
Abstract
The inclusion of First Nations health curricula in programs is critical for the development of culturally safe graduates, however, less is known about how to embed content into curriculum in ways that reflect best practice and pedagogy. The aim of this scoping review was to describe methods and processes of First Nations health curriculum development in nursing, medical, dentistry, and allied health entry-level programs in international peer-reviewed journals. Systematic searches of databases were completed including CINAHL, Proquest, Medline, and Informit; with additional searches in Google Scholar and First Nations-led journals. A total of 104 articles met inclusion criteria; the majority relating to medicine (n = 38) and nursing/midwifery (n = 17) student cohorts. Methods and processes for embedding First Nations health content are described, including First Nations-led development and co-leadership, resulting in a suggested model for curriculum development. Evidence-informed curriculum development is critical to ensure effective methods and processes are adopted and cultural safety learning outcomes are achieved.
Introduction
The purpose of this research was to complete a scoping review of international peer-reviewed journal articles on processes and methods of First Nations health curriculum development in nursing, medical, dentistry, and allied health entry-level programs. First Nations peoples 1 in Australia hold continuing worldviews, thousands of years old. These worldviews have formed concepts, principles, and perspectives for education, health and wellbeing, social systems, agriculture, trade, governance, and law. British invasion, through the imported doctrine of Terra Nullius 2 positioned these fields of knowledges as invisible along with the First Nations peoples. From this context, teaching and learning in higher education continues to be predominantly informed by Western knowledges and colonialist understandings of truth. Challenging colonial agendas and including First Nations ways of knowing, being and doing will begin to decolonize health education. A decolonization process includes embedding continuing First Nations perspectives, and contemporary understandings formed through the intersection with Western knowledges and the resistance to ongoing colonial oppression (Fellner, 2018). This transformative, decolonizing process begins with acknowledging the continent, the First Nations peoples and the Country 3 that curriculum is developed and taught on. The authors would like to acknowledge the unceded sovereign lands of the Dja Dja Wurrung, Yorta Yorta, and Wurundjeri peoples. We acknowledge First Nations continuing ways of knowing, being and doing, and honor the ongoing teachings from Ancestors, Elders, Community, and Country.
Western knowledges will remain epistemologically dominant if health disciplines and practitioners do not first critically and honestly reflect on their own identity and the current hegemony of Western knowledge. In this context, the authors would position themselves; two authors (SG, Badimia Yamatji and MM, Yorta Yorta) are proudly First Nations women who bring a research perspective firmly grounded in First Nations ways of being. We work at the interface of two knowledge systems and believe that when First Nations and Western knowledges are recognized and valued equally, respectful innovative ways of working can emerge (Nakata, 2007). We are committed to creating change by applying a decolonization lens to this research.
Five authors are non-Indigenous of white European ancestry (NH, CM, NL, MW and CB). We approached this research acknowledging our own Western, white lens and knowledge systems, and the biases that accompany this worldview. Throughout the conduct of this review it was important for us to intentionally engage in a two-way, critically reflexive process of knowledge sharing and decision making that aims to minimize the impact of our biases on the scoping review process and outcomes, and privilege First Nations perspectives and processes in the conduct and the outcomes of the research.
Decolonization is defined by Fellner (2018) as an “active, intentional, moment-to-moment process that involves critically undoing colonial ways of knowing, being, and doing, while privileging and embodying Indigenous ways of knowing, being, and doing” (p. 284). Fellner (2018) conceptualizes decolonization of curriculum as an interwoven process using First Nations counter-narratives to deconstruct “colonial ideologies and their manifestations” (p. 284). Disrupting the colonial mindset and privileging First Nations continuing intellectual sovereignty (Rigney, 1999) will improve program curriculum, student learning experiences and graduate outcomes for all entry-level health students. Embedding First Nations perspectives in curriculum positions First Nations worldviews about health and wellbeing for the benefit of both First Nations people and non-Indigenous people. This “both ways” approach to teaching and learning supports student’s critical thinking and capacity to challenge the dominant Western knowledge systems (Nakata, 2004) and creates a “sense of place and identity” for Indigenous students (Fredericks et al., 2017, p. 128). Addressing the privileged position of Western knowledge in health programs promotes the consideration of equal but different ways of thinking, being and doing that resonate with diverse client groups and prevents graduates from being complicit in the ongoing oppression of First Nations peoples (Al-Natour & Mears, 2016; Rose, 2012).
Decolonizing curriculum aims to achieve epistemological equality for First Nation’s knowledges in entry-level health programs (Bennett, Coghlan et al., 2018; Zubrzycki et al., 2014). Decolonizing program curricula is critical to enhance the capacity of graduates to work with First Nations peoples and communities to improve health outcomes and to address the major inequities in health systems and health care, including pervasive issues such as implicit bias and institutional racism (Australian Health Practitioner Regulation Agency, 2020; Department of Health, 2014). Entry-level health education has a role in achieving these objectives, which is now embedded in professional competency standards and program accreditation requirements across health professions in many countries (Department of Health, 2014; Indigenous Physician Association of Canada, 2008; Occupational Therapy Council of Australia Ltd, 2018; Zubrzycki et al., 2014).
Curriculum development is a multi-stage process of planning, design, implementation, and evaluation of teaching and learning content (Khan & Law, 2015), and the objective was to identify and describe processes and methods used for First Nations health curriculum development for health programs. Best practice frameworks for teaching and learning in First Nations health exist that stipulate what curriculum content themes and learning outcomes need to be embedded (Department of Health, 2014). However, a review of existing literature was needed to understand how curriculum is developed and embedded and the scope of methods and processes used. Other relevant issues for First Nations health curriculum development, including curriculum impacts and outcomes, have been well established within curriculum frameworks (e.g., Department of Health, 2014) and in other recent published literature reviews (Francis-Cracknell et al., 2019; Kurtz et al., 2018; Pitama et al., 2018). This scoping review of curriculum development methods and processes provides timely evidence that contributes to the growing knowledge base that is needed to guide this work.
