alpha was calculated for the final subscales as well as for the entire measure as an indication of their psychometric properties. Based on this information, a decision was made to select the final items and scales for the WTPQ.
The Cronbach’s alpha of the entire questionnaire (32 items) and for each of the seven subscales were computed (see Table 5 below). The complete questionnaire displayed good reliability, Cronbach’s α = .76. However, the subscales displayed mixed results, with Cronbach’s α ranging from .55 to .80. Subscales 1, 2, 3, and 5 displayed good reliability with Cronbach’s alpha ranging between .70 and .80. Subscales 6 and 7 displayed adequate reliability with Cronbach’s alphas of .61 and .65 respectively. Subscale 4 displayed very poor reliability with a Cronbach’s alpha of .55. Whilst Anastasi and Urbina (1997) believe that a Cronbach’s alpha ranging between .80 and .90 is satisfactory, Nunnally (1978) asserts that a Cronbach’s alpha of .70 or more indicates good internal consistency.
Reliability Statistics of the WTPQ and Subscales.

Item analysis of the WTPQ was conducted on each of the seven subscales in order to assess whether individual items correlated with the score of each subscale respectively (see Table 6 below).
Inter-Item Analysis of the WTPQ Subscales.

Note. If item-total correlations are <.30 they are in red.
No items displayed corrected item-total correlations below .30 except for item 31 in subscale 7. This indicated that all items on the various subscales correlated with the score for the various subscales, with the exception of item 31. No subscales’ α value improved significantly when any item on a specific scale was removed, except item 29 in subscale 2. The alpha value increased from .71 to .89. Though, if this item was removed then this subscale would only comprise of two items. It was thus decided to retain this item as the overall measure displayed good overall reliability.
Discussion
The factor analysis revealed a 7-factor structure which accounted for 39.9% of the common variance in willingness to participate in child-centered initiatives. Thus, within the South African context, the construct willingness to participate incorporates the latent dimensions of: (1) perceived benefits, (2) incentives, (3) priorities and community needs, (4) peer approval, (5) lack of community cohesion, (6) accessibility and value, and (7) altruistic capital. These findings are analogous to those of another South African study, conducted by Fincham et al. (2010), which identified five latent factors that reflected willingness to participate, namely personal gains, stigmatization, safety and convenience, social approval and trust, and personal costs.
Factor 1, perceived benefits, refers to an individual’s perception of the positive consequences that will amass by engaging in a specific health-related behavior (Leung, 2013). This factor emerged as an enabler to the construct willingness to participate. Murphy et al. (2007) assert that perceived benefits should be regarded as relating to individual gains for the participants, which they believe may enhance the motives of intervention participants. Community members may be more willing to participate in interventions if they also realize that the perceived benefits may have multiple purposes that go beyond individual personal needs. The perception of benefits is often employed to explain an individual’s motives for adopting an intervention (Leung, 2013).
Factor 2, incentives, refers to conditions within the environment that promote participation (Mduluza et al., 2013). This dimension reflected the desire to benefit either personally or financially from participating in the interventions. The dimension included two items encompassing both specific financial incentives and non-financial incentives, also reported in other studies (e.g., Zurn et al., 2005), with the latter including the affirmation of participant-interventionist relationships (Gomby, 2007). The International Council of Nurses (Zurn et al., 2005) reports that incentives do influence participation and can be positive or negative, financial or non-financial, and tangible or intangible. Providing financial and or non-financial compensation for participation in interventions is however a controversial ethical issue. This factor, in particular the absence of incentives, was described as a barrier to willingness to participate.
Factor 3, priorities and community needs, was factorially complex as items measured two seemingly independent dimensions of willingness to participate. The first dimension of the factor, priorities, reflected concerns about having to prioritize specific social and domestic responsibilities especially those due to their impoverished conditions and limited resources. Community needs highlighted participant concerns about their community and how interventions needed to be contextually relevant. Participants indicated that they would be less willing to participate in interventions if these were not relevant to their context. Priorities can also be characterized as the multiple responsibilities that community members are faced with on a daily basis, typical for individuals living in impoverished communities. It is often difficult and overwhelming to juggle all these priorities, and van Niekerk and Ismail (2013) have postulated that such multiple responsibilities restrict engagement in safety promotion initiatives. Individuals with marginal resources also have less control over their work schedules (Ratele, 2012), which in turn affects other responsibilities. The salience of monetary concerns is likely to be driven by the high rates of poverty in this community. Similar concerns about priorities relating to time and financial challenges have been consistently cited as factors affecting willingness to participate (van Niekerk & Ismail, 2013).
