
Abstract
The purpose of this study was to investigate the personal, interpersonal, and organizational factors associated with cardiovascular disease (CVD) prevention behavior among office workers using an ecological model. A total of 221 office workers working in areas such as personnel, design, and accounting, and who work in offices, completed the survey. Health Perception Questionnaire, General Self-Efficacy Scale (GSE), Multidimensional Scale of Perceived Social Support (MSPSS) Scale, the Korean Occupational Stress Scale–Short Form (KOSS-SF), and Social Environment Influencing Health form were used to measure each factor. Health perception (β = .207, p = .003), family support (β = .185, p = .005), and organizational health culture (β = .175, p = .012) were found to have a significant association with the CVD prevention behaviors of office workers. Comprehensive and multidimensional intervention is essential to enhance the CVD prevention behaviors of office workers. This study informs the development of a workplace-based intervention program to prevent CVD among office workers.
Introduction
Cardiovascular disease (CVD) is one of the leading causes of death, accounting for 15.2 million deaths worldwide in 2016 (World Health Organization, 2018). In Korea, after cancer, CVD is the second leading cause of death, with an increase of 34.4% from 10 years ago, and its prevention among office workers has become important (Statistics Korea, 2019). For office workers, heavy work, lack of leisure time, conflicts with seniors and coworkers in the office, and frequent overtime lead to CVD through fatigue, depression, and stress (Rose et al., 2017). In addition, working long hours leads to a lack of physical activity and a higher chance of CVDs (Jeong et al., 2013). Thus, office workers face more psychosocial needs than blue-collar workers, who have many physical needs (Schreuder et al., 2008). CVD in office workers can cause a social burden because it leads to a decrease in the productivity of enterprises (Choi & June, 2005). Thus, it is important to identify the causes of CVD in office workers and prevent its occurrence by increasing their health promotion behaviors.
In previous studies, occupational factors, such as long working hours and long periods of sedentary work, and lifestyle factors, such as inadequate dietary habits, excessive drinking, smoking, and lack of exercise, leading to hypertension, dyslipidemia, diabetes, and obesity, were found to adversely affect workers’ cardiovascular health (E. K. Lee & Kim, 2013; Wilmot et al., 2012; Yoon, 2016). Korean workers have the third highest average annual working hours among the Organisation for Economic Cooperation and Development (OECD, 2017) countries, and they also tend to have poor eating habits, high rates of smoking and drinking, and low physical activity (J. H. Kim & Sakong, 2007).
Appropriate changes in the social environment lead to changes in the health behavior of individuals and this support is essential (McLeroy et al., 1988). The interaction of factors on different levels influences health behaviors and this underlines the need to take into account multilevel variables to understand and change individuals’ health (Sallis et al., 2008). However, most of the studies that have examined the factors affecting CVD in office workers have concentrated on identifying job characteristics, lifestyle, and socioeconomic status in an isolated, fragmentary manner, and have not comprehensively explored other dimensions, such as interpersonal, organizational, and community aspects.
The ecological model focuses on personal, social, and environmental factors as a strategy for promoting health and addresses the importance of interpersonal relationships, organizational factors, community support, and public policies in promoting changes in health-related behaviors (McLeroy et al., 1988). The ecological model can be used for implementing programs that promote healthy lifestyles. For example, Ryu et al. (2020) developed a workplace health promotion program for office workers based on the ecological model using multidimensional factors, including personal (e.g., managing stress), interpersonal (enhancing social support), and organizational (building organizational health culture) levels.
This study used the ecological approach to identify the factors leading to CVD in office workers and the health behaviors that can prevent it. The personal factors in the ecological model are the individual characteristics that influence behavior, such as knowledge, attitudes, beliefs, and temperament (McLeroy et al., 1988). In this study, health perception and self-efficacy were selected to represent the personal factors. Health perception is a subjective assessment of health status (Ware, 1979); that is, how workers perceive and experience their own state of health can affect their health promotion behaviors. Self-efficacy, which is an individual’s belief in their ability to organize and sustain the activities needed to achieve their goals, also has a significant effect on health behaviors (Bandura, 1977). As an important psychosocial component, self-efficacy can directly and indirectly influence health behaviors to control disease (Isa et al., 2018). Furthermore, recognizing and changing health risks can lead to increased healthy behaviors (Ferrer & Klein, 2015). In terms of the personal factors affecting health, health perception and self-efficacy were selected for this study.
