
Abstract
This paper documents, and reflects on key strengths and weaknesses of, existing patient feedback management systems at primary health care in Bangladesh and proposes key implications for future policy and practice. A mixed-method study was conducted in two Upazila (sub-district) Health Complexes (UHC) within one district in Bangladesh. It reports qualitative data from thematic analysis of in-depth interviews (n = 15) with key stakeholders; non-participant observations of feedback environment at UHCs; document review; and a stakeholder workshop. Patient feedback data from publicly available web portals were also analyzed. Multiple parallel patient feedback systems exist at health facilities. Key strengths across all systems included common goals of ensuring accountability and patient voice and high-level commitment. Common weaknesses included lack of documented processes, limited awareness of available channels among patients and a lack of documented actions following feedback. The findings helped to provide a few implications for future policy and practice on patient feedback management.
Introduction
Patients’ feedback based on their experiences of receiving health care is a vital tool for improving quality of health services (Holmes-Bonney, 2010; Hsieh, 2012a, 2012b; Natangelo, 2007). Patients can identify issues that management is not aware of and can offer health-care managers innovative ideas for improvement. The opportunity to respond to patients’ feedback, in turn, leads to responsiveness which is a widely recognized objective of national health systems (Phillips et al., 2016; World Health Organization, 2007, 2012).
Feedback from patients can create an effective interaction between service users and service providers that is a key component of the responsive health system (Lodenstein et al., 2013; Molyneux et al., 2012; Thi Thu Ha et al., 2015). Such interaction is significant in two ways. First, it enables the service users to provide feedback on the service they receive as well as the skill and behavior of service providers (Debono & Travaglia, 2009; Reader et al., 2014; Thi Thu Ha et al., 2015). The term “feedback” from service users is used for both complaints (i.e., grievances) and praises (i.e., positive reflections). Second, the interaction allows improving the quality of health services (Hsieh, 2010, 2011) and strengthening of the human resource management process (Hsieh, 2011; Martineau et al., 2015; Mshelia et al., 2013) through collection and utilization of the feedback.
Patients have the right to file complaints with organizations when they are unsatisfied with the treatment received, and health care organizations should have processes in place for appropriately responding to these on time (“Managing Patient Complaints and Grievances,” 2016; Thi Thu Ha et al., 2015). Globally, the voice of health service users or patients is increasingly in demand in order to develop healthcare services (Renedo et al., 2015). Complaints management systems are, therefore, an established feature of national health systems in high-income countries implemented to improve the patient experience (Stokes et al., 2006). A well-functioning patient feedback system can provide opportunities for developing risk management or healthcare quality improvement programs in which preventive or proactive mechanisms can be set up. Such a system can also enable patients to contribute to the improvement of services and participate more actively in self-care. Tracking the trend of patient complaints may call attention to systems or individual performance problems and suggest areas for improvement. Conversely, positive feedback from patients can highlight well-functioning areas where patients are satisfied with their experiences of healthcare and therefore provide examples of best practice.
Patient feedback typically involves approaching local health facilities, and if needed, subsequently appealing to higher-level authorities such as courts or insurance companies (Holmes-Bonney, 2010; Hsieh, 2010). Specific mechanisms for receipt of feedback include dedicated suggestion mailboxes, email addresses, text messaging systems, telephone hotlines, interactive websites, and office windows staffed with complaints handling officers (Rohwerder & Rao, 2015; Thi Thu Ha et al., 2015). Issues raised by patients can vary in severity, from patients’ concerns of not being listened to, through to death because of poor care. At the same time, specific causes typically relate to professional conduct, provider-patient communication, treatment and care of patients, medical errors, malpractice, lack of skills, waiting for care, and costs (Kuosmanen et al., 2008, pp. 2000–2004; Montini et al., 2008).
A systematic review of the effects of involving users in health care through improving patient feedback found evidence of improved health services (Crawford et al., 2002). However, much of this evidence comes from high-income contexts, suggesting limited patient involvement in health care within low- and middle-income countries (LMICs), and consequently limited research in this area (Mirzoev & Kane, 2018). A review commissioned by the World Bank found only a few descriptions, reviews or evaluations, of feedback procedures in LMICs (Gauri, 2013). Furthermore, there is a dearth of literature on patient feedback systems from primary health care facilities because most evidence comes from secondary and tertiary hospitals.
This paper, therefore, aims to bridge the above gaps in the published literature by reporting an analysis of different patient feedback systems from primary health care facilities in Bangladesh. The specific objectives of this paper are two-fold: first, to identify the existing systems for patient feedback management at primary health care level in Bangladesh, and second, to explore their key strengths and weaknesses to inform future policy and practice of promoting a wider agenda on citizens’ voice and accountability to improve health care quality. Therefore, this paper seeks the answers for two questions: what systems are available at the primary care setting for patient feedback? And, which systems are more functTabional in terms of their inherent characteristics?
