
Abstract
To integrate the care resources of the elderly, while promoting the development of formal social care resources, some countries have gradually turned to the development of family informal care resources. In China, informal family care has a more important role, whereas social formal care resources are far from meeting the needs of older people. Thus, this strategy can only be effective if there is a clear complementary relationship between informal care and formal care. Empirical analysis is selected from the China Health and Nutrition Survey (CHNS) database, which conducted 10 follow-up surveys in 12 provinces and municipalities in China. A two-tier stochastic frontier (TSFA) model was used to analyze the relationship between three different kinds of formal care and informal family care. The formal complementary and substitute effects on informal care eventually led to higher actual informal care level. The net effect of formal care on informal care is positive, and the complementary effects of formal care are still dominant even in different regions. Increasing informal care does not crowd out or reduce formal care; thereby, facilitating the return of care to families can effectively reduce public service expenditures.
Introduction
Under the background of the aging society, choice about elderly care of all countries was made between society and home, to form an optimal care model and provide qualified care for the elderly with minimal social costs. According to the statistics of China’s National Bureau of Statistics, those who are aged 65 years and above reached 176 million, accounting for 12.6% of the total population in China at the end of 2019. To actively face the growing risks of aging and disability, the general office of the Ministry of Human Resources and Social Security of the People’s Republic of China issued the guidance on the pilot of long-term care insurance (LTCI) system in 2016 and began to pilot LTCI policies in 15 regions of the country. Therefore, it is a priority to clarify the interaction mechanism between family and society in elderly care. In accordance with international practice, the form of care for the elderly can be divided into two categories: formal long-term care (LTC; formal care) and informal care (informal care). The former includes community-based informal care, institutional care, and so on, provided by the person signing the contract and get a fixed income by the employment contract. Informal care is a nonpaid, unorganized informal care provided by a spouse, adult child, or other relative, friend, neighbor, and so on, who has a social relationship with the serviced person. Elderly care includes informal and formal care. The former informal care comes from inside the home, which is mainly the daily companionship and life care of the elderly by family members such as children. Houtven and Norton (2004) and Charles and Sevak (2005) have studied that informal care and formal care were substitute in the United States, respectively. But whether informal care and formal care are substitute or complementary, naturally, depends on the exact purpose of using it (Bolin et al., 2008). In traditional society, elderly care mainly comes from within the family. Parents have strong motivations to raise children and to care for them when they are old. In China, exploring this issue has more urgent practical significance. First of all, in China, the current formal care system supply is seriously insufficient and fragmented. For example, the formal care system mainly focuses on the poor or the seriously disabled. Second, since 2016, China has started to pilot LTCI policy, but the pilot policies in the past 5 years have not formed a unified system model. So studying the relationship between formal care and informal care is conducive to promoting the unification and timely adjustment of LTCI policy, as well as clarifying the policy orientation. Influenced by the welfare pluralism, after experienced the socialization of a wide range of elderly services, some countries began to advocate “local aging” and “de-institutionalization” to return to the community and family (Davies, 1995). Most countries gradually combine the transfer payments of families with direct service delivery, and invest funds to nurture family networks to provide services, and gradually establish a new formal care market with competition (Lakdawalla & Philipson, 2002; Pavolini & Ranci, 2008).
The basic purpose of the formal care system is to guarantee the care service for the disabled. However, to some extent, formal care system will have an important impact on the traditional family informal care. From the perspective of system goal, LTCI policy must be supplement to informal family care. However, no matter in theory or practice, there is still relatively less research on the relationship between the two. On one hand, it is urgent to study whether the impact of formal institutional supply on informal family care is in line with the goal of system. On the other hand, in practice, it is also urgent to study the core transmission mechanism of formal institutional supply to informal family care. The studies of above are supposed to provide support for policy adjustment, such as the reasonable matching relationship between formal institutional supply and informal care supply. For this purpose, we select CHNS survey data and use bilateral stochastic frontier model to empirically test the relationship between formal and informal care, and explore the group heterogeneity and its leading factors.