The interpersonal factor is the influence of formal and informal social networks and social support systems, including family relationships and workplace peer relationships (McLeroy et al., 1988). In Korea, unlike in Western culture, family ties are close, and family support has an important impact on maintaining family members’ health. An individual’s social network, including neighbors and friends, influences behaviors and attitudes, ultimately affecting the health of individuals (Oh et al., 2010).
Organizational factors refer to organizational characteristics, regulations, policies, informal structures, and health promotion goals that support the behavior change of individuals within the organization (McLeroy et al., 1988).
Job stress and organizational health culture were selected as the organizational factors and were explored in this study. Job stress is recognized as a major risk factor in the health of workers; the higher the job stress, the lower the health-promoting behaviors (J. S. Kim & Kim, 2016). High levels of stress can lead to atherosclerosis, trigger CVD, and increase the risk of coronary artery disease among workers (Chinnaiyan, 2019; Lecca et al., 2019). The organizational atmosphere in which health-related activities can be carried out also has an impact on an individual’s physical and psychological health. Yun (2017) confirmed that the more favorable the perception of organizational culture, the higher the health-promoting behaviors in individuals.
This study examined the effects of individual factors (health perception, self-efficacy), interpersonal factors (family support, social network), and organizational factors (job stress, organizational health culture) on the CVD prevention behaviors of office workers (Figure 1). The results of this study could inform the development of potential strategies for the prevention of CVD among office workers, including customized intervention programs.

Conceptual framework of the study.
Materials and Methods
Study Design
This cross-sectional study identified factors influencing CVD prevention behaviors among office workers based on an ecological model.
Participants
Eligible study participants included workers aged 20 to 65 years who performed sedentary or administrative work mainly in offices. The study excluded part-time employees who worked less than 4 hr a day, people who were engaged in CVD prevention activities after being diagnosed with a CVD, and those who could influence CVD prevention activities due to an illness or physical disability. A total of 143 responses were calculated as a minimum number of samples using the multiple regression analysis in the G*Power 3.1 program, with a significance level of alpha of .05, effect size medium of .15, and power of .80 (Kong et al., 2016).
CVD Prevention Behavior
CVD is a generic term for conditions affecting the heart or blood vessels, such as myocardial infarction, angina pectoris, hypertension, diabetes, and arteriosclerosis. The level of CVD prevention behavior was assessed using a modified lifestyle questionnaire typically used for health checkups for Koreans, which has been validated by Park (2008). The questionnaire addressed smoking (e.g., What is the average amount of smoking per day?), drinking (e.g., How many times do you drink?), exercise (e.g., How many days per week do you usually do vigorous intensive exercise for more than 20 min, such as sweating or beating heart?), diet (e.g., How much vegetables do you eat at every meal?), stress management (e.g., When you are stressed, do you use positive ways to relieve tension and pressure, such as meditation, music, movies, and travel?), sleep (e.g., How many days do you get enough sleep at least 7 hr in a week?), blood pressure monitoring (e.g., Do you measure your blood pressure regularly?), blood glucose measurement (e.g., Do you regularly measure your blood glucose?), and body weight (e.g., Do you weigh yourself regularly and compare it with your standard weight?). Each behavior was measured on a 5-point Likert-type scale of 1 (not at all) to 5 (very much), for a total of 90 points. The higher the score, the better the CVD prevention behaviors. Park’s (2008) study showed a Cronbach’s alpha of .73; this study recorded .70.
Personal Factors
Health perception was measured using the Health Perception Questionnaire developed by Ware (1979). The measurement consisted of 20 questions (e.g., According to the doctors I have seen, my health is now excellent) about current, past health, future health, health concerns, resistance and sensitivity, and the rejection of a sick role. At the time of development, this instrument’s reliability was a Cronbach’s alpha of .91, with .72 recorded in this study.
Self-efficacy was measured using the General Self-Efficacy Scale (GSE) developed by Schwarzer and Jerusalem (1995) and translated into Korean by Y. M. Lee et al. (1994). The measurement consisted of 10 questions (e.g., “I can always manage to solve difficult problems if I try hard enough”). The reliability of the tool was a Cronbach’s alpha of .76 at the time of development, and .85 was recorded in this study.
