
Abstract
There is often a sociocultural distance between medical practitioners and patients. We bridge that gap in the therapeutic alliance via improved cultural competence and an understanding of the person in their context. The traditional approach in medical education has been of learning via expert-designed curricula, which may tend to mirror the knowledge and needs of the experts. This places individuals at risk who come from culturally and linguistically diverse groups (CALD) with known health disparities: minority groups (e.g., African American); First Nations’ people; immigrants and refugees; people who speak nondominant languages; and lesbian, gay, bisexual, transgender people. The authors briefly review the complex area of cultural competency and teaching delivery. The authors survey the Australian population to provide a tangible example of complex cultural diversity amid curriculum challenges. An evidence-based approach that recognizes specific health inequity; the inclusion of CALD stakeholders, students, care professionals, and education professionals; and codesign and coproduction of curriculum components is recommended. This method of people’s own stories and collaboration may be applied in any international context, correctly calibrating the learning experience. The aim is for medical students to improve their knowledge of self, others, others within groups, and recognition of unconscious biases to achieve better health outcomes within their specific communities.
Keywords
Introduction
Medical practitioners do not represent the population as a whole. Doctors by necessity are extremely well educated, tend to come from more privileged backgrounds than their patients, and are less likely to be economically disadvantaged. Future doctors see the world from this perspective (Seeleman et al., 2009), and an anchoring bias may lead to cognitive shortcuts (Lieder et al., 2017) and assumptions about other groups.
Implicit (or unconscious) bias also permeates health care. Teal et al. (2012) note that implicit bias influences a doctor’s behavior and is equally difficult to address with the potential for disparate care in groups, such as the religious, obese, elderly, and gay, lesbian, bisexual, and transgender groups. Green et al. (2007) demonstrated that physicians in the United States were more likely to recommend thrombolysis for White patients than Black patients who were experiencing acute coronary syndromes. Implicit bias was implicated in pediatrician opioid treatment of pain, reduced in African American patients versus White patients (Sabin & Greenwald, 2012). Gender assumptions may also be expressed in the delivery of clinical care. Safran et al. (1997) noted that 349 U.S.-based physicians were four times more likely in female patients than male patients to advise a restriction of activities despite accounting for medical illness comorbidity. The impact of doctor bias with regard to gender, racial, and ethnic group was further exemplified by Teal et al. (2012).
Awareness of bias is often suggested as a method for addressing these challenges (Santry & Wren, 2012) with knowledge of limitations within self and a sociocultural interest that is focused on the individual while also being patient centered. To address some of these biases, calls for systematic training in cultural competence have arisen in the past decades (Knipper et al., 2010; Saha et al., 2008; Santry & Wren, 2012). “Cultural competence aims to bridge the cultural distance that exists between ourselves as providers and our patients” (Betancourt, 2006, p. 500) and thus provides the potential for effective therapeutic intervention.
In health care, it can be broadly understood as having a full appreciation of how a patient’s cultural background and individual circumstances can influence their healthcare needs and the behavior and attitudes of the clinician.
Awareness of health needs and the elimination of clinician bias is possibly the practical translation of cultural competence for the patient–clinician dyad.
Critics of the term “cultural competence” note that it may be poorly understood and defined, synonymous with ethnicity, nationality, and language (Kleinman & Benson, 2006). This then renders a generalized approach to the cultural treatment of a patient in a particular “ethnic” group rather than an individual consideration of the person and their predicament within the sociocultural and economic context of their group amid the current stressors. Gender and sexuality do not always easily fit within such a narrow definition of cultural competence. Gregg and Saha (2006) argue that cultural competence matters in health care and in understanding health disparity; however, it may not solve the problems of disparity or reduce racism. Kirmayer (2012a) argued that we need to rethink the idea we have of cultural competence, as the clinician–patient encounter may be via a complex prism of difference in power, historic context, language, religion, and other aspects of cultural identity. He noted that the social determinants of health take their form amid the politics of the landscapes in which patients find themselves, and ideally, a best-fit model should integrate the patient and practitioner within the local healthcare setting.