Method
Study Design
The study design was a scoping review as defined by Arksey and O’Malley (2005). The scoping review method was selected to determine what is published on the topic and to identify gaps and issues for future research (Arksey & O’Malley, 2005). The scoping review was informed by best practice methods and principles for access to, interpretation and use of First Nations Knowledges in research, for example the inclusion of additional searching methods to ensure First Nations perspectives were located (National Health and Medical Research Council, 2018; Rigney, 1999). The review method incorporated five stages as described by Arksey and O’Malley (2005) to scope the existing literature, with additional strategies to locate First Nations health literature including manual searches of key First Nations journals and the inclusion of additional charting categories: First Nations authorship and the nature of involvement of First Nations peoples.
Stage 1. Identify the Research Question
The search question was “What methods and processes are used for First Nations health curriculum development in entry-level (pre-registration) nursing, medicine, dentistry, and allied health programs in international peer-reviewed journal articles?”
Stage 2. Identifying Relevant Studies
Search terms were developed to guide systematic databases searches. The combination used across all databases included search terms for First Nations population AND nursing, medicine, dentistry or allied health AND curriculum development (refer to Supplementary information for table of search terms). A total of four databases were searched using this strategy, including CINAHL, Proquest Central (which includes ERIC), Medline, and Informit. Google Scholar was used to locate any additional articles that were published by key authors (those with multiple publications in the search results). Citation searches were also completed using Google Scholar to locate relevant publications that had cited key curriculum frameworks including Committee of Deans of Australian Medical Schools (CDAMS) Indigenous Health Curriculum Framework (Phillips, 2004) and Getting it Right (Zubrzycki et al., 2014) and the Aboriginal and Torres Strait Islander Health Curriculum Framework (Department of Health, 2014).
First Nations literature is not always located through database searches, therefore additional searches were conducted in First Nations-led journals including the Australian Journal of Indigenous Education, AlterNative: An International Journal of Indigenous Peoples, and the Leaders in Indigenous Medical Education (LIME) Good Practice Case Studies and relevant articles were identified for screening. Reference lists of included articles were reviewed during the full text screening stage. All titles were checked by at least two researchers at title/abstract and full text screening stages to determine if they met the inclusion criteria. The inclusion criteria were: (1) published in English language, (2) article published in peer-reviewed scholarly journal, (3) must identify a First Nations population, (4) must identify an entry-level medical, nursing, dentistry, or allied health program, (5) must describe a method or process of curriculum development, and (6) must identify a curriculum outcome. The results of these searches are provided in the PRISMA diagram (Figure 1).

PRISMA.
Stage 3. Study Selection
Title/abstract and full text screening was completed by the research team with each title reviewed by at least two researchers. A third researcher was consulted for conflicts. The most common reason for exclusion was no description of curriculum development. This screening process resulted in a total of 104 articles identified for inclusion. Endnote and Microsoft Excel software programs were used to manage screening processes.
Stage 4. Charting the Data
Data was extracted and charted in Microsoft Excel using the standard fields as outlined by Arksey and O’Malley (2005) and fields that relate to the review question. These fields were: author, year, article title, journal title, health discipline, First Nations population, article type, study aim, study location by country, population/sample, study design and methods, frames of reference, curriculum development method, curriculum development outcome/s, First Nations authorship, and involvement of First Nations peoples.
Stage 5. Collating, Summarising, and Reporting the Results
The literature was analyzed using inductive, summative multiple method content analysis starting with quantitative content analysis to identify the range of methods and processes used for First Nations health curriculum development and count the frequency of use in included articles (see Findings, Table 2). This was followed by qualitative analysis to describe and provide context for the methods and processes identified (QUANT-Qual) (Hsieh & Shannon, 2005). The included articles were reviewed to locate First Nations-identified authors, because First Nations health curriculum development should be led by First Nations knowledges, and knowledge production resulting from this review must privilege First Nations voices (Rigney, 1999).
Findings
Summary of Results
A total of 104 articles were located on First Nations health curriculum development that met the review criteria. The full table of the 104 included studies is provided in the Supplementary file. Of the 104 included articles, 51% were teaching and learning project reports (n = 53), defined as a descriptive article that did not identify research methods and may or may not have had research ethics approval. Forty-eight percent were original research articles (n = 50) that reported research methods and ethics approval. One keynote paper was included (Huria, Lacey, Melbourne-Wilcox, & Pitama, 2017). All studies were located in colonized countries, including Australia (n = 68), Aotearoa/New Zealand (n = 16), Canada (n = 12), and the United States of America (USA) (n = 8). No date limits were applied to the searches to determine the scope of the literature by year of publication. This is presented in Figure 2 which indicates that articles were published from 1995 to 2019 and demonstrates the significant contribution by LIME Good Practice Case Studies publications (26% of included articles).
