
Abstract
Electronic healthcare services are becoming an increasingly essential form of information and communication technology (ICT) that enables the fast and smooth delivery of health care, specifically in countries with scarce resources such as Pakistan. A better understanding of factors contributing to the adoption of electronic health care is needed, yet this remains an under-researched phenomenon. Grounded in the united theory of acceptance and use of technology, this article attempts to fill the gap by proposing and empirically testing the contribution of trust, privacy, task-technology fit, and personal innovativeness of patients’ intentions to adopt electronic health technology. A survey questionnaire was used to collect data from 353 patients in major hospitals in Islamabad, Pakistan. This study used Partial Least Square Structural Equation Modeling for the analysis. Results indicate that the intention to adopt electronic health technology is determined mostly by effort expectancy, social influence, facilitating conditions, task-technology fit, trust, privacy, and personal innovativeness in information technology. The study concludes with several managerial implications and future research directions, which give further opportunities to researchers and practitioners in the field of e-health technology.
Introduction
Over the last few decades, the health sectors in most countries of the world have experienced remarkable changes owing to swift headway in information and communication technology (ICT) (Jang et al., 2016). ICT proliferation is an innovative force and provides the facilities with high-quality healthcare services for patients, security, and deliveries (Blumenthal & Glaser, 2007; Tao et al., 2016). From a healthcare perspective, the provision of services that are sound, cheap, and fast is considered very important. A recent study conducted by Hoque et al. (2017) specified that e-health is a result of ICT and has a major effect on health sector growth in developing countries. The advancement in ICT—the dynamic for e-health technology—has been initiated and recognized as an essential element in the health sector. The World Health Organization (WHO) has defined e-health as the leveraging of information and communication technology (ICT) to connect providers, patients, and administrations; to educate and inform healthcare professionals, managers and users; to stimulate innovation in the distribution of care and organisation the health system; and to develop our health care system (Blaya et al., 2010, p. 244).
E-health originality has been broadly regarded as an opportunity for marked improvement in the public healthcare sector to soften the plentiful supply and demand of medical treatment in both developed and less-developed nations (Ball & Lillis, 2001; Ludwick & Doucette, 2009). The World Health Observatory, part of the WHO, surveyed 96 countries, and the results emphasized the need for e-health tools, determining that the tools are handy and applicable for more than 70% of non-Organization for Economic Cooperation and Development countries (WHO Global Observatory for eHealth, 2006).
In most developed countries, the government has invested—and continuously invests—resources in health care to develop advanced e-health systems that consider the most effective way of providing high-quality healthcare services to its residents. For example, in Germany, the government has developed e-health cards through the Federal Ministry of Health for local patients covered by insurance. Health cards cover patients’ personal information such as insurance details and medical history. Patients will use this “smart card” to gain insurance-covered healthcare services (Mugo & Nzuki, 2014). According to Cline (2012), the United States has invested US$1.2 billion to enable the adoption of electronic health records (EHR) in country hospitals. By using EHR, patient information is gathered electronically. In Canada, the federal government established the Canada Health Infoway, which is controlled and entirely financed by the government and managed by the deputy minister of health. The organization’s purpose is to encourage the use of EHR and electronic health information (HI) to ensure the exchange of medical records and health knowledge in the federal, district, and regional zones across the country.
However, despite the potential of e-health technology services, such as delivery of high-quality health care worldwide, previously published studies have shown that the strategic advantage of e-health technology is especially relevant to the developing countries, where access to essential social services like high-quality health care is limited by weak government policies, political conflicts, and the dearth of modern technology infrastructure (Omary et al., 2010). A study conducted by Hoque et al. (2017) assessing the effects of ICT tools on healthcare delivery in Bangladesh showed how these tools can lead to improving the quality and efficacy of healthcare services. Governments in various developing nations are more optimistic that e-health systems will bring improvement in the quality of health care, accessibility, and capability (Tierney et al., 2010). E-health technology provides better access to healthcare services for all—patients, nurses, doctors, and other medical staff—and can improve the quality of health care as well as enhance collaboration (Khalifehsoltani & Gerami, 2010). Patients and physicians are encouraged to use e-health technologies as effective ways to improve quality and mitigate increased healthcare costs. E-health care can improve both the quality of and access to healthcare services while reducing costs even in the event of a shortage of resources (Nessa et al., 2008).
In general, doctors are usually more positive about e-health than patients in developed countries (Hoque et al., 2017). Previous research found that patients appeared hesitant to employ modern technologies (Hoque et al., 2017). Based on the aforementioned findings, it can be concluded that most research initiatives concentrate on the behaviors of consumers toward e-health adoption and other provider aspects, such as physicians’ and nurses’ perspectives. To the best of our knowledge, no studies had been done in Pakistan from the perspectives of patients, although patients play significant roles in the successful adoption of e-health care. Moreover, most of the preceding research was carried out in the context of developed nations. This study therefore attempted to fill the aforementioned gaps by exploring the issues associated with e-health adoption from patients’ perspectives in a Pakistani context.