Results are reported from Bangladesh, a low-income country in Asia where ensuring patients’ voice and accountability is high on the government agenda (Naylor et al., 2013), and is reflected in different patient feedback systems initiated by the Bangladeshi Government and its Ministry of Health and Family Welfare (MOHFW). We believe that this piece will be of relevance and interest to national and international decision-makers including practitioners, researchers, and development agencies who are interested and are engaged in understanding, and improving, patient feedback management systems in the context of LMICs.
Methods
This paper reports findings from a wider multidisciplinary and mixed-method study. We identified the existing patient feedback systems by a desk review and structured observations in two different Upazila Health Complexes (UHCs) within one district in Bangladesh. Then, we explored their characteristics in terms of strengths and weaknesses from the perspective of both demand and supply side of the primary health care centers by in-depth interviews (IDI) with both service provides and service users. Finally, we validated our findings by a stakeholder workshop involving all actors related to the feedback systems.
The UHCs were focused in this study as they provide the first level referral services from the other two primary health care facilities (community clinics, and union health and family welfare centers) and therefore are a backbone of the country’s health system. There are 421 UHCs in Bangladesh; a typical UHC serves a population of 200,000 to 400,000 and has both in and out-patient departments. The details of the methodology of the overall study are available elsewhere (Ebenso et al., 2017), and this paper discusses the existing systems for patient feedback in Bangladesh. The data reported herewith were collected between January 2017 and March 2018.
The desk review focused on relevant MOHFW guidelines and policies, facility records of feedback management such as staff meetings or clinical reviews, published reports in newspapers, government websites on feedback systems, and data from the publicly accessible MOHFW web portal (http://103.247.238.81/webportal/pages/complain.php). The quantitative data from the web portal were analyzed to evaluate the nature of and trends in patient feedback during the last 8 years (January 2012—December 2019), that is, since the introduction of the respective feedback system. This portal includes details of feedback provided when a patient uses two feedback channels. The publicly available documents related to the patient feedback systems were reviewed (18 in total) to understand existing policy guidelines, reports, regulatory documents, and articles.
Non-participant observations were conducted at four UHCs in one District in April to May 2017, to understand the wider context of the availability and accessibility of feedback systems for patients at UHCs. A structured observation checklist was used to summarize the observation notes, which provided useful data reported in this paper. The checklist answered details of each of the following scenario: (a) Modality of providing feedback or complain, (b) If a Complain box is available, (c) If a Telephone number is available, (d) If a complaint register is available, (e) other information or instructions available, and (f) Informal interactions with service users. Frequencies of use of the available feedback systems were also recorded. The findings of the observation informed the content of the semi-structured guideline used for the IDIs.
The IDIs were conducted with 15 purposefully selected respondents from sub-district and national (MOHFW) levels including patients, service providers, managers, and policymakers (details are shown in the table below) to explore their knowledge and experiences of engaging with patient feedback systems. The interviews were audio-recorded following obtaining informed consent.
Summary of Qualitative Interviews.

Note. UHC = Upazila Health Complexe; MOHFW = Ministry of Health and Family Welfare. (Source: RESPOND project participant recruitment summary, June 2017).
A stakeholder workshop was held in March 2018, which involved about 20 representatives from the government, non-government organizations, and development partners. The aim of the workshop was first, to share, discuss, and validate emerging findings from the other methods and second, to collect further data through exploring participants’ views and experiences. Following informed consent, the discussions were audio-recorded, and the rapporteurs took detailed notes from each group for further analysis.
We followed a “three steps framework” identified by a recent review on patient feedback management (Mirzoev & Kane, 2018) to analyze the findings: (a) collection of feedback, (b) analysis of feedback, and (c) action on feedback. All three steps are important and interrelated, and can be influenced by a number of factors (Mirzoev & Kane, 2018):
Collection of complaints depends on appropriate policy and regulatory framework in place, and the capacity and willingness of patients to complain, which is often influenced by patient expectations of the complaints system;
Analysis of complaints data is determined by availability of appropriate structures, availability of skilled staff to analyze complaints, and effectively communicate results to facility managers;
Action on the information include resolving the issue and responding to the complainant, using the information within health facilities.
Thematic analysis was used to synthesize results from qualitative and quantitative data sources, following the above three steps. The themes under each step included combinations of those determined a priori and those which emerged from the data. The patient feedback data from the publicly available web portal was analyzed using Microsoft Excel to explore the volume of patient feedback by years and types of feedback. Qualitative data from IDIs and observations were transcribed and analyzed manually.
Ethical approvals were obtained from the University of Leeds School of Medicine Research Ethics Committee (Ref MREC16-110) and Bangladesh Medical Research Council (Ref BMRC/NREC/2016-2019/164).
Results
The desk review has found that multiple systems are available in the country for patients to provide their feedback at the primary level. By nature, these systems are managed differently by various actors in the health system. A table summarizing the systems is presented below, and later each of the systems is described based on the three steps of patient feedback management.