Thematic representations of cultural competence were also of interest to Kirmayer (2012a): responsiveness, humility, and safety. The theme of “cultural responsiveness” that a therapist is culturally attuned to the patient ethnic group and this improved health outcome was partially supported by Sue et al. (1991). “Cultural humility” as a theme has emerged and asked leaders to engage clinicians in training to challenge: “unintentional and intentional racism, classism, and homophobia” (Tervalon & Murray-García, 1998).
Another expression of competence is that of “cultural safety” that has arisen in the Maori experience and is driven by Maori nurses (Papps & Ramsden, 1996). The debate about time spent devoted to cultural safety training of nurses versus traditional training of nurses led to a considerable focus on the health disparities between the Maori and the non-Maori people of New Zealand because of political, historical, and social reasons. This included an elevated risk of suicide. Meetings between nurse educators and the community led to direct input into the curriculum, and a set of cultural safety standards were developed called “Kawa Whakaruruhau” (Ramsden, 1990). The concept has been further refined to include age or generation; gender; sexual orientation; socioeconomic status; ethnic orientation; religious or spiritual belief; and disability (Papps & Ramsden, 1996).
In the United States, medical schools have recognized the importance of “cultural competence,” and it is required as a standard. This is currently taught via pedagogical methods, such as student reflections, readings, presentations, lectures, clinical vignettes, and community visits. However, the concept of cultural competence is poorly defined in most curricula, and considerable variability is reported between 18 medical school programs (Jernigan et al., 2016). This theme is echoed by clinical teachers from Taiwan who desire further culturally competent training of medical students but are unsure of commonly agreed goals and methods to deliver that education (Lu et al., 2014).
Cultural competence has been alternatively viewed within the context of medical education by considering the structural elements that contribute to health disparity. It is described as “structural competency,” which considers medical, anthropological, sociological, and historical aspects of the case that lead to presentation and a framework of solutions for the person (Metzl & Hansen, 2014). A core element of structural competence includes “structural humility” drawing on the similar concept of cultural humility (Metzl & Hansen, 2014). There are calls to further refine structural competence in medical education to consider how politics and policy can lead to disadvantage, and this is considered particularly important in the education of a medical professional, especially in the era of COVID-19 (Goel & Kavanagh, 2020).
These various models have been proposed to conceptualize the necessary competencies that educators hope medical students and other health professionals will achieve. These models continue to be dynamic but seek to see a person, often across generations and, within the context of a complex community amid their differing access to opportunity.
Strengthening an approach to cultural competence training can begin with a unifying approach to groups that experience both clinician bias and a health gap. This will be specific to community and context, an interaction between persons, place, systems, and that moment.
Identifying Groups
In any population, demarcations around a group are made for the purpose of description. The authors have chosen to employ the term “Culturally and linguistically diverse” (CALD). This term is commonly used in Australia (Caperchione et al., 2010; Garg et al., 2017; Shanley et al., 2012; Williams et al., 2012; Woolfenden et al., 2014), a country with a large immigrant population and First Nations’ people with significant health disparity. This is a broader and inclusive term that is not necessarily ethnocentric and can include all groups with health disparity. CALD groups, the people who stand apart from the mainstream population, forming subcultural groups with clear mores and values outside the mainstream (see Box 1) should be identified within a given population group. This includes minority groups, First Nations’ people, immigrants, refugees, and those with sexual or gender diversity.
Culturally and Linguistically Diverse Groups (CALD).
Indeed, CALD groups that surround the margin of people most commonly encountered in clinical practice are also the most likely to be exposed to clinician bias (Qureshi et al., 2008). This can lead to health disparities in these minority groups (Blair et al., 2013). Evidence-based practice can also ignore the nuances of dynamics within these subgroups (Kirmayer, 2012b), meaning important opportunities for health intervention may be missed in the very populations where significant health disparities exist.
The ongoing tension of this missed opportunity is evident in the momentum of the Black Lives Matter movement with this social phenomenon capturing unheard voices across the world amid groups who have historically experienced similar economic, educational, and health disadvantage as well as lifelong exposure to bias and discrimination (Sawyer & Gampa, 2018).
