
Abstract
The health status of Nigerian Americans is poorly documented due to data aggregation with other Black ethnicities. This study examined acculturation, health status, and health-promoting lifestyle among Nigerian Americans. This study was conducted remotely utilizing a cross-sectional, quantitative design, with path analyses (N = 161). Acculturation, guided by Berry’s model, was conceptualized through ethnic and dominant society immersion (Stephenson Multigroup Acculturation Scale). Health-promoting lifestyle was measured using Health-Promoting Lifestyle Profile-II and health status through SF-12. Both ethnic and dominant society immersion significantly predicted all health-promoting lifestyle domains; spiritual growth had the largest β coefficient (.35 and .30 respectively) and had a positive predictive effect on physical (β = .38) and mental health (β = .34). Further, interpersonal relations was positively associated with mental health (β = .30). Study findings can impact healthcare practices, particularly culturally congruent care, and policy influencing health outcomes and healthcare equity.
Plain language summary
There are hundreds of thousands of Nigerian immigrants in the United States, but their specific health status is poorly documented due to data aggregation with other Black ethnicities. Even though acculturation influences health behavior in other cultures, this relationship is understudied in the Nigerian immigrant community which influences healthcare equity. This study examined acculturation, health status, and health-promoting lifestyle of Nigerian Americans (N = 161) utilizing a cross-sectional, descriptive, and quantitative design. Key constructs from Berry’s acculturation model guided the study. Acculturation was conceptualized as occurring through varying levels of immersion in one’s ethnic society and the dominant society. Both ethnic and dominant society immersion significantly predicted all health-promoting lifestyle domains; spiritual growth had the largest effect. Further, spiritual growth had a positive predictive effect on both physical health and mental health while interpersonal relations was the only other health-promoting lifestyle domain that was positively associated with mental health. Maximizing spiritual growth and interpersonal relations could improve physical and mental health of Nigerian immigrants. Study findings can impact healthcare decision-making, health practices, and healthcare utilization which may in turn influence health outcomes and reduce disparities in care. This study was limited to a convenience sample of first-generation Nigerian Americans, recruited from larger cities, thereby limiting generalization of study findings. Self-reporting is another limitation of this study which can introduce bias into study findings.
Keywords
Health status specific to Nigerian Americans is not well documented due to data aggregation with other Black ethnicities (Commodore-Mensah et al., 2018; Joseph et al., 2017; Omenka et al., 2020; Singh et al., 2013; Zan & Fan, 2017). Like most Black individuals compared to White Americans, Nigerian Americans are reportedly more likely to suffer from chronic conditions and be overweight or obese, self-report lower ratings of overall health, and have worse mortality profiles (Hamilton & Massey, 2019; Hurston et al., 2024; Ike-Chinaka, 2013; Webb et al., 2024). Even compared to their African American counterparts, Nigerian Americans and other immigrants from sub-Saharan Africa are noted to have higher health risks (i.e., risk for cardiovascular disease) (Obichi & Dee, 2022).
Immigrants are generally healthy upon arrival in their new country of residence, such as developed countries, but their health status tend to decline with increased duration of residency (Taylor & Sarathchandra, 2015). Among Nigerians, their risk for poor health appear to increase with long-term U.S. residency (Ike-Chinaka, 2013). For example, there is consistent relationship between U.S. residency and obesity (Ike-Chinaka, 2013; Obisesan et al., 2017; Roshania, 2008). Whether acculturation contributes to this decline is lacking from the literature, particularly for Nigerian Americans, their health-promoting lifestyle, and current health status.