As shown in Table 2, the feedback systems at the primary level of care fall into two broad categories where there are three centrally managed systems and two locally managed approaches. In the centrally managed systems, the issues raised, often alongside the actions taken, are documented and subsequently available. However, while the locally managed approaches also have mechanisms for reporting back to the patients, these do not typically have record-keeping processes. Each of the five systems is set out in more details next.
Patient Feedback Systems at the Upazila Level.

Note. GRS = Grievance Redress System; MOHFW = Ministry of Health and Family Welfare; DGHS = Directorate General of Health Services; MIS = Management Information System; SMS = short messaging service; UHC = Upazila Health Complex; UHFPO = Upazila Health and Family Planning Officer; NGO = Non-government Organization; UNO = Upazila Nirbahi Officer (Sub-district Executive Officer).
Government’s Grievance Redress System
In 2007 (revised in 2008), Government of Bangladesh established a Grievance Redress System (GRS), administered by the Cabinet Division, to facilitate quick action on grievances of the citizens, enhance the accountability of public officials and facilitate responsiveness to such complaints (GRS in Bangladesh, 2016). In 2011, the Cabinet Division designed and developed an online platform, and a total of 52 government ministries and agencies introduced GRS mechanism (GRS in Bangladesh, 2016).
Collection: Using this platform, anyone can use an online form to electronically submit their dissatisfaction or aggravation on the services or products, processes or unlawful acts related to expected/given services, and refusal to provide services to citizens by the government officials (www.grs.gov.bd). Citizens may include their name while providing feedback so the feedback can be traceable to them or may choose to remain anonymous. They can also attach documents and audio or video file in support of their complaints.
The submitted form goes to the grievance redress officer of the relevant government office, and the complainant is given a tracking number and information about the grievance redress officer. The redressal is to be done within 60 days of the complaint submission. Complainants can submit their complaints to specific cells under an office, in that case, the redressal time lessens to 30 days. Registered users can get details of their complaints and track the latest actions taken by logging anytime into the platform. They can also appeal if they are not satisfied with the actions finally taken. Also, they can rate the action taken and leave their comments after the redressal. For an anonymous complaint, the complainant is not given any tracking number or the information of the redress officer and therefore, cannot know about the progress of the redressal process. An anonymous complainant gets the warning of possibilities to get tracked down and punished in case if the complaint is submitted in the purpose of harassing someone. Also, any complainant proven guilty of harassment or providing misinformation can be blacklisted, and further cannot submit any complaint using the platform until removed from the blacklist.
Analysis and action: Respective ministry analyze the complains. Complainants in this system get SMS or email regarding the resolution status of their complaints. Through the GRS, grievances can be explicitly submitted to the MOHFW or any of the 52 ministries. Section 3 of the Citizen Charter of Health Service Division of MOHFW (www.mohfw.gov.bd) provides a list of designated personnel and the expected time to solve the issue with the contact detail of the personnel to be contacted at different stages of grievance redress process. The frequency and type of complaints against health services are not available publicly in this system, thus preventing us from providing a breakdown of the nature of grievances.
Our interviews with different stakeholders revealed that this system and its functions were unknown to many central level officers, local-level service providers, and the service users. Moreover, we did not find any evidence of promotion at the UHCs on this platform. Our observation at the facilities led us to assume that, even if people were aware of GRS online platform, the system would not be useful to many of the health seekers at Upazila level because of their limited access to computers and lack of internet literacy. From the stakeholder workshop, we found that a handful of high-level government officials were aware of the GRS platform; however, they could not share details of its management process.
MOHFW Complaints and Suggestion Box
Since 2012, the MOHFW has implemented a more direct GRS at the UHCs to enhance the voice of its service users through allowing them to provide feedback to a specific phone number using the short messaging service (SMS) (Naylor et al., 2013). Initially introduced by the Management Information System (MIS) unit of DGHS to monitor the presence and performance of health staffs, it has now become one of the most widely used patient feedback systems in the country covering service users of sub-district (Upazila), district and specialized public health care facilities. After launching the SMS service, the DGHS actively promoted the service to create local awareness, as one respondent reported: I had personally done that (instruction sent to the local level). I instructed every UHC to print these instructions of mobile number SMS and give it to every Chairman, officer and UNO office, and where there is public gathering. Also kept the signboard at the emergency section. We have instructed these by an official letter from MIS. That was in 2011. (Central level officer: 002)
However, we found no evidence of such promotion during the study, neither centrally nor locally, except the printed board (see Figure 1). The board was available at three UHCs out of the four containing same instructions and mobile number to send SMS directly to the MIS unit of DGHS in case of anyone having any complaint or advice. Thus, people who notice the board can send SMS using a mobile phone and convey their feedback.

Board promoting SMS complaint and suggestion box.