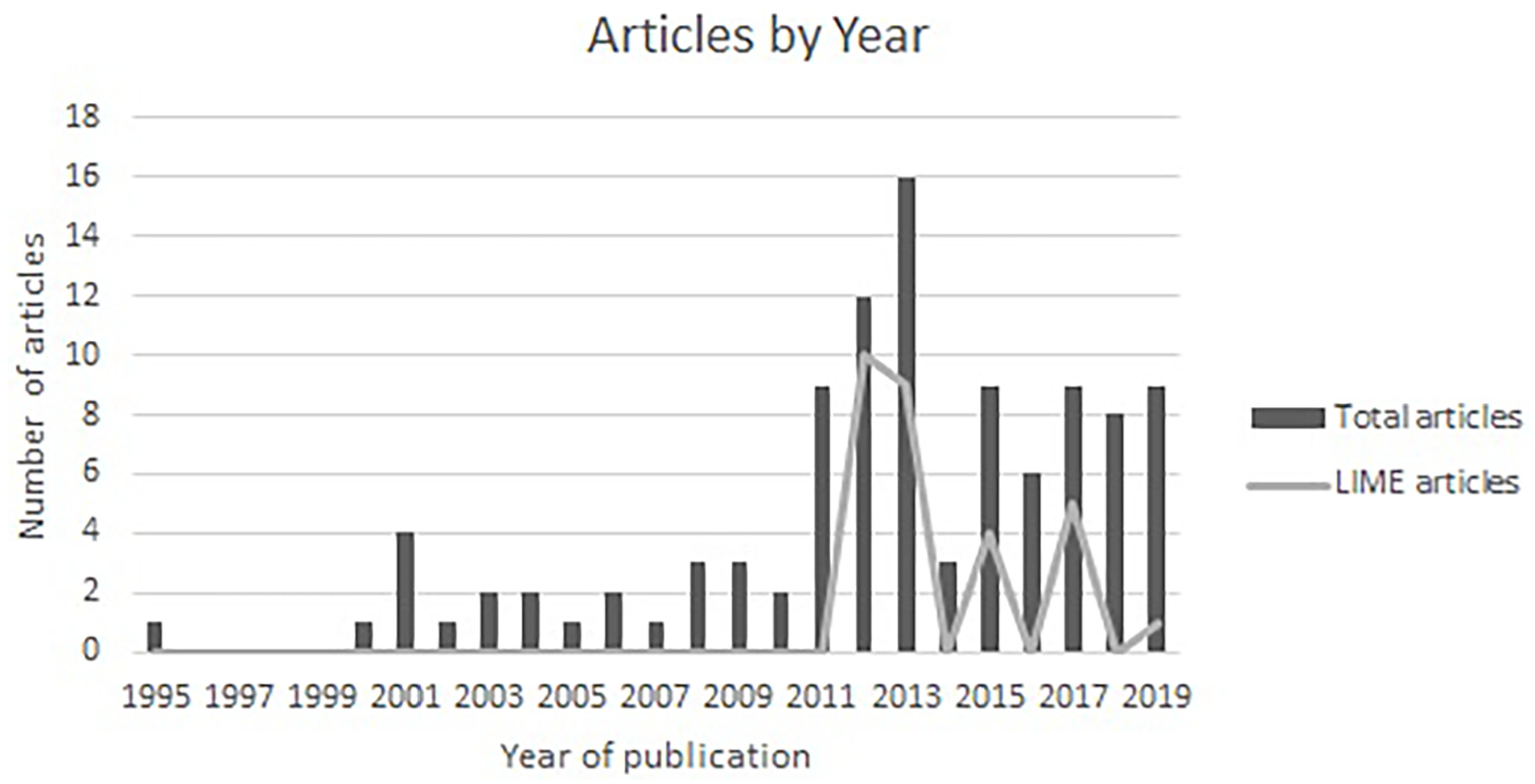
Studies by year of publication.
Articles were more commonly published in First Nations-led publications including the LIME Good Practice Case Studies (n = 27) and The Australian Journal of Indigenous Education (n = 6), in addition to mainstream health journals, including Australian Psychologist (n = 4), Contemporary Nurse, Australian Journal of Rural Health, BMC Medical Education, and Focus on Health Professional Education (all n = 3). No other journal published more than two included articles.
The included articles were charted by student discipline cohort (see Table 1). The category interprofessional (n = 12) was used to define student cohorts with more than one discipline in the same classroom. The category multidisciplinary (n = 9) was used to define interprofessional curriculum developed for more than one discipline specific cohort including whole of department or university projects (Andersen, 2009; R. G. Jones, 2011, 2012).
Studies by Discipline of Student Cohort.

Examples of interprofessional learning include the Curtin University (Australia) interdisciplinary Indigenous Health unit delivered with 22 disciplines (Bullen & Roberts, 2019a, 2019b; Goerke & Kickett, 2013; Hendrick et al., 2014; Kickett et al., 2014), a Maori Health Week activity (Aotearoa/New Zealand) for pharmacy, medicine and nursing students (Horsburgh & Lamdin, 2004; Kairuz & Shaw, 2005), and an online module on culturally sensitive care developed for nursing, medicine, health promotion and social work students (Canada) (Carter & Rukholm, 2009). Twenty-four articles explicitly identified First Nations authorship and three articles stated that all authors were non-Indigenous. In 74% of included articles author positionality was not clearly stated (n = 77).
Methods and Processes for Curriculum Development
The included articles were charted and analyzed to identify methods and processes used for First Nations health curriculum development. The methods and processes are presented in Table 2 and described in a narrative synthesis. Table 2 reports the number of included articles in each category and references (first author surname and year of publication). The narrative synthesis presents definitions and descriptions of the processes/methods and references included studies to draw attention to examples and exemplars. Not all included articles are referenced in the narrative synthesis for each category because of the large number of included articles. Included articles often utilized multiple methods for curriculum development therefore interrelationships between categories are highlighted. The processes/methods are presented in order of frequency in Table 2 and in the narrative synthesis, from more prevalent or frequently used to least prevalent, to provide a lens for interpreting the scope of the literature. Following the narrative synthesis, the scoping review findings has been further interpreted in Table 3 to provide a visual interpretation of the key methods and processes in a suggested model for First Nations health curriculum development that illustrates the scoping review findings.
Curriculum Development Methods and Processes Listed in Order of Frequency.

A Suggested Model for First Nations Health Curriculum Development.

Student Consultation via Surveys, Interviews and Focus Groups
Student consultation was conducted via surveys, interviews and focus groups (n = 47). Surveys were used to evaluate student learning and to inform ongoing curriculum development. Curriculum development processes involved consultations with First Nations students specifically in two instances (Haight et al., 2019; Zuchowski et al., 2013).
