
Abstract
Attention deficit hyperactivity disorder (ADHD) is one of the most common behavioral disorders in children. Children with ADHD have difficulties regarding the regulation of their emotions and activities and of the maintenance of attention and impulse control. Families with children with ADHD encounter many challenges, and the public health nurse is highlighted as helping and supporting these families. The aim of this study was to investigate families with a child having ADHD from the parents’ perspective. A cross-sectional study was performed. In total, N = 264 parents of children with ADHD, 217 mothers and 47 fathers (48.2%), responded on a questionnaire regarding psychological distress, family sense of coherence, and family functioning. Parents with ADHD and parents with children not medicated for ADHD seemed most vulnerable. Parents’ well-being and psychological distress seem to influence family functioning the most, with the behavior of the child with ADHD and support from the community health services had importance.
Attention deficit hyperactivity disorder (ADHD) is one of the most common behavioral disorders diagnosed in children, with a prevalence of approximately 5% of school-aged children worldwide (Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007). Children with this disorder have difficulties regarding the regulation of their emotions and activities, and of maintaining attention and impulse control (Barkley, 2006), but it is a clinically heterogeneous group and some children have more impairments in inattention, hyperactivity, and impulsivity than others. Interventions include both medication, a behavioral assessment of the child and parental supervision (Barkley, 2006). Twin studies estimate a heritability of 76%, which is influenced by both biological- and family-environmental factors (Faraone et al., 2005), and that children with ADHD are more likely to have a parent with ADHD than other children. Families with children with ADHD encounter many challenges in the family unite and in society at large. Support from the community health service has been described as important to families with a child with ADHD (Moen, Hall-Lord, & Hedelin, 2011, 2014). The parents may encounter both public health nurses and psychiatric nurses in the community in the child’s case or for their own needs.
Families With Children Having ADHD
Living in a family with a child having ADHD influences the whole family both inside the family sphere and socially (Moen, Hall-Lord, & Hedelin, 2014). Mothers have described their caregiver role to a child with ADHD as demanding and stressful (Peters & Jackson, 2009). Mother–teen conflicts and a greater degree of stress and conflicts within the family have also been reported with adolescents diagnosed with ADHD (Edwards, Barkley, Laneri, Fletcher, & Metevia, 2001). The psychological distress of having a child with ADHD has been found, with more symptoms of anxiety and depression in mothers, and mothers of a child with ADHD are twice as likely to have a psychiatric diagnosis than other mothers. The difference between fathers of a child with ADHD and other fathers is lower, but significant (Kvist, Nielsen, & Simonsen, 2013). Inconsistency in paternal discipline and the father’s low involvement have been associated with ADHD and may add more maternal stress, thereby highlighting the need for the involvement of fathers in the treatment of ADHD (Ellis & Nigg, 2009). Humphreys, Mehta, and Lee (2012) found an association between ADHD in children and depression in their parents. Family environment and inconsistent parent boundaries and limit settings are described as being associated with having a child with ADHD (Schroeder & Kelley, 2009). In the developmental stage of early childhood, positive parenting may act as a protective factor against conduct problems (Scaramella & Leve, 2004). Foley (2011) described a higher level of family dysfunction in families with children having ADHD. Family functioning is important in managing everyday life and can be described as a dimension that influences the family in relation to problem-solving, communication, roles, behavioral control as well as affective responsiveness and involvement (Miller, Ryan, Keitner, Bishop, & Epstein, 2000). Parents whose children have ADHD and are on medication have reported less problematic behavior in their child and better family functioning than parents with children having ADHD who are not medicated (Moen, Hedelin, & Hall-Lord, 2015). Family functioning has been found to be the strongest association for the referral of children to the specialist mental-health service (Reigstad, Jørgensen, Sund, & Wichstrøm, 2006). Further studies are needed to explore family functioning in families with children having ADHD.
