
Abstract
The efficacy of high fidelity patient simulation (HFPS) over low fidelity patient manikins (LFPM) in improving learning outcomes among undergraduate nursing students in Malaysia remains unknown. The aim of this study is to compare learning outcomes (knowledge and critical thinking skills) using an adult code blue drill simulated program using HFPS versus LFPM among undergraduate nursing students in Malaysia. In an experimental study, final-year undergraduate nursing students (N = 407) from three centers in Malaysia were trained in code blue management and assigned to either control (LFPM) or intervention (HFPS) group. Pre- and post-test assessment was conducted using 30-single best answer questions and the California Critical Thinking Disposition Inventory. A repeated-measures analysis of covariance (ANCOVA) showed significant differences in knowledge levels (intervention, η2 = 0.146; control, η2 = 0.130) and critical thinking skills (intervention, η2 = 0.119; control, η2 = 0.066). Simulation-based education using HFPS is advantageous over LFPM in increasing knowledge and critical thinking skills in code blue management among nursing students.
Keywords
Introduction
High fidelity patient simulation (HFPS) with simulation-based education is an effective skill learning tool that links classroom learning to real-life clinical experience for novice nursing students (Adamson, 2015; Adib-Hajbaghery & Sharifi, 2017). It is a form of experiential learning designed to promote patient safety (Cant & Cooper, 2017). HFPS simulates realistic clinical situations (Adamson, 2015; Cant & Cooper, 2017; Jeffries, 2012) and prepares students for clinical tasks with no risk to the safety of actual patients as opposed to low fidelity patient manikins (LFPM) (Adamson, 2015; K. S. Dunn, 2017; Jeffries, 2012; Kaddoura et al., 2016; Mauro et al., 2017; Richardson & Claman, 2014).
The combination of knowledge with the critical thinking (CT) skills has been found to increase the quality of registered staff nurse response in carrying out prompt, professional nursing tasks, and improved patient care (Chiang & Chan, 2014; Kaddoura et al., 2017; Nursing and Midwifery Board of Ireland, 2015; Simpson & Courtney, 2002; Weatherspoon et al., 2015). The Consensus Statement of Scheffer and Rubenfeld (2000) conducted in nine countries, including Brazil, Canada, Iceland, The Netherlands, England, Thailand, Korea, Japan, and 23 states in the United States, concluded that affective and cognitive components were important in CT of nursing.
Clinical skills are essential component in nursing education, consisting of 50% of the nursing curriculum (Nursing Board Malaysia, 2018). Clinical reasoning is an important component of competence in nursing practice; thus, students exposed to HFPS were found to have increased CT abilities when compared with students with no prior HFPS exposure (Adib-Hajbaghery & Sharifi, 2017; Chiang, & Chan, 2014; Weatherspoon et al., 2015).
To the knowledge of the authors, there is limited published literature relevant to nursing education in Malaysia (Isa & Saiboon, 2020; Ismail et al., 2019). There is even lesser evidence evaluating the effectiveness of simulation-based education (code blue management) and learning outcomes (knowledge and CT) for nursing students (Isa & Saiboon, 2020; Ismail et al., 2019). There is therefore a need to evaluate HFPS implementation in the Malaysian setting to allow objective achievement and evaluation of the learning outcomes.
This study is therefore novel given the country context. In addition, instruments used in the previous studies may not be suitable for the nursing students undergoing the rigors of clinical training in this country context as the aforesaid instruments have not been subjected to validation like the California Critical Thinking Disposition Inventory (CCTDI) in this study. We thereby sought to determine the effectiveness of HFPS compared with LFPM in increasing knowledge and CT skills using an adult code blue drill simulated program among final-year nursing students in Malaysia.
Method
Study Design and Participants
This multicenter, experimental, pretest–posttest double-arm intervention study used universal sampling to recruit all third-year diploma-nursing students (N = 409) from three public- and private-sector nursing schools. The syllabus of these nursing schools is regulated by the Nursing Board of Malaysia, Ministry of Education. Recruited participants enrolled in the diploma of nursing program in participating universities/institutions were standardized. Inclusion criteria were completion of the following courses: theory for anatomy and physiology, fundamental in nursing, communication skills, psychology and sociology in nursing, pharmacology, disorders in fluids and electrolytes, and cardiovascular and respiratory management. Completion of clinical postings for medical and surgical was an inclusion criteria. Nursing institutions that did not have HFPS during the recruiting period were excluded, as were students who deferred or did not complete clinical postings. Nursing students who did provide consent were randomized into either intervention (HFPS) or control (LFPM) group.