The majority of articles in this category conducted student consultations using survey tools for longitudinal and pre- and post- curriculum evaluation. Institutional subject (course) evaluation survey data was used in seven studies to inform curriculum development and evaluate student satisfaction and learning outcomes (Bernhardt et al., 2011; Gair, 2016; Kamaka, 2013; Kickett et al., 2014; Mortley, 2011; Ryder & Edmondson, 2015; Ryder et al., 2013). In five articles, brief feedback surveys were collected immediately after the delivery of a learning activity (Harmon-Vukić & Schanz, 2012; Paul et al., 2015; Smith et al., 2015; Soucy et al., 2013; Tobin et al., 2015). Survey tools used with students included the Preparedness to Practise Questionnaire adapted for an Aboriginal health context (Paul et al., 2006, 2013, 2019), the Cultural Capability Measurement Tool (West et al., 2019), the Racism, Acceptance, and Cultural-Ethnocentrism Scale (Grigg and Manderson (2015) in, Power et al., 2018), and the Readiness for Interprofessional Learning Survey (in Horsburgh & Lamdin, 2004; Kairuz & Shaw, 2005).
Researchers utilized interviews and focus groups with students to gain more in-depth perspectives and understanding of learning experiences (Forsyth et al., 2019b; Haight et al., 2019; Horsburgh & Lamdin, 2004; Kairuz & Shaw, 2005; Svarc et al., 2018; Thackrah et al., 2017; Zuchowski et al., 2013) including a Talking Circle (Lowe & Wimbish-Cirilo, 2016).
Relationship Building
Curriculum development involved relational work and building partnerships with First Nations peoples and communities within and external to the university (n = 37). This category includes studies that explicitly described processes used to build genuine relationships with First Nations peoples and communities as a key process for curriculum development.
Curriculum development involved building relationships within universities and with external community partners. Relationship and partnership building was embedded in curriculum development processes and was identified as key to achieving outcomes (Andersen, 2009; Andrews, 2012; Bennett, Coghlan et al., 2018; Bernhardt et al., 2011; Broughton, 2010, 2013; Haight et al., 2019; Horsburgh & Lamdin, 2004; Jacklin et al., 2011; B. Jones & Ingham, 2013; MacLeod, 2012; Morgan et al., 2009; Pitama, 2012; Power et al., 2018; Ross et al., 2013; Ryder & Edmondson, 2015; Virdun et al., 2013; Woolley et al., 2013). Relationship building was integrated in pedagogy. Bernhardt et al. (2011) described relationships built on trust and respect to be the underlying philosophy for their audiology and speech-language pathology program. Students were reported to value Indigenous health curriculum that included building relationships with peers and educators (Huria, Palmer et al., 2017).
At Curtin University, researchers identified that relationships between internal university departments were key to the development and implementation of the first year interprofessional Indigenous Cultures and Health Unit (Flavell et al., 2013; Hendrick et al., 2014). Authors from the Centre for Aboriginal Medical and Dental Health (University of Western Australia) argued that “staff built on existing relationships to gradually introduce content using a partnership approach” (Paul, 2012, p. 30), and warned that “inclusion of content without the associated partnership and collaboration” contributes to tokenism (Paul et al., 2013, p. 11). Seven articles in this category identified that commitment to collaborative and respectful relationships was critical for sustainable university-community partnerships required for effective curriculum development and delivery (Bernhardt et al., 2011; Carter & Rukholm, 2009; Duffy et al., 2013; Flavell et al., 2013; Hays, 2002; MacLeod, 2012; Tobin et al., 2015). Relationship building was critical for non-Indigenous educators engaged in First Nations health curriculum development work (Schmidt, 2019).
Partnership development was critical for clinical placements and cultural immersions with First Nations community organizations and health and medical services (Carriage et al., 2017; Crampton et al., 2003; Dowell et al., 2001; Huria, 2012; Nelson et al., 2013; Paul et al., 2019; Pitama, 2012; Thackrah et al., 2017; Tobin et al., 2015; Warren et al., 2016). Relationship building and partnership development was integral to First Nations-led development and was supported through First Nations teaching and subject coordination, and by appointing a First Nations reference or advisory group.
First Nations Teaching and/or Subject Coordination
First Nations educators (including academics, health professionals, community members, and Elders) were appointed by universities in teaching and subject coordination roles to develop and deliver curriculum (n = 37). Educators were appointed to develop teaching and learning content for assessments, guest lectures, short modules, entire subjects, and programs. Across the 37 articles, appointments included simulation patient, academic, educational design, and cultural advisor positions and to take part in educational events. Bolton and Andrews (2018), for example, describe the value of First Nations health teaching in Indigenized place and space (Melbourne Museum Bunjilaka Gallery).Elders were employed in cultural immersion programs with positive student feedback (Crampton et al., 2003; Dowell et al., 2001; Moffitt, 2016; Tobin et al., 2015). Indigenous community members employed in tutor and simulated patient roles found that students were respectful and actively participated in and appreciated the educational experience (Ryder et al., 2013). At Curtin University, 50% (n = 25) of tutors in the first year interprofessional Indigenous Cultures and Health Unit were Aboriginal (Kickett et al., 2014). The subject was coordinated by a Noongar academic “who is a highly respected community member and elder” (Kickett et al., 2014, p. 39).
Appointing First Nations educators in teaching and subject coordination roles was critical for curriculum development and had benefits of connecting students with First Nations professionals and leaders, countering negative stereotypes, and increasing understandings of cultural diversity (Kickett et al., 2014; McDermott & Sjoberg, 2012). First Nations teaching and subject coordination was supported through First Nations led development, co-leadership, relationship building, and First Nations consultation and collaboration.
Consultation With First Nations Educators
First Nations educators (academics, health professionals, community members, Elders) were consulted by university staff for knowledge and expertise to inform curriculum development (n = 33). First Nations peoples were contracted for curriculum development work in positions including Indigenous adviser, mentor or project consultant (Gair et al., 2003). First Nations community stakeholders were consulted for input into curriculum design including Elders and community leaders and professionals from Indigenous community controlled organizations (Bennett, Redfern, & Zubrzycki, 2018; Bernhardt et al., 2011; Carriage et al., 2017; de Leeuw & Finnigan, 2012; Hendrick et al., 2014; Horsburgh & Lamdin, 2004; Huria, 2012; R. G. Jones, 2011; Mahara et al., 2011; Moffitt, 2016; Nash et al., 2006; Nelson-Hurwitz et al., 2019; Power et al., 2018; Thompson, 2001). Consultations included working with Aboriginal film makers and creative content producers (Bennett, Redfern, & Zubrzycki, 2018; Jackson Pulver, 2012).
