
Abstract
The family of emergency surgery patients experience psychological pressure due to the uncertainty of the surgery. The purpose of the study was to examine the effects of information delivery intervention provided by an operation theater nurse on anxiety and satisfaction levels of the family of emergency surgery patients. A quasi-experimental pretest–posttest control group design is used. A total of 60 participants were included in the study as the family of patients undergoing emergency surgery within 6 hr in the emergency room of K hospital in Seoul, Korea (intervention: n = 30, control: n = 30). The information delivery intervention consisted of information on the operating room environment and surgery progress. The tools included the Anxiety scale to examine the anxiety levels and Perioperative Family Needs Questionnaire (PFNQ) to measure family satisfaction levels. Participants in the intervention group had a lower anxiety level (p < .001) and higher family satisfaction with the intervention (p < .001) than that of the control group. The information delivery intervention provided by an operation theater nurse was effective. It decreased the anxiety level and increased the satisfaction for the family member of emergency surgery patients. These findings can be used as clinical evidence to explore nursing interventions or strategies for the patient’s family during an emergency surgery.
Introduction
If a patient has been placed in a life-threatening status due to an accident or illness, family members may suffer financial and social crises (Hamester et al., 2016). In addition, feelings of tension and anxiety tend to increase (Hamester et al., 2016; Lee & Lee, 2012). If a family member is hospitalized, the family goes through various challenges, such as adapting to an unfamiliar hospital environment. If a family member undergoes surgery, the other members experience stress, anxiety, and alienation due to the inability to cope with such process (Kushnir et al., 2015; Oberoi et al., 2016; Y. A. Yun, 2012). Furthermore, the sudden recommendation for surgery is given while they are still mentally devastated due to extreme pain, anxiety, and discomfort (Balogh-Mitchell, 2012; Lim et al., 2015).
Literature Review
In South Korea, the number of surgeries done on emergency room patients increases every year. There were 11,273 cases in 2009, 44,735 cases in 2010, 46,371 cases in 2011, and 48,996 cases in 2012 (National Emergency Medical Center, 2012). As a result, the patients and their families are filled with anxiety. In the user’s satisfaction survey for emergency room service improvement, satisfaction with “waiting time until emergency surgery” was 25.1% (National Emergency Medical Center, 2012). This indicates that the anxiety and discomfort of patients scheduled for surgery and their families become higher as the waiting time increases (Lim & Chung, 2007; Oberoi et al., 2016).
Anxiety is a negative emotional response caused by stress or threatening situations (Lim et al., 2015; Oberoi et al., 2016). It is one of the most important phenomena closely associated with health. Moreover, it is commonly experienced by people who require nursing intervention (Hamester et al., 2016; Lim et al., 2015; Oberoi et al., 2016). There are instances when the family members feel more anxious and restless in imagining the worst-case scenario (Fortier et al., 2009; Y. A. Yun, 2012). This increase in anxiety may result in a broken trust between the family and health professionals. For this reason, sufficient information on the progress status of surgery and psychological support are desperately needed (Kloos & Daly, 2008; Yang, 2010). The role of the family is crucial in the patient’s recovery and safety after surgery (Lee & Lee, 2012; Oberoi et al., 2016; Peles Bortz et al., 2016). Measures must be sought to reduce the family members’ anxiety while at the surgery waiting room (Curran & Datto, 2014; Lai et al., 2016; Yang, 2010). To reduce the anxiety of patients and their family members, information on surgery should be provided to the patient’s family (Oberoi et al., 2016; Y. A. Yun, 2012). Methods of providing information regarding surgery include visual information provision programs (booklets or video slides) and indirect information regarding the progress of the patient (status board installed in the waiting room and text messaging via SMS) (Lai et al., 2016; J. H. Yun & Kim, 2010). The patient status board communicates only the patient’s location, not how the patient is doing. In addition, there is a direct method of information provision for nurses to directly inform the family about the surgery status (Hong & Lee, 2004; Lai et al., 2016; Yang, 2010). Leske (1996) and Yang (2010) suggested that directly explaining the status of the surgical progress is most effective in reducing anxiety and increasing the satisfaction with nursing of the patient’s family members. In the study by Lee (2003) on anxiety regarding surgery and satisfaction with nursing of the families of surgery patients, the family members wanted to directly meet the surgeon and listen to the explanation of the surgical result. Furthermore, they expected to have sufficient time to ask the surgeon some questions and receive satisfactory answers. Good communication between the patient’s family and health professionals by directly explaining the status of the surgical progress can reduce the family’s anxiety and increase their satisfaction with nursing (Balogh-Mitchell, 2012; Lai et al., 2016; Oberoi et al., 2016; Yang, 2010; Y. A. Yun, 2012).