Viewing the existing literature, recent years witnessed a series of theoretical models (such as IDF, TAM, TRA, and TPB, spelled out below) used by researchers to investigate consumers’ acceptance of the technology. Among them, many scholars used the unified theory of acceptance and usage of technology (UTAUT) to examine user behavioral intention (BI) and the actual use of technology (Ali et al., 2016; Khan, Yu, et al., 2018). UTAUT is considered a unique tool among researchers and is regarded as a distinctive research model because it provides a clear link between the construct and customer-driven BI. This model specifically focuses on the factors that determine users’ BI from the perspective of patients. Given the broad position of the UTAUT model, we selected it for empirical research along with task-technology fit (TTF), privacy, trust, and personal innovativeness (PI) in information technology (PIIT). A study conducted in Africa looked at the adoption of e-health technology, using UTAUT as a base model, and concluded that UTAUT is the best technique for determining users’ intentions in less-developed countries, an additional reason for choosing it for the current study (Ami-Narh & Williams, 2012). In addition, the model incorporated education, age, gender, and experience as control variables to understand clearly the effect of selected variables on target variables (Liu et al., 2016). Recognizing the gap in the literature acknowledged by Ahlan and Ahmad (2014), this article adds to the literature of e-health, based on less-developed countries, where the adoption of technology is under consideration. Also, it was found that the Pakistan health sector uses e-health technology to improve essential services and services in real time (Naseem et al., 2014).
Literature Review
E-health is a fairly recent term that was rarely used before 1999 and now seems to be used to define not only internet medicine but virtually anything related to computers and medicine (Eysenbach & Jadad, 2001). Possibly, the word was used by industry managers and marketers, not academics. They developed and used this term in line with other “electronic” terms such as e-commerce, electronic enterprise, electronic solutions, and so on in an effort to communicate promises, values, and illusion to the healthcare sector and realize new possibilities the internet might hold for the healthcare sector (Eysenbach & Jadad, 2001). Hage et al. (2013) say e-health refers to any interactive communication and information technology aimed at enhancing community quality of life and/or individual health outcomes. It is also a way to provide medical procedures or studies in distant places. E-health is an emerging field at the intersection of medical information, public health, and industry and applies to HI services provided or developed over the internet and other related technologies. In a broader sense, this concept is not just about technological advancement but also about state of mind, attitude, and dedication to networked global thinking, enhancing health care at local, national, and global levels through ICT.
Khan, Yu, et al. (2018) conducted a study titled “Assessing the Physicians’ Acceptance of E-Prescribing in a Developing Country: An Extension of the UTAUT Model with Moderating Effect of Perceived Organizational Support” and discovered that the adoption of e-prescribing by physicians could increase efficiency, improve time management, and increase production.
Qureshi et al. (2014) conducted a study as “An Investigation into the Adoption and Use of Issues of E-health in Public Sector Hospitals of Developing Countries.” This systematic review aimed to summarize the existing literature, identifying challenges and opportunities that promote the implementation of e-health technology in public health hospitals. The study findings illustrated the various facets of e-health systems in terms of their implementation and use in developing countries.
Naseem et al. (2014) conducted a study on Pakistan’s healthcare sector outlined in the article “E-health: Effect on Health System Efficiency of Pakistan.” The study established that electronic health technology can play an important role in managing many infectious diseases through effective monitoring. The implementation of e-health would contribute to greater productivity and increased access for the general public health system and the eradication of diseases in Pakistan. The main aim of the research was to find out how and why physicians decide to use the e-health application in an outpatient setting.
Bhutto et al. (2010) concluded that health informatics could help healthcare facilities improve the delivery of health care in Pakistan.
There is a shortage of studies in underdeveloped countries that highlight e-health in a comprehensive way. Because of the lack of robust theoretical bases around e-health technology in developing Asian countries, our present study employs an established UTAUT method, which has not been used much in e-health, as a lens through which an emerging field can be properly investigated.
Developing countries provide a unique context when it comes to technology adoption because of issues, such as digital division and cultural beliefs, which are much less noticeable in developed countries. Very few studies have examined e-health technology adoption in developing economies, which makes it a significant area of study for researchers. Therefore, the objective of the present study is to investigate the acceptability of UTAUT in influencing the intention of patients in developing countries to use and accept e-health technology.
Theoretical Background and Hypotheses Development
Various theoretical models have been used by scholars to examine user acceptance of technology: innovation diffusion theory (IDF; Rogers, 1995); the technology acceptance model (TAM; Davis, 1989); the theory of reasoned action (TRA; Fishbein & Ajzen, 1975); social cognitive theory (Bandura, 1991); technology life cycle the personal computing utilization model (Thompson et al., 1991); and UTAUT (Venkatesh et al., 2003). Among them, UTAUT is considered a unique and popular tool that has been used in many previous studies to understand the factors affecting the usage and acceptance of new technologies, including e-health. Previous studies have mentioned that UTAUT can explain up to 70% variation in the user’s intention (Lin & Anol, 2008; Nuq & Aubert, 2013). UTAUT holds that four key constructs—performance expectancy (PE), effort expectancy (EE), social influence (SI), and facilitating conditions (FC)—are the direct determinants of BI. Gender, age, experience, and voluntariness of use were introduced to moderate the effect of the four key constructs on usage intention and behavior (Venkatesh et al., 2003). However, one drawback of UTAUT is that its determination coefficient (R2) can be reached only if main relations with up to four variables are moderated.
Recently, Venkatesh et al. (2012) have made some changes to the UTAUT model based on their research results in Hong Kong. They introduced three new constructs into UTAUT. The first is hedonic motivation (intrinsic motivation). The second is price value. The third is habit, extending UTAUT into UTAUT 2. Several scholars have used the extended UTAUT 2 to clarify customers’ acceptance of the technology (Alalwan et al., 2017; El-Masri & Tarhini, 2017; Mahfuz et al., 2017; Nikolopoulou et al., 2020). Reviewing past Information Systems (IS) models, Venkatesh et al. (2003) claimed that UTAUT shows significant changes in the variance explained by BI and the use of technology. Several scholars used UTAUT in the context of health care in a few recent studies. In a study conducted in Bangladesh on the adoption of electronic health cards (EHR) among doctors, UTAUT was used and the author found that FC, SI, and PIIT are key factors affecting physicians’ intentions to adopt EHR systems, whereas PE, resistance to change, and EE did not have a substantial effect on doctors’ behavior (Hossain et al., 2019).