At the Māori Indigenous Health Institute, University of Otago, Christchurch, Māori simulated patients were asked to provide feedback on the scenarios in advance of workshops (Huria et al., 2013). Power et al. (2018) consulted key Indigenous stakeholders in two different forums to develop a graduate attribute, including Indigenous health, education and policy workers and Indigenous health professionals working in roles specific to Indigenous health care (p. 844). Ryder et al. (2013) described a “values consultation interview process” undertaken with Elders, Aboriginal Health Workers and Community representatives (p. 20).
Interviews with stakeholders were reported to ensure curriculum was culturally appropriate and authentic, incorporated First Nations perspectives, and was supported by strong local connections (Nelson-Hurwitz et al., 2019; Sullivan & Sharman, 2011). Nguyen and Gardiner (2008) explored the issues impacting on First Nations community involvement in medical education, including motivations, barriers and required supports. First Nations consultations provided critical scrutiny of content and input to counter what has been traditionally white-centered allied health curriculum (Gair et al., 2003; Wilson et al., 2015).
First Nations-Led Development
Twenty-seven included studies explicitly identified First Nations leadership as central to curriculum development. First Nations-led development is inclusive of other methods and processes identified in this review including relationship and partnership building, First Nations teaching and subject coordination, and working with a First Nations reference or advisory group.
Curriculum development at the Otago Medical School in Aotearoa/New Zealand identified Indigenous leadership as a key component of their 9-year process that has produced curriculum effective for increasing students’ knowledge of racism and bias (Huria, Lacey, Melbourne-Wilcox, & Pitama, 2017), supporting them to see “Indigenous health curriculum as an equal part of their medical education” (Huria, Palmer et al., 2017, p. 7). At Otago, First Nations-led curriculum development ensured Indigenous principles and culturally safe ways of working were embedded in the process (Huria, Palmer et al., 2017; Pitama, 2012), enabling increased community involvement in teaching and student learning (Pitama, 2012).
First Nations-led development ensured that First Nations educators lead curriculum decision-making, through identified leadership positions (e.g., Elders (Carter & Rukholm, 2009), First Nations identified project officers (Andrews, 2012; Bennett, Redfern, & Zubrzycki, 2018; Bennett, Coghlan et al., 2018; Bernhardt et al., 2011; Duffy et al., 2013; Woolley et al., 2013), and First Nations identified academics (R. G. Jones, 2011, 2012; McDermott & Sjoberg, 2012; Ryder & Edmondson, 2015; Thompson, 2001; West et al., 2019)).
Many studies were led by First Nations education centres or units or health organizations (including, the Centre for Aboriginal Medical and Dental Health at University of Western Australia (Allen et al., 2017; Paul et al., 2006, 2013, 2015), the Poche Centres for Indigenous Health (McDermott & Sjoberg, 2012; Ryder & Edmondson, 2015), the Māori/Indigenous Health Institute at University of Otago (Huria, 2012; Huria et al., 2013; Huria, Lacey, Melbourne-Wilcox, & Pitama, 2017; Huria, Palmer et al., 2017; Pitama, 2012) (for a full list see the Table of Included Articles in Supplementary Information).
First Nations-led development enabled Indigenous pedagogical knowledges to be accessed and safely included, for example the Hui Process and Meihana Model (cited in Huria, 2012; Huria, Lacey, Melbourne-Wilcox, & Pitama, 2017; Huria, Palmer et al., 2017), Eight Ways of Learning pedagogy (cited in Bennett, Coghlan et al., 2018; West et al., 2019), and the Medicine Wheel (cited in Carter & Rukholm, 2009). First Nations-led development was recommended to improve inclusion of First Nations health curriculum in programs, preventing symbolic or incoherent inclusion. Authors argued that leadership roles need to be continually reinforced in the context of colonized and hierarchical systems which can undermine First Nations expertise and authority (Paul et al., 2013).
Literature Review
A literature review process was undertaken in 21 included articles to gather relevant evidence to inform curriculum and for developing reading lists. Most studies utilized literature reviews to complement other curriculum development methods. A literature review was used to identify literature by First Nations authors, find best practice examples in First Nations contexts, and to improve educators’ knowledge of critical topics including cultural safety (Bennett, Coghlan et al., 2018; Forsyth et al., 2018, 2019a, 2019b; Gair et al., 2003; Morgan et al., 2009; Shah & Reeves, 2015; Wilson et al., 2015). A literature review enabled educators to collate evidence and develop staff and student resources, for example by creating an annotated bibliography (Gair et al., 2003). A secondary benefit of conducting a literature review as part of curriculum development was improved non-Indigenous educator knowledge and capacity (Gair, 2007, 2016). Literature reviews were also conducted to understand ways of working and effective collaborative processes (Keogh et al., 2010).
Co-Leadership
Co-leadership was described as curriculum development led by First Nations and non-Indigenous educators utilizing collaboration and shared decision-making (n = 20). This process was interrelated with relationship building and was usually driven by First Nations leadership and ways of working (Forsyth et al., 2018, 2019a, 2019b; Francis-Cracknell et al., 2017; Jackson Pulver, 2012; McDermott & Sjoberg, 2012; Power et al., 2018; S. Thompson, 2001; Virdun et al., 2013). Co-leadership was observed in shared leadership of projects, working groups, subject coordination and teaching teams, and co/team-teaching models (Castell et al., 2018; Francis-Cracknell et al., 2017; Gair, 2016; Goerke & Kickett, 2013; Kickett et al., 2014; MacLeod, 2012; McDermott & Sjoberg, 2012; Power et al., 2018; Ryder et al., 2013; S. Thompson, 2001; Virdun et al., 2013). Co-leadership was supported by First Nations representation on school management committees (Hays, 2002; Thompson, 2001; Wain et al., 2016), First Nations involvement in staff and student recruitment processes and training and education (Hays, 2002), and Non-Indigenous staff training and education (capacity building) (Power et al., 2018; Thompson, 2001).