Most acculturation studies in the literature have focused on the Latino population (Hernandez-Rodriguez, 2018; Kapke et al., 2017; Schwartz et al., 2015) and Asian Americans (Myers & Rodriguez, 2004; Suinn, 2010). Yet, there are more Nigerian Americans residing in the United States than any other African country (Ekwemalor & Ezeobele, 2020) increasing from approximately 376,000 (Migration Policy Institute, 2015) to 681,650 (United States Census Bureau, 2021). Despite the dramatic increase of US immigration particularly among Nigerians (Corra, 2023), acculturation studies on Nigerian Americans are sparse and outdated. Further, investigating African-born migrants as one aggregated, homogenous ethnic group minimizes the large diversity that exists in the continent of Africa (Deslandes et al., 2024). Therefore, this study focusing on Nigerian Americans contributes valuable data to facilitate their overall health considering the extent to which they adapted to their new homes.
Many studies present a unidimensional understanding of acculturation (Deslandes et al., 2024; Schwartz & Unger, 2017). Instead, Berry’s 1992 acculturation model (Berry, 1992) was used to guide this study leveraging the comprehensive concepts of dominant society immersion (DSI) and ethnic society immersion (ESI). Berry conceptualized acculturation as taking place through varying levels of DSI or adapting to a new culture, and ESI or connection to one’s ethnic culture. Other studies have also used Berry’s model (Deslandes et al., 2024; Schmitz & Schmitz, 2022) to better understand the complex intersection of acculturation and health. Both adoption to host culture and maintenance of home culture are relevant in studying the full spectrum of acculturation (Deslandes et al., 2024). Therefore, this study explored: (a) how the bidimensional conceptualization of acculturation predicts health-promoting lifestyle, and (b) how this lifestyle predicts the health status of Nigerian Americans.
Healthy People 2030 emphasized health-promoting lifestyles and health equity as priority areas (Office of Disease Prevention and Health Promotion, 2020). Hence, understanding acculturation within the context of DSI and ESI is important; these immersion experiences influence health behavior and adaptation (Berry et al., 2012; Berry, 1992, 1997; Liebkind et al., 2012) Therefore, findings from this study can help advance the understanding of acculturation and health which is important to researchers, health practitioners, and policymakers toward enhancing health promotion, disease prevention, equitable health care, and health outcomes.
Theoretical Framework
Berry’s behavioral shift model in acculturation (Berry, 1992) guided this study. Berry contended that intercultural contact produces changes in behavior—behavioral shifts—that can lead to varying degrees of adaptation. Behavioral shifts encompass values, attitudes, and lifestyle preferences. Berry’s model identifies cultural maintenance as a core factor in this acculturation process (Berry et al., 2012; Berry, 1992, 1997; Berry et al., 1989). A person’s DSI/ESI efforts will depend in part on how much individuals would like to preserve their customs, traditions, and identity. Acculturation depends essentially on participation in and contact with cardinal and non-cardinal cultural groups (Berry et al., 2012; Berry, 1992, 1997; Berry et al., 1989).
Utilizing Berry’s model, this study aimed to evaluate acculturation (DSI and ESI), behavioral shifts (i.e., changes in health-promoting lifestyle), and adaptation outcome (i.e., health status) among Nigerian Americans.
Therefore, we set out to question the following:
(1) Does acculturation (DSI and ESI) predict the health-promoting lifestyle domains (i.e., nutrition, physical activity, stress management, interpersonal relations, spiritual growth, and health responsibility) of Nigerian Americans?
(2) Do the health-promoting lifestyle domains predict the health status (physical health and mental health) of Nigerian Americans?
Methodology
A cross-sectional, descriptive, and quantitative design was employed in this study, which was deemed exempt by the Institutional Review Board protocol #1605444 at University of Nevada, Las Vegas. Data were completed online due to the coronavirus disease 2019 (COVID-19) pandemic between the periods of July to September 2020 with no personal identifiers collected. We adhered to the standard manuscript guidelines on reporting cross-sectional, observational studies (Equator Network, 2022).