Interpersonal Factors
To measure family support, we used the Multidimensional Scale of Perceived Social Support (MSPSS) Scale developed by Zimet et al. (1988). The MSPSS consists of family support, friendship support, and special support from meaningful others. In this study, four items of family support (e.g., My family really tries to help me) were used, and a Cronbach’s alpha of .95 was achieved.
Social network was measured using the Social Network Scale (LSNS) developed by Lubben (1988). The LSNS includes a social network of family members, friends, and relatives. The measurement consisted of 10 questions (e.g., How many relatives do you see or hear from at least once a month?) and the Cronbach’s alpha was .70 in this study.
Organizational Factors
Job stress was measured using the Korean Occupational Stress Scale–Short Form (KOSS-SF) developed by Chang et al. (2005). It consists of 24 questions (e.g., Due to many things to do, I always feel time pressure): job demands, lack of job autonomy, job conflicts, job instability, organizational system, inappropriate compensation, and work culture. Cronbach’s alpha was .51 to .82 at the time of development of the form and it was .84 in this study.
The organizational health culture was measured using the Social Environment Influencing Health developed by J. A. Lee (2016). The questions are about the group’s use of alcohol and its health practices. The measurement consisted of eight questions (e.g., My workplace regularly conducts health education) and Cronbach’s alpha was .72 in this study.
Each measurement tool was used after receiving consent via e-mail from the developers. The general characteristics included gender, age, marital status, education level, length of work, average weekly working hours, and monthly income. Disease-related characteristics included chronic illness, the presence of a family history of CVD, and medications.
Research Procedure
The data collection was conducted from April 20 to May 23, 2019, in J, S, G, and S cities of Korea through convenient sampling. The researcher visited schools, financial institutions, public corporations, and public institutions and obtained approval from managers or directors of the institutions after explaining the purpose of the study. The study was presented to a total of 300 office workers. Of these, 260 workers showed interest and gave explicit consent to participate in the study.
The researcher distributed a self-reporting questionnaire directly to those who voluntarily accepted the research participation, explaining the purpose and purpose of the study, confidentiality, and rights of participants in the study. A total of 260 questionnaires were distributed, of which 239 were returned (return rate = 95.6%). Of these, 221 were used for the final data analysis, excluding 18 questionnaires that were incomplete or inadequate.
To maintain the confidentiality of the study participants, the questionnaire was filled out at the participant’s desk and directly sealed upon completion. During the completion of the questionnaire, participants were allowed to ask questions at any time. The questionnaires that were answered were immediately retrieved on the spot. Participants who participated in the questionnaire were given a gift as a token of appreciation.
Data Analysis
The collected data were analyzed using the SPSS/WIN 23.0 program as follows. Descriptive (frequency, percentage, mean, and standard deviation), and an independent t test and analysis of variance (ANOVA) were used to compare the differences of CVD prevention behaviors according to demographic characteristics. The normality of the variables was tested, and all assumptions of the parametric tests were checked. A correlation analysis of each variable was also conducted. Hierarchical regression was used to determine the effect of individual and organizational factors on CVD prevention behavior.
Ethical Considerations
This study was approved by the Institutional Review Board of Jeonbuk National University (IRB No. 2019-04-016-001).
Results
Characteristics of the Participants
Among the participants, 57% were females and 58.4% were above 40 years of age. Most (72%) of the participants had a partner. The educational level of 76.9% of the participants was a university degree. Among the participants, 48.9% were worked for 10 to 29 years. Most (89.1%) worked between 40 and 50 hr per week. The income level of 39.8% of the participants had 2,010,000 won to 3,000,000 won, 12.2% of participants had a chronic disease, 25.8% of participants had a family history of CVD, and 10.4% were currently taking medications (see Table 1).
Characteristics of the Participants and Differences in CVD Prevention Behavior According to Characteristics of Participants (N = 221).

Note. CVD = cardiovascular disease.
Differences in CVD Prevention Behavior According to Characteristics of Participants
The CVD prevention behavior was significantly higher in women than in men (t = −2.02, p = .045), and in those working less than 40 hr per week than those working more than 51 hr (F = 3.68, p = .027). The prevention behaviors of those with a family history of CVD were significantly higher than those with no family history of CVD (t = 2.79, p = .006; see Table 1).