Some studies have shown that anxiety is reduced by providing information to the patient’s family in various ways. However, most South Korean hospitals are using the patient status board for providing information to the surgical patients’ families, thereby reducing their anxiety (Hong & Lee, 2004; Y. A. Yun, 2012). It briefly shows the patient’s status before surgery, during surgery, and under recovery. Recently, studies have been conducted on nursing interventions for psychological stability in relation to the anxiety experienced by the patient’s family. However, these have been limited to adult regular surgery and pediatric regular surgery. No studies have been performed on the family members of emergency surgery patients. Therefore, this study was conducted to identify an efficient nursing intervention method for patients who underwent emergency surgery and their families. The aim of this study was to examine the effects of information delivery intervention provided by an operation theater nurse on anxiety and satisfaction levels of the family of emergency surgery patients.
Hypotheses
Based on the above, the following hypotheses were generated:
Method
Design
A quasi-experimental pretest–posttest control group design was used.
Participants
A total of 60 participants were included in the study as the family of patients undergoing emergency surgery within 6 hr in the emergency room of K hospital in Seoul, South Korea (intervention group: 30 samples, control group: 30 samples). The participants were recruited through convenience sampling. Group assignment to the intervention group and control group was done via coin toss. For the coin toss, heads indicate being assigned to the intervention group, and tails indicate being assigned to the control group. Eligibility criteria included subjects aged ≥19 years who consented to participate in this study with clear consciousness and full capability to verbally understand in Korean (Figure 1).

Flow diagram.
Sample size adequacy (n = 26 in each group) using G power was estimated based on an alpha level of .05, effect size of .8, and power of .8 (Faul et al., 2007). Therefore, the sample size of this study was appropriate.
Intervention
Information delivery intervention provided by the operation theater nurse as an experimental intervention included the information on the operating room environment and surgery progress. The information on the operating room environment was developed by an investigator with 13 years of operating room experience. The information on the surgery progress was organized based on previous studies (Lai et al., 2016; Lim & Chung, 2007; Yang, 2010) and the investigator’s practical experience. Its validity was reviewed by the operation theater charge nurse, three operation theater nurses with more than 10 years of experience, and one nursing professor. For the operating room environment, pictures were taken for all surrounding environments of the operating room. These include the interior of the operating room and recovery room, from the time the patient entered the operating room from the surgery waiting room until the patient’s arrival to the recovery room. In addition, 16 PowerPoint slides were made according to the order of the patient’s experience. The information was provided directly by the investigator through a computer at the surgery patient’s waiting room located at the entrance of the operating room. For the surgery progress, information provision included the start of anesthesia, start of surgery, sample’s availability (if a sample was collected), end of surgery, and transfer to the recovery room. The information was directly provided by the investigator for the reliability of the study.
Data Collection and Ethical Considerations
Data were collected from January 2016 to March 2016. The investigator met the patient’s family after contacting the investigator’s colleagues, who were on duty and going to the hospital. The investigator explained the study purpose to the patient’s family by using the subject information sheet. In addition, the investigator obtained the informed consent form from the subjects. For the intervention group, information on the operating room environment and surgery progress as an experimental intervention was provided by an operation theater nurse. For the control group, simple information on surgery standby, surgery progress status, and location after surgery was supplied via the patient status board. This was provided to the patient’s family in the caregiver’s waiting room located outside the operating room. These communicate only the patient’s location, not how the patient is doing. After 10 min of transferring the patient to the recovery room, the patient’s family filled out a questionnaire at the waiting room. These were collected by the researcher. For the prevention of diffusion of treatment, study process for the control group was first done. After 3 weeks, the procedure for the intervention group was started.
