
Abstract
Hypertension continues to emerge globally as one of the most dangerous cardiovascular disease risk factors. The toll of hypertension as a chronic disease on population health and the resultant impact on the often already stressed medical systems of developing nations is a serious concern. Shifting existing paradigm and resources from communicable to chronic disease prevention continues to be a formidable task. This article presents the results of a cross-section analysis of Adansi South, Ghana, residents (N = 539) 5 years and older to investigate the blood pressure status and select hypertension risk factors across all age groups. Approximately a third of Adansi South respondents (27.1%) were identified as hypertensive. While the largest percent of the hypertensive subset was in the 40 to 59 age group, of concern was the emerging pattern among young and adolescent respondents who were either identified as hypertensive and/or having modifiable risk factors for hypertension like elevated body mass index (BMI). A rationale for expanding adolescent health education and health promotion is offered, and alternative methods for deploying health promotion activities in resource-limited areas are proposed and discussed.
Hypertension, once rare in traditional African societies, is rapidly becoming a major chronic disease problem in Sub-Saharan Africa. An estimated 10 million to 20 million people in Sub-Saharan Africa have hypertension (Cappuccio, Plange-Rhule, Phillips, & Eastwood, 2000). A study on hypertension conducted in Ghana between 1972 and 1987 revealed a prevalence rate of 4.5% among rural dwellers and 8% to 13% in the urban areas (Pobee, 1993). In 2003, the prevalence of hypertension in urban Accra was found to be 28.3% (Amoah, 2003) and 28.7% in Ashanti (Cappuccio et al., 2004). Trends in hypertension prevalence and incidence continue to grow in Ghana. According to the 2008 annual district report, hypertension was one of the fourth leading causes of outpatient morbidity, and contributed to some of the highest rates of mortality (Ghana Ministry of Health, 2007). Cooper, Amoah, and Mensah (2003) assert that hypertension is one of the roots of epidemic levels of cardiovascular disease in Africa.
Historically, there has been a definitive focus on communicable disease in Africa and other developing regions rather than chronic, lifestyle-related diseases like hypertension. A shift in emphasis from communicable to chronic disease requires models of effective health care delivery to evolve in a different way (Allotey, Reidpath, Yasin, Chan, & Aikins, 2011; Beaglehole et al., 2008; Nishtar, 2004; Samb et al., 2010). While chronic and communicable disease share some overlapping goals (surveillance, diagnosis, and treatment), chronic disease differs due to the often long-term course of development of the disease and enhanced emphasis on lifestyle factors as mediators of disease. The time lag between development of risk factors and the disease provides a significant window for intervention, but it also extends the time that valuable and often scarce health care resources that characterize developing economies must be utilized for care and treatment.
Adansi South, Ghana, is in many ways representative of the difficulties many regions face in balancing few resources (limited numbers of hospital facilities, health care worker shortages, and health spending) to battle communicable diseases while the negative impacts of chronic disease on the health care system and the populace continues to increase. According to the Adansi South Ministry of Finance and Education (2012), Adansi South District is one of the 27 districts in the Ashanti Region. The district is 899 sq. km, approximately 4% of the total area of the Ashanti region. The total population for New Edubiase (the district capital) was 98,526 in 2006 (Ghanadistricts.com, n.d.). Children 0 to 14 years old constituted 48% of the population. The growth rate for the district is 3.5% that is higher than the regional growth rate of 3.4%, and the national growth rate of 2.7%. There is one hospital at New Edubiase. In all, 200 distinct communities have been identified and many of those communities are served by community-based volunteers trained to assist health officers to carry out basic primary health care activities such as immunization, Health Education, and Growth Monitoring (Ghana Ministry of Health, 2007). While Malaria continues to be the number one cause of morbidity in Adansi South, hypertension was listed fourth on the list of top 10 diseases in 2008 (Ghana Ministry of Health, 2007).
Method
In 2007, the authors conducted a small, cross-sectional study to examine the prevalence of hypertension and associated risk factors (age, gender, body mass index [BMI], substance use, family history) in the Adansi South region. Study authors used the World Health Organization (WHO; 1996) classification of hypertension for adults, and the National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents classifications for children and adolescents (Falkner & Daniels, 2004; see Table 1). Data were collected by using the WHO STEP-wise approach for surveillance for non-communicable disease (WHO, 2002). STEPS is a sequential process starting with gathering information on key risk factors by use of questionnaires (Step 1), then moving to simple physical measurements (Step 2), and then recommending the collection of blood samples for biochemical assessment (Step 3). Steps 1 and 2 were used in this study. Data collected included personal identification, socio-demographic data, general knowledge of hypertension and its risk factors, and biophysical data that consisted of blood pressure measurement, weight, and height of respondents.
Classifications of Hypertension for Adults, Children, and Adolescents.