Complementary Effect of Formal Care on Informal Care
The relationship between formal care and informal care is the core of this paper. From the perspective of system design objectives, both in theory and practice, formal care is a supplement to informal care. Promoting the level of informal care at home and the development of market-oriented LTC service is another important goal of formal system supply. But in the existing theoretical research, due to differences in research methods, there is no agreement on the relationship between formal and informal care. The starting point of present studies on the relationship between formal care and informal care is to find the optimal combination of care methods to reduce government spending on elderly care. In terms of bilateral effects, first, formal care has a complementary effect on informal care, and its mechanism of action is as follows: (a) Relieve informal care stress—Among the many external factors, the most direct impact of formal care on informal care is to reduce the pressure on informal care, to reduce the cost of informal care, and so on, but this is only for formal care projects that do not charge (Barrett et al., 2014; Börsch-Supan, 2012; Houtven & Norton, 2004; White-Means & Rubin, 2004). In areas with better social organization development, formal care has an advantage in mitigating informal care. The involvement of formal care will enhance the confidence of family members in providing care and improve the overall level of informal care (Bonsang, 2009; Imaiso et al., 2012). (b) Technology overflow—Formal care is mostly provided by third-party institutions, such as institutional pension plans, nursing homes, and so on (Frey et al., 2017; Ltd, 2002). Family members can learn and imitate the content and methods of services provided by professional caregivers. And in the process of informal care, the level of care is continuously improved, thereby improving the ability of informal care (Kalwij et al., 2012; Gaughan et al., 2015).
So, Hypothesis 0 (H0) was made:
The Crowding Effect of Formal Care on Informal Care
Second, formal care will also have a restraining effect on informal care to some extent, and its mechanism of action is as follows: (a) Social dependence on care—With the continuous involvement of formal care, third-party supply care services place higher demands on service quality, and the technical advantage of formal care forces family members to abandon their existing care services and rely on formal care services (Cantor, 1989; Ettner, 1994; Gray, 2003; Herron & Wrathall, 2018; Rickne, 2013; Stabile et al., 2006). Therefore, the formation of dependence on formal care makes the substitute effect of formal care on informal care (Cox et al., 2004; Cox & Jimenez, 1992). Especially when the cost of informal care is higher than that of formal care, the family chooses formal care rather than informal care (Chen et al., 2019; Hashimoto & Takahashi, 1995). (b) Formal care market competition—Due to the high cost and low-yield characteristics of elderly care service market (Bieber et al., 2017; Demeny, 2011; O’Shea et al., 2018), third-party enterprises have more demand to protect their income after intervention, to maintain a competitive advantage, so the main body of formal care will enhance its technological monopoly, such as the technological monopoly of medical device research (Geerts & Bosch, 2012). However, it will also tend to supply more general market-based aged care services, resulting in general informal care needs being substituted by formal care. However, there is still an insufficient supply for special needs, such as professional care (Ford and Mccormack, 1999; Houtven & Norton, 2008). Scholars have suggested that the use of different estimation methods will also lead to different conclusions (Bolin, 2008; Charles & Sevak, 2005; Liu & Yan, 2015; Pezzin & Reschovsky, 1996). And some studies have shown that there is no significant relationship between formal and informal care (Christianson, 1988; Motel-Klingebiel et al., 2005; Mettler & Vimarlund, 2011).
According to the previous analysis, we propose the following two hypotheses:
Informal and Formal Care of the Elderly in China
However, the LTC system in China relies heavily on informal care provided by family members. In China, the existing research on the relationship between formal and informal care of the disabled elderly in China is rich. For example, Hu found that projected demand is sensitive to changes in older adults disability trajectory and the availability of formal care provided by the government, but less sensitive to an increase in singleton households in the future (Hu, 2018). As one of the fastest growing elderly populations in the world, the health of older adults in China will have obvious implications for future formal and informal care costs, an issue that is of great concern to Chinese policy makers (Lyatamila & Zhao, 2016). Hu and Sai (2016) examine the factors affecting the receipt of informal care among older adults in China. And they found that the determinants of receiving informal care differ remarkably according to the sources of care. And disability and living arrangements are the most important determinants. The above results show that the supply of formal LTC services has an important impact on the traditional family informal care, and due to the differences of family characteristics, health status, and other individual factors, there are significant differences in the degree of benefit of different groups in the formal care. However, existing studies have not examined the impact of formal care on informal care from the perspective of bilateral effects. In fact, there are differences in the two-way effects of formal care, resulting in differences in net effects and institutional design goals, which will also be the focus of our research.