Collection: All SMS texts go into a publicly available web portal (http://app.dghs.gov.bd/complaintbox/?actn=lstmsg) containing issues that service users provided feedback on, dates of receipt of feedback and name of the health center.
Analysis: Once feedback is given, an MIS officer at the DGHS office located in the capital city of the country often sends a preformatted email to the UHC (or respective hospital) about the case.
Action: Each SMS received is subsequently followed-up by the MIS officer with phone calls to the patient and/or the local authority of the health facility that the feedback was about, and the solution posted on the web portal. However, when either party cannot be reached, an option in the portal shows that “Pending due to non-availability of authority/sender,” and the MIS officer requires further follow-up with the feedback. The other processing steps are based on the communications between central (MIS, DGHS) and local level (UHC), and subjective judgment of the designated officer handling the feedback. The following fields are there at the portal to be filled in by the MIS officer with predefined options such as Category, Rank, Type(s), Action and Solution. The options for each of this field available to the designated officer are presented below (Table 3). The officer has options to put comments about the message and respond to the sender by SMS from the portal. All of these become publicly available at the portal.
Steps and Options for MOHFW Complaint and Suggestion Box.

Note. MOHFW = Ministry of Health and Family Welfare; DGHS = Directorate General of Health Services.
An example of a complaint and response at the portal is given below:
Initially, during the data collection period, only one person was handling all feedback coming through this system. Gradually a team comprising of three members was formed to handle the processing and action on SMS complaints.
Over the last 8 years (2012–2019), the numbers of feedback sent through this system increased gradually, especially after 2016 (Figure 2). Most feedback received from all public health facilities via SMS service was for the negligence of responsibility (16.22%) followed by the absence of workforce (14.65%) and service (8.63%). Interestingly, the highest percentage of complaints were categorized as “Other” (20.24%)—a strong indication of the need to revise the categorization of the feedback. Also, 7.36% feedback marked as not traceable indicated the limitation of the system to resolve the feedback (Figure 3).

Number of SMS feedback each year.

SMS complaint types (2012–2019).
The use of SMS feedback system has been working as one of the quality indicators for assessing the performance of health facilities since 2014, and it bears a score against the minimum required number of SMSs sent from a health facility and the actual number of SMS sent in a month.
Health Call Center (16263)
Another patient feedback system is the “Health call center (16263),” namely “Shastho Batayon,” implemented by the MOHFW’s Directorate General of Health Service (DGHS) since April 2016.
Collection: Anyone can call this number to speak to a doctor for health consultation free-of-charge, information about an ambulance, lodge complaint against or advice for any public or private hospitals, inform about any accident, and seek information about hospitals, doctors, or health care. The DGHS promotes this service through different platforms, including public health facilities, electronic and print media, digital fairs, and formal reports. Initially, introduced to provide service information, this platform has now allowed the callers to lodge complaints against any health care center. One central level officer mentioned, This is an interesting thing that people are using the number of Sasthya Batayon for complaining, rather than the SMS number that we have provided them to do so. (Central level officer: 001)
Analysis and action: When someone lodges any complaint or provide advice using this number, that is sent to the MOHFW complaint and suggestion box by the call operator. The processing and action on the feedback follow, as mentioned above. However, all the complaints were not sent to the MIS as one of their officer mentioned: Sastho Batayon is a different platform. But those complaints there also comes to me. They send it to me. (Central level officer: 002)
Frequency of complaints to the call center is available publicly on an online dashboard (http://16263.dghs.gov.bd/report/report.php), and it increased over the years. The total number of calls and complaints received from 2016 to 2019 are presented in Figure 4. However, the types of complaints received were publicly available in a separate web portal (http://103.247.238.81/webportal/pages/shastho_batayon_only_complain.php) till 2018.