Another study was conducted in Pakistan by applying UTAUT with the extension of perceived credibility and organization support, and the result showed that all constructs are decisive factors in the adoption of e-prescribing among physicians (Khan et al., 2018). Bawack and Kamdjoug (2018) used the same research model (UTAUT) to explain the clinical adoption of HI system services in developing countries (in this case, Cameroon) and discovered that young clinicians are more likely to accept and adopt these services than older ones. Hoque et al. (2017) examined the acceptance of technology by patients in Bangladesh with UTAUT. In another study, Hoque and Sorwar (2017) applied UTAUT in the healthcare sector and successfully identified the variation and the approval of mobile health technology in older people. Aggelidis and Chatzoglou (2009) used modified TAM to verify the applicability of the theoretical model to interpret the acceptance and validation of ICT’s adoption in hospitals and discovered that it has the potential to revamp the quality of health service, improve the effectiveness of hospital staff, and decrease health costs.
Based on the review of UTAUT’s application in previous healthcare contexts, we have planned to use the UTAUT framework to understand the factors that influence the use of e-health technology by patients (Venkatesh et al., 2003). UTAUT is considered a unique research model and has been used in many previous studies to explore user acceptance of new technology. The model explains that PE, EE, SI, and FC rightly influence the user’s intention to use the technology. However, behavioral BI explains users’ specific user behavior (UB) with new technologies. Age, experience, gender, and voluntariness of use are the critical moderators of the UTAUT framework. The next sections enlighten the hypotheses established in this study to measure the identified factors.
PE
Venkatesh et al. (2003) theorized that PE is “the degree to which the user can trust that using the technology will help to overcome difficulty and help him or her to achieve the desired goal in job performance.” If the system brings benefits, it will contribute to service adoption (Tojib & Tsarenko, 2012). Previous study work reveals that the majority of past health studies find a good relationship between PE and BI (Alam et al., 2019, 2020). PE affects users’ intentions to implement a new e-health service that can promote general health system information (Gagnon et al., 2016). According to Slade et al. (2013), PE helps individuals develop satisfying health experiences. PE has a positive effect on users’ intention to adopt a new technology (Khan et al., 2018). Thus, the argument given encourages the development of the following hypothesis:
EE
EE is defined as “the extent of ease connected with the use of a system” (Venkatesh et al., 2003). In general terms, users are encouraged to adopt new technology if they believe the technology is beneficial and valuable in their everyday lives (Ali et al., 2016). Martins et al. (2014) investigated the significant influence of EE on BI. Numerous scholars have identified the positive effect of EE on the adoption of technology and consider it a vital element of users’ intentions to use e-health services, m-health monitoring systems, and the EHR system (Boontarig et al., 2012; Lian, 2015). Thus, we postulate the following hypothesis:
SI
People are no doubt affected by others in their community and in their social networks, such as colleagues, friends, and family members, when it comes to using information technology. In a technology context, the effect is called SI. SI has been explained as “the degree to which an individual sees other important [people] believe he or she should use the new system” (Venkatesh et al., 2003). SI has been adequately taken into account and confirmed as a predictor of personal behavior (Zuiderwijk et al., 2015). In a study conducted in South Korea, the author found that SI played a significant role and explained that it is an essential precedent for BI (Kim et al., 2011). Previously published work also supports and explains the positive effect of SI on users’ intentions in the use of e-health services (Ahmad & Khalid, 2017; Sun et al., 2013). This research empirically supports the strong relationship between SI and BI. Hence, we develop the following hypothesis:
FC
Another significant predictor of e-health technology is FC. In earlier research work, FC were shown to affect BI and the adoption of technology in a significant and positive way. FC are defined as “the level to which an individual trusts that a structural and practical infrastructure exists to support the use of the system” (Venkatesh et al., 2003). User access to an adequate set of FC, such as hardware/software, technical support, online tutorials, and online demonstrations, are essential to developing the intention to use. Practically, the beneficial effect of FC on usage behavior regarding e-health services and HI system has been supported by many studies (Boontarig et al., 2012). Therefore, in the context of Pakistan, we propose that users need sufficient FC to plan to use online technology. We postulate the following hypothesis:
TTF
Experimental evidence proved that an individual will not readily accept and use new technology if the technology neither satisfies their needs nor improves their performance (Gebauer & Ginsburg, 2009). Various theories of technology adoption usually consider the individual perception of the technology. TTF shows that individuals do not rely solely on their choice of technology in their opinions. The individual can find the technology useful and accept it based first on TTF and not by any other perception regarding technology. The theoretical basis of TTF says that individuals will not adopt the technology if they do not find it appropriate for their daily tasks, and it does not improve their functioning (Oliveira et al., 2014). Therefore, it is supposed that the right TTF will increase BI for the user to use and adopt the technology (Zhou et al., 2010). Thus, we posit the following hypothesis:
Privacy
Privacy and trust is a topic of increasing importance in health care. Privacy is a fundamental principle in the doctor–patient relationship. Patients need to exchange information with their doctors to facilitate correct diagnosis and treatment and also to avoid harmful interactions between drugs. Sankaranarayanan and Sallach (2014) clarified that patients mostly agreed to exchange information with doctors but did not usually share all their HI with other parties, such as family members and coworkers. Patients’ awareness of privacy increased with the advancement and use of knowledge and information technology in the healthcare sector (Angst & Agarwal, 2009). Westin (2006) explained that patients have great concern for their personal HI and care about the dissemination of that information without their consent. Therefore, we posit the following hypothesis:
Trust
Mayer et al. (1995) defined trust as “willingness to rely on exchange partners where one has confidence.” Sillence et al. (2006) argued that trust is the most critical factor affecting a patient’s intention to use an electronic health system. Briggs et al. (2002) surveyed 2,500 people who were seeking online health counseling and discovered that individuals would trust online technology if the risk factor was low. Ek et al. (2013) investigated the critical role of trust in the adoption of electronic health services. Trust has, therefore, a vital role in the development of online technology and also helps to reduce the fear of harmful and fraudulent activities in the technological environment (Afshan & Sharif, 2016). Accordingly, we offer the following hypothesis:
PIIT
PI indicates how willing someone is to accept or use new technology. Park et al. (2015) found that PI subsequently helps to promote individual innovative behavior, specifically acceptance of innovation. Rogers (1995) defined PIIT as “[t]he degree at which an individual is quite early in adopting new technologies.” Different scholars have concluded that innovative users have a higher level of incubation of new technology because they are more tolerant of uncertainty, risk-oriented, adventurous, and self-confident (López-Nicolás et al., 2008; Tan et al., 2014). Agarwal and Prasad (1998) found that PI significantly affects a user’s intention to adopt and use new e-health services. Sorwar and Hoque (2015) identified PIIT as one of the main concerns in terms of e-health and healthcare accreditation. In this case, we define PIIT as “individual willingness to test new information technology (IT),” and we hypothesize the following:
BI
BI is considered an immediate antecedent of UB and indicates an individual’s inclination to perform a specific action. In previous IS/IT literature, BI has been extensively found to have a substantial effect on physician adoption of e-health services and to be considered a significant predictor of UB of HI systems (Han et al., 2004; Kijsanayotin et al., 2009). A study conducted in Bangladesh determined that doctors’ and patients’ BI leads to the adoption of e-health technology (Hoque et al., 2016). In the context of Pakistan, we believe that a user’s intentions to adopt e-health will lead them to adopt it. Accordingly, the study posits the following hypothesis:
Method
Data Collection and Sampling Method
The targeted population of this study consisted of patients in major hospitals in Islamabad, Pakistan. Similar to prior research on technology acceptance, particularly in the healthcare field, quantitative survey methods were used to gather data to verify the proposed model (Khan et al., 2018). Furthermore, the survey method is considered suitable and is a widely used research method that predicts BI and studies the relationship between constructs (Rossi et al., 2013). The questionnaire was formulated in two sections: A and B. Section A contained demographic information. The author asked participants to provide complete information about their age and education as well as their experience. Section B contained 35 items about all constructs in the research model, as shown in Figure 1, which could be answered by using a 7-point Likert-type scale ranging from “Strongly Disagree” to “Strongly Agree.” Before distributing the questionnaire to patients, a pilot study was conducted, and the response was used to develop and test the final survey. After completing the pilot study, the authors started to gather data from patients at various hospitals. The study distributed 400 questionnaires containing 35 items among participants and asked them to rate their responses about e-health technology. A total of 353 copies were successfully reverted, and the response rate was 88.25%. Forty-seven questionnaires were excluded because of incomplete responses; 353 correctly completed questionnaires were used to analyze the proposed hypotheses in the model. In this study, the respondents’ participation was entirely voluntary, and no payment was made.
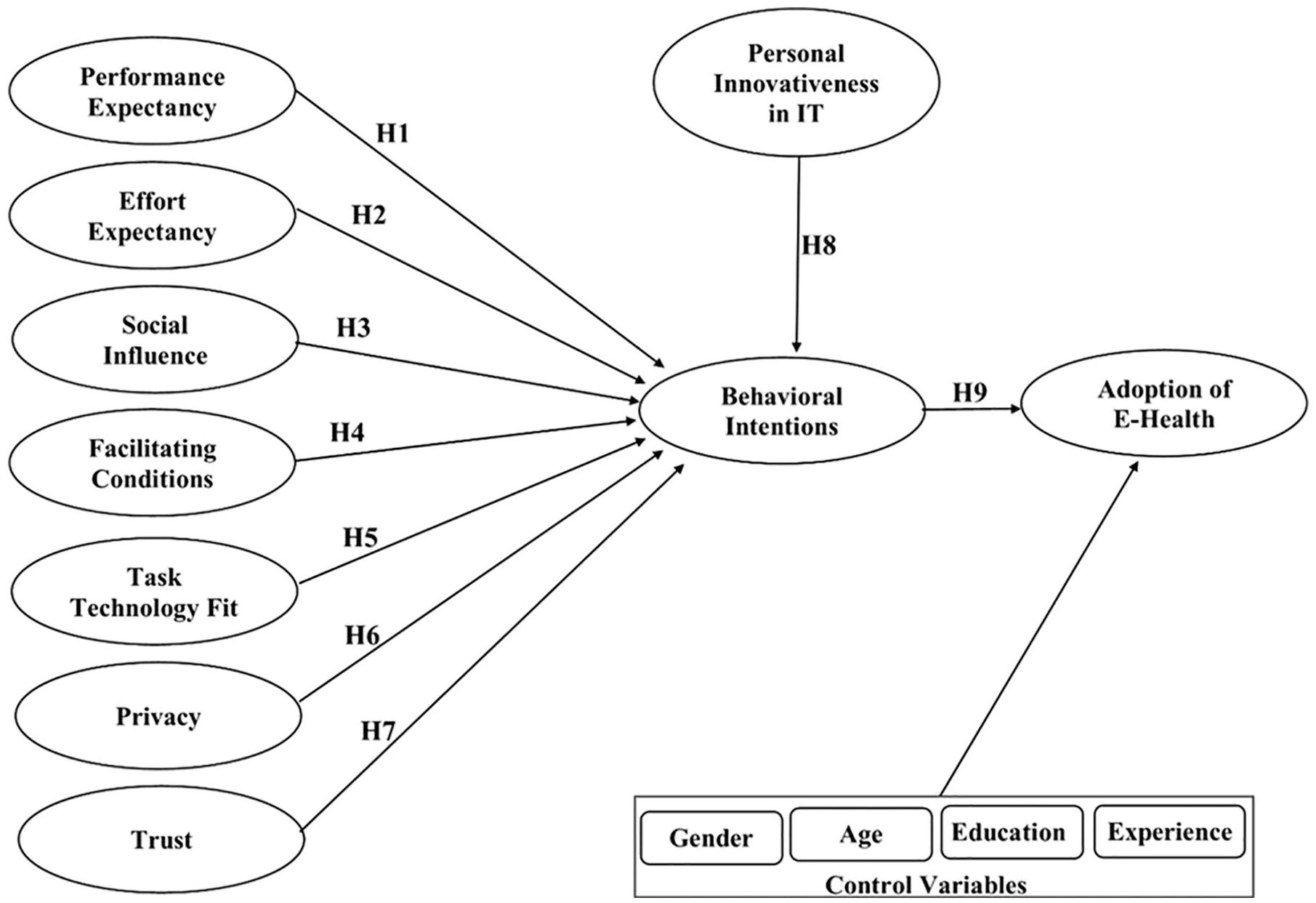
Hypothesized model.

Results for the structural model.
Data Analysis
SmartPLS 3 software, version 3.2.6, was used to perform the partial least squares structural equations (PLS-SEM) testing and validation of the proposed research model and the hypothesized relationship between the constructs (Hair et al., 2016). In general, PLS-SEM is one of the most popular and commonly used kinds of software for measuring the relationship between several dependent and independent constructs (Hair et al., 2016). The collected data from the questionnaire were entered into Excel Sheet and then imported into SmartPLS. In this way, PLS-SEM was used to analyze the proposed structure model, as it is the dominant multivariate method broadly used in social science (Khan et al., 2018).
Measurement
Measurement items for all variables were adopted from prior literature and slightly modified according to e-health technology. All questions from the survey were tested on a 7-point Likert-type scale.
As shown in Table 1, the gender, age, education, and experience were added to the main variables to examine relationships and get accurate results. Previous e-commerce studies showed that BI also affects gender, age, education, and experience. Khan, Hameed, et al. (2018) found insignificant results in gender, age, and education on acceptance of Massive Open Online Courses (MOOC). Khan, Liu, et al. (2018) reported insignificant results in terms of education, age, and gender when implementing online stock trading. Pavlou (2003) has mentioned that experience plays a significant role in future intentions. The present research, based on the potential influence of these variables, used gender, age, education, and experience as control variables to improve the model’s predictive capacity.
Sample Characteristics.
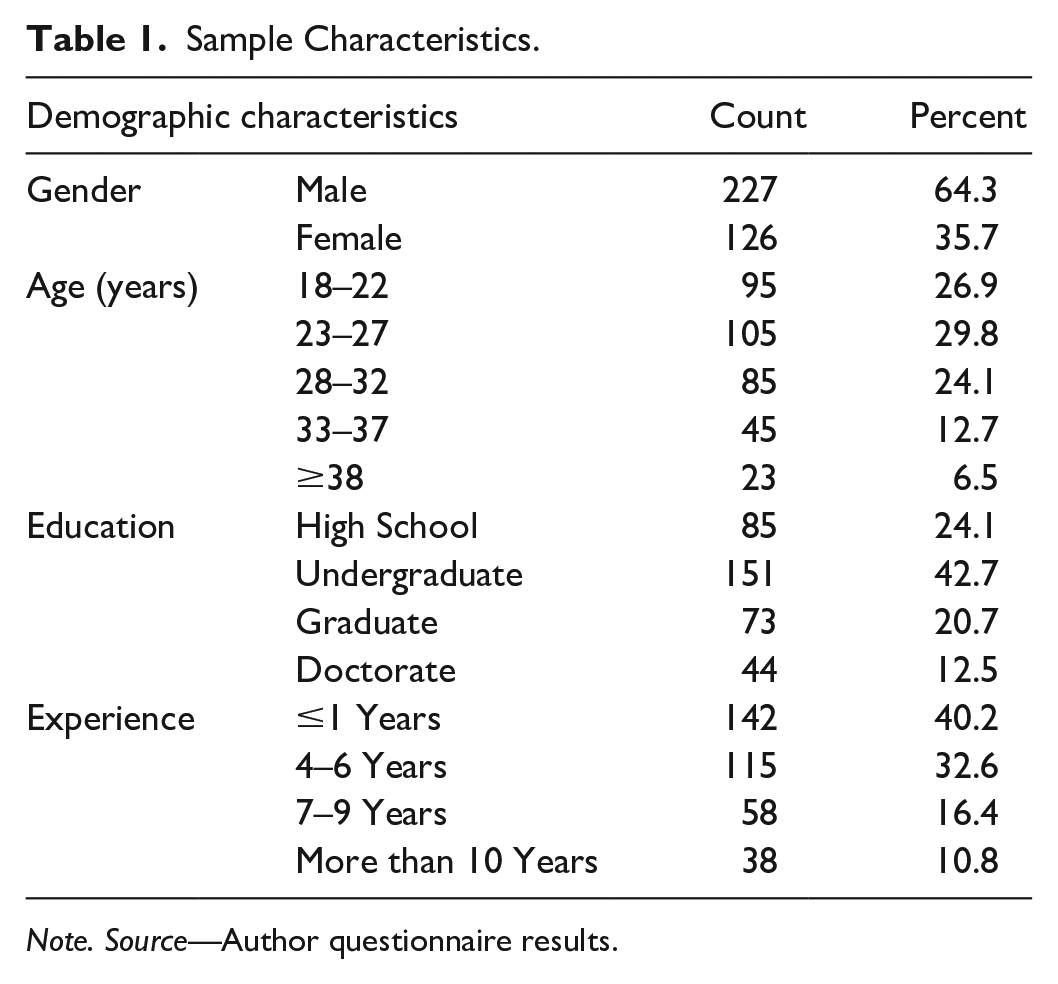
Note. Source—Author questionnaire results.