In summary, the existing research has the following shortcomings: (a) There are many studies that have analyzed the unilateral effects of formal care on informal care, that is, substitute or complementary. (b) Under the premise of “substitute” or “complementary” effects, the net effect of formal care on informal care has not been measured in detail, but specific quantitative research can provide policy support for regional formal care supply. (c) There are many studies on formal and informal care literature from micro-individuals, but neglected that formal care has a certain threshold effect on community characteristic variables. Compared with the existing literature, the main marginal contribution of this article focuses on the following two points: (a) In terms of research methods, with the help of bilateral stochastic frontier model, we empirically test the impact of formal care on informal care, investigate whether the impact of formal care on informal care is bilateral or unilateral, and explore the dominant force of its net effect, so as to break through the limitations of existing research methods. (b) From the perspective of research, we focus on the LTC for disabled people, take the net effect of formal care on informal care and its transmission mechanism as the core, reveal the relationship between formal care and informal care, and explore the group heterogeneity in different situations, so as to enrich the research perspective of LTC services.
Methods and Data
Two-Tier Stochastic Frontier (TSFA) Model Setting
According to the previous theoretical analysis, formal care has two effects of complementary and substitute effects on informal care. We measure the magnitude of the two effects and their net effects by the TSFA model, identifying the impact of formal care on informal care. The decomposition formula for informal care is:

Among them,
We use the following formula to convert the absolute value to a percentage of the formal care complementary effect or the substitute effect above or below the optimal level. We only list the core results of TSFA model derivation here. Refer to Appendix B of this study for the specific derivation process. The conversion formula is as follows:


Furthermore, the net effect of formal care on informal care can be expressed as:

Data and Variables
Data sources
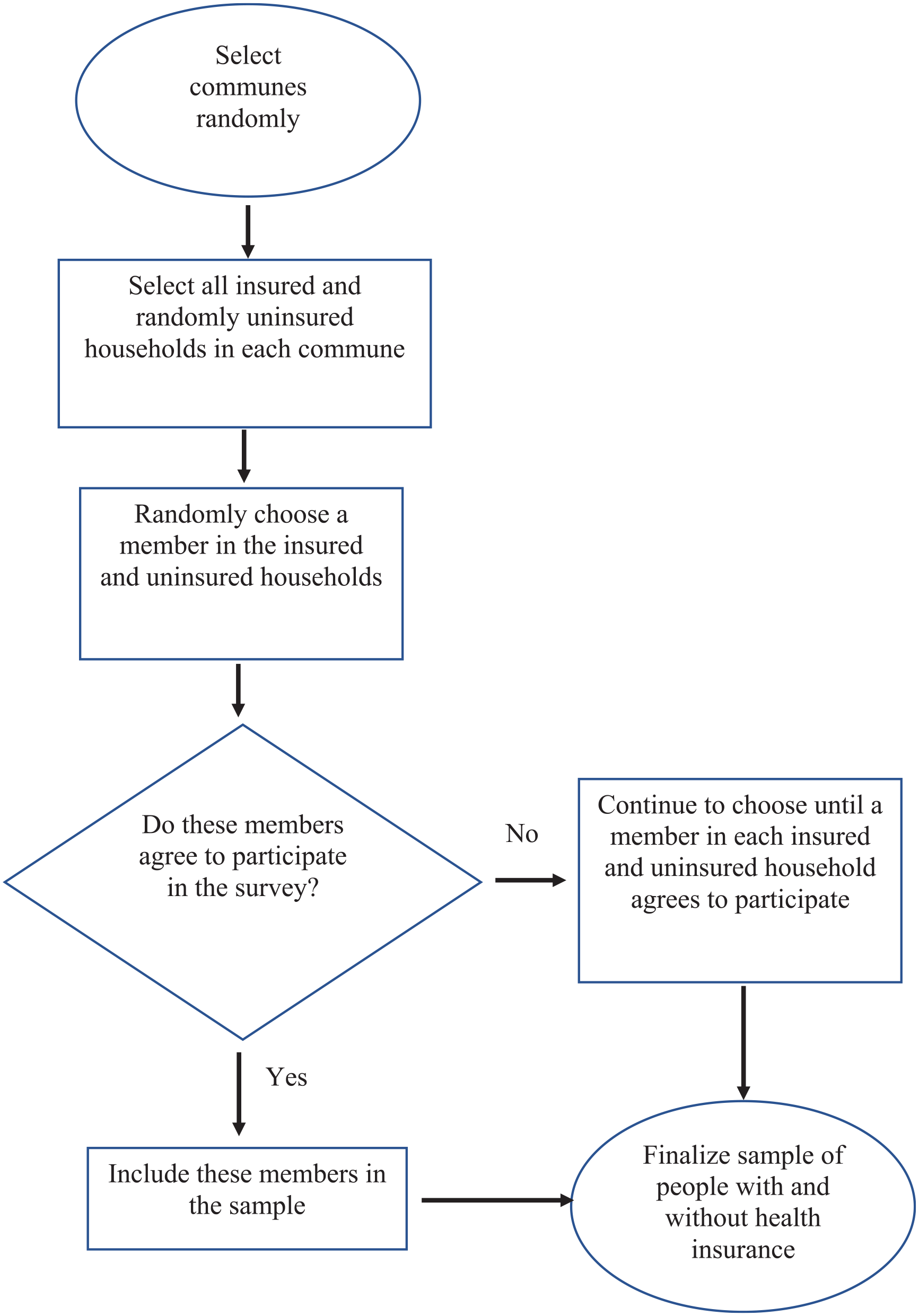