Being the parent of a child with ADHD is a complex and difficult situation that requires an inner force to meet the daily challenges (Moen et al., 2011). Sense of coherence (SOC) may be described as an overall capacity to cope with stressful life situations, a health-protective life orientation (Antonovsky, 1996), which may reflect the inner force that parents describe. Parents reporting a strong family SOC may have a more positive appraisal of the circumstances, viewing the demands of parenthood as a challenge, and to be confident in the availability of resources to cope with demands (Ngai & Ngu, 2011), such as having a child with ADHD. SOC has also been associated with mental health and well-being (Sørensen et al., 2002). Well-being is defined as a subjective feeling, and a way that the individual experiences and evaluate himself or herself and his or her life (Sørensen & Næss, 1996).
Previous research has found that the situation for mothers with children with ADHD as demanding and stressful. Fathers have been less investigated; hence, studies with both mothers and fathers are needed. Even if children with ADHD are more likely to have a parent with ADHD, there has been a limited amount of research on this group of parents. Furthermore, there is a need for knowledge related to parents with children who are medicated for ADHD and not. Previous studies have found that characteristics in parents, the family, the child with ADHD and support from health services have exerted an influence on family life. How these various characteristics influence on family functioning needs further investigation.
Purposes of the Study
The aim of this study was to investigate families with a child with ADHD from the parents’ perspective by addressing the following research questions:
Method
Design and Sample
This study was a part of a cross-sectional study with members of an ADHD association. This association is a voluntary support organization with membership fees. The target population where 1,964 parents fulfilled the inclusion criterion of being the parent of a child with ADHD aged 15 years old and younger (Moen et al., 2015). The sample size was calculated to be sufficient by consulting a statistician, and assuming a drop-out rate of approximately 50% (Field, 2013). Moreover, the sample was randomly chosen (Figure 1).

Sample flowchart.
From the group of fathers, 35 mothers responded instead of the fathers, based on their own view. Due to no statistically significant differences being found between those mothers and the other participating mothers (n = 182) concerning the included variables, the 35 mothers were included. The response rate was 48.2% (mothers 82.2% and fathers 17.8%). One questionnaire from a father was excluded because of more than 50% internal drop-out rate, with the remaining 264 participants including 217 mothers and 47 fathers.
Ethical Considerations
An ethical committee for medical and health research approved the study. Ethical research principles in accordance with confidentiality, nonmaleficence, and justice were followed during the entire research process (Northern Nurses’ Federation, 2003).
Data Collection
The member lists of an ADHD association were blinded, and a randomized sample was drawn. An employee at the ADHD association had information about the members and sent the questionnaire with an information letter by postal mail to the sample.
The data collection took place from February 2013 to June 2013, and two reminders were sent 6 weeks apart. Information given in the member register showed that parents who responded to the questionnaire did not differ significantly from nonresponding parents in terms of gender, place of residence, and age of the child with ADHD.
Measures and Instruments
The questionnaire included questions regarding the characteristics of the parents and children with ADHD, as well as five instruments.
Parents characteristics included questions regarding age, gender, marital status (cohabitants/married or single/divorced/widow/widower), education (compulsory school, upper secondary school or college/university), parents’ self-reported ADHD diagnosis (yes, do not know, no), and place of residence (urban or rural).
Characteristics regarding the child with ADHD included age, gender, and child on medication (yes, no).
Support from the health services included two questions: “To what extent do you experience that your family has been supported by the community health service regarding the child with ADHD?” and “To what extent do you experience that your family has been supported by the specialist health service regarding the child with ADHD?” The response rate ranged from 1 = not at all to 7 = to a high degree, with only the anchors defined.
The Hopkins Symptom Checklist–10 (HSCL-10), a short form of the HSCL-58 (Derogatis, Lipman, Rickels, Uhlenhuth, & Covi, 1974; Tambs & Moum, 1993), was used to measure the degree of psychological distress in parents (primarily symptoms of anxiety and depression) within the last week. This instrument contains 10 items, for example, “Suddenly scared for no reason” and “Feeling of worthlessness.” The response options used a 4-point scale from “not at all” to “extremely.” A sum score was calculated by adding all the items, ranging from 10 to 40, and the lower score the better. The instrument has been validated in other studies (Tambs & Moum, 1993). The Cronbach’s alpha coefficient in this study was .87.