Participants and Data Collection
The study sample consisted of first-generation, adult Nigerian Americans living in the United States for best representation of the population fitting to the research questions in this study. In this study, first-generation Nigerians refer to individuals who were born in Nigeria and subsequently immigrated to and residing in the United States. Other inclusion criteria required that participants were aged 18 and older, and could read, write, and understand English. Since the official language in Nigeria is English, adult Nigerian Americans are mostly fluent in English. Exclusion criteria were those who obtained Nigerian citizenship by marriage. Nigerian Americans who were born and/or lived in countries other than Nigeria prior to immigrating to the United States were also excluded to avoid the confounding effects of acculturation in other regions of the world. Finally, biracial, or bicultural Nigerians were excluded in order to avoid any confounding effects of cultural and national identity.
Convenience and snowball sampling was used to obtain the sample. These sampling techniques are widely recognized as essential to studying hard-to-reach populations, such as immigrants who are dispersed and may lack a formal organization, with the ability to gather unique social knowledge and insights into community networks (Kirchherr & Charles, 2018). Due to the COVID-19 pandemic, the study was done completely online, including recruitment efforts and data collection. Participants were recruited electronically via a scripted e-mail describing the study to informal contacts and key individuals who had connections to the population, such as existing relationships with local pastors and other sociocultural organizational leaders who subsequently shared the information with their constituents and provided referrals. Informational flyers were also posted on specific social websites associated with Nigerian organizations, helping to facilitate snowball sampling. The scripted email and informational flyers contained a Qualtrics link that potential participants used for the study. The link consisted of the inclusion/exclusion criteria, informed consent, and online surveys.
A priori power analysis (Hair et al., 2016) for partial least squares, similar to structural equation modeling or path analysis (Hair, 2017) was used assuming the statistical significance level = .05, power = 0.8, maximum number of arrows pointing into 1 dependent variable = 2 to 10, with 4 minimum effect sizes (R2 = .10, .25, .50, and .75). The minimum sample sizes are 157, 75, 48, and 31, respectively. Given that the effect size in this study may be small (R2 = .10), we aimed for at least 157 participants to provide sufficient power for statistically significant results.
Measures
All measures were validated and reliable using self-report surveys conducted electronically. The written informed consent was integrated into the first section of the online survey; all participants were given the option to consent before proceeding to the measures. We collected demographic data, which included educational attainment, age, gender, and chronic diseases.
Stephenson Multigroup Acculturation Scale (SMAS)
The SMAS is a validated, 32-item questionnaire, applicable across ethnic groups, with two subscales that assess the extent to which respondents feel immersed in the dominant culture (DSI) and nondominant culture (ESI) (Gamst et al., 2012). DSI has 15 items while ESI has 17 items. Responses to each item were based on a four-point Likert scale: 1 = False, 2 = Partly False, 3 = Partly True, and 4 = True. Scores were determined by averaging the ratings of participants on each subscale item and dividing them by the number of subscale items in order to obtain a subscale mean. Mean scores for each subscale ranged from 1 to 4, with higher scores indicating greater ESI or DSI. SMAS has a Cronbach’s alpha of 0.97 for ESI and 0.90 for DSI (Gamst et al., 2012).
Health-Promoting Lifestyle Profile-II (HPLP II)
The HPLP-II measures lifestyle preferences across six domains of nutrition, physical activity, stress management, interpersonal relations, spiritual growth, and health responsibility (Walker et al., 1987). This scale has been used among African populations (Panebianco-Warrens et al., 2014). There are 52 items in this validated scale, all of which employ a 4-point Likert response format. The mean of the six subscale scores were calculated, ranging from 1 to 4, with higher scores indicating a better lifestyle pattern for the specific domain (Walker et al., 1987). The alpha coefficients for the subscales ranged from 0.793 to 0.872 (Walker et al., 1987).