For ethical considerations, the researcher obtained written permission from the hospital. After this procedure, the researcher contacted the study participants to obtain their consent. The researcher explained the purpose, sample criteria, experimental intervention of the study, participation details, and instruments of this study. The study participants were informed that they could voluntarily join the study and withdraw their participation from the study at any time. They were also informed of the anonymity of the data. The researcher obtained written consents from the study participants.
Measures
The study questionnaire was designed to measure the general characteristics of the study participants, anxiety, and family satisfaction. Validity of all questionnaires was confirmed by two nursing professors and three experts.
General characteristics of study participants
It consisted of gender, age, marital status, education, religion, relation with the surgical patient, waiting experience during surgery, type of surgery, and stress level. This consisted of a total of nine items.
Anxiety
The State-Trait Anxiety Inventory (STAI) developed by Spielberger (1972) was standardized for Koreans by Kim and Shin (1978). State anxiety scale was used to measure the anxiety level of the study participants. Trait anxiety scale was excluded because it is used to examine how people feel across typical situations on a daily basis. It consisted of 20 items with 4-point Likert-type scale. The possible score range was 20 to 80, and the higher the score, the higher the level of anxiety. Reliability of this scale was Cronbach’s α of .87.
Family satisfaction
Perioperative Family Needs Questionnaire (PFNQ) developed by Carmody et al. (1991) was revised by Park (2002). This scale was used to measure the level of family satisfaction with intervention. It consisted of 20 items with 4-point Likert-type scale. The possible score range was 20 to 80, and the higher the score, the higher the level of family satisfaction with intervention. Reliability of this scale was Cronbach’s α of .88.
Analysis of Data
The collected data were analyzed using the SPSS version 21.0 statistical software program. General characteristics of the study participants were analyzed using descriptive statistics with frequency, percentage, mean, and standard deviation. The homogeneity test of study variables (anxiety and family satisfaction with nursing) at the preintervention between two groups was analyzed using the independent t test. Effects of information delivery intervention provided by the operation theater nurse were analyzed using the independent t test. A p value of less than .05 was considered statistically significant.
Results
General Characteristics of Study Participants and Homogeneity
In terms of gender, 60.0% were female and 40.0% were male in the intervention group. In the control group, 66.7% were female and 33.3% were male. In terms of age, the mean scores were 33.42 ± 3.34. The mean scores of the intervention group and control group were 34.08 ± 3.22 and 32.75 ± 3.46, respectively. In terms of education level, 56.7% had high school education in the intervention group. In the control group, 50.0% were high school graduates, thus representing the highest proportion. For the relation with the surgery patient, 40.0% of the participants in the intervention group had parents and 40.0% of the participants in the control group had children. In terms of the waiting experience during surgery, most participants had no experience about that (intervention: 83.3%, control: 76.7%). In terms of type of surgery, 46.7% of the participants in the intervention group and 43.3% in the control group indicated appendix surgery. In terms of stress level, most participants had some severe stress levels or over (intervention: 90.0%, control: 90.0%). Between the two groups, there were no significant differences in the general characteristics of the study participants. In the homogeneity test of study variables (anxiety and family satisfaction with nursing) at the preintervention between the two groups, there were no significant differences (Tables 1 and 2).
General Characteristics of Study Participants (N = 60).