Correlations Among Personal, Interpersonal, and Organizational Factors and CVD Prevention Behavior
CVD prevention behaviors correlated with health perception (r = .204, p = .002), family support (r = .187, p = .005), and health culture (r = .177, p = .008; see Table 2).
Correlations Among Personal, Interpersonal, Organizational Factors and CVD Prevention Behavior (N = 221).

Note. CVD = cardiovascular disease.
Effects of Personal, Interpersonal, and Organizational Factors on CVD Prevention Behavior
The condition of the regression analysis was confirmed to be satisfactory prior to the analysis. The Durbin–Watson index was 1.933 (dU = 1.865 < d), which was close to 2, independent of the dependent variable, and the variance inflation factor (VIF) index was 1.108 to 1.943; all variables were less than 10 and showed no multicollinearity. The Kolmogorov–Smirnov test results of the standardized residuals satisfied the assumption of normality (p = .554 > .05) and the Koenker test result (p = .062, > .05) of I. H. Lee (2018), using the Easy Flow Statistics Macro.
In the first stage of the hierarchy, those working more than 51 hr per week showed worse CVD prevention behaviors than those working less than 40 hr (B = −7.13, p = .014). Individuals with a family history of CVD showed better CVD prevention behaviors than those without a family history of CVD (B = 3.30, p = .002). This model accounted for 7.0% of the variance in CVD prevention behaviors (adjusted R2 = .070, F = 5.167, p = .001). Adding personal factors, health perception (B = 0.360, p = .001) was associated with CVD prevention behavior, accounting for 10.8% of the variance in CVD prevention behavior (adjusted R2 = .108, F = 5.448, p < .001; Model 2). Family support had a significant influence (B = 0.375, p = .003) on CVD prevention behavior. This model accounted for 13.8% of the variance in CVD prevention behaviors (adjusted R2 = .138, F = 5.409, p < .001; Model 3). Organizational health culture (B = 0.361, p = .012) was associated with CVD prevention behaviors. The final model accounted for 15.8% of the total variance in CVD prevention behaviors (adjusted R2 = .158, F = 5.115, p < .001; Model 4). Overall, health perception of personal variables was the most significant predictor of CVD prevention (see Table 3).
Effects of Personal, Interpersonal, and Organizational Factors on CVD Prevention Behavior (N = 221).
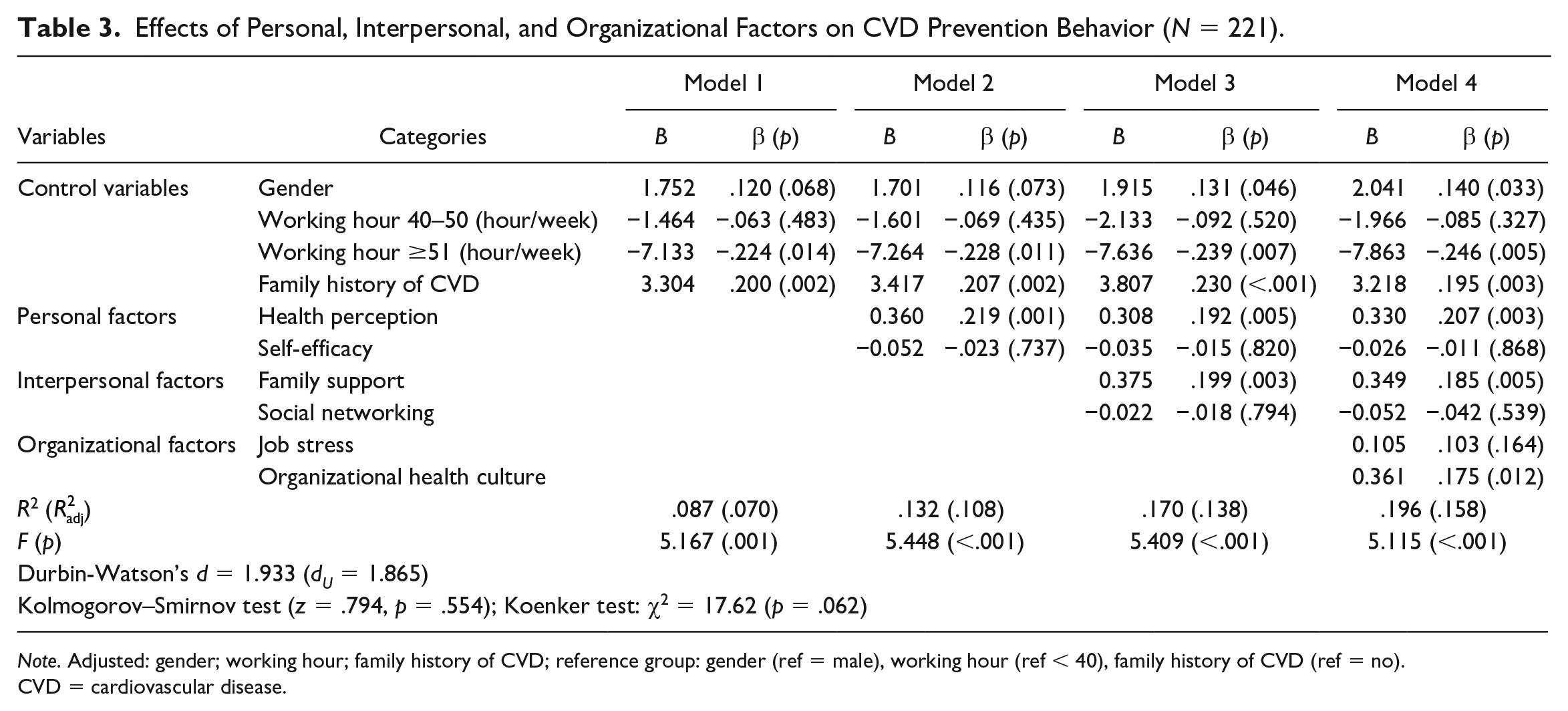
Note. Adjusted: gender; working hour; family history of CVD; reference group: gender (ref = male), working hour (ref < 40), family history of CVD (ref = no). CVD = cardiovascular disease.
Discussion
Increased incidence of CVD and the mortality rate of workers can affect individual health as well as the productivity and economic status of organizations and countries. Office workers with sedentary lifestyles have a high risk of CVD (Wilmot et al., 2012). This study considered interpersonal and environmental factors affecting individuals based on an ecological model to identify the factors that affect the CVD prevention behaviors of office workers. The results of this study showed that women were significantly more likely to practice CVD prevention behaviors than men (B = 2.041, p = .033), which is consistent with studies showing that healthy lifestyles (K. Kim et al., 2007) aimed at preventing CVD, including exercise habits, stress management, and smoking cessation (Xu et al., 2015), were higher in women than in men. This can be explained by the tendency of women to be more responsible for their own health (Davidson & Freudenburg, 1996), having generally lower smoking and drinking rates and higher interest in diet than men. This suggests that strategies for preventing CVD should be developed by considering gender differences, and