Short Form-12 Version 1 (SF-12)
The SF-12 measures physical (PCS) and mental composite scores (MCS) (Farivar et al., 2007; Ware et al., 2002). The SF-12 has been used in diverse populations, and is weighted and summed to provide easily interpretable scales for physical and mental health (Farivar et al., 2007; Larson, 2002; Soh et al., 2021; Ware et al., 2002). Scores range from 0 to 100 based on responses to twelve questions, where 0 represents the worst health status and 100 represents the best health status. Summary scores for the PCS and MCS were calculated using oblique (correlated) instead of orthogonal (uncorrelated) scoring to be consistent with current studies using the SF-12 (Farivar et al., 2007). Reliability scores for the PCS ranged from 0.88 to 0.89 and between 0.76 and 0.78 for the MCS (Farivar et al., 2007; Soh et al., 2021; Ware et al., 2002).
Analyses
Data were extracted from the online survey and collated using encrypted Excel spreadsheets. Data cleaning was conducted for any missing data, coding inconsistencies, and outliers (Kwak & Kim, 2017). The SPSS version 25 and Mplus version 8 were utilized for statistical analyses. Demographic information was analyzed using descriptive statistical methods, including percentages, means, and standard deviation. With the bidirectional relationship between ESI and DSI, path analyses were conducted utilizing the Mplus software to analyze the research questions. The endogenous variables in the path diagram (see Figure 1) were connected by unidirectional arrows, representing the standardized path coefficients. Each β coefficient can range from −1.0 to +1.0, indicating the strength and direction of the predictive relationships between the variables. The path model was validated through Mplus checking for discriminant validity, convergent validity, and internal consistency reliability of each variable by composite factor analysis.
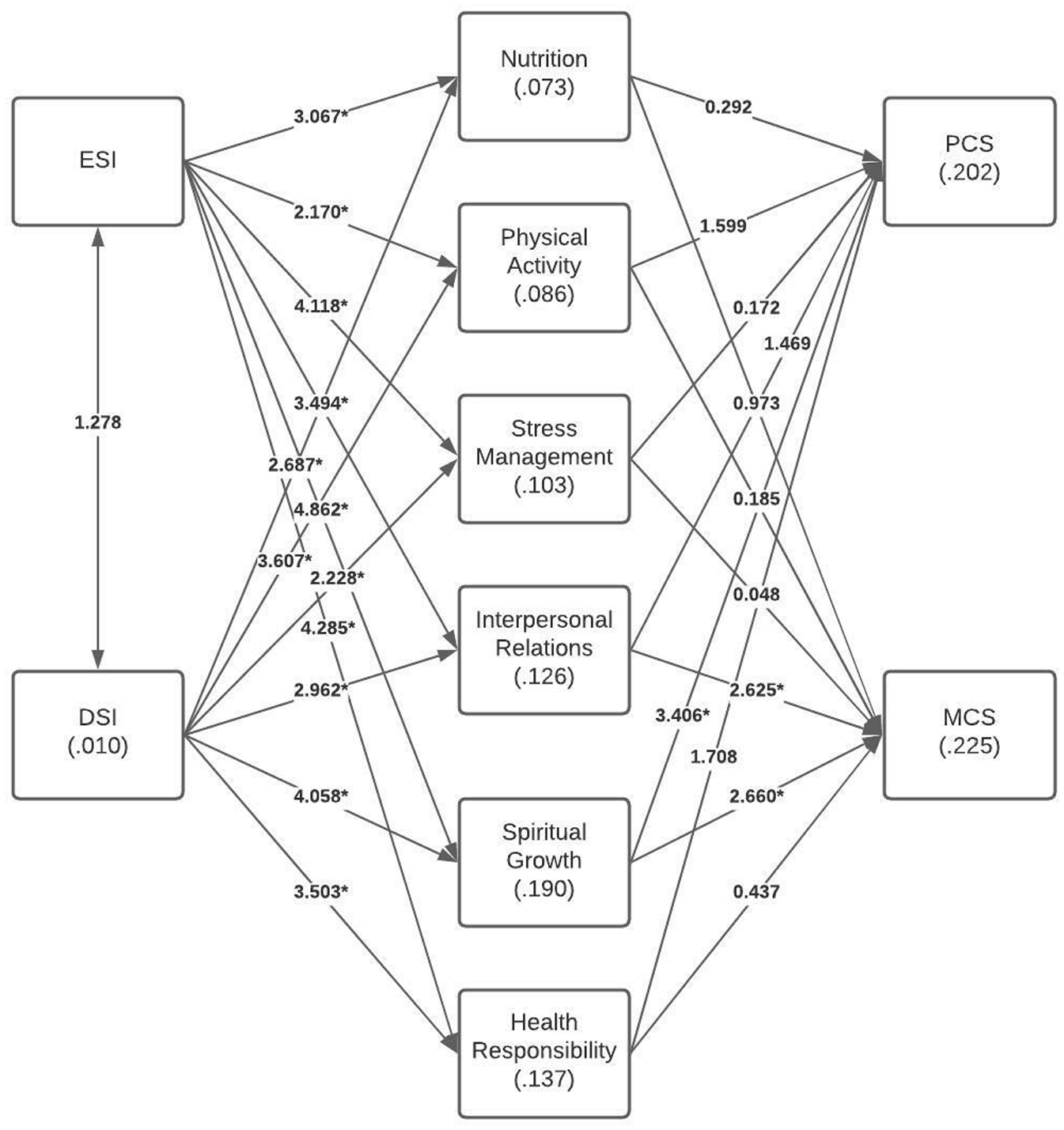
Observed R-squared values of endogenous variables and bootstrapped t-statistics of each path of the path model.
The minimum effect size to indicate a valid model is R2 ≈ .10, meaning that about 10% of the variance in the dependent variable is explainable (Hair et al., 2016). The research questions were tested by evaluating the statistical significance of each β coefficient after bootstrapping using the Monte Carlo method. The mean and standard error (SE) of each β coefficient were computed and t-tests were conducted to determine if the mean value of each β coefficient is significantly different from zero at the .05 level of significance (where t = β/SE). The hypotheses were supported if p < .05 for the path coefficients. All inferential tests were performed at the 95% level of confidence (p < .05).
