
Abstract
The development of a country is strongly influenced by a higher smoking rate among the young population. Understanding knowledge and attitudes regarding smoking among young people lies at the heart of effective tobacco control policies. Bangladesh is a large, low-income country in South Asia with a high rate of youth smoking. As yet, however, little attention has been paid to knowledge and attitudes among rural youth. Face-to-face interviews were conducted with 385 youth males from the rural Mymensingh district of Bangladesh aged 15 to 24 were interviewed face-to-face. Univariate distribution (i.e., frequency analysis), bivariate analysis (i.e., Chi-square tests), and multivariate analysis (i.e., binary logistic regression model) were performed to determine the influence of knowledge and attitudes on youth male smoking. The percentage of youth smoking is 40.3 with knowledge and attitudes revealed as the more influential factors of smoking. For example, the chance of being a smoker with a satisfactory knowledge score is significantly lower than their counterparts (Odds ratio [OR]: 0.47 [0.30, 0.70]). Similarly, respondents with satisfactory attitudes scores have a significantly lower chance (OR: 0.40 [0.26, 0.61]) to be a smoker than those having an unsatisfactory score. This study exposes the influences of knowledge and attitudes among the youth toward smoking in rural parts of the Mymensingh district of Bangladesh. The findings and recommendations of this study will be more helpful to the authorities in revising the existing smoking policies accordingly to reduce and prevent youth smoking for the betterment of the country.
Introduction
Use of tobacco products is a preventable cause of death and diseases at all stages of life (Caplan et al., 2011; Sychareun et al., 2013; Tomson et al., 2003) and is responsible for around 7 million deaths globally each year (World Health Organization [WHO], 2021). Generally, all kinds of tobacco products are harmful, and all levels are unsafe of exposure to tobacco (WHO, 2020). Use of tobacco is a global epidemic among young people (United States, 2012; WHO, 2014). There is evidence which demonstrates that most people attempt their first cigarette before age 18 years and turn into daily smokers by adolescence. European studies suggest most start smoking before they are 18 and most become regular smokers in adulthood (Eurobarometer, 2015). In the United States, among regular smokers, about 90% began smoking at or before age 18 (Giovino, 2002; Johnston et al., 2019).
Bangladesh is a large country in South Asia. It has a population of 165 million and life expectancy is currently 72.59 years. In Bangladesh, 35.5% of its population of 37.8 million adults currently use tobacco (Bangladesh Bureau of Statistics, 2017). By gender, 45% of men smoke compared to just 1.5% of women (WHO, 2013), and cigarette/bidi smoking is the most common type of smoking among men.
There is a national tobacco control law that bans the sale of tobacco to under 18-year-olds, however, it was found that male university students started smoking at an average age of 17.8 years (Hossain et al., 2017). This scenario is quite similar throughout the country.
Studies show that the smoking status of people (especially youths) was largely influenced by their knowledge and attitudes toward smoking. (Ramezankhani et al., 2010). In China, for example, studies related to adolescent smoking showed that lower knowledge of adolescents regarding the harmful effects of smoking was largely associated with smoking among that group (Yan et al., 2014). In Iran, a study found that the lack of appropriate attitudes toward smoking was largely responsible for the smoking of students and those with less knowledge and inappropriate attitudes toward smoking were more likely to be smokers (Heydari et al., 2013). It is evident that exposure to anti-smoke intervention programs improved the knowledge and attitudes of adolescents regarding smoking (Chen et al., 2014; Tahlil et al., 2015) and reduced the behaviors of smoking globally (Sun et al., 2007). Hence, it is essential to understand smoking-related knowledge and attitudes of individuals in order to design better interventions.
Numerous studies conducted across the world focused on the knowledge and attitudes of some sections of the youth regarding smoking (e.g., Abou-Faddan & Ahmed, 2012; Abuelfoutoh et al., 2014; Demaio et al., 2014; Liu et al., 2019; Myint et al., 2019; Nakhostin-Roohi et al., 2013; Shalaby & Soliman, 2019; Tubachi et al., 2018; Xu et al., 2015). In Bangladesh, a study identified that the prevalence of smoking was 20.5% among the people in the age group between 18 and 90 from 2001 to 2003 (Flora et al., 2009). Another study conducted in 2006, showed that 53.6% of men aged between 15 and 59 years were smoking where the overall percentage of smoking was higher in poorer areas (59.8%) as compared to more wealthy areas (46.4%) (Khan et al., 2009). Findings of a study based on the data set from nine South and South-east Asian countries’ showed that, in 2007, smokers consisted of 60% of Bangladeshi men aged between 15 and 54 years, due to the positive influences of low level of education and existing poverty (Sreeramareddy et al., 2014). In Bangladesh, data from Global Youth Tobacco Survey 2007, pointed out that the smoking prevalence among boys who were attending grades 7 to 10 and aged 13 to 15 years was 12.3% while the total prevalence was 15.8% (Islam et al., 2016; Rahman et al., 2011). Considering male students, aged between 18 and 26 years, another study highlighted that the rate of smoking was 49.1% (Hossain et al., 2017).