Study Setting
Written approval was obtained from all participants and participating schools. Ethical approval was obtained from the Medical Ethics Committee, University of Malaya (No. 956.67). Invitation letters were sent to the administrators of each of the nine eligible schools using HFPS in their nursing program; however, only three schools agreed to participate. Both verbal and written consents were obtained from individual participants.
Procedure
All participants were given the 30-single best answer (SBA) questions, demographic questions, and CCTDI questionnaires to complete pretest. These students were briefed on the environment, availability of equipment, role of each participating student, and a written case scenario. The researcher then delivered a presentation on code blue management for 40 min. Code blue management refers to the management of a cardiopulmonary emergency. In this study context, the code blue scenario was used to assess the participants’ knowledge of airway management, cardiopulmonary resuscitation, administration of medication, identification of life-threatening arrhythmias, and team collaboration on a deteriorating patient. Randomization was conducted by assigning the participants to control and experimental situation using a spreadsheet and systematic random sampling.
Students participating in the study were evaluated for both theory and practical sessions for a code blue situation. The control groups only used the LFPM before and after the study (pretest and posttest). Both groups (control and intervention) were measured at baseline pretest. For both groups, the environment of the code blue drill simulated program was set and arranged in a similar manner except for the control groups with LFPM while the intervention groups were exposed to HFPS posttest. For the control groups using LFPM, feedback was given after the practical sessions without need for video recording.
Participants from the intervention groups were informed that video recording was part of the teaching–learning process. Sample size difference between control and intervention groups was due to withdrawal of students from the control group.