The study utilized data from the CHNS. The database covers data about multiple provinces in China under geographical characteristics, economic development levels, and differences in public resources and health indicators. A total of 10 surveys were conducted between 1989 and 2015, and each survey interviewed approximately 4,400 families, including 19,000 individual samples and some community statistics. This study selected 10 surveys data from 1989 to 2015 to conduct follow-up studies. In data processing, we use wave, individual ID, family ID, and community ID as keywords to merge data in STATA15.0. In terms of regional characteristics, to facilitate comparative analysis, the data of 53 (Yunnan), 33 (Zhejiang), and 61 (Shaanxi) added in 2015 were excluded. Finally, valid sample data including 10 surveys in 12 provinces and cities including Beijing, Liaoning, Heilongjiang, Shanghai, Jiangsu, Shandong, Henan, Hunan, Hubei, Guangxi, Guizhou, and Chongqing were obtained. On the age sample, families with elderly people aged 60 years and above are selected. In order not to affect the statistical results, we also excluded some missing or invalid values.
Variables
Dependent variables—Informal care
The content of informal variables in this study is mainly obtained through three questions. First, it includes (a) personal care, for example, bathing, catering, shopping, taking public transportation, managing money, and using the phone; (b) practical household help, for example, help from spouse, other family members, friend, relative, or neighbor; and (c) engagement in other housework, such as buying food, cooking, cleaning the room, and washing clothes for the family. Consistent with Bolin et al.’s (2008) research, the above three parts obviously consist of assistance as well as care, but for simplicity, all help will be named informal care in the following. Second, according to the alternatives: (a) no difficulty, (b) have some difficulties, but still can finish, (c) it needs help to complete it, (d) can’t finish at all, and (e) do not know. We select the people who have difficulties and need help as the basic sample, and the primary caregiver is “1, spouse; 2, other family members; 3, friends, relatives, or friend” as the informal caregiver. The informal care variables were determined according to the response asked: “1. Did you do this activity last week?” and “2. How long does it take on average per day? (minute).” In other words, the former reflects the category variables of informal care, and the latter reflects the number of informal care. Finally, we choose the previous question because we found that there are more statistical missing values in the questionnaire, and the reason may be that most respondents do not have a clear understanding of their time spent on informal care. So the first question can better reflect the real situation. And the values 1 to 3 represent personal care, practical household help, and engagement in other housework, respectively. The specific statistics are shown in Table 1. And we finally got 2,883 valid samples.