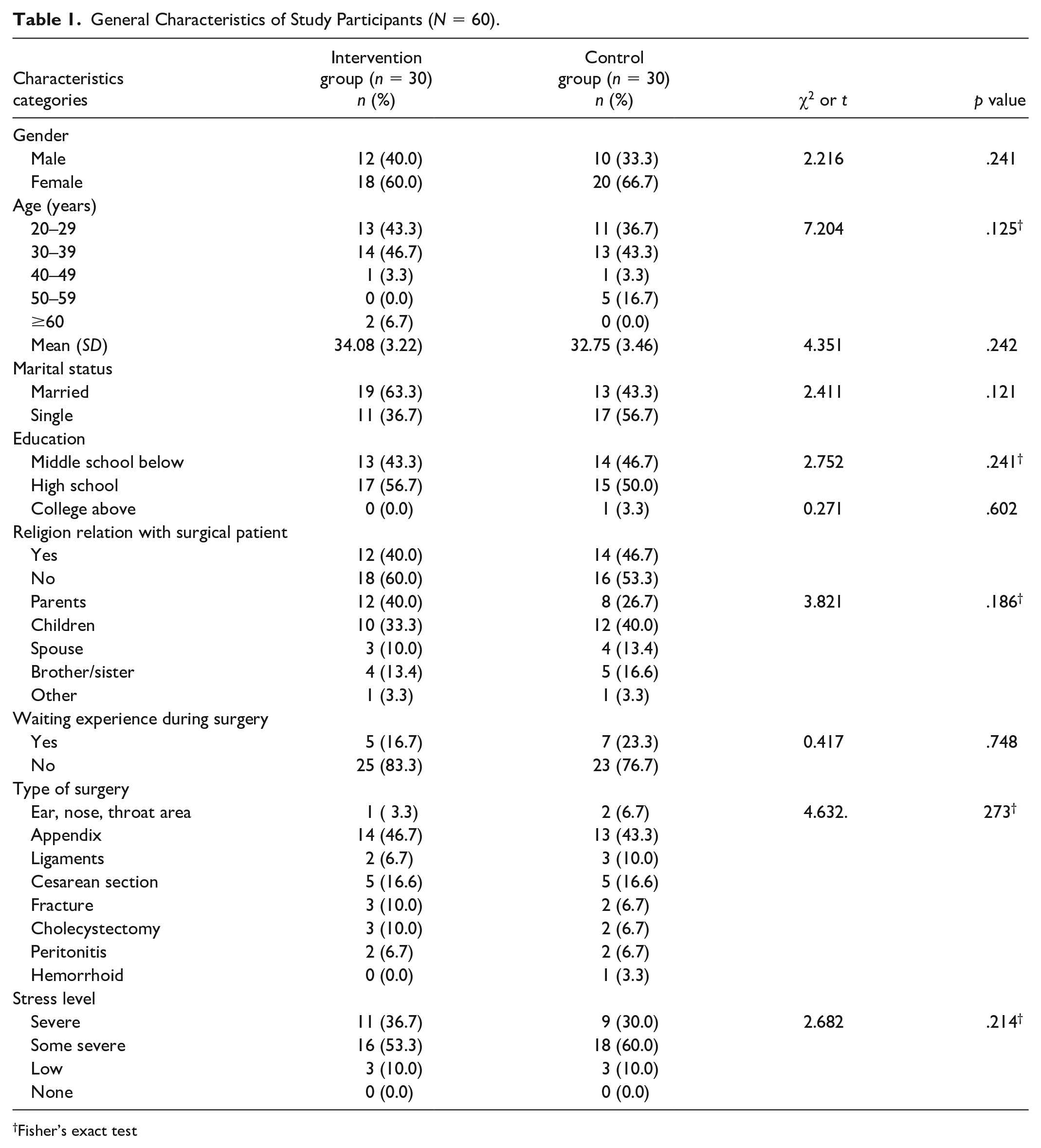
Fisher’s exact test
Homogeneity Test of Study Variables at the Preintervention between Two Groups (N = 60).

Effects of Information Delivery Intervention Provided by an Operation Nurse
The analysis showed that the intervention group had a lower anxiety level (p < .001) and higher family satisfaction with the intervention (p < .001) than the control group (Table 3).
Effects of Information Delivery Intervention Provided by an Operating Nurse (N = 60).

p < .05.