At posttest, each set of questionnaires (except for the 30-SBA questions) was again administered to both control and intervention groups after practical session; 30-SBA questions were assessed 2 months later. Both students and assessors were blinded during the practical sessions. Students and assessors alike were informed of whether they were assigned to control or intervention group before the start of the practical session on the same day. All students and assessors underwent the same briefing at baseline pretest. After completion of pretest for both groups, a session on the theory of code blue management was delivered by the researcher. Students and assessors were not informed at pretest whether they would be chosen in the intervention of HFPS. All students and assessors were informed before the start of the practical session for posttest whether they used LFPM or HFPS on the same day. The practical sessions for control and intervention groups were conducted concurrently in the skills laboratory at pre- and posttest, and it took 10 min to run a single group (see Figure 1).
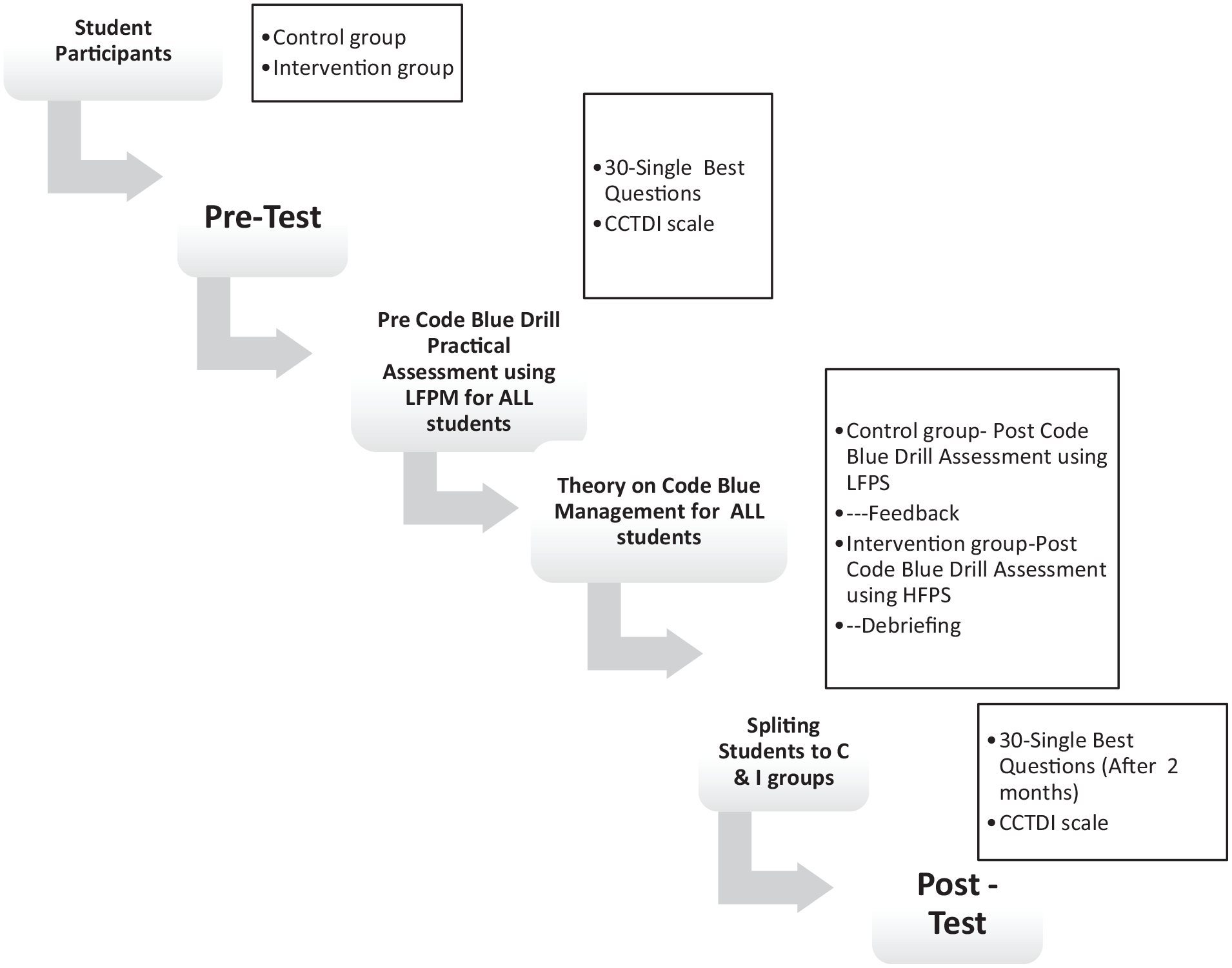
Flowchart on HFPS and LFPM (pretest and posttest).
Two assessors evaluated the practical sessions using a standardized checklist to monitor students’ skills performance during a code blue situation. These assessors made their observations independently for 10 min based on the standardized checklist and subsequently arrived at a consensus on the final scores for each subgroup (five students each). The computer screen in the simulation training displayed changes in vital signs including electrocardiogram wave, pulse rate, blood pressure, respiratory rate, and oxygen saturation. The debriefing session was conducted immediately after the practical session. For the HFPS group, the video recorded was replayed on the screen for students’ reflection on their own performance during the code blue practical session. Control group received feedback without video recordings.
Instruments
The 30-SBA questions and 75-item licensed CCTDI were reviewed by a panel of experts. These self-administered 30-SBA questions and licensed CCTDI items went through forward and backward translation from English to Bahasa Malaysia to provide bilingual options for local diploma-nursing students from public and private universities. Test and retest for 30-SBA questions were also performed with a reliability of .770.
The 30-SBA questions have a maximum total score of 30 marks, comprising of determining responsiveness (one item), airway management (seven items), breathing (six items), circulation (six items), drug management (five items), defibrillation management (four items), and team collaboration (one item). Each correct answer was accorded one mark. The total score for knowledge was recoded using rubric scoring.