Results
Normality of Data and Common Method Bias
Skewness and kurtosis were conducted to check the normality of the data. The finding indicated in Table 2 shows that the data were normal as the skewness and kurtosis were found within the range of ±2 as advised by George and Mallery (2010). Common method bias (CMB) is one of the prime sources of measuring model error. According to Podsakoff et al. (2003), when the data are collected from one source at a point in time for both endogenous and exogenous variables, CMB might exist. Statistically, if Harman’s one-factor test results for a single factor account for 40% or more, there may be CMB problems in the data. To test for CMB, Harman’s one-factor test was applied. The results show that total dispersions are 32.79%, which meets the standard of 50%. This result indicates that the present data are free of any significant CMB issues.
Factor Loadings, Cronbach’s Alpha, CR, and AVE.

Note. CR = composite reliability; AVE = average variance extracted; Cα = Cronbach’s alpha.
Reliability and Validity Testing
At first, the reliability and validity were checked for all constructs. Reliability is usually indicated by internal consistency, which is measured by Cronbach’s alpha and composite reliability (CR). As suggested by Joe (1993), the Cronbach’s alpha (Cα) and CR values are not less than .70, which is a sign of satisfactory consistency. To ensure the convergent validity, the average variance extracted (AVE) was evaluated where the loading items were all above 0.50, indicating a sound validity (Ketchen, 2013). The model was analyzed using Cα, CR, and AVE. Table 2 shows the results for Cα, CR, and AVE values. Table 2 shows that the estimated values of Cα are more significant than 0.70 for all constructs. The CR value is acceptable if it lies in the range of .60 to .70. However, a CR value between .70 and .90 is also considered acceptable (Nunnally & Bernstein, 1994). In the present study, the value of CR for BI is .914. That is slightly more than the threshold but lies in the acceptable range. Nunnally and Bernstein (1994) explain that a CR value higher than .95 is usually unacceptable because it means the selected question is considered as unrelated or objects measure the same phenomenon repeatedly. Thus, the condition of convergent validity is acceptable in the study (see Table 2).
Furthermore, after reviewing the reliability, data were also assessed for validity. To ensure convergent validity, the AVE was assessed. Convergent validity refers to how well the structural indicators load or converge on their constructs (Petter et al., 2007). Statisticians have the opinion that the value of AVE must be higher than 0.5 in the case of a reflective construct. In the present research, the AVE value for all variables is above the threshold, which shows good convergent validity.
In addition, data were tested for discriminant validity. Discriminant validity refers to the level to which one construct in the model is different from another construct in the same model (Hair et al., 2016). The square root of AVE usually estimates discriminant validity. The square root value of AVE should be greater than the correlations of each construct(s) (Fornell & Larcker, 1981). Table 3 presents the results and shows that the square root values of AVE for each hypothesis are more significant than the correlation values as desired, which fulfills the discriminant validity requirement. The bold values in Table 3 indicate the square of AVE, and the off-diagonal value shows the correlation among constructs. Table 5 shows the cross loadings.
Discriminant Validity Results.

Note. N = 353. The bold diagonal numbers show sound discriminant validity. BI = behavioral intention; EE = effort expectancy; FC = facilitating conditions; IT = information technology; P = privacy; PE = performance expectancy; AEH = Adotion of e-Health; PIIT = personal innovativeness in IT; SI = social influence; T = trust; TTF = task-technology fit.
Evaluation of Structural Model
Hypotheses testing
The structural model classifies relationships between constructs in the research model. The bootstrapping with 2,000 sampling method was used to test the path coefficients of hypotheses by using statistical software SPSS. Our data results support all hypotheses except PE. First, the study examined the relationship between the endogenous and the exogenous constructs by path coefficient (β) and t-statistics. In the next step, the study revealed the role of control variables such as education, experience, age, and gender. The results for path coefficient (β) and t-statistics are presented in Table 4.
Hypotheses Decision Table.

Note. BI = behavioral intention; EE = effort expectancy;; IT = information technology; FC = facilitating conditions; P = privacy; PE = performance expectancy; PIIT = personal innovativeness in IT; SI = social influence; T = trust; TTF = task-technology fit; AEH = Adotion of e-Health.
Significance levels at 1% (p < .1). **Significance levels at 5% (p < .05). ***Significance levels at 10% (p < .01).
Item Loadings and Cross-Loadings.