Similarly, many lesbian, gay, bisexual, and transgender (LGBT) people experience discrimination or criminal sanction and poor health across many nations, with efforts from this group to improve input and international human rights law (Gerber & Gory, 2014). Disadvantaged and disempowered people would like to have a voice and a role in their own narrative.
A criticism of this approach is to label and generalize characteristics to the group. However, identifying groups that face known health disparities remains important, and then understanding the individual predicament via adequate teaching reminds students that within-group difference may be immense. The prism of cultural identification with a group remains deeply important for some individuals as a core part of self, for example, “I am a Fijian born woman living in Toronto.”
Australia as an Example
The role of a medical curriculum that encompasses holistic and thoughtful teaching on cultural competence cannot be underestimated in providing communities with the empathic and culturally sensitive doctors that are required.
The authors examined Australia as an Organization for Economic Co-operation and Development country, with significant educational resources (HERI Budget Overview 18-19, 2018) and serving a diverse population of 23.4 million people (Census QuickStats: Australia, 2016).
The purpose of examining one country and the national curriculum is to illustrate the heterogeneous population and the potential health disparities. This may serve as a template for other countries that have different populations and needs.
Australians are a plural society. The last Australian Census was conducted in 2016 and demonstrated a growing trend toward an increasingly multicultural society. In this thriving country, one-third of all Australians were born overseas, and one-third of Australian households report a language other than English spoken at home (Census QuickStats: Australia, 2016). The heterogeneity of diversity is further exemplified in that the top three countries of overseas birth are England 3.9%, New Zealand 2.2%, and China 2.2%—incredibly the remaining 25% of all overseas-born Australians represent other cultural minorities (Census QuickStats: Australia, 2016). This includes almost 650,000 First Nations’ Australians, encompassing multiple nations and language groups as well as some 800,000 refugees and displaced persons from across the globe since 1945 (Australian Human Rights Commission, 2018a).
Immigrants and refugees are more likely to suffer from chronic health conditions (Murray & Skull, 2005), which are then compounded by risk factors, such as poverty and discrimination as well as difficulty accessing culturally appropriate healthcare services (Department of Health, 2018; Gracey, 2014).
The impacts of marginalization on health outcomes are also seen in many other cultural minority groups within Australia. Australia’s Aboriginal and Torres Strait Islander communities endure a markedly lower life expectancy—a 10.6-year gap—compared to nonindigenous Australians (Census QuickStats: Australia, 2016). The suicide rate is more twice that of the nonindigenous population at 23.8 deaths per 100,000 (Abs.gov.au, 2020). Aboriginal Australians makeup 28% of the custodial population despite being just 2% of the population and are more likely to experience health issues, including substance use and mental health issues with incarceration rates increasing in Australia (Lloyd et al., 2017). The impact of colonization, forced separation of families across generations, dispossession from lands, health difficulty, and ongoing interaction with the justice system exacerbates this cycle of health disparity and socioeconomic loss.
Despite a history of significant discrimination, LGBT communities are also more visible, with 3% of Australians now comfortable to publicly identify themselves as LGBT or other in Australia’s last census (Census QuickStats: Australia, 2016) and increasing numbers of Australian men (9%) and women (15%) reporting same-sex attraction in a large nongovernment survey (Royal Australian and New Zealand College of Psychiatrists (RANZCP), 2019). However, mental health outcomes for LGBT communities are among the lowest of any demographic, primarily due to discrimination, with same-sex attracted people more likely to experience suicidality (RANZCP, 2019). Emerging evidence also reports significant health disparities that extend across multiple health outcome parameters for LGBT populations (Hafeez et al., 2017). It should thus be of great concern that more than one-third of LGBT people in Australia withhold their sexuality or gender when accessing public services and when these very services are required to close such health gaps (Australian Human Rights Commission, 2018b).