Results
There were 198 individuals recruited for this study. However, 37 participants did not complete any of the survey items so these records were removed from the dataset so the study sample size was 161. No missing data and outliers were noted. Validity and assumptions of linearity, causal closure, and unitary variables were met. Multicollinearity was evaluated and none of the correlation coefficients were above the cut-off of .80 or .90 (Pallant, 2010).
Based on Table 1, 77.7% of participants were 25–54 years of age. Majority were female (63.4%). All but 5% had an education beyond secondary school; no one was at the primary level. The majority were married (65.8%) with 21.7% who was never married and employed full time (64%) with 19.3% who were students. There were 44.7% who reported having an annual net household income of $75,000 or greater. The majority had health insurance (78.3%) and hypertension was the most reported chronic disease (23.6%).
Frequency Counts and Percentages for Demographic and Health-Related Data on the Study Sample (N = 161).

Note. Two participants selected the marital status choice of “other” and then stated in the text field that they were “single.” The percent values do not add up to 100 for the variable of current medical condition because a study participant could have had more than one medical condition. The zip code zones were retrieved from https://www.unitedstateszipcodes.org/. The zones used in the table are categorized by the first digit in the five-digit zip code.
There were 33.5% who lived in the United States for over 15 years. Participants were represented in all geographic areas with most in Zone 7 at 29.2% (Arkansas, Louisiana, Oklahoma, Texas) and Zone 2 at 23.6% (District of Columbia, Maryland, North Carolina, South Carolina, Virginia, West Virginia) (United States Postal Service, 2021).
Based on Table 2, the means for acculturation, ESI and DSI, were 3.17 and 3.11 out of 4, respectively. Means for the six domains for health-promoting lifestyle ranged from 2.31 (physical activity) to 3.14 (spiritual growth) out of 4. The physical and mental health scores were 54.91 and 53.56 out of 100, respectively.