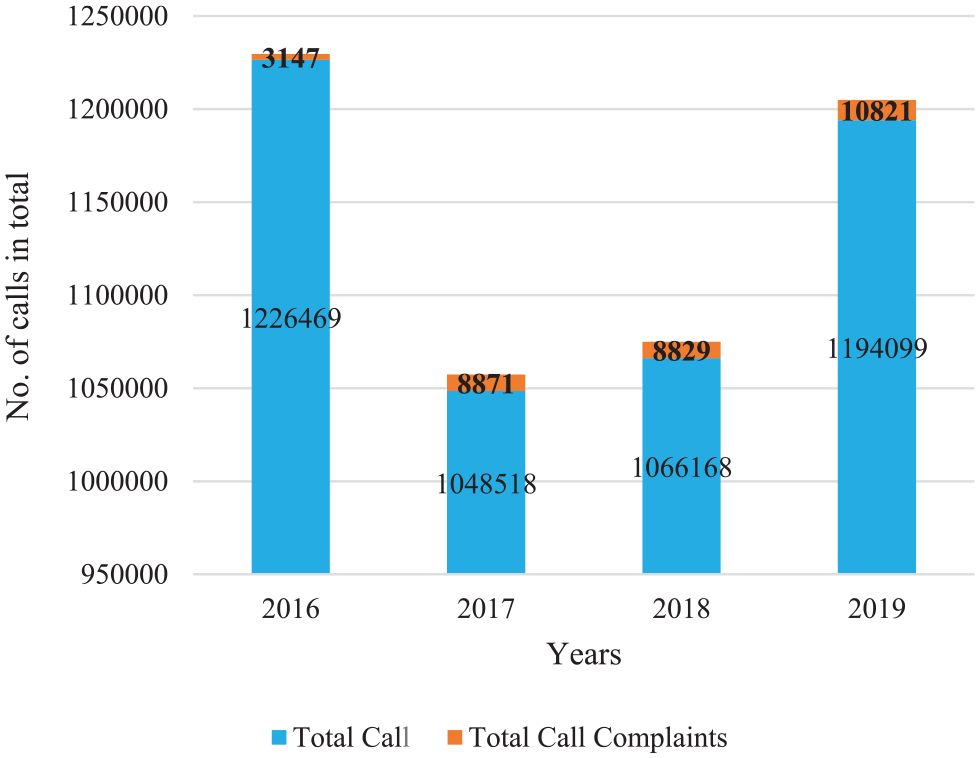
Number of calls and complaints via the health call center (2016–2019).
In contrast to the GRS and Complaint and Suggestion Box (SMS service), the health call center allows its users to share feedback on their experience in both public and private health facilities. Also, the promotion of the call center is visible in both electronic and print media. However, similar to the other two systems mentioned above, we did not observe any promotional message or activities at the UHCs during the period of data collection.
Two locally managed approaches to collecting feedback, written and verbal channels, are set out next.
Written Feedback
Collection: As described in Table 2 above, patients or their representatives can provide written feedback either through suggestion boxes or by writing to the UHC head or management committee. Suggestion boxes are usually placed on an outside wall of UHC.
Analysis: The UHC management committee comprises of approximately 21 members and is usually chaired by a local Member of Parliament. It includes Upazila Nirbahi Officer (Sub-district Executive Officer), Upazila Chairman, Vice Chairman, Upazila Health and Family Planning Officer (UHFPO), Resident Medical Officer (RMO), and several community representatives. Internal issues, problems, and needs of the health center, and decisions to solve these problems are discussed during the meetings.
Action: The meeting minutes are shared monthly with the Management Information System (MIS) unit of DGHS. The MIS then compiles the decisions taken by the facility and publishes them in a publicly available dashboard (dashboard.dghs.gov.bd/webportal/pages/hmc_meeting.php).
The written feedback is usually scarce at the UHCs. During our observation and later, interviews with the UHFPO, we found no physical evidence of any written complaint lodged by any service recipient: In my 11 years of service here, I never got any written complaint. (Provider: 003)
The complaint boxes were found in three UHCs out of four observed, and all of those were unlabelled, unused, and often misused as donation boxes of the waste bin (see Figure 5). Thus, there was no evidence of collecting any feedback using the complaint box.

Complaint box at one Upazila Health Complex.
Verbal Feedback
Many respondents felt that the provision of verbal feedback is the most frequently utilized channel. However, due to the absence of any documentation at UHCs of verbal feedback, this evidence remains anecdotal: The documentation of every complaint is not done here. SMSs which are sent are already documented. Verbal complaints made by patients are not documented. However, I think a system should be there which will allow to document the complaints regularly and discuss it. (Provider: 001)
Collection: Patients can provide feedback verbally either directly to the UHC staffs, UHFPO, or through the management committee. At the UHC, often feedback is received through the mobile numbers at the emergency section or in person.
Analysis and action: The UHC staffs or the doctors then try to resolve the issues locally, with the support from the UHFPO as appropriate. However, many service providers felt the need to start documenting complaints to deal with and escalate the issues to the proper authority, as one provider emphasized: “The benefit of record keeping is, if complaints are coming against a particular person repeatedly, it will be easier to take action against her/him. . . Based on these documents, it can be said, “All of these are because of patients’ complaints, here I have no role” (Provider: 004)
Thus, currently, the verbal feedback is either addressed immediately through counseling or remembered and discussed during the monthly meeting of the management committee at the UHCs. The processing and actions taken on the verbal feedback are not documented as well: We respond verbally. If there is any problem, we try to solve it promptly. We try to resolve the reason of the complaints, such as, problems in bed or problems in service or patient not getting the doctor or patient not getting medicine or doctor/staff behaved badly with the patient etc . . . In some cases, when we cannot resolve the problem locally, we counsel and assure the patient that we will try to resolve the issue as early as possible. (Provider: 001)
Still, the verbal feedback remains the first choice for many patients as presented by one of the patients at UHC: I think the verbal way is the best. If a man comes to the hospital and says, “I have a problem, I want to speak to the authority directly.,” then it is easy to solve. (Patient: 003)
Strengths and Weaknesses of Patient Feedback Systems
As multiple initiatives seek to manage patient feedback in Bangladesh, each system has its strengths and weaknesses, which are briefly set out next, followed by identification of key common issues across all feedback systems.