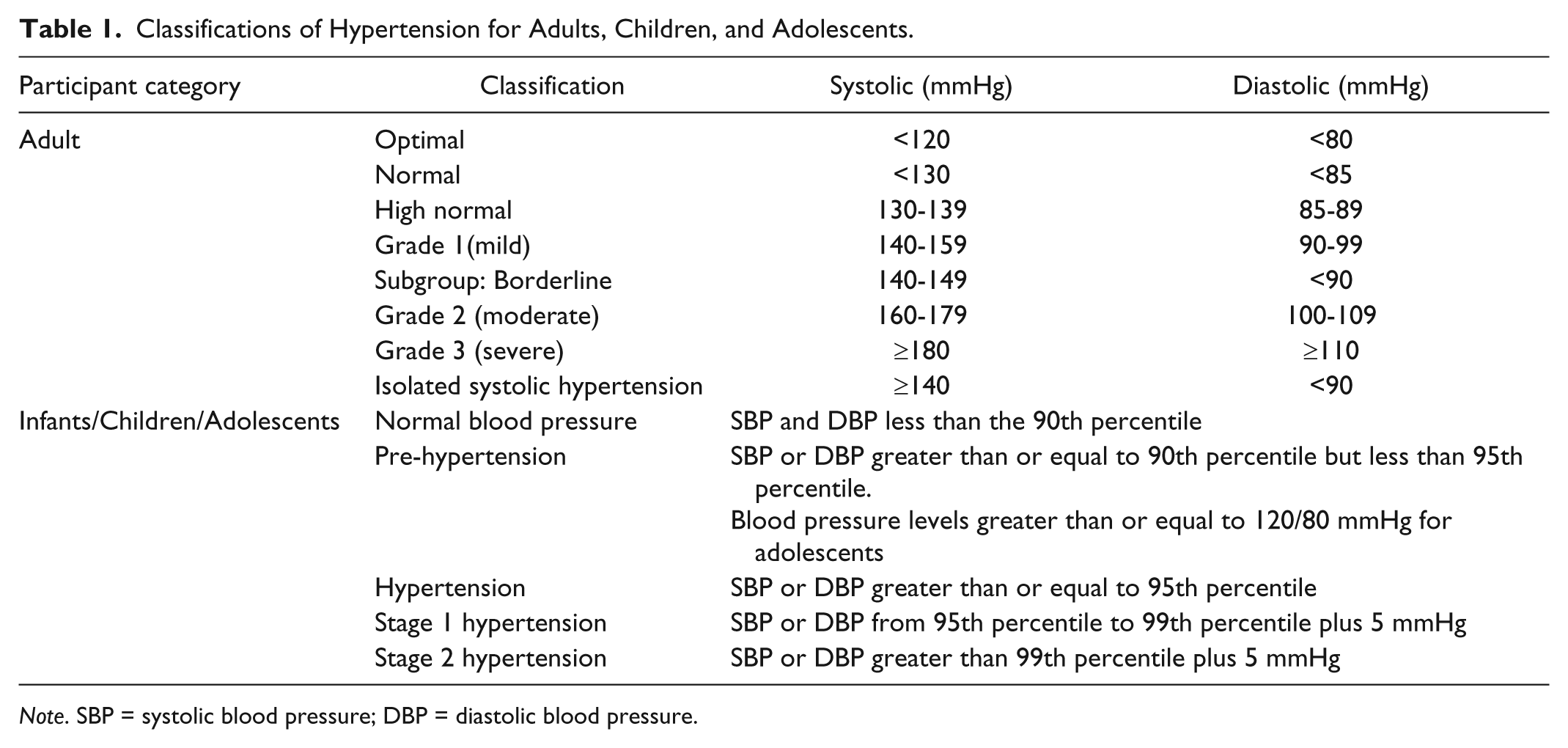
Note. SBP = systolic blood pressure; DBP = diastolic blood pressure.
At least two blood pressure measurements were taken for each study respondent using the OMRON digital sphygmomanometer. Before taking the measurements, the respondent was advised to sit quietly and rest for 5 min with the legs uncrossed and the right arm free of clothing. After two readings, if the difference between the first and second readings was >10 mmHg, then a third reading was taken and recorded and the average of the closest two was used for analysis. Subjects were weighed on a standard scale without shoes and looking straight ahead. The heights of respondents were measured in centimeters using a non-elastic plastic measuring tape. Respondent height was recorded without footwear. The BMI was then calculated and determined using the WHO BMI classifications (2002). The BMI was used to classify study respondent body weight as underweight (BMI less than 18.5), normal weight (BMI = 18.5-24.9), overweight (BMI = 25-29.9), or obese (BMI = greater than 30; WHO, 2002).
The study population consisted of 539 respondents aged 5 years and above. Under age study subjects received parental consent to participate in the study. A random cluster sampling procedure was used. The cluster was selected with probability in proportion to the size of the village in terms of households. In all, 42 clusters were selected from the five sub-districts and 13 individuals aged 5 years and above were targeted from each cluster for interview. Eligible subjects in each household were randomly selected per age group. Fifty questionnaires were administered in five sub-districts. All questionnaires were pre-tested before final administration. Data were primarily collected by community health nurses and community-based surveillance (CBS) staff. Data collectors were given training session that included interview techniques, detailed introduction to data collection tools, and physical measurement instruments. Data entry and analysis were made using SPSS statistical software.