Across the country, there is a general understanding that smoking can be started at a young age. However, the effects of knowledge and attitudes toward smoking are unknown. Furthermore, rural youth in Bangladesh lag behind their urban peers in terms of knowledge, attitude, information socioeconomic status and other related services. Therefore, smoking prevalence among young people may be higher than in urban areas. Under these circumstances along with the deficit of related studies, especially in the youth sector (i.e., aged 15–24 years) in rural areas we targeted to highlight the influence of knowledge and attitudes of youth aged 15 to 24 years toward smoking in Bangladesh. It is believed that this study will provide necessary information on knowledge and attitudes toward smoking among rural youth to facilitate the implementation of related programs and policies that are geared toward eradicating youth smoking.
Methods
Data
The study used primary data from the research project “Knowledge, awareness and practices among youth smokers in Trishal Upazila under the Mymensingh district: A micro-survey study,” funded by Jatiya Kabi Kazi Nazrul Islam University. The project data were collected from youth males between the ages of 15 and 24 (persons aged 15–24 are called the youth as defined by United Nations (1981) with the following two criteria of inclusion: (a) persons aged 15 to 24; and (b) male, from the rural areas of Trishal Upazila, Mymensingh district of Bangladesh from 25 November 2019 to 15 December 2019. Trishal Upazila is situated about 20 kilometers and about 90 km away from Mymensingh division and the capital Dhaka respectively. There is one municipality and 12 unions of that Upazila.
At 95% level of confidence (Z = 1.96) and 50% prevalence of youth smoking (p = .50; due to the unknown prevalence of youth smoking, 50% prevalence was considered), considering the margin of error is 5% (i.e., e = 0.05), then the equation for selecting sample size is:

Using the above formula, 384 to 385 was the required minimum sample size. A multi-stage sampling method was used to obtain the required number of sample. First, a union (Trishal Union) of Trishal Upazila and then five wards of this Union (namely, Ward 1, 2, 3, 8, and 9) were selected by simple random sampling method. Subsequently, data from 385 youth males from those selected wards were collected by systematic random sampling. By considering the total number of youth males in the selected areas (wards), obtained from the latest census report of Bangladesh for the year 2011 (Bangladesh Bureau of Statistics, 2015), the data were collected by interviewing one of every five youth males from each wards as selected. The breakdown of the total youth males interviewed as: 53 of 265 from Ward 1, 81 of 404 in Ward 2, 74 of 370 in Ward 3, 91 of 454 in Ward 8, and 86 of 432 in Ward 9. A well-designed questionnaire in Bengali (the national language of Bangladesh) providing information on demographic (current age, number of family members etc.), socioeconomic (education status, occupation status, monthly income etc.) and smoking-related (smoking status, smoking knowledge, smoking attitudes etc.) information was passed face-to-face to 385 male youths by trained interviewers. After being read the approval declaration form for the survey, the respondents were requested to give their consent verbally. In Bangladesh, smoking is generally severely restricted by religion (Islam) and the existing cultural environment (conservatives), where smoking among women is far from being considered. So, only youth males were considered for the project.
Outcome Variable
As the outcome variable, the current smoking status of the youth is considered which was dichotomized by considering 1 if a respondent is smoking for the 6 months preceding to the survey and 0 for not. Only smoking cigarette/bidi was considered in this study as there was no evidence of other forms of smoking such as e-cigarettes or water pipe etc.
Explanatory Variables
Previous literature has found that a range of knowledge and attitude characteristics are associated with the smoking status of youth (Al-Shami et al., 2018; Hamner & Stumpf, 2001; Liu et al., 2019; Nguyen et al., 2016; Swe & Bhardwaj, 2012) were included in the current study. The survey contained eight questions to test young people’s knowledge on general traditions of smoking and its health effects:
(1) Do you think smoking is bad for health?
(2) Do you think smoking puts someone at risk of chronic disease?
(3) Do you think smoking is harmful to non-smokers?
(4) Do you know that there is a law banning smoking in public places?
(5) Do you know about the age prohibition regarding the sale of tobacco products?