Co-leadership is described in several articles relating to the Curtin University (Australia) first-year interprofessional Indigenous Cultures and Health Unit (Bullen & Roberts, 2019a; Flavell et al., 2013; Goerke & Kickett, 2013; Hendrick et al., 2014; Kickett et al., 2014; Sonn et al., 2000). In these Curtin University studies, co-leadership is described as First Nations and non-Indigenous collaboration for curriculum development that involves a reciprocal intercultural partnership (Kickett et al., 2014). A rationale for co-leadership (of a working party) was stated as “[co-leadership] recognizes the importance of Indigenous leadership, knowledge and sensitivity to guide the process and to share knowledge,” which requires everyone to be aware of and respectful of each other’s cultures and not value one more than another (Power et al., 2018, p. 843). Co-leadership for governance and management of curriculum development projects was attributed to high quality curriculum outcomes (Wain et al., 2016). Co-teaching as a type of co-leadership was reported to increase student sharing of different perspectives during cultural safety workshops (McDermott & Sjoberg, 2012).
Consultation With Non-Indigenous Academics
In 14 articles, curriculum development involved consultation with academics via survey, interview, and/or focus group. Studies in this category selected academics for consultation based on their academic role (Bennett, Redfern, & Zubrzycki, 2018; Bernhardt et al., 2011; Forsyth et al., 2018, 2019a; Francis-Cracknell et al., 2017; Haight et al., 2019; R. G. Jones, 2011; Lower, 2001; McConnochie & Ranzijn, 2012; Mortley, 2011; Wilson et al., 2015; Zimmerman et al., 2019). In three articles, non-Indigenous academic staff were specifically consulted for their views on teaching First Nations health (Sonn et al., 2000; Wilson et al., 2015; Zimmerman et al., 2019), some educators “did not feel equipped” (Wilson et al., 2015, p. 117) or “feel the irony in teaching about oppression from a position of white privilege” (Sonn et al., 2000, p. 148). Zimmerman et al.’s (2019) consultations identified that non-Indigenous nursing academics perceptions of their teaching capacity were influenced by previous academic and/or clinical experiences. Survey methods were also used for academic consultations to obtain perspectives on curriculum development and collect feedback (Bernhardt et al., 2011; Francis-Cracknell et al., 2017; Lewis & Prunuske, 2017).
Working Group
Curriculum development involved establishing a working group with representation from key stakeholders in 12 articles. This included multidisciplinary working groups with representatives across disciplines (Bennett, Coghlan et al., 2018; Francis-Cracknell et al., 2017; Muir-Cochrane et al., 2018; Power et al., 2018; Virdun et al., 2013). Some working groups were discipline-specific, for example speech therapy (Bernhardt et al., 2011), medicine (Jarvis-Selinger et al., 2008; Smith et al., 2015), nursing (Nash et al., 2006), and psychology (McConnochie & Ranzijn, 2012). Working groups could also include First Nations industry experts and professionals (Smith et al., 2015). One article described a student-led working group that organized a placement in a remote Indigenous community (Warren et al., 2016).
Curriculum Mapping
A mapping or audit process was used to identify First Nations health curriculum content in existing programs (n = 11). Only one study described prospective mapping to plan curriculum development (Smith et al., 2015). Mapping processes were used to gather detailed information on how First Nations perspectives were included (Goerke & Kickett, 2013; Nash et al., 2006; Power et al., 2018; Virdun et al., 2013; Wilson et al., 2015), to identify overlap, gaps, issues, and/or inconsistencies (Bennett, Coghlan et al., 2018; Goerke & Kickett, 2013; R. G. Jones, 2011; Zimmerman et al., 2019), and to obtain a baseline for further development (Lewis & Prunuske, 2017; Lower, 2001). To conduct mapping, First Nations health curriculum content was defined by Lower (2001) as “any information which related specifically to issues/work with Aboriginal groups, utilized Aboriginal cases studies and/or readings” (p. 33). Zimmerman et al. (2019) utilized the Aboriginal and Torres Strait Islander Health Curriculum Framework (Department of Health, 2014) for mapping Bachelor of Nursing curriculum identifying gaps in history, humility, white privilege and racism. Mapping processes were recommended to increase educator’s engagement in curriculum development and to promote reflection and discussion (Nash et al., 2006). Findings from curriculum mapping of one program could also be shared to inform curriculum development in other health programs (Paul et al., 2013).
Non-Indigenous Staff Training and Education (Capacity Building)
In 10 included articles, training, resources, and support (including cultural mentoring) was provided to build capacity of non-Indigenous educators engaged in curriculum development and delivery (Bennett, Redfern, & Zubrzycki, 2018; Bennett, Coghlan et al., 2018; Goerke & Kickett, 2013; Harris et al., 2012; Jackson Pulver, 2012; Kairuz & Shaw, 2005; Nash et al., 2006; Power et al., 2018; Thompson, 2001; Virdun et al., 2013). In Bennett, Redfern, and Zubrzycki (2018), an Aboriginal team member was also the cultural mentor to non-Indigenous project team members, which was reported to provide critical guidance on cultural protocols. Formal training was provided to non-Indigenous educators to ensure teaching quality (Jackson Pulver, 2012; Kairuz & Shaw, 2005). Goerke and Kickett (2013) argued that a “culturally safe space for educators to meet and talk” is crucial so they can “learn from each other and challenge racism” (p. 73). Non-Indigenous educators are recommended to “demonstrate openness toward Indigenous peoples and knowledge and have an awareness of the existence of Indigenous knowledge systems and ways of working in their local context” (Goerke & Kickett, 2013, p. 73). Staff professional development needs were assessed using the Indigenous Perspectives Tertiary Educator’s Awareness, Knowledge, and Skills Scale (Nash et al., 2006).