Note. BI = behavioral intention; EE = effort expectancy; FC = facilitating conditions; PE = performance expectancy; PI = personal innovativeness; SI = social influence; TTF = task-technology fit; AEH = Adotion of e-Health. The bold values show the cross loadings of each construct.
Importance-Performance Map Analysis
The importance-performance map analysis (IPMA) shown in Figure 3 expands the PLS-SEM findings by analyzing the average values of the constructs’ scores. The purpose of IPMA is to recognize the most important fundamentals of the construct that have the strongest effects on the construct but with low yield (Ringle & Sarstedt, 2016).

IPMA results.
The results of IPMA indicate that PI has the highest importance with the total impacts of 52.2. A unit increase in PI will increase the adoption of e-health services up to 52.2. Thus, to increase the adoption of e-health services, the policy makers should consider awareness campaigns regarding the benefits of IT innovativeness by individuals.
Discussion
This article postulates that PE has a positive effect on patients’ intentions to accept and use e-health technology (β = −0.045, p = .422) but that was not supported. The results are apparently unexpected, considering that in the adoption of technology, several previous studies affirm a significant relationship between PE and BI. For example, Phichitchaisopa and Naenna (2013) found that PE has a significant effect on the acceptance of healthcare information technology (HIT) and noticed that the factor has positive effects on physician adoption of EHR. Similarly, I. U. Khan, Yu, et al. (2018) also discovered a positive association between PE and BI on physician adoption of e-prescribing technology. Several other scholars, such as Hossain et al. (2019), are of the view that PE directly influences a user’s intention to use new technology. Our findings reflect the fact that most patients in Pakistan are not familiar with e-health technology and the benefits they may derive from it (Qureshi et al., 2014). In addition, Pakistan lacks adequate ICT support in the health sector (Ali & Abbas, 2019). Lack of instruction on the implementation of e-health technologies, lack of computer skills, lack of knowledge, and lack of sufficient and quality health facilities are all factors. Many patients are afraid to use e-health technology because they believe that their HI may be misused (Azhar et al., 2009). The abovementioned arguments might suggest that PE plays no significant role in the adoption of e-health in Pakistan’s current situation. Moreover, our results are also consistent with several preceding studies. For example, Vanneste et al. (2013) found an insignificant effect of PE on users’ BI to adopt new healthcare technologies.
The second and third hypotheses, which proposed that EE and SI positively influence a patient’s intention were supported. The results are in line with earlier work (Hoque & Sorwar, 2017). Furthermore, the result for EE (β = 0.113, p = .006), denoted by H2, the influence BI to accept e-health has supported the outcome of earlier research work (Chen & Hsiao, 2012; Dünnebeil et al., 2012). These results also help to better clarify the contradictory findings of previous research regarding patients’ BI to use online postings of emergency department (ED) wait times of Jewer (2018) who had found that EE did not affect patients’ BI to use online posting of ED. The current results support AlAwadhi and Morris (2008) findings that SI (β = 0.224. p = .000) becomes more critical when an individual has insufficient experience with online services. Wills et al. (2008) also showed that SI plays a critical role in adopting EMR. Holtz and Krein (2011) discovered that SI is a crucial factor in the adoption of an electronic medical record (EMR) system.
Data analysis also shows that FC’s positive effect on patients’ intentions (β = 0.160, p = .000) was supported, which means that healthcare users need tools like the internet and also need digital equipment as they move toward BI (Venkatesh et al., 2012). Moreover, to better investigate the user adoption of e-health technology, the current study added TTF, trust, privacy, and PIIT to the UTAUT model because few studies have applied these constructs in health care and the few that have done so have reached different conclusions.
The results support the proposed notion of the fifth hypothesis (TTF) and show a significant effect on patients’ intentions to adopt e-health technology (β = 0.157, p = .009), which further determines the patient’s adoption. In the context of online technology, our result is also consistent with the work of Junglas et al. (2008)and Zhou et al. (2010). Thus, when a healthcare provider provides their services, they need to take into account the need for a task between users and the function of e-health technology.
The study posited that PI positively influences a patient’s BI to adopt e-health technology. This hypothesis was supported by data (β = 0.408, p = .000) signifying that PI positively affects patients’ intentions. These results are also similar to the results of (Hoque et al., 2016), who found that PIIT plays a significant and conspicuous role in users’ intentions to accept e-health. On the other hand, the result of the current study is also associated with the findings of Hossain et al. (2019) who established that PI plays an essential role in users’ behavior when it comes to accepting healthcare technologies. Thus, it shows the user’s tendencies to discover and experiment with PI. Consequently, it will make it easier for patients to connect and share information and also experiment with new ICT and actively engage them when presenting such technology.
The seventh hypothesis, which predicted that trust would have a positive effect on patients’ intentions to adopt e-health technology (β = 0.134, p = .010) was accepted and was consistent with the findings of previous work such as that authorized by Hoque et al. (2017) who assumes this trust has a strong and positive influence on patients to use e-health technology. In previous research work on technology acceptance, several authors identified trust as the most critical variable in the adoption of online technology. Gefen et al. (2003) indicated that trust has a direct effect on users’ BI to accept online technology. Zhou (2011) found that trust is a crucial determinant for selecting and using online technology.
In addition to the essential UTAUT variables, privacy was investigated in the context of Pakistani health care and was accepted (β = 0.082, p = .053). The association between privacy and BI, denoted by H6, was found to be significant. Our result also supports the findings of the previous study (Wilkowska & Ziefle, 2011). Similarly, our results are also dissimilar to the findings of Hoque et al. (2017) who found that the relationship between privacy and the acceptance and adoption of e-health technology in the context of Bangladesh was not significant.