A key strength of the
On the other hand, the “ I am hearing about the SMS system just now. I did not know about it. (Provider: 004)
A reason might be the inappropriate installation of the single promotional instruction to inform about the system—the board with messages on it. One patient articulated this by saying: I think the board and the box failed to attract my attention. Those are probably not eye-catchy. (Patient: 001)
Such lack of awareness undoubtedly affects the collection of feedback. Also, lack of literacy of the service users at UHCs obstruct them using the SMS complaint system as evidenced by the following statement: It is difficult for them because most of them do not know reading or writing. Since we are rural people, we depend on agriculture. That is why everyone is not able to read. Thus it is not easy for them . . . I will put the SMS system in number three (ranking the options for giving feedback). (Patient: 004)
While awareness among users could boost up the utilization of SMS complaint system at the local level, guidelines could play a role in processing those. However, the scenario reflected from the provider side indicated otherwise: Actually, we do not have any guideline. . . If there were guidelines and the things on what to do regarding complaints were written there, I think that would bring some transparency in the process as there would be certain points. (Provider: 001)
In the context of having no clear policies or guidelines on SMS complaint management, including the recording of follow-up actions, the system is managed by a small team who are based in the MIS unit. In result, there is little clarity on the basis for decisions and steps in the processes of their decision-making. Earlier during the data collection period, a single person handled all the feedback followed own judgment and available options in the web dashboard to process any feedback: If you ask about the written guideline as I showed you the options (referring to online SMS system), that is a guideline . . . My guideline is the options in the software; I cannot go beyond that. (Central level officer: 002)
The lack of public awareness of the system and the absence of a clear guideline to process the feedback ultimately leads to non-structured analysis and uncoordinated actions on that feedback: We neither have any guideline nor policy. We do not have any particular policy, and we resolve any problem (by ourselves). We cannot solve a problem hundred per cent some of the issues we leave incomplete. (Provider: 005)
Therefore, at least three drawbacks of the SMS complaint system are notable: (a) dependency on a few persons at MOHFW to follow up on the issues received through SMS, (b) lack of operating guidelines or a manual for the feedback management system (e.g., to guide the assessment of “severity” of the complaint, and resolution of the issue), and (c) unavailability of written contact details of the person/s to be contacted at the local level.
Some service providers in our study felt that the The drawback of complaining at Sasthya Batayon is that these complaints are not being recorded, some are only digitally entered. So, in this case, as well, the real scenario is not coming to the central level. (Central level officer: 001)
Though the number to the health call center was observed to be promoted nationally more than the SMS complaint system, the awareness was still not enough at the local level (sub-district level) as proven by the response of a patient who said, As you mentioned that there were helpline phone numbers hung in health complexes if these are promoted, it will draw attention. (Patient: 006)
Thoughts of the providers also aligned with the experience of patients while commenting on the GRS, SMS complaint system and the health call center: People are not aware of these systems. That is because there has been no workshops or promotion on those. (Provider: 001)
Suggestion boxes are easier for providing written feedback; however, during observations, no readily available pens and paper were found for writing feedback which constrains the use of suggestion boxes. However, as per our observation, suggestion boxes are not used or promoted in UHCs which may be a reason for the reluctancy of the service users in providing written feedback. Another reason for not lodging any such feedback was perhaps because the patients were generally unaware of the suggestion boxes, as found from the statement below: In my experience, there is no system for providing complaint. I have never seen any complaint box or any other system here. (Patient: 001)
One service provider at UHC, however, presented different aspects to explain the unwillingness of patients to choose written feedback as an option: Patients do not want to give written complaints because of some reasons; one is that they may be illiterate. Secondly, they may think that it would be a time-consuming matter, thirdly they are happy if their purpose of coming to the health centre is fulfilled. (Provider: 003)
Therefore, written feedback was found to be the least preferable option by the service users comparative to all other systems. However, there were options to reach the local authority directly by both verbal and written complaints: They can complain about verbally. We have a managerial system; they can complain verbally or in written form to the management committee, basically to UHFPO . . . If UHFPO receives any complaint, he makes an investigation committee; the members would verify the complaint, follow the investigation rules and do the things they need to do. (Provider: 003)
The local authority at UHC works in the form of its management committee that provides a platform for MOHFW and Ministry of Local Government, Rural Development and Cooperatives (MOLGRD) to work together to address patient feedback and improve the service provision at the UHC. However, non-functionality of the committees, absence of the community representatives and local leaders in the meetings, inadequate resources and lack of authority of the committee to reward or punish health care providers for their performance remain significant constraints. A central-level policymaker reflected that: Practically, we know that the hospital management committees are not active that much . . . But this is a great tool for governance. (Central level officer: 001)
A local leader who was a member of the committee stated that: I am a member of some committees . . . But going to Upazila Health Complex for any meeting, I have been Chairman for about eight months; that never happened. (Local Leader: 001)
This lack of coordination between service users, service providers, and local leader naturally causes minimal, or no promotion of the provision of submitting written complaints at the UHCs. The reluctance of patients and the absence of coordination and guidance from the provider’s side toward written feedback can be a few of the reasons why patients preferred verbal feedback more than using other systems. A provider said, They think if they just verbally complain about something, the authority will take care of the rest. If the patients receive counselling or see that some immediate measurement has been taken, they would leave happily.