The CCTDI has undergone many revisions (P. A. Facione, 2015; Insight Assessment, 2015) and it has been translated into many languages for use in many research studies on the CT disposition among nurses and nursing students (Hwang et al., 2010; Insight Assessment, 2015). The CCTDI has a total of 75 items, which measure the creative and CT style of students. These are seven subscales in CCTDI, including Truth-Seeking (TS; 12 items), Open-Mindedness (OM; 12 items), Analyticity (AN; 11 items), Systematicity (SYS; 11 items), Confidence in Reasoning (CR; 9 items), Inquisitiveness (IN; 10 items), and Maturity of Judgment (MJ; 10 items). Each scale score describes an aspect of overall disposition toward using one’s CT to form judgments about what to believe or what to do. Individuals may be positively, ambivalently, or negatively disposed on each of the seven aspects of overall disposition toward CT with the total score ranging from 70 to 420.
Pre-test 30-SBA questions and the 75 CCTDI items were distributed to all students prior to a lecture on managing a deteriorating patient. Post-test CCTDI questions were administered immediately post-HFPS, and the posttest for 30-SBA questions was answered by all students after 2 months.
Statistical Analysis
Statistical Package for the Social Sciences (SPSS; Version 21) software was used for analysis of covariance (ANCOVA) to test the main effects and interactions between categorical and continuous dependent variables and was controlled for covariate variables in seven demographic characteristics. Odds ratio and confidence intervals were used to test the effectiveness of posttest on knowledge after 2 months. The Pearson correlation test was also used to test the association between knowledge and CT.
Results
Of 409 eligible student nurses, a total of 389 students voluntarily participated in this study. Twenty students were excluded from the study due to incomplete post-test practical assessment and for their absence on the day of the study. The overall total response rate was 95%.
Approximately two thirds of the participants in this study were 20 years old (n = 259, 67%). Majority were female students (n = 359, 92%) while only 30 (8.0%) were male students. Based on the standard entry qualification for diploma in nursing in Malaysia, 98% of the participants (n = 384) had a GCE O-level CGPA (General Certificate of Education or pre-university Cumulative Grade Point Average) between 3 and 3.5. Students were assigned to control (n = 180, 46%) or intervention (n = 209, 54%) group. Notably, 40% of the students (n = 155) reported prior simulation training, while 60% of the students (n = 234) reported no previous exposure to HFPS. The various roles assigned in practical sessions were evenly distributed (Table 1).
Characteristics of Participants in Control and Intervention Groups (N = 389).

Note. Control group = no intervention; Intervention group = exposed to HFPS. CGPA = Cumulative Grade Point Average; HFPS = high fidelity patient simulation.
p < .005 considered significant.
There was a significant difference between pretest versus posttest for both control and intervention groups on airway management, breathing, circulation, defibrillation, and team collaboration (p < .001; Table 2).
Mean Score of Seven Knowledge Domains in Code Blue Management for Intervention and Control Groups at Pre- and Post-Exposure to High Fidelity Patient Simulation (N = 389).

p < .001 considered significant.
Drug management was also statistically significant for the intervention group compared with the control group post-exposure, while it was not significant for any group in determining non-responsiveness. There was marked improvement in intervention group compared with the control group on mean score percentage (posttest vs. pretest) for breathing, circulation, drug management, defibrillation, and collaboration (Table 3). The magnitude of differences in mean total knowledge score at pre-exposure phase and post-exposure phase after 2 months was statistically significant as indicated by a higher eta square in the intervention group compared with the control group (η2 = 0.130, p < .001), even after adjusting for age, gender, and CGPA.
Mean Score Percentage Difference of Seven Knowledge Domains in Code Blue Management for Intervention and Control Groups at Pre- and Post-Exposure to High Fidelity Patient Simulation (N = 389).

Note. Positive percentage = improvement for intervention group versus control group; Negative percentage = decrement for intervention group versus control group.
A repeated-measures ANCOVA showed significant differences in knowledge levels (intervention, η2 = 0.146; control, η2 = 0.130) and CT skills (intervention, η2 = 0.119; control, η2 = 0.066), controlled by age, gender, and CGPA. The power of test was 85.5%. There was a significant difference in total mean for (post–pre) exposure between control and intervention groups. The reduction in scores was found for OM, IN, AN, SYS, CR, and MJ for both control and intervention groups. The post-test and pre-test difference was statistically significant between both control and intervention groups for IN (p = .001), AN (p = .001), and MJ (p = .001). The CCTDI subscale attributes decreased after posttest for all attributes, but TS showed an increment (Table 4).