Measures of Central Tendency and Cronbach’s Alpha Coefficients of the Subscales Derived from the Survey Instruments for the Study Sample (N = 161).
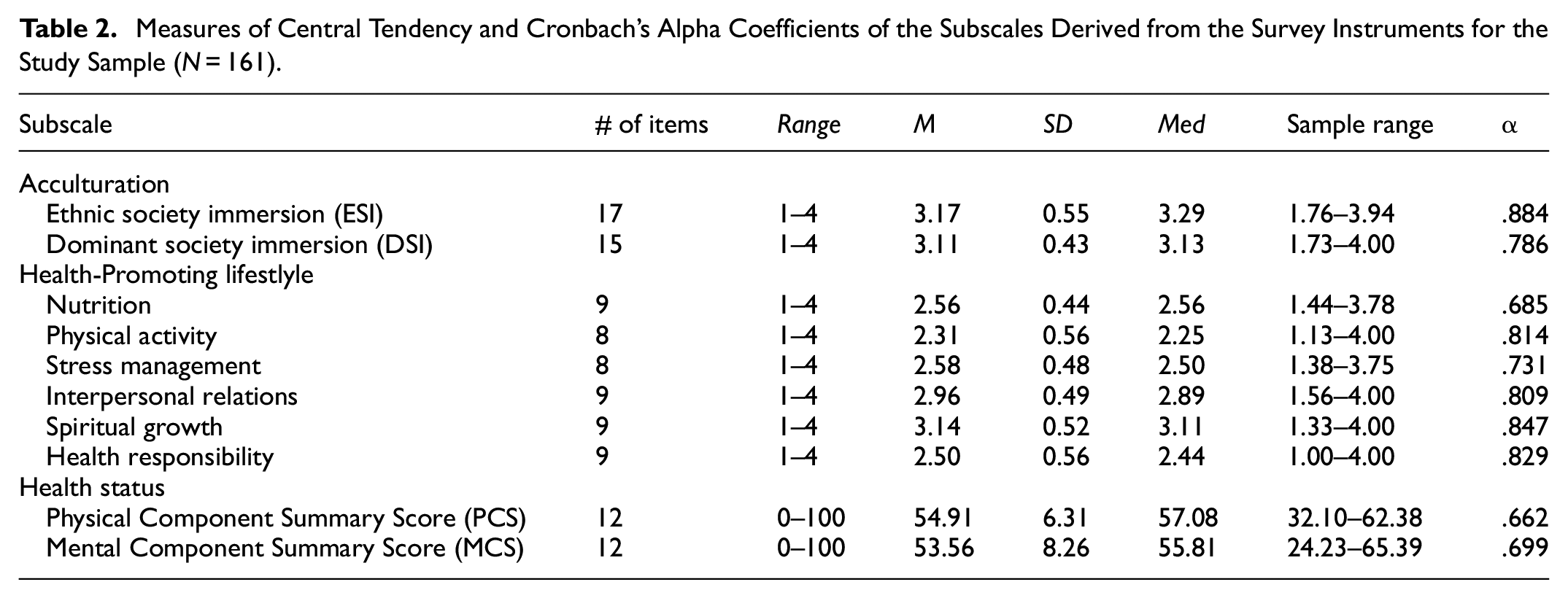
Table 3 presents the standardized coefficients, standard errors, t-statistics, and p-values for the observed (sample) as well as the bootstrapped (5000 iterations of sampling with replacement from the observed data) standard errors, 95% confidence interval for the standardized coefficients, t-statistics, and p-values of the bootstrapped data. Figure 1 includes the bootstrapped R2 values and t-statistics of the bootstrapped path coefficients. The bootstrapped R2 values ranged from 1% to 23%. T-statistics greater than 1.96 are statistically significant at the 95% level of confidence (p < .05).