(6) Do you think a ban on cigarette advertisements can reduce smoking?
(7) Do you think raising taxes on tobacco products can reduce smoking?
(8) Do you think lessons about the harm of smoking can reduce smoking?
Each of the above questions had two possible answers: yes and no. The questionnaire on attitude comprised of 6 questions to evaluate attitudes regarding smoking:
(1) Where did you first hear about smoking?
(2) Which source(s) of information about the harmful effects of smoking do you have available? Both these questions had five alternatives: family; friends; advertisements; neighbors/relatives; and others
(3) What is the smoking status of parents? The alternatives are: only father: and none of them
(4) Which other family members are smokers? The alternatives are: brother; paternal/maternal grandfather; others; and none
(5) What is the smoking status of close friends? The alternatives are: some of them; all of them; and none of them
(6) Do you think quitting smoking is good for your health? The alternatives are: yes and no.
Knowledge and attitudes of the youth were summed up by transforming these into knowledge scores and attitude scores and were grouped into two levels, such as satisfactory and unsatisfactory, according to individual values. A satisfactory level was decided as a score of more than or equal to the median value and an unsatisfactory level was decided as a score of less than the median value.
Statistical Analysis
Based on the descriptive statistics of the research sample, the median split method was used applied to classify respondents into those with satisfactory or unsatisfactory knowledge and attitudes about smoking. To find out the differences in the percentage of smokers by above mentioned explanatory variables, Chi-square tests were used. All the variables significant at level p < .20 in the Chi-square tests were included in the regression analysis (Tareque et al., 2015). In the logistic regression analysis, multicollinearity was tested by using the standard errors for the regression coefficients. Numerical problems like multicollinearity among the explanatory variables can be determined as a standard error larger than 2.0 (Chan, 2004). In the present study, it was noted that no evidence of multicollinearity was found. Finally, a binary logistic regression model was applied to highlight the effects of knowledge and attitudes for the determination of the smoking status of the youth males. All the analysis is said to be statistically significant by considering p < .01. Sampling weights are not applied. All statistical analysis of this study was executed by using SPSS version 16.0 for Windows (SPSS Inc., Chicago, IL, USA).
Ethical Considerations
The current study is based on the project entitled “Knowledge, awareness and practices among youth smokers in Trishal Upazila under Mymensingh district: A micro-survey study,” approved and financially supported by the Jatiya Kabi Kazi Nazrul Islam University. At the first phase of the survey of the project, it is guaranteed that all the information gathered from the respondents will be kept confidential and the data will only be used for research purpose by using a consent statement highlighting voluntary participation in the study on knowledge, awareness and practices on youth smoking. A waiver of ethical approval, as the project had no minimal risk to the subjects, was granted by the ethics committee of the of Jatiya Kabi Kazi Nazrul Islam University. After reading the consent statement, respondents were requested to give their consent verbally. Also, written consent from the respondents was not allowed due to the reason that some of them might not be able to read or/and write, and thumb impression was also avoided as it is used mostly in formal activities like property transfer, voting system etc. and people are not aware the informal use of this, that collectively could resist the study respondents to participate to the interview, and consequently, the data collection process might be put at risk. Any identifying information from the dataset was excluded from this study.