Total Mean Score for Critical Thinking Skills in Control and Intervention Groups Pre- and Post-Exposure to HFPS.

Note. HFPS = high fidelity patient simulation; CI = confidence interval.
Statistically significant, p < .005.
Table 5 shows the statistically significant correlation between seven knowledge components and CT skills at pre-exposure to HFPS. CT skill scores for both intervention and control groups were significantly improved and were found to be higher in the intervention group (η2 = 0.119) compared with the control group (η2 = 0.066, p = .005), even after controlling for age, gender, and education. Out of the seven domains in knowledge, total scores of circulation domain alone were associated with total CCTDI scores at both pre-exposure stage (r = .114, p ≤ .005) and post-exposure stage (r = .115, p =.005).
Correlation Between Seven Knowledge Domains and Critical Thinking Skill Scores at Pre-Exposure to High Fidelity Patient Simulation (N = 389).

Correlation is significant at the .05 level (two-tailed). **Correlation is significant at the .01 level (two-tailed).
Discussion
This study showed the influence of demographic characteristics on student knowledge and its retention. Findings were in line with prior studies demonstrating higher knowledge retention rates using the HFPS compared with LFPM approach (Cant & Cooper, 2017; Livne, 2019; Tawalbeh & Tubaishat, 2014).
Knowledge scores for both intervention and control groups were significantly improved after 2 months. However, knowledge gain was reflected in the higher post-test scores for the intervention group, similar to past studies (Adamson, 2015; Cant & Cooper, 2017; Livne, 2019).
In this study, students aged 21 and above as well as with prior experience in using HFPS had better knowledge test scores. Students with more experience are generally able to perform better in simulations, through integration of clinical experience, past simulation, and their ability to work in teams to readily manage the given scenario (Chmil et al., 2015; Najar et al., 2015).
Our findings also indicated that most demographic characteristics except for gender had no association with the CCTDI test scores (Cazzell & Anderson, 2016; N. C. Facione & Facione, 2014). Male nurses comprised only 8% of the participants in this study, reflective of the current nursing employment in Malaysia. This is consistent with past studies, which found a greater female preponderance in nursing (Tanner, 2015; Zamanzadeh et al., 2013). These findings reinforce the concept that CT disposition is an independent trait that does not rely on general personal characteristics. Research reported that work experience had no relationship with nursing students’ mean score or subscale scores (D. L. Dunn et al., 2002).
In this study, we found that scores for CT declined for both intervention and control groups posttest. Apart from the confidence scale, it is unusual to see lower post-test scores for the CCTDI. Hence, our study findings differed those reported from past studies (Kaddoura et al., 2016). Gains in CT skills have not been found to be statistically significant in pre–post study in non-English-speaking Asian countries such as in Japan (Adib-Hajbaghery & Sharifi, 2017), Korea (Adib-Hajbaghery & Sharifi, 2017; Kim et al., 2014), Taiwan (Hwang et al., 2010), and Hong Kong (Chiang & Chan, 2014; Shinnick & Woo, 2013). One possible reason for such difference in the findings between Eastern and Western countries on CCTDI scores may be attributable to the mode of thinking, social customs, and beliefs implied in this test (Chiang & Chan, 2014).
CT skills require personal awareness, willingness to accept challenges, and personal traits, taking six stages for developing the CT ability over time. A significant reduction in CT skills in this study suggests that further research and a longer period of posttest in phases are necessary. The current Malaysian education system is examination-oriented and thus does not require much CT (Abidina et al., 2020; Khairy et al., 2018). According to D. L. Dunn et al. (2002) reported increases in CCTDI scores from sophomore to junior years of baccalaureate nursing program, although significant reduction in CCTDI scores were seen from junior to senior year. However, other research (P. A. Facione, 2014, 2015) suggests that increases in subscale scores and total score are possible but that overall disposition toward CT appears to be stable over years. CT is best developed through repeated exposure to practice where learners’ thinking processes are supported by integrated contextual knowledge, skills, and behaviors (Facione, 2015; Park et al., 2012).