Indeed, when we consider that more than one-third of the Australian population is now composed of CALD communities, it is absolutely paramount that healthcare practices reflect Australia’s pluralistic society. It is also important that future doctors possess the relevant skills of cultural competence to meet the needs of Australians, with evidence demonstrating that this can benefit CALD patients through improved clinician understanding, knowledge, and attitudes (Crandall et al., 2003; Horvat et al., 2014).
Medical Education in Australia
The Standards for Assessment and Accreditation of Primary Medical Programs by the Australian Medical Council (AMC, 2012) provides a framework of reference for the core components of medical education (AMC, 2012). This allows the development of local medical school curricula among the 20 (Accredited Medical Schools, 2020) medical schools in Australia. It alludes to the significance of obtaining cultural competence, in part by borrowing from the definition put forth in a statement by the Medical Council of New Zealand (AMC, 2012): “Cultural competence requires an awareness of cultural diversity and the ability to function effectively, and respectfully, when working with and treating people of different cultural backgrounds.” (AMC, 2012, p. ii)
In the current AMC Standards, there is a clear demarcation between its consideration of the Aboriginal and Torres Strait Islander populations and those of other CALD backgrounds. The former is well described, the AMC aims for medical graduates to specifically understand factors: “including history, spirituality and relationship to land, diversity of cultures and communities, epidemiology, social and political determinants of health and health experiences.” (AMC, 2012, p. 3)
As such, the integration of Indigenous teaching into medical school education has been emphasized, although the practical translation of this teaching is not well articulated. In addition, although there is preliminary research into how cultural competence can help minimize health inequities in Indigenous Australians, this is largely qualitative (Bainbridge et al., 2015), and thus tangible outcomes have not yet been sufficiently demonstrated.
However, CALD populations beyond First Nations’ Australians are not well represented by the AMC Standards. Outside the AMC’s definition of cultural competence, there is a point pertaining to diverse populations, which merely mentions the: “health, illness, disease and success of treatment of populations.” (AMC, 2012, p. 3)
In attempting to account for the breadth of populations in Australia, this statement is broad and does not necessarily acknowledge the minority populations, especially those at greatest risk of harm. Moreover, it is nebulous; if there are no tangible goals on which a curriculum can be established, there is little imperative to integrate it in a meaningful way.
The need for a clearer stance and overall better teaching on cultural competence has long been identified: “In general practice we are all individual . . . I think our organization deals better with people from our own culture than with people from CALD groups. It’s not on purpose, it’s just that they are a minority.” (Komaric et al., 2012, p. 322)
Woodward-Kron et al. (2016) also highlight two pertinent themes: First, a poor understanding of other cultures was a significant impediment to building rapport, perpetuating the divide between patient and doctor, and the second one of the biggest barriers to effective intercultural communication was uncertainty, stemming from a lack of exposure to these situations: “I really didn’t know what to do. ” Woodward-Kron et al. (2016, p. 88)
Australian medical schools are not alone in struggling to meaningfully identify or translate effective cultural competence strategies with regard to known health disparity for minority groups. Within the context of cultural competency relating to LGBT populations, much can be done at the curriculum level to improve LGBT education and training in a range of domains (Cooper et al, 2018). Importantly, lack of knowledge and understanding was identified as a key factor, leading to bias and cultural misunderstanding of members of this group. A similar call for medical curriculum improvement for the LGBT group has also arisen in Africa (Müller, 2015). This is a gap in the framing of The Standards for Assessment and Accreditation of Primary Medical Programs by the Australian Medical Council (AMC, 2012) as it poorly recognizes this minority group with considerable health disparity.
Reformulating the Curriculum to Promote Change
Sukhera and Watling (2018) have devised a framework for integrating implicit bias recognition into health education. They note that unconsciously held biases can shape healthcare decisions and unfavorably affect the outcome of a wide range of minority groups to exacerbate health disparities. Their 6-point framework offers potential points of leverage for curriculum improvement and change. It can be summarized as follows: 1. A safe learning environment; 2. Increased knowledge of implicit bias; 3. How bias influences behavior, decisions, outcomes and disparities; 4. Increased self-awareness; 5. Efforts to reduce bias; and 6. Awareness of the effect of bias on others. This then reaches out to all groups that may belong to a health minority.