Action Research
An action research or action learning process was used in seven articles, supporting First Nations and non-Indigenous educators to work collaboratively for curriculum development and enabling co-leadership (Duffy et al., 2013; Gair et al., 2003; Hendrick et al., 2014; Ross et al., 2013; Sonn et al., 2000; Wilson et al., 2015; Woolley et al., 2013). An action research process was used to support a longer term iterative process of curriculum development involving multiple phases of consultation, information gathering and literature review, reflexive discussion, content development, and evaluation (Duffy et al., 2013; Gair et al., 2003; Hendrick et al., 2014; Ross et al., 2013; Sonn et al., 2000; Wilson et al., 2015; Woolley et al., 2013). Authors utilized this method recognizing that decolonizing programs and institutions required an enduring commitment to personal and professional development and systemic change (Gair et al., 2003; Hendrick et al., 2014). An action research process for curriculum development was also argued to promote sustainability (Ross et al., 2013) and create processes that were transferrable to other programs (Wilson et al., 2015).
In a study at James Cook University (Australia) (Duffy et al., 2013; Ross et al., 2013; Woolley et al., 2013), a participatory action research method was guided by established principles for ethical research with Aboriginal and Torres Strait Islander peoples (National Health and Medical Research Council, 2018). This ensured processes reflected integrity, reciprocity, respect, equality, survival, and shared responsibility (Duffy et al., 2013, p. 5). First Nations health professionals, Elders and community leaders (n = 13) were employed as co-researchers (Duffy et al., 2013; Ross et al., 2013; Woolley et al., 2013). Yarning Circle discussions guided by an agreed terms of reference supported respectful and equal sharing of views (Duffy et al., 2013; Ross et al., 2013; Woolley et al., 2013).
First Nations Reference or Advisory Group
A First Nations reference group or advisory group was established to provide governance and oversight of curriculum development and expert advice (n = 6) (Duffy et al., 2013; Gair, 2016; Jacklin et al., 2011; Ross et al., 2013; Wain et al., 2016; Woolley et al., 2013). In the James Cook University (Australia) study the action research group was also the Indigenous Reference Group (Duffy et al., 2013; Ross et al., 2013; Woolley et al., 2013). An Aboriginal and Torres Strait Islander Advisory Group made decisions about a subject (unit) including topics, readings and assessment for social work students, ensuring majority of readings were First Nations authored (Gair, 2016). An Aboriginal reference group was established to advise the Dean for an undergraduate medical program at Northern Ontario School of Medicine (Jacklin et al., 2011). Authors argued that an Indigenous reference group supported the facilitation of a culturally respectful curriculum development process that enhanced First Nations participation (Wain et al., 2016).
Out-Sourcing to First Nations Organisations
A final curriculum development method was to out-source and purchase curriculum from First Nations organizations (n = 5). Out-sourcing was utilized to develop a 3-hr cultural safety workshop for occupational therapy students by Anishnawbe Health Toronto (Jamieson et al., 2017), and for cultural immersion placements or programs (J. Benson et al., 2015; Jamrozik, 1995; Pickrell, 2001; Tobin et al., 2015).
Discussion
The findings address the review question, describing the scope of methods and processes of First Nations health curriculum development in entry-level nursing, medicine, dentistry and allied health programs in international peer-reviewed journal articles. The curriculum development methods and processes described provide critical guidance to inform this work currently underway in universities in many colonized countries.
A total of 104 articles were identified with majority published in peer-reviewed First Nations-led publications. This finding demonstrates the importance of incorporating additional searches of First Nations-led journals when conducting literature reviews, because of the ongoing and institutionalized influences of colonization in mainstream journal publications which can act as gatekeepers to knowledge production (McMahon, 2017). Researchers refer to this additional search process as “relational mapping” (Gower and Belcher, personal communication 18 June, 2018 with author), which can be used to find literature not currently identifiable through database searches, and to reveal a community of practice in the literature for a particular topic.
Processes of curriculum development identified in this review that align with best practice and pedagogy in First Nations education more broadly (beyond health) are the First Nations-led and co-leadership approaches. First Nations-led development enables curriculum development to be conducted through a decolonizing process that disrupts extant Eurocentric curriculum and ways of working, and privileges First Nations perspectives (Al-Natour & Mears, 2016; Fellner, 2018). Co-leadership processes occur at the Cultural Interface and create a Third Space for developing epistemologically equal curriculum that is culturally strong in both First Nations and Western knowledges and worldviews (Dudgeon & Fielder, 2006; Nakata, 2007). Relationship building was an interrelated process that is integral and inseparable from these approaches, which aligns with First Nations pedagogy that argues learning needs to occur on a foundation of connection, belonging, and trust (Drummond, 2020).
First Nations leadership is required as a foundation for decolonizing curriculum. Utilizing the curriculum development methods identified in this review without First Nations leadership or governance could result in tokenism or “extractive colonization” where First Nations perspectives are included in curriculum in ways that perpetuate colonial discourses (Drummond, 2020, p. 2), for example by presenting deficit discourses. Embedding First Nations health curriculum in health programs must include an identifiable “Indigenous voice” as First Nations peoples “insert their own narratives, critiques, research, and knowledge production” into curricula (Nakata, 2007, p. 8). First Nations-led development exemplifies how First Nations epistemologies, perspectives, and processes can be prioritized through curriculum development processes. First Nations-led development is inclusive of First Nations academic employment and co-leadership practices, which increases capacity of First Nations and non-Indigenous staff within universities. This process should be adopted by educators to recognize the expertise of First Nations academics in higher education, while identifying a place for non-Indigenous academics but only when they engage respectfully with “Indigenous communities, research, knowledges, programs and histories” (Thunig & Jones, 2021, p. 5). The alternative process of out-sourcing to First Nations organizations can also be utilized to maintain First Nations leadership, however there is a risk that developed curriculum could be included as an adjunct rather than embedded, core program content.