Results
Table 2 provides select demographics, risk factors, and hypertension status of respondents. There were slightly more females (53.8%) than males (46.2%). Most of the respondents were between 20 and 39 years old (31.4%). In regard to substance use, the majority of the total sample was identified as non-drinkers (86.1%), and non-smokers (97%). Twenty-six percent of the respondents had a BMI in the underweight category; 50% had a BMI in the normal weight category, and 24% were in the overweight BMI category. Approximately 82.2% of the total respondents had no family history of hypertension, and almost a third of the respondents (27.1%) were identified as having hypertension.
Distribution of Select Demographic and Risk Factors (N = 539).

Note. BMI = body mass index.
Table 3 presents information about age, substance use, BMI, and family history of those identified as having hypertension (n = 146). Thirty-nine percent of the respondents who were identified as hypertensive were in the 40 to 59 age group, and almost a quarter (24.7%) were in the 20 to 39 age group. Almost 25% (24.6%) of the hypertensive subset identified as alcohol drinkers, and 9% identified as smokers. Approximately 42% (41.7%) of the hypertensive subset had BMI ≥25. Greater than a third of the hypertensive subset (34.9%) identified a family history of hypertension.
Age, Substance Use, Elevated BMI, and Family History Among Hypertensive Respondents (n = 146).

Note. BMI = body mass index.
Discussion: Opportunities for Health Promotion
Almost a third (27.1%) of the sample was identified as hypertensive in Adansi South, Ghana. While the highest percentage of hypertensive respondents were in the 40 to 59 age group (39%), of equal concern is the percentage of respondents (35%) in the combined 13 to 19 and 20 to 39 age groups who were identified as hypertensive. These study results highlight possible points of health education and promotion intervention among adolescents and young adults in Adansi South. There was a twofold increase in the percent of respondents with hypertension between the 13 to 19 and 20 to 39 age groups (see Table 3). Table 4 highlights that in the total sample (N = 539), there was almost a fourfold increase in the percent of respondents with a BMI ≥ 25 in the same age groups.
BMI Distribution by Age in Total Sample (N = 539).

Note. BMI = body mass index.
There is a paucity of research on the potential impacts of leveraging adolescent and school-based health promotion for making chronic disease prevention an early rather than late stage priority in resource-limited regions. Adolescent health is frequently under the umbrella of school health. Popular models like the coordinated school health model (Allensworth & Kolbe, 1987; Lohrmann, 2010) provide a well-integrated, ecological framework for improving the health of children and adolescents and by extension of the community. While those concepts continue to be sound, they may lack feasible carryover in developing nations due to the widely variable nature of access to education. Considerations of new, region-specific models of school health need to be a part of the conversation of adolescent health promotion.
In Africa, much of the current school-based health promotion work focuses heavily on sexual and reproductive health (Brieger, Delano, Lane, Oladepo, & Oyediran, 2001; Green, Halperin, Nantulya, & Hogle, 2006; Kirby, Laris, & Rolleri, 2007). According to the health sector report on Ghana Districts, adolescent sexual health education for the prevention of HIV is already a priority (Ghanadistricts.com, n.d.) as well as the expansion of school feeding programs (Adansi South, Ghana District, 2011). Expanding existing adolescent health education to have a more comprehensive focus on overall wellness to prevent development of chronic cardiovascular disease risk factors may be an imperfect, yet viable alternative to having to implement new programs when resources are scarce.
Alternative education settings also need to be explored in resource-challenged areas. In places where adolescents may work to help support families, worksites may be able to serve as an education setting. In addition, health educators may be able to capitalize on adolescent’s affinity for and high comfort levels with technology to diffuse health education messages via cell phones and other mobile technologies. Cell phones and by extension SMS messaging and use of mobile reminders have been shown to have positive impact in several HIV intervention studies in Africa (Lester et al., 2010; Swendeman & Rotheram-Borus, 2010). There is not a comprehensive body of research regarding the efficacy of leveraging mobile technologies for health promotion messaging for chronic diseases prevention in Africa, though those techniques have been used with success in the United States (Fjeldsoe, Marshall, & Miller, 2009).
This study highlighted hypertension as an important health issue in the Adansi South district. High blood pressure and the resulting morbidity are clearly poised to add to the disease and financial burden of Adansi South if effective prevention measures are not instituted. Ultimately, the strength of a health promotion approach is prevention. Economically, socially, and medically, prevention of diseases rather than treatment yields the greatest benefit to a population. Given that resource-limited areas like Adansi South, Ghana, are noted to have a deficit in health care dollars, staff, and infrastructure to care for chronic disease burdens, health promotion efforts should still have a prominent place in health care. Despite the challenges, health promotion professionals in Adansi South and other developing regions can benefit from expansion of adolescent health promotion in their current and future strategic health care planning decisions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.