Harvard Medical School (White et al., 2017) has also reformulated the approach to culture and has picked up similar themes to Sukhera and Watling (2018), including self-awareness, with a model that asks medical students to reflect on who they are and then frame the interaction with others in a dyadic manner. The Harvard model attempts to move beyond a focus simply on a definition of cultural competence as one of seeing and creating hypotheses. Instead, it emphasizes an understanding of self-identity in relation to one’s own culture as the reference point to see the culture of others in a transactional and deeper manner (White et al., 2017).
Cultural Competence and Patient / Consumer Coproduction
The medical curriculum may be limited in time, but the possibility for further added value should always be carefully considered. Patient/consumer codesign and coproduction of medical education adds to the existing strategies used in patient participation in medical education. This value is further refined when patients who experience inequity contribute to learning design and the curriculum.
There is a debate that focuses on the language that describes healthcare users who may not wish to be known as “patients” but rather as “consumers.” This may address a power imbalance between the person experiencing the illness and the clinician as a provider or reframe a stigmatizing diagnosis. If a recovery-oriented approach is taken, patients may become well and then go on to share their stories in the absence of illness. When unwell, people may prefer the term patient (Costa et al., 2019); however, this is not so clear now with the term consumer regularly used (Goldstein & Bowers, 2015; Mold, 2015; Wolf, 2018). In promoting a culture that embraces the input of people with lived experience of illness, the authors wish to use both terms.
A potential way forward is to ask patients/consumers to contribute to the wealth of the curriculum. Their stories and guidance in shaping the curriculum will authentically fill gaps that educators can otherwise only imagine, increasing understanding, highlighting possible biases, increasing self-awareness, and promoting reflection. Indeed, first-person stories have been employed successfully at medical schools, translating an idea into action via mechanisms that promote cognitive dissonance, reflection, and reevaluation in the medical student cohort (Kumagai & Lypson, 2009). This displaces the potential effect that clinician bias may exacerbate disparity because it is a genuine attempt to see and know people in partnership.
Coproduction is a concept borne outside medicine, in industry, some decades ago. One of the earlier definitions of coproduction simply stated it as “the contribution of service users to the provision of services” (Realpe & Wallace, 2010). As medical practitioners, the tradition of doing things “to” or “for” a patient can be displaced by a move to “doing with” a patient/consumer via the codesign and coproduction paradigm. This process is far more participatory than simply being a patient role player. At all points, there will be checking in to see that what the patient/consumer sees as important is present in terms of content.
Successful coproduction involves co-planning, codesign, codelivery, and co-evaluation to ensure a shift in the balance between expert-led design to that of a culture that also values input from patients/consumers (Roper et al., 2018). It is patients/consumers who have knowledge and expertise to assist the framing and balance in the curriculum to meet community needs.
Slay and Stephens (2013) see codesign as people’s voices being heard, debated, evaluated, and acted upon and the coproduction as the opportunity to deliver the service they have just shaped. This is then a process of active participation. Batalden et al. (2015) view coproduction in health care as the act of patients and professional groups engaging in civil discourse as they co-plan and execute coproduced high-value health care that improves outcomes. The personalized experience of patients/consumers can create value and ensure quality for a health organization in the process of coproduction via active collaboration (Turakhia & Combs, 2017).
The work of the Maori nurses in understanding the wishes of the Maori population to reduce health disparity appears to attain high levels of cultural competence and is an example of coproduction (Papps & Ramsden, 1996; Ramsden, 1990). Similarly, Leckning et al. (2020) reported work by experts to design a practice guideline for the psychosocial assessment of Aboriginal and Torres Strait Islander people presenting to hospital with self-harm and suicidal thoughts by 12 Aboriginal and Torres Strait Islander people and 16 nonindigenous people. Although not an educational example, it is another example of culturally competent codesign.