The Well-being (Well) measures the degree of happiness, satisfaction, and how rewarding or unsuccessful life is perceived to be (Sørensen, Bøe, Ingebrigtsen, & Sandanger, 1996), and the Cantril ladder (Cantril, 1966). The instrument contains four items, including “Would you say that you live a happy life at the moment?”; “When you think of how you are currently, are you most satisfied or dissatisfied?”; and “Would you say that your life is mostly filled with disappointments, or most encouragements?” The items are answered on a 7-point scale. The Cantril ladder contains one question: “Here is a ladder with 10 steps. If we think that the highest step on this ladder stands for the best life you could think of, and the lowest the worst. What step would you say suits you in your present life?” This question was answered using a 10-point scale. The mean score of the instrument was calculated by adding all the items, with the Cantril ladder multiplied by 7 and divided by 10, before adding the three other items, ranging from 1 to 7, with the higher the score the better.
The Strengths and Difficulties Questionnaire (SDQ; parent version) rates the child’s behavior and covers five dimensions: Emotional problems, conduct problems, hyperactivity, peer problems, and prosocial behavior (Goodman, Ford, Simmons, Gatward, & Meltzer, 2000). This instrument consists of 25 statements, including examples such as “Considerate of other people’s feelings,” “Constantly fidgeting or squirming,” and “Picked on or bullied by other children.” Each statement has three response alternatives: “not true,” “somewhat true,” or “certainly true.” The sum score was calculated by adding all the statements, which ranged from 0 to 50, with the lower the score the better. The instrument has been validated in other studies (Heyerdahl, 2003). The Cronbach’s alpha coefficient in this study was .78.
The FSOC scale measures the family’s global SOC (Antonovsky & Sourani, 1988; Sagy & Antonovsky, 1992). The FSOC is constructed and based on the three components in SOC, namely, comprehensibility, manageability, and meaningfulness (Sagy & Antonovsky, 1992), though FSOC is best understood as a single global factor (Ngai & Ngu, 2011). The scale consists of 12 items such as “Let’s say you’re tired, disappointed, angry, or the like. Does it seem to you that all the members of the family will sense your feelings?” and “To what extent it seems to you that the family rules are clear?” The items had a 7-point response options with the anchors defined. A scale score was computed by adding the items together ranging from 12 to 87, with higher scores denoting a strong sense of family coherence. The instrument has been validated in another study (Sagy & Braun-Lewensohn, 2009). The Cronbach’s alpha coefficient in this study was .87. The scale has not been previously used in this country, and was translated with inspiration from the elements of Brislin (1970). The instrument was pilot tested with 20 adults in the authors’ workplace, and some formulations were clarified, thereby making them more understandable.
The Family Assessment Device (FAD) measures the general family climate and functioning (Epstein, Baldwin, & Bishop, 1983), and in this study, the subscale of General Functioning was used (Miller et al., 2000). The subscale contains 12 statements, including six statements regarding healthy functioning in the family, such as “In times of crisis we can turn to each other for support,” as well as six statements describing unhealthy functioning in the family, such as “Planning family activities is difficult because we misunderstand each other.” The response options ranged from 1 = totally agree to 4 = do not agree at all. The FAD total score was calculated and the lower the mean score, the greater the family functioning. The instrument has been validated in other studies (e.g., Kabacoff, Miller, Bishop, Epstein, & Keitner, 1990). The Cronbach’s alpha coefficient in this study was .90.
The questionnaire was pilot tested with 10 parents in the ADHD association and was considered as relevant and not offensive, and no changes were made.
Statistical Analysis
Statistical analyses were performed using IBM Statistics SPSS, version 20.0. Descriptive statistics with frequencies, percentages, means, and standard deviations were used. Comparisons between groups were analyzed using Pearson’s chi-square tests, independent-sample t tests and one-way ANOVA. A post hoc test, Tukey honest significant difference (HSD), was used to find out where the difference among the groups occurred. A sequential linear multiple regression analysis (Field, 2013) was performed with FAD as a dependent variable, together with parents’ gender, age, self-reported ADHD, HSCL, Well, medication of the child, SDQ, and support from the health services as independent variables. The internal consistency was measured using a Cronbach’s alpha. All tests were two-tailed with a p value <.05.