Discussion
In the control group, the anxiety score decreased by 2.36 points after the intervention from 59.23 points to 56.87 points. Meanwhile, in the intervention group, the anxiety score decreased by as much as 25.87 points after the intervention from 62.37 points to 36.50 points. The results showed that provision of direct information rather than simple information via the patient status board was effective in reducing the anxiety of the patient’s family. This result was similar to those of Eldridge (1984) and Lai et al. (2016), in which the patient’s family had more trust in the medical staff after the provision of information, which remarkably reduced stress and anxiety. The study by Y. A. Yun (2012) targeted a total of 63 family members of regular surgical patients who underwent tonsillectomy. The simple information was provided via the patient status board for the control group, whereas information was provided via text message service and patient status board for the intervention group. Yun’s study result was consistent with this study in that the provision of additional information and simple information was effective in reducing the anxiety of the patient’s family. In the study by Lim and Chung (2007), an operating room nurse directly provided information to the family members of 40 patients while at the waiting room during surgery for stomach and breast cancer. As a result, their anxiety was significantly lower, which was consistent with the result of this study.
In this study, the family satisfaction in the intervention group and control group was 44.03 points and 30.40 points, respectively. The family satisfaction appeared to be higher in the intervention group than in the control group. This indicates that provision of direct information was effective in satisfying the patient’s family. To effectively provide information, the person must be familiar with the operating room and surrounding environments. In addition, they must have surgical experience, good communication skills, and risk intervention ability (Lai et al., 2016; Lee & Lee, 2012). The investigator of this study directly provided surgery information to the patient’s family members and somewhat fulfilled their psychological and emotional needs while working at the operating room. As a result, the subjects felt embarrassed or anxious at first in being operated on emergency, but after the information was provided, they became stable. In terms of family satisfaction with intervention, the difference before and after the information provision was 12.63 points, thus indicating that it was effective. This result was consistent with that of the study in which the family satisfaction increased after a booklet for digestive cancer was provided to the families of open surgery patients (Park, 2002). This was also consistent with the study result in which information was provided using a text message service to regular surgery patients. Significant effects were shown in the family satisfaction through the provision of information for the surgical patient’s family (Huang et al., 2006; Kushnir et al., 2015; J. H. Yun & Kim, 2010). In this study, however, family satisfaction with intervention increased from 29.87 points to 30.40 points in the control group, using simple information via the patient status board. However, there was no significant effect on satisfaction. Although the use of a patient status board somehow satisfied the needs of the patient’s family, the provision of more specific information on surgical progress may contribute to increasing their satisfaction.
Limitations
The major limitation of this study was the samples’ degree of representation and generalizability. The samples used in this study were recruited only from a hospital in the metropolitan city of South Korea, which limited the characteristics of the resulting data. However, the main purpose of this study was not to produce generalizable results, but to provide information for future research.
Implications
Intervention for the patient’s family during surgery is an important element to fulfill the needs and reduce the anxiety of the patient’s family, who wanted to be constantly informed and assured of the patient’s status during surgery (Oberoi et al., 2016; J. H. Yun & Kim, 2010). Therefore, proper nursing intervention to directly check the factors of anxiety and fulfill the needs of the families of surgery patients must be provided. This can be done through customized nursing and holistic nursing. Concrete nursing interventions and strategies are required for providing exact and more information to the patient’s family during an emergency surgery. Findings from this study may be implied as evidence to explore strategies for reducing anxiety and increasing the satisfaction of the patient’s family during an emergency surgery in South Korea.
Conclusion
In conclusion, providing information directly was an effective intervention for reducing anxiety and increasing the satisfaction of patient’s family. Findings of this study can reduce the anxiety and increase the satisfaction of the patient’s family during an emergency surgery. Repetitive studies on the specific timing of information provision, contents to effectively reduce the anxiety of the patient’s family, and multilateral efforts to explore various methods need to be conducted in the future.
Footnotes
Acknowledgements
The authors are very thankful to all the participants for their valuable contribution.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board in a University, Seoul, South Korea (KHSIRB-15-055(RA)).