These findings explain the number of calls increasing over time more than the number of SMS used for complaints. Patients’ preference to convey their feedback on health services verbally rather than by writing also validates the need to explore more explicitly into the feedback mechanisms for the systems available in the country. We found that despite a high-level political commitment to improve patient feedback systems, there was no formal recording or process tracking system for verbal feedback in the UHCs. However, the introduction of health facility assessment under the health system strengthening initiative of MIS, DGHS to improve the quality of health service provision has the opportunity to introduce new mechanisms in the health centers to promote ideal feedback management systems.
Service providers also shared the view that patient feedback allows them to distinguish between good and bad clinical practices, helps patients get proper care and builds up a healthy relationship between service users and providers. These are exemplified in the two quotes below: By doing so, we will be benefited that patients can get proper treatment, they are getting hygiene and clean environment along with that we will not face any awkward situation while serving them . . . I mean, it would be helpful to upgrade the standards of health services. (Provider: 005) Of course, if we can inform the patients about the solution, they will be really happy thinking that their complaints led to some solutions. With being happy, he even will encourage his neighbours, thinking that here the problems are being solved and communicated well. It will improve the relationship between hospital and patients. (Provider: 001)
The table below summarizes the strengths and weakness of the patient feedback systems currently available at the Upazila level.
Available Systems for Patient Feedback at Upazila Level in Bangladesh.

Note. GRS = Grievance Redress System; MOHFW = Ministry of Health and Family Welfare; SMS = short messaging service; MIS = Management Information System; UHC = Upazila Health Complexe; UHFPO = Upazila Health and Family Planning Officer. Source: UNDP (2016).
Discussion
This paper documented and analyzed the current patient feedback systems available at primary health care level in Bangladesh. It was found that multiple systems are operating for managing patient feedback at UHC. These are not integrated and duplicate each other, but all are ultimately concerned with ensuring accountability of health facilities to patients’ needs. Each system has its strengths and weaknesses. Key strengths across all systems include common goals and political commitment to ensuring voice and accountability reflected in the introduction of different feedback channels and systems. In contrast, vital common weaknesses include a lack of documented processes and guidelines and limited patient awareness of available channels.
The high-level MOHFW political commitment to patient feedback systems is reflected in the Program Implementation Plan of the 4th health sector program (2017–2022) of Bangladesh with targets of 30% and 60% of total grievances to be adequately responded to by the years 2020 and 2022, respectively (“Programme Implementation Plan (PIP) of the Health, Nutrition and Population Sector Development Programme, 2017-2022,” n.d.). Currently, one indicator used to assess the performance of the UHC is “the grievance redress system is in place.” If the UHC receives at least five complaints per month, it gets the full score against this indicator. However, the assessment does not monitor solutions of received complaints, and the phone numbers used to send the feedback are not verified, ultimately making it susceptible to manipulation.
The widespread use of cell phones and internet technology in Bangladesh make online and SMS-based feedback channels accessible and affordable to larger groups of the population. This advantage coupled with clear instructions on how to provide feedback—for example, through the SMS instruction boards at UHCs—should further improve access to available feedback channels. Our study suggests that from the providers’ perspective, the processing and action on feedback depend much on the existing clear guidelines. However, other studies suggest that though the policies and guidelines are expected to accelerate the rate of action on received feedback, institutional culture, and communication skills of the providers acted as barriers to that (Adams et al., 2018; Allan et al., 2015). Therefore, while implementing any guideline to the health facilities, its existing values and practice must be taken into account to ensure proper utilization of the existing feedback systems.
Existence of a law or a policy for addressing complaints, transparent processes, and/or guidelines for handling complaints, along with the availability of competent staff, can also stimulate an open and transparent implementation of procedures for handling patient complaints, as shown elsewhere (Thi Thu Ha et al., 2015). Published evidence also suggests that establishing easy-to-use channels, developing standard operating procedures, flowcharts, policies and guidelines can help clear all stages of the feedback process from collection and through to managing and acting upon the information (Mirzoev & Kane, 2018; Rohwerder & Rao, 2015). In the absence of such policies and guidelines in Bangladesh, it is not clear who is responsible for managing feedback at different levels, which can lead to lack of organizational commitment and ultimately limited learning from patient feedback for service quality improvement and staff management.