Results
The mean age of the parents was 41.55 years and the majority of the parents were cohabitating or married. Some of the parents (15.2%) reported having ADHD themselves. Comparisons between mothers and fathers regarding characteristics in parents revealed only one significant difference in age, as the fathers were older (M age = 44.60, SD = 5.85) than the mothers (M age = 40.88, SD = 5.78), (t = 3.98; p = .001).
The mean age of the children with ADHD was 12 and most of the children were boys. In addition, most of the children were on medication for ADHD, and the parents rated their child’s behavior (SDQ) with a mean score of 23.39 (SD = 6.33). Support from health services in the municipalities was rated with a mean score of 4.15, while support from the specialist health services was rated with a mean score of 4.78 (Table 1).
Description of Parents, Children and Families.

Note. ADHD = attention deficit hyperactivity disorder; SDQ = Strengths and Difficulties Questionnaire.
SDQ, sum score could range from 0 (most favorable) to 50 (least favorable).
Support from health services, scores could range from 1 (lowest) to 7 (highest).
Psychological distress (HSCL) reported by the parents had a total mean score of 18.24 (SD = 5.61), and well-being (Well) had a mean score of 4.86 (SD = 0.92). FSOC was described with a total mean score of 57.88 (SD = 10.85) and family functioning (FAD) with a mean score of 1.98 (SD = 0.52).
Independent-sample t tests were conducted to compare the parents’ gender, marital status, and the educational level, as well as the children’s gender and medication, and place of residence in relation to HSCL, Well, FSOC, and FAD. Mothers reported significantly more psychological distress (HSCL; M = 18.59, SD = 5.66) than fathers (M = 16.53, SD = 5.08), (t = 2.26; p = .025), whereas single parents (M = 4.53, SD = 1.02) showed a significantly lower well-being (Well) than married/cohabiting parents (M = 4.91, SD = 0.90), (t = 2.29; p = .023). One-way between-group ANOVAs were conducted to explore the impact of the parents’ self-reported ADHD with regard to HSCL, Well, FSOC, and FAD (Table 2).
Comparing Parents With Self-Reported ADHD.

Note. ADHD = attention deficit hyperactivity disorder; CI = confidence interval; HSCL = Hopkins Symptom Checklist; Well = well-being; FSOC = Family Sense of Coherence; FAD = Family Assessment Device.
ANOVA.
HSCL-10, sum score could range from 10 (most favorable) to 40 (least favorable).
Well, scores could range from 1 (most favorable) to 7 (least favorable).
FSOC, sum scores could range from 12 (weakest) to 84 (strongest).
FAD, scores could range from 1 (most favorable) to 4 (least favorable).
There were significant differences regarding psychological distress (HSCL), well-being (Well), FSOC, and family functioning (FAD). Post hoc comparisons using the Tukey HSD test showed that parents with self-reported ADHD, and those who did not know whether they had ADHD, had more psychological distress than those not having ADHD. Furthermore, parents with ADHD reported a weaker well-being (Well) and weaker FSOC, and rated a less favorable family functioning (FAD).
Independent-sample t tests were conducted between parents with a child medicated for ADHD and not, with regard to HSCL, Well, FSOC, and FAD, and there were statistically significant differences between parents with a child medicated for ADHD and those who did not (Table 3).
Comparing Parents With Children Medicated for ADHD and Not.

Note. ADHD = attention deficit hyperactivity disorder; HSCL = Hopkins Symptom Checklist; Well = well-being; FSOC = Family Sense of Coherence; FAD = Family Assessment Device.
Independent-sample t test.
HSCL-10, sum score could range from 10 (most favorable) to 40 (least favorable).
Well, scores could range from 1 (least favorable) to 7 (most favorable).
FSOC, sum scores could range from 12 (weakest) to 84 (strongest).
FAD, scores could range from 1 (most favorable) to 4 (least favorable).
The parents with a child not medicated for ADHD had statistically significant more psychological distress (HSCL), a weaker well-being (Well), a weaker FSOC, and poorer family functioning (FAD) than parents of medicated children.