Codesign and coproduction at the micro-system level improve patients’ experiences with treatment and care (Vennik et al., 2015). Coproduction also shifts the medical student from considering a paternalistic frame of care to one of shared decision-making and responsibility for health care (Ewert & Evers, 2012), with an increase in the total resources available for care, especially if relatives or other members of the community are positively engaged in the treatment plan. This cocreation of care is also satisfying for staff (Ding et al., 2019) who learn about a patient’s story. Encountering patient stories is extremely rewarding for medical students (Kumagai et al., 2008), as is the process of understanding their own narrative as the reflective other (Warmington & McColl, 2016), with possible benefits in terms of insights into one’s own resilience strategies as future medical practitioners (Jenkins et al., 2018).
Vijn et al. (2018) achieved a coproduced training program inviting the input of four main groups: patients (chronic and oncologic disease), students, care professionals, and educational professionals. This was run in an evolving quality cycle that reported some attention to balancing factors, such as ethnic and socioeconomic status. This improved patient-centered care and was rapidly responsive via a plan do study act framework.
Building on Vijn et al. (2018) and while holding the Sukhera and Watling (2018) six-step frame in mind, as well as the reflective and transactional aspects developed at Harvard (White et al., 2017), a positive way forward may be to take a local approach in curriculum design. In a deliberative way, the people in the local population who experience health disparity or known to be subject to clinician bias need to be identified. Careful mapping of the local population should occur to assist with curriculum development.
Coproduction should emphasize the three elements of knowing others, knowing self, and knowing biases while covering key educational material. The authors recommend the following method to include CALD stakeholders, within a local community region, given the evidence of bias and the value of patients’/consumers’ own contributions that can be tailored to the existing medical curriculum. We outline a seven-phase approach to achieve curriculum alignment with local CALD stakeholders that ends with successful codesign and coproduction (see Table 1). Such a framework can be applied to specifically selected populations of any cohort to ensure that contributions to the curriculum emphasize cultural understanding, in turn potentially reducing known health inequity. Such a framework is reflective and has a quality improvement cycle, and as such gains may potentially be amplified.
Phased Development to Achieve Coproduction.
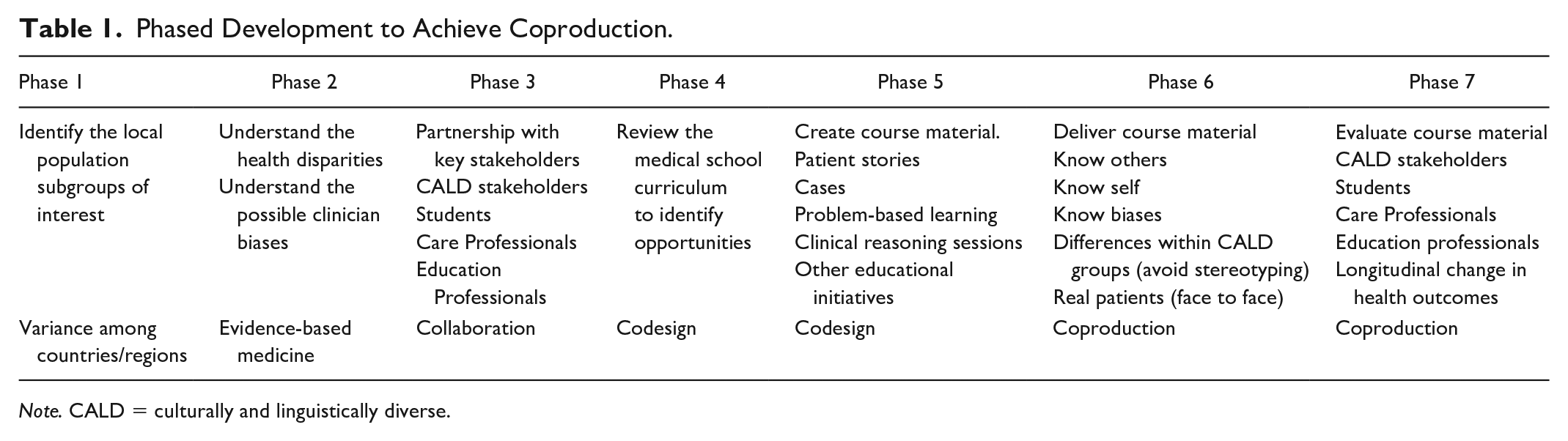
Note. CALD = culturally and linguistically diverse.