The need for dedicated staff for handling grievances at all levels with adequate training on policies and procedures is widely acknowledged in the literature (“National Complaints Management Protocol for the Public Health Sector of South Africa,” 2013). On the other hand, literature also highlights that disproportionate resources are often consumed for a small number of complaints and the medico-legal claims process (Goldsmith et al., 2015). Staff dedicated to the patient feedback system in Bangladesh are minimal. At the central level, the SMS feedback system is maintained by a single person who manages feedback from the whole country, which raises questions of sustainability of the system.
The findings suggest that the numbers of SMS transmitted to the MOHFW are limited, and people are often unaware of their rights to provide feedback. Due to perceived low social status, many patients felt powerless to complain to the appropriate authority. An investigation of patients’ complaint handling processes in public hospitals in Vietnam showed similar findings where patients had also lacked the power to complain and inform change in the system (Thi Thu Ha et al., 2015).
A greater sense of community ownership of health facilities and facility management committees can promote active participation in decision-making by the elected community members. This will lead not only to better awareness among users of their rights to complain but also empower them to demand better services of their local facilities (Few et al., 2003). In Bangladesh, the existence of UHC management committee, CG and CSGs can provide excellent platforms for encouraging community engagement at community and Upazila levels. However, as shown earlier, management committees are not always functional, and greater involvement of the community with the patient feedback system needs innovative and effective promotional ways, such as involving local NGOs, civil society organizations and news media (Gauri, 2013).
Translating patients’ intentions to give feedback into an actual utilization of feedback channel requires a quick and easy medium. Many patients, particularly those with low levels of literacy, face challenges of writing an SMS on a mobile phone or on paper. Consequently, there is a clear preference for verbal communication regardless of whether the feedback is intended for local doctors, managers or the call center number. To adequately reach patients with low-literacy levels, health systems need to incorporate verbal alongside written feedback (King et al., 2010; Weingart et al., 2005).
From the provider’s side, there is a need to ensure that details of the feedback system and the possible actions and outcomes following complaints are communicated clearly to staff. This will ensure that staff and managers can respond to feedback constructively rather than feeling threatened by the system (Allsop & Jones, 2008; Dixon-Woods et al., 2012), and will help integrate information from patient feedback into effective service quality improvement processes.
Our analysis suggests different policy and practice implications for improving feedback management at public health facilities. Some have been highlighted throughout the discussion, and at this point, we would like to specifically emphasize three key issues. First, wider promotion of available user feedback systems and channels, coupled with efforts to make these channels more accessible and easier-to-use (e.g., combining verbal and written ways of providing feedback) should help improve the actual utilization of available feedback channels. Second, developing clear operational guidelines (including a detailed manual) for managing patient feedback within health facilities should help staff improve their practices of collecting, analyzing and acting upon the feedback. Third, improving the functionality of facility management committees and ensuring the availability of staff with knowledge and skills necessary for adequate documentation of feedback, should help ensure institutional learning from feedback within health facilities for service quality improvement.
Study Limitations
A key strength of this study is its pioneering nature in documenting different feedback management systems in Bangladesh. However, some limitations are acknowledged, which may represent areas for future research. First, the focus was only on two UHCs and given the pilot nature of many feedback management systems; other regions may have further examples. Second, comparing feedback management systems from PHC with the hospital sector would be a useful exercise in future research. However, the intention in this paper was not to be methodologically comprehensive, and the practice-oriented nature of this piece should inform the future debate on the relative merits of different patient feedback systems in LMICs.
Conclusion
Multiple systems are operating for managing patient feedback at primary health care in Bangladesh. These include three centrally managed and two locally managed approaches, each with its strengths and limitations. Three policy implications—facilitating the utilization of available feedback channels, improving staff practices of feedback management and ensuring institutional learning from patient feedback for service quality improvement—although directly targeting policymakers in Bangladesh, should also be relevant to many other contexts. Many underlying challenges in ensuring effective feedback management systems (such as limited awareness of service users, or lack of favorable policy environment which incentivises staff to address cases openly and transparently) are common to many LMICs and indeed many high-income settings (Thi Thu Ha et al., 2015). Therefore, the above policy implications arguably can also apply to many other similar contexts.
Footnotes
Acknowledgements
The authors are grateful to the Health Economics Unit of the Ministry of Health and Family Welfare, employees of the participating Upazila Health Complexes and patients who participated in the interviews for their invaluable contribution to this study.
Authors’ Note
Tolib Mirzoev is now affiliation to London School of Hygiene and Tropical Medicine, UK.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The RESPOND project “Creating responsive health systems: improving the use of feedback from service users in quality assurance and human resource management in Bangladesh,” from which this manuscript is written, was funded by the joint MRC/ESRC/Wellcome/DFID Health Systems Research Initiative, grant number MR/P004105/1.