Finally, the results show that UB is a critical construct that was predicted by the original BI toward e-health. The model describes 54% of the variance in patients’ BI in the adoption of e-health technology and 39% of variance in adoption of e-health. Also, the results show that BI has a positive effect on patient behavior regarding e-health. Thus, H9 is supported. The overall results of hypotheses can be seen in Figure 2.
Theoretical Implications
The current study results contribute to the inclusion of the determining factors that affect the intention to adopt electronic health. From a theoretical perspective, this research makes an outstanding contribution to the theory and efficient management. The fundamental contribution of current research is to information systems research on the scope of e-health accreditation in a developing country, namely, Pakistan. Second, the present analysis applied UTAUT, the most widely used and accepted model, to find users’ intentions to adopt e-health (Venkatesh et al., 2003). UTAUT integrates eight different theories and is considered a base model for the researcher. Prior studies applied different technology-based models to investigate the consumer’s acceptance of technology, but the application of these technological models in health care is scarce (Cocosila & Archer, 2010). The current case is the first attempt to extend the original UTAUT model with the additional variables, TTF, privacy, trust, and PIIT, in the setting of Pakistan. This study considers the modified UTAUT model, which significantly contributes to health literature and is among the few to discover the factors that influence the use of e-health technology among patients in developing countries. The study results also provide additional sustenance for the UTAUT model, including an additional variable in e-health technology acceptance. Thus, the current study concludes that the extended UTAUT model is applicable to health care. In addition, the research clarifies the adoption and acceptance level of new technologies to improve the health care of patients. That is, this kind of research will help increase the intention of patients to benefit from adopting and using technology in health care. The proposed extended theoretical model makes a remarkable contribution to literature, and the result also provides more sustenance to UTAUT with the additional variables in the adoption of e-health technology.
Practical Implications
This study also has practical implications for the paybacks of enlightening the adoption of e-health technology in developing countries. The results of this study highlight the significance of improving e-health technology in the context of less-developed countries. A study conducted by Hoque et al. (2017) says that the primary reason why patients in developed economies have lower use of e-health technology is that little attention has been paid to the theoretical understanding of its undesirable use. The current study findings provide practical guidance for the successful introduction of e-health technology in developing economies. Second, our experimental results provide practical strategies for the successful adoption of e-health service in developing nations.
Moreover, because of our general approach, the survey results can be easily modified in the context of other developing countries to help in planning and adopting e-health. This study is also beneficial for e-health technology designers and providers to help them understand the challenges and problems of designing and implementing successful e-health technology. Adding to the practical contribution, prior studies, such as the one by Hoque et al. (2017), observed the vital role of patient acceptance and positive e-health behavior, our research comprehensively explores the factors affecting patients’ intentions to embrace e-health technologies in a broader context. Furthermore, we introduced gender, age, education, and experience as control variables to understand their effect on the target variables.
Limitations and Future Research Directions
Although our study provides useful information about e-health feasibility, the current research is not free of limitations. Ideas for further research have ascended from the limitations and results of this study. A potential weakness of the current research is that it is cross-sectional, which means it is a convenient, fast, and cheap source of data collection. Researchers have criticized cross-sectional studies because of bias, where the participants in the study do not adequately reflect the viewpoint of the entire population, affecting the research findings and the potential to generalize from them. This is because of the survey and the fact that the respondents were interviewed only once to participate in filling out the survey questionnaire (Sedgwick, 2014). Therefore, the authors suggest that further study should apply a longitudinal technique for data collection, where participants in the survey will be interviewed more than once. Second, we cannot generalize the findings to non-developed countries because this research is specific only to the context of Pakistan. The data were collected from Islamabad, the capital city of Pakistan, so we recommend ongoing research that includes a comparative analysis of rural and urban adoption of e-health. Past published research also shows that moderators of age, gender, experience, and voluntariness of use play a substantial role in predicting users’ acceptance of technology (Sharma et al., 2013). The research has also shown that factors such as age, gender, experience, and voluntariness of use play an important role in predicting users’ acceptance of information technology (Sharma et al., 2013). Further research may also consider the moderating roles of age, gender, experience, and voluntariness of use on the BI of patients, which might influence their decisions to use e-health technology. Despite the abovementioned limitation, the present research was able to examine and investigate the leading factors that affect the patients’ willingness and decision to accept and adopt e-health technology in developing economies—in this case, Pakistan.
Conclusion
Given the lack of research work on e-health technology acceptance and its adequacy in developing countries, the present study extended the well-established UTAUT framework with the contribution of additional variables, that is, trust, privacy, TTF, and PIIT, to examine the adoption of e-health technology by patients in the developing economy Pakistan. The study found that EE, SI, FC, TTF, privacy, trust, and PIIT significantly influence patients’ intention to accept e-health technology. The actual study results also suggest that no positive relationship exists between PE and patients’ BI to accept e-health technology. The results seem different and not in line with the results of other studies. However, it is believed that the findings genuinely reflect the cultural and socioeconomic aspects of developing countries such as Pakistan. The findings provide insight for e-health service providers, policy designers, and policy makers to design and develop policies and strategies for successful employment of the adoption of e-health technology among patients, specifically patients in a developing environment like Pakistan.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The dataset collection and analysis of this research were partially supported by the National Natural Science Foundation of China (NSFC) under Grant Nos. 71771077, 72071063; Fundamental Research Funds for the Central Universities with No. PA2020GDKC0020 and Anhui Provincial Key Research & Development Plan with No. 202004h07020016.