Factor 4 is the lack of community cohesion that loaded significantly, and refers to the degree to which an individual or group is socially close, interrelated, and/or share resources with other individuals or groups (Durkheim, 1997; Yuksel & Turner, 2008). Community cohesion relates to encouraging positive relationships, which engender feelings of trust and belonging in communities; in turn this fosters individuals’ willingness to participate in initiatives (see Communities and Local Government, 2007; Fidzduff, 2007; Kim & Blieszner, 2017). In South Africa, community cohesion is reported to have emerged after the democratic transition post 1994 as a means of changing the political and economic landscape, and has been linked to, and often treated as synonymous with nation-building (Palmary, 2015). However, participants reported an overwhelming lack of cohesion in their community which they believed had an impact on community members’ willingness to participate in interventions. This was evident in the factor analysis where the factor related to community cohesion emerged as a barrier. Kawachi et al. (2004) assert that community cohesion and connectedness can be enhanced if community members participate in community activities which in turn fosters community involvement. Strong social bonds are needed for community members to mobilize and act on issues that affect them (Homan, 2010).
Factor 5, social approval, reflected the desire to receive social rewards for participating in interventions, such as approval from friends and family. Social approval suggests beliefs about what other individuals do, and what these individuals think we should do, in relation to a reference group (Mackie et al., 2015). It implies the social influence a peer group or community exerts on its individual members, as each member attempts to conform to the expectations of the group. Social approval guides an individual’s behavior in particular social settings (Mackie et al., 2015). In other words, the social reinforcement received by individuals has key implications for social behavior in that individuals will by and large consistently behave in a manner to gain approval and avoid criticism (Mackie et al., 2015). It is argued that the cumulative change in social approval toward participation in interventions by community members will result in subsequent behavioral change of the community (see Mackie et al., 2015). However, the results indicated that this dimension was factorially problematic as it comprised only two items that related specifically to seeking approval. Whilst a three item factor criteria was specified prior to the factor analysis, this dimension only rendered two items valid. We decided to retain these two items for both conceptual and practical reasons, aligned to previous literature, which indicates that once the scope of definition is taken into account, even single-item measures may suffice (Bergkvist & Rossiter, 2007; Drolet & Morrison, 2001; Wanous et al., 1997). In this study, participants were more likely to participate in interventions if their families, friends, and community reacted positively toward their decision to do so. To this extent, creating awareness around the purpose of the intervention and its benefits in addressing the identified social problem in the community may be associated with greater positive reactions by others (see Minch et al., 2017). Broader community awareness of the intervention is regarded as an essential enabling factor (Brown & Topcu, 2003).
Factor 6, accessibility and value, was also found to be factorially complex as items measuring two seemingly independent dimensions of willingness to participate loaded on the same factor. Accessibility, the first dimension of this factor, refers to “the opportunity that an individual at a given location possesses to take part in a particular activity or set of activities” (Hansen, 1959, p. 74). Accessibility highlights that participation in interventions need to be convenient and easily reached. The second dimension, value, connotes the worth participants attached to the child-centered interventions, and how positive perceptions of value would increase willingness to participate in these interventions. Value refers to the relative worth, utility, usefulness, or importance of something such as a quality, attitude, or method (Value, 1994). In this study, participants were likely or willing to participate in child safety initiatives if these initiatives were convenient and practical. The importance of the accessibility of interventions to potential participants was similarly identified by previous studies (see Mills et al., 2004). Participants stated that if interventions were to be implemented close in their community, community members would participate more willingly, with transportation costs then no longer a relevant factor, also reported in other studies (see Mills et al., 2004).
Factor 7, altruistic capital, is “an asset that enables individuals to internalize the effect of their actions on others” (Ashraf & Bandiera, 2017, p. 70). In other words, altruistic capital refers to the notion that every individual has an inherent aspiration to serve others. Ashraf and Bandiera (2017) argue that altruistic capital can increase or decrease depending on the individual’s intrinsic proclivity and the degree to which he or she functions in an environment that encourages the accumulation of altruistic behavior. Some participants reported a strong desire to act for the benefit of the community’s children by assisting in safety promotion efforts, thus endeavoring to improve safety for children in the community. This is consistent with other research that suggests that the need for an individual to act for the greater social good as opposed to individual benefit is one of the most frequently cited motivators for participation (George et al., 2015; Kafaar, 2015; Sahay et al., 2005). Although altruism emerged in this study as an enabler of own involvement, it may also be viewed as an enabler at the community level, where supportive and cohesive communities act for the greater good. It appears that participants’ altruism may have been driven by concerns about the high rates of child injury and violence in their community, and the related consequences, as experienced and witnessed by participants. Understandings of altruism within the South African context often align with the African philosophy of Ubuntu where the common good of society is placed before the good of any one individual (Venter, 2004).