healthy lifestyle programs should be tailored for men with high smoking and drinking rates. Furthermore, the longer working hours of the office worker participants were found to have a significant effect by lowering CVD prevention behaviors (B = −7.863, p = .005). In a meta-analysis of long working hours and the risk of CVD, those with long working hours were found to have a 1.37 times (95% confidence interval [CI] = [1.11, 1.70]) greater risk of developing CVD (Kang et al., 2012). Therefore, to improve CVD prevention behaviors among office workers, working conditions must be changed, including reducing working hours, guaranteeing rest time during repeated or sedentary work, and providing health education around the need for regular exercise, lifestyle corrections, and regular health checkups. The Korean government has been enacting amendments to the Labor Standards Act, which cuts working hours from a maximum of 68 to 52 hr in a week (Ministry of Employment and Labor, 2019). The office workers with a CVD family history showed significantly higher prevention behaviors than those without a family history of CVD (B = 3.218, p = .003), consistent with the results of another study (Kong et al., 2016). This may be because individuals with a CVD family history are more interested in preventing CVD and more motivated to change their health behaviors in a favorable way, including acquiring knowledge about maintaining and promoting cardiovascular health. Therefore, in approaching individuals with a family history of CVD, it is important to examine and discuss their risk factors, and they should be supported to practice health-promoting behaviors to lower their risk of CVD. In the fourth model of the hierarchy, which includes organizational factors, the explanatory power increased by 15.8%, indicating an increase of about 7.0% in explanatory power as individual factors and organizational factors were added. This shows that the degree of prevention of CVD in office workers is influenced by various factors, such as individual and organizational factors. Among the individual factors, in terms of health perception, the higher the perceived health, the better the CVD prevention behaviors (β = .207, p = .003). In particular, the results of this study showed that health perception has the greatest influence on CVD prevention behaviors. Health perception can be a motivator in health promotion behaviors and can affect a person’s attitude toward such behaviors (N. H. Kim & Sohng, 2009). Recognizing and changing health risks can lead to increased healthy behavior (Ferrer & Klein, 2015). Therefore, a tailored strategy directed toward office workers with low health perception is needed to encourage and educate them to practice health-promoting behaviors. Among interpersonal factors, family support of the participants had a significant effect on the prevention of CVD (β = .185, p = .005). Family support makes family members feel worthy through love and respect and gives them a sense of belonging to a communication and mutual accountability network (Cobb, 1976). Unlike Western countries, Korea is traditionally a family-centered culture, and family support is a driving force in the mutual interaction around health-promoting activities. The family can therefore play an important role in solving health problems and achieving a healthy life in office workers. The family should be involved in the healthy lifestyle change of office workers who have high risks of CVD, such as obesity and heavy smoking.