Multivariate Relationship of the Findings
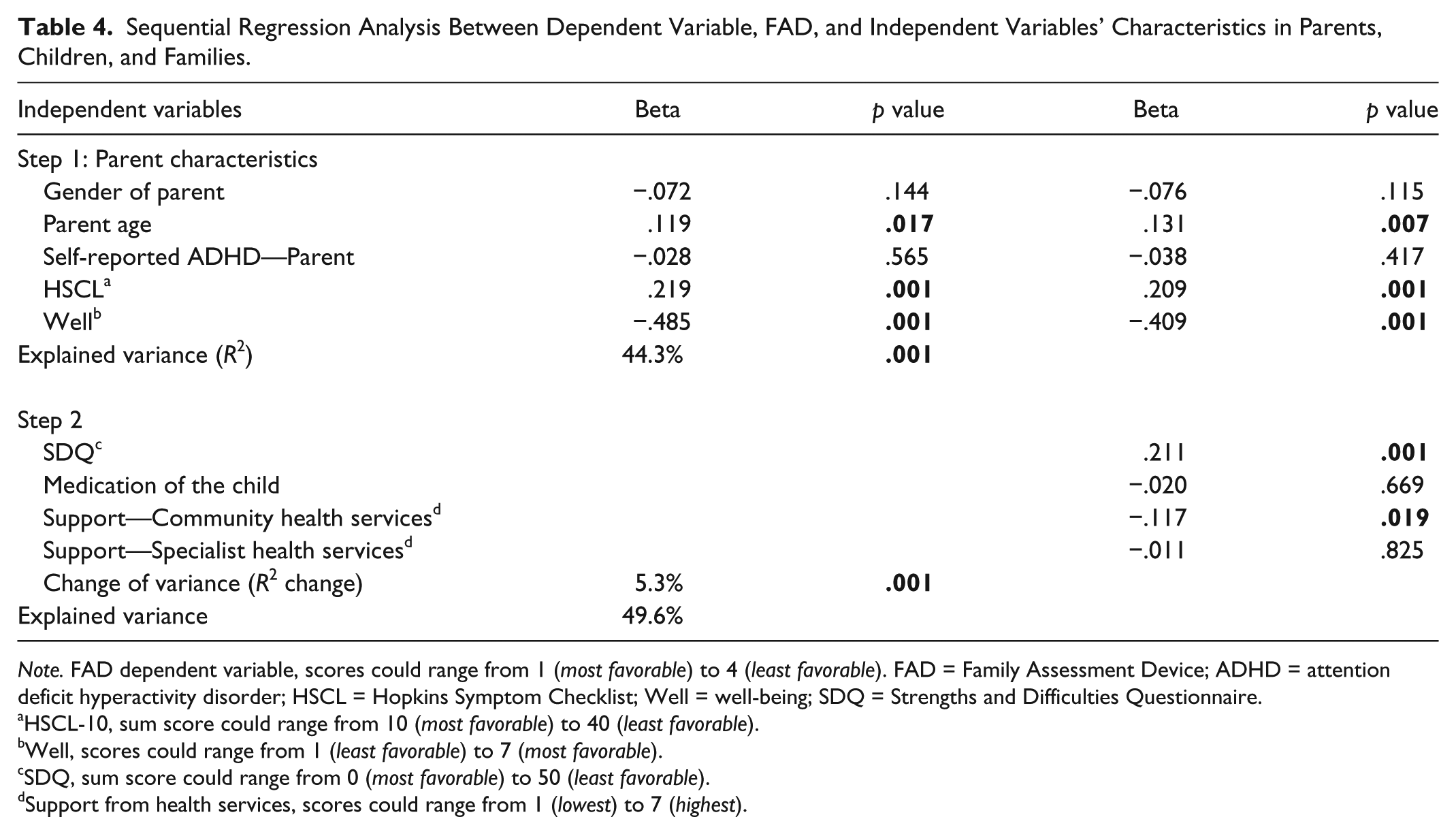
A sequential linear multiple regression analysis was run to investigate the impact of the independent variables on the dependent variable, family functioning (Table 4).
Sequential Regression Analysis Between Dependent Variable, FAD, and Independent Variables’ Characteristics in Parents, Children, and Families.
Note. FAD dependent variable, scores could range from 1 (most favorable) to 4 (least favorable). FAD = Family Assessment Device; ADHD = attention deficit hyperactivity disorder; HSCL = Hopkins Symptom Checklist; Well = well-being; SDQ = Strengths and Difficulties Questionnaire.