Descriptive Statistics of Core Variables.

Independent variables—Formal care
Here we refer to the six categories of formal care, namely, independent variables. According to the definition of formal care variables, we choose any local health worker visit, any doctor visit, any hospitalization, and the number of hospitals as the proxy variables of formal care variables. And they all represent the care services provided by formal medical service providers, such as professional medical care. Specifically, the four indicators are defined as follows: formal care provided in the household environment, and the variable was defined as having received any of the following categories of care: when you feel uncomfortable, (a) get a local health worker at home to get care, (b) go to the doctor (clinic, hospital), (c) when life is difficult, medical staff can help, and (d) is there hospitalization in the past 4 weeks? The variables indicating the amount of utilization were as follows: the number of (a) doctor visits (if the respondent’s answer is an outpatient visit, then the respondent has spent so much money, for example, including all registration fees, drug fees, treatment fees, etc., in units, divided by the average cost per visit, and will be treated as formal care usage.) and (b) hospitalizations (in the past 4 weeks, have you been in the hospital for a few days or have you lived for a few days?). However, it should be emphasized that the professional care services provided by professional nursing homes or nursing staff are not included here, as the survey data are mainly for the general elderly population with noninstitutional care. In the survey options, the number of outpatients (including door-to-door service) or inpatients was used for quantitative reflection. In combination with the sample data processing, there are many missing values in the number of hospitalizations, and finally, we eliminated the variable in the empirical test.
Control variables
This study is based on micro-studies of family units and thus controls the family characteristics, community characteristic variables, and individual characteristics that affect informal care. Family characteristics include family capital and family size. Community feature variables mainly include communities in statistics like economic component score, housing component score, and market component score. Individual characteristics include age, years of education, health conditions, and physical activity. Descriptive statistics for core variables are shown in Table 1. And we use the social service score and the transportation component score as instrumental variables to handle the endogeneity of the regression results. The reason is that the social service score and the transportation component score are related to formal care, but their development is strictly dependent on the financial input of the local government, so it can be assumed to be exogenous.
The specific descriptive statistics are shown in Table 1. The mean value of informal care was 1.5544, while the average mean time for informal care was 3.7618 hr, and the mean value of the logarithm was 1.3183. The mean local health worker visit for formal care and mean doctor visit were 0.0131 and 0.0567, respectively. Besides, the average hospitalization was 0.0130 and the number of hospitalizations was 0.0842.
Results
We first estimate the measurement model, and the results are shown in Table 2. The results in the second and third columns show that any hospitalization will substitute the individual’s informal care. The fourth column of Table 2 is the result of using the instrumental variable regression for the model. The results show that any local health worker visit and any doctor visit have complementary effects on the individual’s informal care. Using the instrumental variables two-stage least squares (2SLS) estimator, we obtained a negative and significant correlation between formal and informal care, which suggests that the two are substitute, too.
Basic Estimation Results of Two-Tier Stochastic Frontier Model for Informal Care..

Note. The detailed regression results of the third column are shown in the Appendix A. Model (3) is the result of processing the tool variables for the three variables, so it is the result of the three sets of tests. Here, just for the convenience of display, put together, not the tool substitution of the three variables at the same time, the adjusted R2 of the three sets of data are .1032, .0625, and .0921, respectively. OLS = ordinary least squares; 2SLS = two-stage least squares.
p < .05. **p < .01.
We test the appropriateness of the employed instruments, as shown in Table 3. The results show that any local health worker visit rejected the null hypothesis that the instruments have no joint effect; however, the results of the two cases of any doctor visit and any hospitalization accepted the null hypothesis that the instruments have no joint effect. And we tested overidentifying restrictions. The results show that weak instrumental features for instrumental variables under any local health worker visit and any doctor visit, however, any hospitalization, rejected the null hypothesis that there is no weak instrumentality. And we also tested the null hypothesis and the original hypothesis is “H0: variables are exogenous.” The results show that the original hypothesis was rejected under any local health worker visit. Therefore, we use the instrumental variable for analysis under Model (3) in Table 2. Both any hospitalization and any doctor visit accepted the null hypothesis, which means that there is no endogenous problem. Therefore, when we further study the relationship between informal and formal care, we analyze it by the bilateral stochastic frontier model in Table 2, and the reasons are explained in the theoretical basis.