Finally, the organizational health culture was found to have a significant effect on the prevention of CVD (β = .175, p = .012). The health culture of an organization is shared by its members and it affects their health and health-promoting behaviors (Lin & Lin, 2014). The organizational environment can affect individuals and communities in a way that impacts personal problems, psychological problems, stress, and the quality of life (Kompier, 2002). It is therefore likely that the health of individuals working in an organization can be greatly influenced by how the organization strives to maintain and promote the health of its workers. Consequently, it is necessary to develop a program that takes into consideration organizational and environmental factors in the workplace to promote the lifestyle of the workers. From a long-term perspective, the health of the organization to which a worker belongs is closely related to the productivity of the organization. Therefore, organizations should support the development of an optimal health culture through purposeful communication, effective resource utilization, and an appropriate problem-solving process. The key role of an individual’s physical environment is clearly addressed, and, therefore, the workplace should be considered in health promotion efforts (e.g., exercise equipment installation).
Ecological models are concerned with the relationship between individuals and their surrounding environments. This study is one of the studies aimed at identifying factors that significantly influence the CVD prevention behaviors of Korean office workers based on an ecological model. The study contributes by providing evidence that health perception, family support, and organizational health culture should be the most emphasized factors to promote CVD prevention among office workers. In addition, it is important to study how policy factors, such as disease prevention, early detection, and the health management of the organization, affect the health of workers.
This study has some limitations. First, there is a limit to the inclusion of policy factors that may affect the health behaviors of the participants in the ecological model. However, this study sought to understand the multidimensional influences based on ecological models by sampling various types of office workers in various places, such as private workplaces, public institutions, schools, and hospitals in four cities and provinces in Korea. The results of this study showed that the factors influencing the prevention of CVD in office workers were diverse and based on an ecological model rather than on isolated, fragmented factors. Therefore, multidimensional approaches and interventions are needed to maintain office workers’ cardiovascular health. Notably, this is the first study to address these important points.
Conclusion
This study was conducted to identify the factors affecting CVD prevention behaviors among office workers, based on an ecological model. The higher the perception of health and family support, and the better the organizational health culture, the better the CVD prevention behaviors. Therefore, comprehensive and multidimensional interventions are required for the prevention of CVD in office workers.
Based on the findings from this study, we suggest the following. First, the various laws and policies of organizations can directly or indirectly affect workers’ CVD prevention behaviors and state of health. Thus, it is suggested that research be conducted to reveal the multidimensional factors influencing health-promoting behaviors through ecological models that include more policy factors. Second, we propose a comparative study that includes nonoffice workers to evaluate the influence that different environments may have on the prevention of CVDs.
Footnotes
Ethical Considerations
The study was approved by the Jeonbuk National University Institutional Human Subjects Review Committee (IRB No. 2019-04-016-001).
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2019S1A5C2A01080989).