HSCL-10, sum score could range from 10 (most favorable) to 40 (least favorable).
Well, scores could range from 1 (least favorable) to 7 (most favorable).
SDQ, sum score could range from 0 (most favorable) to 50 (least favorable).
Support from health services, scores could range from 1 (lowest) to 7 (highest).
The variables related to the parents entered in Step 1 (parents’ gender, age, marital status, self-reported ADHD, HSCL, Well) explained 44.3% of the variance on FAD, and were significant (p = .001). The variables related to the child (SDQ and medication of the child) and the variables related to perceived support from the health services were added in Step 2, and explained 5.3% of the variance on FAD (p = .001). The combination of the independent variables explained 49.6% of the variation in the dependent variable, FAD.
Younger parents, low psychological distress, higher well-being, less problematic child behavior, and perceived support from the community health services had a positive effect on family functioning.
Discussion
Schroeder and Kelley (2009) described family functioning as one of the core problems in families with children having ADHD because these families have problems in organization and with family conflicts. The results of the sequential linear multiple regression analysis revealed that variables related to the parents explained 44.3% of the variation in family functioning. Over time, the load in the demanding life situation may negatively affect the parents and explain why the parents’ higher age negatively influenced family functioning. Paternal age and the influence on family functioning require further investigation. The parents’ psychological distress and well-being explained most of the variation. The impact of parental mental health and stress, and family conflicts, is important in families’ everyday life with children having ADHD (Kvist et al., 2013). The child’s behavior, the medication of the child, and support from the health services further described 5.3% of the variation in family functioning in the present study. These results highlight the importance of characteristics in parents and the interaction between family members, and how this interaction influences the family as a whole and the family function. Hence, the family as a whole should be in focus, and support from the community health services is essential. The public health nurse is one of the first in the health services these families meet, either in the local child health clinics or as a public health nurse at schools, and may be a trusted follower in the mapping and follow-up of families with children with ADHD in multidisciplinary collaboration with school personnel (Moen, Hedelin, & Hall-Lord, 2014).
Mothers reported more psychological distress than fathers, and it has been described that mothers are taking more responsibility in the upbringing and everyday life in families with a child with ADHD (Moen et al., 2011; Peters & Jackson, 2009). The mothers’ load of perceived responsibility may lead to psychological distress and reflect the typical gender roles in families (Gage, Everett, & Bullock, 2006), in which mothers are socialized into their families of origin to assume the primary caregiver role.
Psychological distress has been associated with lax parenting and not responding to the child’s misbehavior (Gerdes et al., 2007). Psychological distress is associated with less warmth and a positive involvement in their children with ADHD (Kashdan et al., 2004). This may escalate the family problems, as children with ADHD need a predictable everyday life (Moen, Hall-Lord, & Hedelin, 2014). Paternal warmth has been found to be particularly important in children’s peer acceptance, less peer rejection, and less social behavior, especially in boys (Hurt, Hoza, & Pelham, 2007) asking for a more positive involvement from fathers in the upbringing of children with ADHD. To help support the mother in the parental role, a positive involvement from the father in the upbringing of children may influence the FSOC.
Single parents reported weaker well-being than married/cohabitating parents, as single parents have to take all the responsibility by themselves, which may explain the weakness in well-being. There were no significant findings related to psychological distress, although the participants might experience weak well-being (cf. Sørensen & Næss, 1996).
Parents with ADHD reported more psychological distress (HSCL), weaker well-being (Well) and FSOC, and less favorable family functioning (FAD) than the other parents. There may be a divergence between parental decision making, less family structure and support, and less communication, sensitivity, and connection. Another study described mothers with ADHD symptoms having a low involvement and positive parenting, as well as high levels of inconsistent discipline (Chronis-Tuscano et al., 2008). Structure and routine in the family have been regarded as prerequisites for providing family life with a sense of security and control, which also made the life with a child with ADHD more stable (Moen, Hall-Lord, & Hedelin, 2014). Some of the parents (15.2%) had ADHD themselves, but 17% reported they did not know whether they had ADHD. The question is whether the stress and the challenge in parenting a child with ADHD may give them symptoms comparable with the ADHD diagnosis. In another study, parents who had ADHD themselves had sought medical assistance and got a better life with counseling and medication (Moen, Hall-Lord, & Hedelin, 2014). There is limited research in parents with own ADHD and how their vulnerability and other characteristics may influence family function. It is important that parents with ADHD receive support and supervision, both from the public health nurse and teachers in school or kindergarten, to help make the family life stable with structure and predictability.