Specification Test of the Instrumental Variable Regression.

Variance Decomposition: Explanatory Ability of Formal Care Effect Model in Informal Care
The variance decomposition in Table 4 is the decomposition of the effect of income inequality, not the decomposition of income inequality (distinguish from the second part). The income inequality decomposition has been completed in the research method of the second part of this study, and then by the TSFA model, put the decomposed formal LTC into the residual items
Analysis of Informal Care Effects of Formal Care.

The Extent of Formal Care Impact on Informal Care
To calculate the substitute effect and complementary effect of formal care, the level of informal care is deviated from the level of frontier informal care. The regression results in Table 5 show that, on the whole, the complementary effect of formal care on informal care makes the actual informal care level higher than the frontier informal care level of 45.87%. The substitute effect of formal care reduced the actual informal care level by 43.41%. The interaction between the two ultimately resulted in an actual informal care level that was 2.46% higher than the frontier informal care level. The average informal care level calculated according to the sample in this study was 1.5544, an increase of 0.0373 over the frontier informal care level. The distribution of complementary effect, substitution effect, and net effect of formal care and informal care is shown in Figure 1.
Estimation of the Effects of Formal Care on Informal Care.

Formal care for informal care complementary effects, substitute effects, and net effect nuclear density.
The fourth to sixth columns of Table 5 report in detail the distribution of formal care complementary effects, substitute effects, and net effects. We also performed a robust estimate of the sample; Q1, Q2, and Q3 represent sample proportions at 25%, 50%, and 75%, respectively. In the first quartile (Q1), the combination of formal care substitute effect and complementary effect increased the informal care level by 2.64%, higher than the average level of 2.46%. In the second quartile (Q2) and the third quartile (Q3), the combination of formal care substitute effect and complementary effect increased the informal care level by 2.46% and 2.28%; both are equal to or less than the average. The reason is that in the first quartile family, such families are poor with low incomes and low economic assets, and the community has problems such as low economic level, poor health quality, poor living conditions, low market level, poor social services, inconvenient transportation, and poor educational environment (Bondarenko, 2008; Mcmahon & Luthar, 2007; Quane & Rankin, 1998). Limited to the overall development level of the community, the informal care level with the intervention of formal care, the overall informal care shows a higher level (Barrett et al., 2014; Gray, 2003); thus, the net effect of formal care makes the overall informal care level increase of low-income families more significant. In the second and third quartile, the overall development level of the community is much better than the first quartile family, and the average family asset level is also relatively good. Both the substitute and complementary effects of formal care have a small impact on such family, showing a lower net effect level.
Discussion
Regional Distribution Characteristics of Formal Care
To further verify the robustness of the estimated results, this study further introduces provincial and regional samples to identify the interprovincial differences in the effects of formal care substitute and complementary effects on informal care. The test results are shown in Table 6. The results show, among the 12 provinces selected from the sample, from overall perspective of the region, the social effectiveness of informal care in the eastern and western regions should be higher than that in the central region. And the formal care in the western regions has the highest net effect on informal care.
Distribution of Net Effect of Formal Care on Informal Care.

The explanation for this regional difference is as follows: (a) From the perspective of alleviating the pressure of informal care and complementary effects, the overall economy in the eastern region is better than that in the central and western regions. Families in these areas have relatively good economic conditions, so informal care is less affected by the overall impact of formal care. However, it is opposite in western regions. The overall income level of family in these areas is low, but the involvement of formal care can promote the overall informal care level of such families through higher technology complementary effects (Demeny, 2011; Herron & Wrathall, 2018). That is, the complementary effect of formal care is higher than its substitute effects, which promotes the high net effect of formal care in the region, thus verifying the rationality of H0. (b) From the perspective of dependence of formal care and formal care market competition, the income of family in the eastern region is relatively higher. The involvement of formal care will, to a certain extent, lead to family dependent on society and market plunder by third-party participants. In the eastern region, the regional economy is developed with mature formal care market, which makes more families willing to choose to buy professional services provided by third parties (Cantor, 1989; Bieber et al., 2017), and choose to enjoy at home, which belongs to informal care, in fact. Therefore, the dependence of formal care and market competition have not caused the high substitute effect of informal care in the eastern region. In the western region, due to the relatively lagging economic level, the family income and asset levels are low. On one hand, the family within the western region is not dependent on formal care; on the other hand, the development of formal care institutions in this region is lagging behind. As a result, the overall substitute effect of formal care on informal care is low. Therefore, the verification of H1 is correct.