All medical students see patients during clinical years. Yet depending on geographic sites and the duration of programs, mere reliance on clinical encounters alone may not provide the depth or breadth of opportunities, in particular with respect to exposure to population segments. Medical schools may design cases that revolve around problem-based learning (PBL) sessions, clinical reasoning skills, or a similarly structured learning set. Within the context of this learning, the student may encounter a patient vignette with varying degrees of sociocultural detail, depending on the learning outcome(s). Some vignettes encountered in medical school need to be culturally diverse, representing the various CALD segments in various locations and allowing student reflection and discussion. Patient scenarios can equally apply to a person who does not speak the main languages of the region, of a socioeconomic group, or of a minority. The production of PBL cases and vignettes without input from germane parties can be perceived as being overly or negatively stereotyped and lacking in authenticity (Kamaka, 2010; Lypson et al., 2008). The codesign and coproduction of educational material by CALD stakeholders, students, care professionals, and education professionals will enhance the curriculum. This is in addition to the inclusion of face-to-face encounters with diverse groups of local patients/consumers who experience health inequity.
Three vignettes have been provided as examples, modeled on actual patient stories. The authors suggest they more likely represent material produced by coproduction, drawn from patient population segments likely to experience health disparity within the Australian context (see Box 2). The cases serve as prompts, creating exposure and stimulating learning. They are unique and represent individuals within populations. Multiple stories and inputs from people across the curriculum will promote understanding of the diversity within local groups and a greater opportunity for reflection among students.
Patient Stories From the Australian Context.

Evaluative processes should focus inclusively on CALD stakeholders, students, care professionals, and education professionals. It may be possible to take a longitudinal approach and consider the impact of such a program on specific health disparities.
The Importance of Real Patients and Their Stories
There is a preference among medical students for “real” patients (Lypson et al., 2008). Promisingly, involving patients in curricula can be resoundingly effective. Zanetti et al. (2014) found that workshops facilitated by individuals representing minority communities were received particularly well by students and factored into their appreciation of cultural competence. Roh and Nirta (2018) reported similarly positive findings with the introduction of a cultural diversity program where multicultural guests were the speakers. In a more formalized setting, the discipline of mental health has now realized the potential of patient/consumer coproduction and is using this tool to calibrate better systems of working with rather than working for (Reeve et al., 2016).
Limitations
In examining the Australian population, the authors have considered evidence from the international literature, which may not apply within the Australian context. The focus on the Australian context allows specific examination of gaps and disparity in one region and reflection on the manner in which cultural education might be more effectively delivered. This may serve as a source for local reflection and international adaptation as each region has specific challenges related to addressable health disparity.
Conclusion
Medical students face the herculean task of navigating an ever-expanding palate of information. The medical faculty frames the learning and is often faced with very difficult choices about what to keep and what to forgo. Amid this tension, there is a rising expectation from the community that as clinical academics, we will be able to formulate this difficulty and arrive at the very best solutions for the community.
Defining our curriculum, without reference to or participation of people who have the greatest health disparities, risks a disservice to those who may gain the most from health care. There is emerging evidence that thoughtful inclusion, where we walk in partnership with patients/consumers, may deliver better health for people in minority cohorts.
Reframing the medical curriculum using principles of codesign and coproduction, via the appointment of willing outsiders who can work with students, care professionals, and education professionals to help them know themselves, others, and to become aware of their biases may extend the curriculum and add value for all who participate.
Each country faces a very specific set of challenges within the context of the local population. National medical school standards may be very general and not capture the nuances of complex heterogeneous populations with health disparity. A thoughtful effort may enrich medical faculties who might find they learn a few lessons from the outside, creating solutions with new partners that were not otherwise seen. In turn, this may promote generational change within the workforce to address health disparities within our communities. Codesign of medical curricula to address health disparity is a fertile area for future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.