It must be recognized that within universities, curriculum development takes place in contested and colonized spaces which are not easily accessed by First Nations educators (Fredericks, 2011; Nakata, 2007; Thunig & Jones, 2021). When implementing the curriculum development methods and processes identified in this review, educators need to be cognizant of and proactively dismantle the barriers experienced by First Nations educators in higher education institutions, of white supremacy and resulting institutional and interpersonal racism (Fredericks, 2011; Thunig & Jones, 2021). Kickett et al. (2014) argued that “Teaching in this space comes with considerable emotional labor, which is significant for Aboriginal tutors whose personal and familial identity is at risk from racism in these encounters” (p. 39). These barriers must be addressed as a priority, prior to and alongside First Nations health curriculum development to create contexts that privilege First Nations expertise.
Additionally, further research is needed on how to include First Nations student perspectives as key stakeholders in curriculum development. While student consultation was the most frequent method of curriculum development in included articles, First Nations student perspectives were only specifically sought out and incorporated in three articles, presenting an urgent gap to be addressed that could also contribute valuable insights on how to develop health curricula that is anti-racist and culturally safe (Fernando & Bennett, 2019; Kurtz et al., 2018).
There is a wide scope of methods, processes, and resources for First Nations health curriculum development including survey tools from which educators can draw from. The creators of the Cultural Capability Measurement Tool (West et al., 2019) identified in the current scoping review, for example, have conducted multiple studies to develop, test, and validate this tool for use with undergraduate health student cohorts (West et al., 2017, 2018). Future research on First Nations health curriculum development could include critical appraisal of available survey tools.
In this review, studies were predominantly from medicine and nursing disciplines, with more recent increases in dentistry, social work, and psychology. The high volume of published literature in medicine and nursing is likely because of First Nations leadership and established accreditation requirements, both in Australia through the Australian Indigenous Doctors Association and the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives, and internationally, for example through the Truth and Reconciliation Commission of Canada, the Treaty of Waitangi (1840, Aotearoa), and publication of curriculum frameworks (e.g., Department of Health, 2014; Indigenous Physician Association of Canada, 2008; Phillips, 2004; Zubrzycki et al., 2014). The findings of this scoping review provide critical guidance for educators, particularly those from disciplines where there is limited published works, where accreditation requirements might be more recent, or who are new to First Nations health curriculum development.
Limitations
The scoping review search strategy was effective for addressing the search question and provided multidisciplinary findings, however led to a large number of included articles. This is common for scoping reviews (in comparison to other review types) which determine the scope of the literature and typically can include over 100 studies (Tricco et al., 2016). However, because of the large number of included peer reviewed journal articles, a grey literature search was not completed which could have provided additional insights for this scoping review and could be completed in future research.
The analysis of included articles involved multiple researchers and phases to ensure rigorous synthesis of results and all articles were reviewed by at least two authors including a First Nations author, however human error could cause errors in categorization. Articles were categorized using quantitative content analysis based on explicit methods and processes, therefore implicit details that were not clearly stated could not inform categorization. Therefore some articles, for example, which might have utilized First Nations-led development but did not describe this in-text, might not have been included in this category. Future reviews could use author consultation as an additional review stage to clarify study details with authors (Arksey & O’Malley, 2005).
Conclusion
Embedding First Nations health curriculum in entry-level health programs positions First Nations perspectives within higher education for the benefit of both First Nations and non-Indigenous students. Existing best practice curriculum frameworks direct educators to what content needs to be included in entry-level health programs, however, educators need an understanding of methods and processes to effectively embed curricula. This scoping review has identified and described curriculum development methods and created a suggested First Nations health curriculum development model that can be utilized by educators including First Nations-led development and co-leadership which align with best practice and pedagogy.
Improved curriculum development processes will contribute to the development of curriculum and programs that are culturally strong from both First Nations and Western perspectives and worldviews. Barriers must be overcome to ensure First Nations expertise is privileged during curriculum development. The findings of the review are crucial in addressing calls for decolonizing programs in higher education while simultaneously advancing efforts to build graduate cultural capability outcomes that are required for clinically and culturally safe healthcare for First Nations and non-Indigenous peoples.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440231163834 – Supplemental material for Methods and Processes for First Nations Health Curriculum Development for Nursing, Medicine, Dentistry and Allied Health Entry-Level Programs: A Scoping Review
Supplemental material, sj-docx-1-sgo-10.1177_21582440231163834 for Methods and Processes for First Nations Health Curriculum Development for Nursing, Medicine, Dentistry and Allied Health Entry-Level Programs: A Scoping Review by Shirley Godwin, Nerida Hyett, Mishel McMahon, Carol McKinstry, Natasha Long, Mary Whiteside and Chris Bruce in SAGE Open
Supplemental Material
sj-docx-2-sgo-10.1177_21582440231163834 – Supplemental material for Methods and Processes for First Nations Health Curriculum Development for Nursing, Medicine, Dentistry and Allied Health Entry-Level Programs: A Scoping Review
Supplemental material, sj-docx-2-sgo-10.1177_21582440231163834 for Methods and Processes for First Nations Health Curriculum Development for Nursing, Medicine, Dentistry and Allied Health Entry-Level Programs: A Scoping Review by Shirley Godwin, Nerida Hyett, Mishel McMahon, Carol McKinstry, Natasha Long, Mary Whiteside and Chris Bruce in SAGE Open
Footnotes
Acknowledgements
The authors would like to acknowledge the technical support provided by Michelle Collins and library support from Natalie Crothers.
Authors’ Note
This manuscript is an original work that has not been submitted to nor published anywhere else.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a La Trobe University Scholarship of Teaching and Learning grant.
Ethics Statement
Ethics approval not applicable
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.