In this study, the items under each dimension or subscale measure an essentially unidimensional trait, with these factors largely in accord with their corresponding theoretical constructs. With validity theory providing a framework to guide the thinking around the concept WTP and about the process of development and validation of a measuring instrument, it becomes possible to specify exactly which dimension of the construct the WTPQ is measuring. It is argued that specifying the different dimensions of a construct often paves the way for a more sophisticated understanding of what is to be tested (Babbie & Mouton, 2001). In this study, the internal consistency of the WTPQ was good (α = .76) with Cronbach’s alpha reflecting the proportion of common variance accounted for by the measure. Thus, the WTPQ accounts for 76% of common variance, supporting future use of this measure. Furthermore, the SEM (standard error of the mean) for the WTPQ was 10.8, meaning that an individual’s total score on the WTPQ should only vary by 10.8 points with repeated measure. Thus, if an individual receives a total score of 100/145, if repeated that individual’s score would fall between 90 and 110. Questions were formatted in such a way that the aggregate results from each category could create a score for ranking the willingness of people or communities to participate in interventions.
Conclusion
The construct validity of the WTPQ was examined employing EFA to evaluate the factors underlying the questionnaire’s items. Based on the study findings, the WTPQ is considered a reliable measure of the construct willingness to participate among community members in an under resourced community in the Western Cape, South Africa. The measure similarly displayed initial construct validity, as is demonstrated by the presence of seven latent factors that reflected various barriers and enablers of willingness to participate, generally aligned with those identified in the literature. These factors account for 39.9% of the common variance in willingness to participate.
However, while community cohesion or lack thereof was not found to directly influence or predict the construct willingness to participate in the literature, in this study it emerged as a latent factor. The experiences of community members from high-income countries may differ from those from economically low- to middle-income countries, such as South Africa. Thus, it would seem that contextual considerations may impact willingness to participate and thus must be taken into account before the implementation of interventions. The study thus provides further insight into the willingness to participate of community members in low-income settings by highlighting: the role that context can play and how the seven factors from this analysis may impact willingness to participate. These findings aligns with previous research that purports the multi-dimensionality and context-specific nature of the construct.
The subsequent criterion against which the WTPQ was evaluated was reliability. In the initial findings the WTPQ was found to be internally consistent and reliable in measuring the construct willingness to participate across time, advocating future use of this measure. However, the WTPQ subscales were found to have mixed results, with only four subscales comprising of good internal consistency. In general, the study yielded promising evidence of reliability and validity for the WTPQ. Upon further refinement, this measure could be utilized as an effective tool for the assessment of willingness to participate in safety promotion intervention programs.
Limitations
The WTPQ is a newly developed measure still in its infancy stages, so the diversity of interventions that could be responded to has not been accounted for in the questionnaire. Thus, varying interventions may have a differential impact on willingness to participate. Even if the WTPQ is administered across the entire population, it may still have a differential impact, greater for some communities than for others. In the current study, the WTPQ administered was only in Afrikaans, which may have influenced the internal consistency of certain of the scales, as is evident by some of the lower Cronbach’s alpha scores. As a result of the language diversity in Broadlands Park and the preference for English as a second language, it was felt that administering an Afrikaans questionnaire to community members would be appropriate if the data collectors explained problematic concepts or terms that participants might have encountered. The WTPQ is a newly developed instrument that has been subjected to initial validation methods. As a result, none of the limitations are considered to be serious or affecting the validity and reliability of the study. However, it is important to note that, validation is a continuous process.
Recommendations
Ideally, further validation studies are needed for the WTPQ and its subscales, as this was beyond the scope of the broader study. In particular, externally validating the WTPQ is recommended it was not externally validated with another established measure that evaluates the same construct. It was challenging to interpret the factor structure of the WTPQ as the latent constructs that the factors represented were somewhat difficult to identify and label, and several items overlapped considerably. Therefore future research must be undertaken to confirm the factor structure of the WTPQ, through CFA, in a similar sample as utilized in this study to test the factor structure of the WTPQ that emerged in this study.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440211043928 – Supplemental material for Validation of an Assessment Tool to Measure Psycho-Social Factors Associated With Willingness to Participate in Child-Centered Initiatives
Supplemental material, sj-docx-1-sgo-10.1177_21582440211043928 for Validation of an Assessment Tool to Measure Psycho-Social Factors Associated With Willingness to Participate in Child-Centered Initiatives by Ghouwa Ismail and Ashley Van Niekerk in SAGE Open
Footnotes
Acknowledgements
We would like to acknowledge assistance from the community-based fieldworkers/interventionists in Broadlands Park and Erijaville.
Availability of Data and Material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by the University of South Africa, the South African Medical Research Council, and the National Research Foundation.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the ethical guiding principles stipulated by the University of South Africa [3526-5965, Department of Psychology, Ethics Committee], and the ethical code of conduct recommended for social research (Babbie & Mouton, 2001). All the respondents gave their written and oral consent to participate. The study was performed according to the Declaration of Helsinki ethical principles for involving human respondents. To maintain the principle of non-maleficence, the respondents were guaranteed confidentiality, which was taken into account when reporting the findings. In accordance with respecting the respondents’ autonomy, all the respondents were informed that they had the right to withdraw from the project at any time without suffering any consequences.
Supplemental Material
Supplemental material for this article is available from the corresponding author on reasonable request.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.