Threshold Effect Under Family Characteristics
To further analyze the regional differences of the impact of formal care on informal care, we analyze the threshold effect of formal care on informal care from the aspects of family income, human capital, and family size.
From the perspective of family economic income, the previous regression results show (Table 7) that the coefficient of family economic income is 0.0322, and family economic income has a significant impact on informal care. The results show that the net effect of formal care on informal care is 2.46% in the high-income group and 2.46% in the low-income group. The net effect gap between the two groups is 0, indicating that there is no obvious threshold for the impact of family income on formal and informal care.
The Impact of Family Characteristics on the Net Effect of Formal Care.

The Table 7 results show that the net effect of formal care on informal care is 2.47% in the high human capital group, 2.45% in the low human capital group, and the difference between the two groups is 0.02%. At a certain value, the crowding out effect of formal care on informal care decreased significantly.
When taking family size as the threshold analysis, the Table 7 results show that the net effect of formal care on informal care is 2.43% in the high family size group and 2.48% in the low family size group. And the difference between the two groups is 0.05%. This shows that family size has a significant threshold effect on the level of formal care, that is, when family size is lower than a certain threshold, the family size has a comprehensive promotion effect on the net effect of formal and informal care.
Conclusion
With the CHNS survey data of family and community from 1989 to 2015, this study empirically tests the bilateral effects of formal care on informal care levels using a TSFA model. With that, the substitute effect, complementary effect, and net effect of formal care on informal care are further estimated. Several conclusions can be made as follows: (a) The results of the TSFA model show that formal care has a significant impact on the level of informal care. And the formal care substitute effect makes the informal care level lower than the frontier informal care level of 43.41%. The complementary effect of formal care makes the informal care level higher than the frontier informal care level of 45.87%. The interaction between the two makes the actual informal care level higher than the frontier informal care level of 2.46%. (b) In terms of regional distribution characteristics, the regional sample estimation results show that the overall net effect of formal care in the eastern and western regions of China is higher than that in the central regions.
By the above analysis, we believe that formal care promotes the growth of informal care levels because the complementary effect of formal care is higher than the substitute effect of formal care. Therefore, we can adjust the deviation from the optimal level of informal care from the following aspects with this study. (a) Substitute effect of formal care should be reduced. The government can appropriately adjust and optimize the income redistribution system to ensure that vulnerable families receive better income security. At the same time, by lowering the threshold of social service supply, the possibility of formal care for vulnerable families is enhanced, and more opportunities for disadvantaged families to become better are provided. (b) Complementary effect of formal care should be improved. Increasing the complementary effect of formal care can effectively exert its incentives for families, improve informal care capacity through complementary effects, reduce informal care costs, and relieve family economic difficulties caused by the high cost of informal care. On one hand, we can improve the formal care policy, such as professional technology and service complementary in formal care, to enhance the improvement of informal care capacity and reduce the burden of survival. On the other hand, the government transfer payment system and social security policies should be optimized, such as the tax system and the social insurance system should be improved to gradually reduce the tax burden and social insurance contributions of vulnerable groups. Thus, a better social environment for vulnerable members can be provided and the cost pressure of informal care also can be reduced.
Because the CHNS data are merged, we have less than 100 valid samples of synthetic samples of the hours of informal care and the number of hospitalizations in the full sample, which will cause bias in the regression results. Therefore, we did not examine the relationship between informal and formal care in quantity, but only considered the impact of LTC. This is also one of the main research limitations of this study.
Footnotes
Appendix A
Basic Estimation Results of Two-Tier Stochastic Frontier Model for Informal Care..