Results
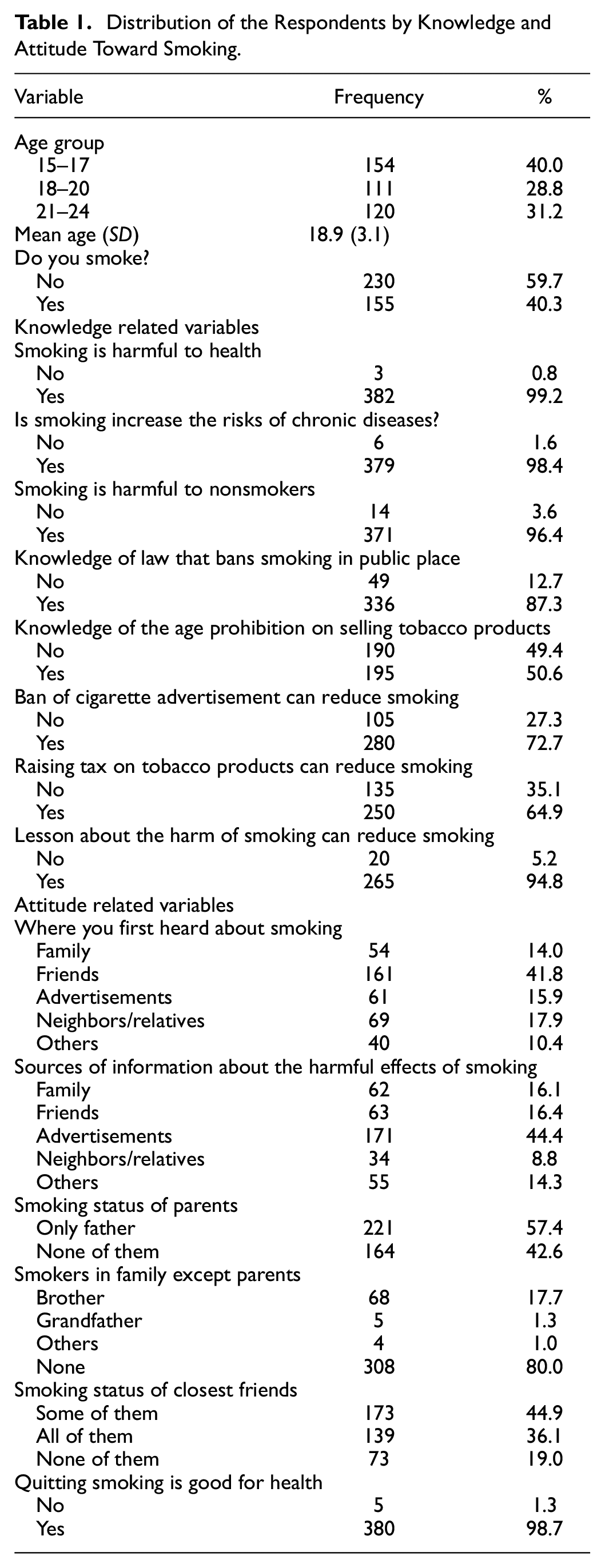
The overall status of knowledge and attitude of respondents regarding smoking were summarized in Table 1. The average age of the respondents was 18.9 years. Most of them were 15 to 17 years (40%), respondents aged 18 to 20 years consist of 28.8%, while 31.2% of respondents were aged from 21 to 24 years. Also, 40.3% of respondents were currently smoking cigarettes/bidi. Almost all the respondents (99.2%) thought that smoking is bad for health and it brings the risks of chronic diseases (98.4%) also it is similarly harmful to other nonsmokers (96.4%). A majority of respondents knew about the law of banning smoking in public places (87.3%). A total of 50.6% of the youths were aware of the age-limit on selling tobacco products. They also thought that a ban on cigarette advertisement (72.7%) and raising taxes on tobacco products (64.9%) could reduce smoking. Most of the respondents heard about smoking for the first time from their friends (41.8%), and advertising was the source of information about the harmfulness of smoking for the majority of the respondents (44.4%). A substantial percentage of the respondents’ fathers were smokers (57.4%), and 80% had no smokers in their family except their parents. About 81% of respondents’ intimate friends were smokers. Almost all the respondents thought that “quitting smoking is good for health” (98.7%).
Distribution of the Respondents by Knowledge and Attitude Toward Smoking.
The median knowledge score as shown in Table 2 was 7. The respondents with a knowledge score of ≥7 were classified as having satisfactory knowledge, while knowledge score of <7 were classified as unsatisfactory knowledge. Similarly, respondents have been categorized as having either a satisfactory or an unsatisfactory attitude based on the median of the attitude score (≥14 or <14, respectively).
Score of Knowledge and Attitudes Toward Smoking.

A significant difference was found in smoking knowledge level based on respondents (p = .000). The majority of respondents who possessed very less or no knowledge about smoking were unsatisfactory (51.7%) and turned into smokers afterwards, while the many of the respondents with satisfactory smoking knowledge (66.5%) could resist themselves and remained non-smokers even afterwards. There is also a significant difference between a satisfactory and an unsatisfactory attitude toward smoking (p = .00). Respondents with an unsatisfactory attitude toward smoking contains the highest proportion of those who turned into current smokers (51.6%) compared to a satisfactory level of attitudes. On the other hand, the percentage of respondents having satisfactory attitudes toward smoking is higher (70.0%) among current non-smokers as compared to the unsatisfactory attitudes level (Table 3).
Relationship Between Smoking Status with Knowledge and Attitudes Score.

Table 4 presented the results of the binary logistic regression model, yields the odds of being smokers by categories of the explanatory variables, that is, the knowledge and attitudes score. It was found that both the knowledge and attitudes scores have a significant effect on youth smoking. Respondents with a satisfactory knowledge score were 53% less likely to smoke as compared to those with an unsatisfactory knowledge score (odds ratio: 0.47 and 95% confidence interval: 0.30, 0.70). On the other hand, the likelihood of being a smoker was lower among the respondents with a satisfactory attitude score than those with an unsatisfactory attitude score (odds ratio: 0.40 and 95% confidence interval: 0.26, 0.61).