Interestingly, our findings indicate that the TS scores increased for both control and intervention groups. It has been reported specifically that TS is the most difficult to improve in CCTDI (D. L. Dunn et al., 2002; Kaddoura et al., 2016; Noone & Seery, 2018). Despite reduction in the mean score for overall disposition and subscale scores, the study further reported an improvement in TS subscale of CCTDI, similar to the findings by Weatherspoon et al. (2015) on TS as the student’s desire for best knowledge even if such knowledge fails to support or undermines his or her own beliefs, preconceptions, or self-interests. Educators are recommended to facilitate this attribute with role modeling to seek the truth. There is a need to integrate simulation-based education in the nursing curriculum as a learning process for nurses to improve their reasoning behavior.
There was no significant correlation between the level of knowledge and critical skills for the intervention group at pre-exposure phase and post-exposure phase. Nonetheless, CT caused a significant reduction in the mean score for overall disposition and subscale scores at post-exposure stage of HFPS.
One significant finding of this study was that the intervention group using the HFPS appeared to be more effective in facilitating practical code blue learning compared with the use of LFPM in the control group.
Age and experience in HFPS significantly influenced knowledge at pre–post exposure to HFPS after 2 months even though other demographic characteristics were not significant for CT skills. This finding implies that older age and experience in HFPS increased preparation and readiness, explaining higher knowledge scores (Cant & Cooper, 2017; Fisher & King, 2013; Noone & Seery, 2018).
Implications for Nursing Education
This study provides evidence for the effectiveness of HFPS in code blue management. High fidelity simulation training should be introduced in nursing programs to achieve specific learning outcomes, tailored to different levels of students to prepare them for collaborative teamwork to deliver safe and effective clinical care. Nurses’ knowledge and CT skills are important for the development of reasoned behavior in managing unpredictable code blue situations. Nurses need to work in tandem with interprofessional health care teams and should accordingly possess the skills to respond in a timely manner and make accurate decisions.
Simulation-based education is a teaching strategy, which facilitates the education of safe practitioners with repeated simulation practice to achieve clinical competency among students by acknowledging self-strengths and limitations through debriefing sessions. Nurse educators should provide innovative teaching strategies to cater learners’ background (age, gender, level of study, academic performance, and experience in simulation-based education). Written guidelines and training are recommended for faculty members to enhance teaching and learning process objectively (Mahat et al., 2018). Indeed, simulation-based education is another specialized area of training, research, and development for nursing to achieve best practice recommendations.
Limitations
The study was limited to students in third year of the Diploma in Nursing program. This does not allow generalization of findings on simulation-based education for drawing stronger evidence-based data through qualitative and retrospective studies. It is of course possible to use the LFPM to attain similar student learning outcomes as with the HFPS. However, the use of the latter simulates real-life medical scenarios more closely compared with traditional modalities and LFPM, offering a distinct advantage in this respect. The cost efficacy of implementing HFPS should thereby be weighted when considering its use.
Conclusion
Simulation-based education using HFPS appears to increase the knowledge and CT skills among nursing students in terms of code blue management. CT levels were found to decrease in overall for both intervention and control groups at posttest. The TS subscale appeared to increase in the posttest. HFPS can help in fostering positive learning outcomes among nursing students without replacing hands-on clinical experience.
Footnotes
Acknowledgements
We would like to extend our appreciation to Professor Dr. Pamela Jeffries for permission to use her questionnaire—Simulation Design Scale (SDS) and Educational Practice Scale for Simulation (EPSS)—on satisfaction and to the School of Nursing, University Malaya Medical Center, Nilai University, Malaysia, Universiti Technologi Mara, Malaysia, Laerdal Malaysia (IT support and simulator Sim Man 3G) and IDS Medical Systems (M) Sdn. Bhd (IT support and simulator Meti Man).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Universiti Malaya (UM), Malaysia (Grant Number: PG127-2012B) and Universiti Tunku Abdul Rahman (UTAR), Malaysia (Grant Number: UTARRF 6200/F05). The author (C.M.H.C.) acknowledges support from Universiti Kebangsaan Malaysia (Grant Number DIP-2018-035).