FSOC includes the component of meaningfulness, which is important in family life, and parents have described hope for the future and coping in the parental role of having a child with ADHD (Moen et al., 2011). A family collective characterization given in FSOC is not independent of its individual elements, but it is also not a simple aggregation of the individuals (Ngai & Ngu, 2011). Mapping relationships among the members in the family may provide a key to understanding the collective orientation and help facilitate family adaptation in the management of children with disabilities such as ADHD (cf. Sagy & Antonovsky, 1992). Parents’ management training focusing on all family members may profit the whole family (Moen et al., 2011; Peters & Jackson, 2009).
Parents with children not medicated for ADHD reported more psychological distress, weaker well-being and FSOC, and poorer family functioning. Medication helps the child to facilitate concentration and avoid unimportant impressions that lead to less hyperactivity and aggression in the child with ADHD (Moen, Hall-Lord, & Hedelin, 2014). Consequently, less symptoms may lead to more predictability in family life, less conflicts, and better family functioning. Medication is described as only one of many interventions (Barkley, 2006). Other interventions, as parent management training, have been described as helpful regarding family function (Moen et al., 2011), not investigated in this study. Hansen and Hansen (2006) described parents facing a multitude of dilemmas in giving medication to their child with ADHD. However, parents may be more confident with medication when they have seen the beneficial effects that the medication had on their child (Moen, Hall-Lord, & Hedelin, 2014). The general practitioner and the public health nurse should cooperate in the supervision of parents considering medication of their child, and support the parents in their decision making. Multidisciplinary collaboration with the health service, psychological pedagogical service, and school personnel may benefit families with children with ADHD.
Strengths and Limitations
There are both strengths and limitations in this study. The response rate in the study was only 48%, in spite of two reminders. However, the power analysis was estimated assuming a drop-out rate at 50%. Pearson’s chi-square tests were run to compare the respondents with the nonrespondents and revealed no significant differences with regard to parents’ gender, the child’s age, and place of residence. Some of the mothers responded instead of the fathers, thereby giving a low response rate from the fathers. There are similar experiences from other studies that include mothers and fathers of children with ADHD (Cussen, Sciberras, Ukoumunne, & Efron, 2012; Hurt et al., 2007). The participants were members of the ADHD association, so the results may not be generalizable to parents who are not members.
Conclusions and Implications for Practice
Parents’ well-being and psychological distress, the behavior of the child with ADHD, and support from the community health services all influence family functioning. Parents with ADHD and parents with children not medicated for ADHD seem to be most vulnerable. The results indicate that both characteristics in parents and children influence family function. Parent management training with focus on effective parenting strategies, as well as training in parental cognition for the perception of parental stress, self-esteem, and locus of control, may help these parents in their parenting and help strengthen family functioning. The fathers need support to become engaged in the treatment and follow-up of children with ADHD to help ease the loads of perceived responsibility in mothers. In particular, parents with ADHD should be considered for treatment and family intervention strategies. Medication of the child seems to improve family life, and parents need support in their decision making, and focusing on the entire family is essential as a part of the early interventions. Parents need multidisciplinary support and supervision from the health service and personnel in school and kindergarten, both in their parenting and in their decision making and follow-up, and focusing on the entire family is essential because early interventions may help the family.
Footnotes
Acknowledgements
We would like to thank the Norwegian ADHD Association for helping us with the recruiting of participants and Jari Appelgren of Karlstad’s University for the valuable discussions concerning statistical analysis.
Author Contributions
Ø.L.M., M.L.H.-L., and B.H. designed the study; Ø.L.M. collected the data; Ø.L.M., M.L.H.-L., and B.H. conducted the analysis of data; and Ø.L.M., M.L.H.-L., and B.H. prepared the manuscript. All the authors have seen this final version and agreed upon it.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.