Influence of Knowledge and Attitudes Score on Youth Smoking.

Note. β = regression coefficient; CI = confidence interval; ® = reference category; SE = standard error.
Level of significance: ***p < .001.
Discussion
This study is based on documenting the state of knowledge and attitude about smoking and their relationship with the current status of youth smoking. To our knowledge, this is a large-scale study that exposes the influences of knowledge and attitudes of youth toward smoking in the rural Mymensingh district of Bangladesh. The findings of this study demonstrate that most of the respondents in the study area (40%) are in the age group 15 to 17 years and is cigarette/bidi smokers.
The findings of this study show similar findings from other previous studies about knowledge variables such as the health penalities of active and passive smoking (Al Mamun et al., 2018), smoking in public places (Sinha et al., 2008), the law of banning the sale of tobacco to minors (Abuelfoutoh et al., 2014), the banning of advertisements (Abuelfoutoh et al., 2014), an increase in taxes (Forster et al., 2007; Van Walbeek, 2005) and the lessons of negative effects of smoking (Bala et al., 2017; McVey & Stapleton, 2000). In short, measures concerning smoking reduction are well-known to smokers. The study also shows similar results as the previous literature regarding the attitudes variables such as the sources of information about smoking and the adverse effects of smoking (Myint et al., 2019), smokers in the family and friends (Al Moamary et al., 2012; Gupta et al., 2014; Myint et al., 2019), and quitting smoking is good for health (Xu et al., 2015).
This study also shows that despite the knowledge on the harmful effects of smoking, the youths go on with smoke, as in some other previous studies (Gupta et al., 2014; Tsering et al., 2008). In line with other studies (Dereje et al., 2014; Liu et al., 2019; Zhu et al., 2004), the study found that satisfactory knowledge about smoking was significantly associated with lower prevalence and a lower likelihood of being a smoker. Also, for attitudes, this study exhibits that a satisfactory score is also significantly associated with lower smoking rates and lower likelihood to be a smoker as shown in previous studies (Al-Shami et al., 2018; Liu et al., 2019; Myint et al., 2019). There is a need to raise awareness of the effects of smoking through different avenues recognizing that knowledge of the risks of smoking might be advantageous, but a broader understanding among youth needs to be improved (Nguyen et al., 2016). In this regard, a thorough understanding of the causes of youth smoking is important to facilitate the implementation of programs and policies aimed at reducing or accelerating the quitting of youth smoking.
Conclusion
In sum, this study investigated the knowledge and attitudes of smoking among male youths in rural parts of the Mymensingh district. As it is observed from the discussion, youths with satisfactory knowledge and attitudes are less likely to be smokers. Also, many youths with unsatisfactory knowledge and attitudes are found to be smokers. This points out that there is a lack of active enforcement and effective awareness of the injurious effects of smoking. The results of this study may assist health educators, policymakers and researchers to better understand smoking among youths and help in developing more efficient tobacco education intervention programming, which could lead to reducing or preventing youth smoking in the country. Appropriate authorities may take the following recommendations for the prevention of youth smoking: (a) the tobacco product law along with the economic and health vulnerability should be provided as a part of the school curriculum, (b) awareness about the vulnerable effects and consequences of smoking for youth and their families should be provided by the educational institutions and mass media, and (c) strict enforcement of the smoking law in public places is essential. The evidence provided in this study can be an initial step in eradicating and controlling smoking among youths.
Limitations
There are some limitations in this study. Due to the cross-sectional nature of our survey, it is not possible here to make a direct link between the explanatory variables and the outcome variable. This study only reflects the knowledge and attitudes of the youth population from rural Mymensingh district, and it may not be generalized to all Bangladeshi male youths.
Footnotes
Author Note
This research was conducted while Stuart Gietel-Basten was at Khalifa University while on research leave from the Hong Kong University of Science at Technology. He is are now at the Hong Kong University of Science and Technology and may be contacted at
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current study is based on the project titled “Knowledge, awareness and practices among youth smokers in Trishal Upazila under Mymensingh district: A micro-survey study,” approved and funded by the Research and Extension Center, Jatiya Kabi Kazi Nazrul Islam University (JKKNIU), Bangladesh.
Ethical Approval
A waiver of ethical approval, as the project had no minimal risk to the subjects was granted by the ethics committee of the Research and Extension Center, JKKNIU. The letter detailing this is available on request.