| (1) | (2) | (3) | |||
|---|---|---|---|---|---|
| Variable | OLS marginal effect/coefficient of informal care | Frontier marginal effect/coefficient of informal care | Ivregress 2SLS marginal effect/coefficient of informal care | ||
| Any local health worker visit | −0.1310 | −0.1200 | −4.1850* | ||
| (−1.09) | (−1.03) | (−1.76) | |||
| Any doctor visit | −0.0074 | −0.0144 | 12.2000 | ||
| (−0.07) | (−0.14) | (0.65) | |||
| Any hospitalization | −0.2490** | −0.2250* | −0.3970 | ||
| (−2.08) | (−1.96) | (−0.12) | |||
| Age | 0.0059 | 0.0048 | 0.0011 | 0.0026 | 0.0063 |
| (1.00) | (0.84) | (0.53) | (0.54) | (0.95) | |
| Age squared | −0.0001** | −0.0001* | −0.0001*** | −0.0001 | −0.0002** |
| (−2.00) | (−1.86) | (−2.77) | (−1.37) | (−1.97) | |
| Years of education | −0.0439*** | −0.0412*** | −0.0442*** | −0.0304** | −0.0419*** |
| (−10.97) | (−10.48) | (−15.87) | (−2.00) | (−10.60) | |
| Health conditions | −0.0535 | −0.0627 | 0.6810** | −5.1710 | −0.0384 |
| (−0.78) | (−0.95) | (2.19) | (−0.64) | (−0.21) | |
| Physical activity | −0.0085*** | −0.0084*** | −0.0063*** | −0.0037 | −0.0084*** |
| (−4.77) | (−4.88) | (−9.76) | (−0.83) | (−3.82) | |
| Family capital | 0.0128 | 0.0155 | 0.0192*** | 0.0127 | 0.0109 |
| (1.06) | (1.32) | (4.61) | (1.03) | (0.85) | |
| Family size | −0.1530*** | −0.1470*** | −0.1380*** | −0.1540*** | −0.1510*** |
| (−7.21) | (−7.14) | (−18.59) | (−5.68) | (−7.08) | |
| Economic component | −0.0073 | −0.0059 | −0.0059 | −0.0094 | −0.0071 |
| (−0.56) | (−0.47) | (−1.20) | (−0.74) | (−0.50) | |
| Housing component | 0.0211 | 0.0196 | 0.0087 | 0.0345 | 0.0212 |
| (0.92) | (0.87) | (1.12) | (0.87) | (0.77) | |
| Market component | −0.0065 | −0.0078 | −0.0083* | −0.0010 | −0.0047 |
| (−0.68) | (−0.84) | (−1.70) | (−0.17) | (−0.44) | |
| Province | Yes | Yes | Yes | Yes | Yes |
| Wave | Yes | Yes | Yes | Yes | Yes |
| _cons | 3.9140*** | 5.5410*** | 3.6910*** | 3.0110*** | 3.8360*** |
| (17.06) | (22.95) | (31.82) | (3.74) | (17.28) | |
| Adjusted R2 | .0620 | — | .1032 | .0625 | .0921 |
| sigma_u2 | — | 2.3437 | — | — | — |
| sigma_v2 | — | 1.3540 | — | — | — |
| sigma2 | — | 3.6977 | — | — | — |
| gamma | — | 0.6338 | — | — | — |
| N | 2,883 | 2,883 | 2,883 | 2,883 | 2,883 |
Note. t statistics are in parentheses. OLS = ordinary least squares; 2SLS = two-stage least squares.
p < .1. **p < .05. ***p < .01.
Appendix B
Acknowledgements
The authors are very grateful for the financial support of the National Natural Science Fund of China and Zhejiang Philosophy and Social Science Planning Project.
Author Contributions
H.L. revised the article critically for important intellectual content and approved the version to be published and carried out language retouching and modification. M.X. and Y.T. made a substantial contribution to the concept and design of the work, interpretation of data, and drafted the article.
Availability of Data and Materials
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received financial support from the National Natural Science Fund of China (71904167) and Zhejiang Philosophy and Social Science Planning Project (20NDQN302YB).