Observed and Bootstrapped Standardized Coefficients and Tests of Significance for Path Analysis Addressing Research Questions 1 and 2 (N = 161).

Note.β = Standardized Coefficient; SE = Standard Error of Standardized Coefficient; CI = Confidence Interval; t = t-statistic (β/SE); p = p-value of t-statistic.
p < .05.
In response to the first research question (based on Table 3 and Figure 1), ESI was a statistically significant predictor of all six health-promoting lifestyle domains. All of the β coefficients were positive, indicating that an increase in ethnic society immersion was associated with increases in each of the six health-promoting lifestyle variables. The β coefficient for spiritual growth was largest of the six significant path coefficients (β = .35, SE = 0.07; p < .001), indicating that ESI had the greatest predictive value on spiritual growth while the lowest was physical activity (β = .16, SE = 0.08; p = .033). DSI was also a statistically significant predictor of all six health-promoting lifestyle domains with all of the β coefficients being positive. The β coefficient for spiritual growth was also largest of the six significant path coefficients (β = .30, SE = 0.07; p < .001), indicating that DSI had the greatest predictive value for spiritual growth with stress management as the least (β = .19, SE = 0.07; p = .012).
For the second research question, one path coefficient related to health-promoting lifestyle was statistically significant for PCS. Spiritual growth had a positive predictive effect on PCS (β = .38, SE = 0.10; p ≤ .001), indicating that increases in spiritual growth were associated with increases in physical health. Two path coefficients related to health-promoting lifestyle were statistically significant for MCS. Interpersonal relations was positively associated with MCS (β = .30, SE = 0.10; p = .004) suggesting that participants who reported better interpersonal relations experienced greater mental health state. Spiritual growth was also significantly correlated with MCS (β = .34, SE = 0.11; p = .001) and had the larger β coefficient compared to interpersonal relations.
Discussion
This study presents demographic data consistent with sparse published literature for Nigerian Americans (Ekwemalor & Ezeobele, 2020; Obichi & Dee, 2022; Obisesan et al., 2017) and appears to be representative of the Migration Policy Institute (Migration Policy Institute, 2015) report in terms of employment and education. According to this report, Nigerian Americans are highly educated and contribute meaningfully to the economy. This is important because literacy including English proficiency play a key role in acculturation and significantly influence health risk perceptions (Splain & Khambaty, 2024).
Compared to existing literature, this study sampled Nigerian Americans across all U.S. postal zip codes acquiring a representative sample. Existing literature on detailed demographics and acculturation studies among Nigerian Americans are deficient and when available, are mostly not recent (Adewunmi, 2015; Akinde, 2013; Ike-Chinaka, 2013; Ndika, 2013). Without current, relevant information, the Nigerian American population can remain medically underserved.
Health Status
Based on the SF-12 physical and mental health scores (PCS and MCS), participants scored an average of 54.91 and 53.56, respectively. Reportedly, scores at 50 or lower on the PCS may indicate a physical condition while a score of 42 or lower on the MCS may indicate clinical depression (Ware et al., 2002). The physical and mental health status of Nigerian Americans meet the cut points for PCS and MCS.
Hypertension was the most reported chronic condition (23.6%) in this study consistent with previous findings among similar populations but with lesser proportion of prevalence (Akinlua et al., 2017; Commodore-Mensah et al., 2014; Obisesan et al., 2017). Among the general African American population, approximately 51.1% had hypertension (Ostchega et al., 2020, April). It is possible that retaining healthy, cultural dietary and physical practices could be protective factors among Nigerian immigrants.
It has been reported that as the years of immigrant stay increases, the degree of health problems also increases (Constant et al., 2017). This observed phenomenon is generally referred to in the literature as the healthy immigrant effect and acculturation is regarded as a possible cause (Constant et al., 2017; Ichou & Wallace, 2019). It is important to be able to target health promotion, disease prevention, and treatment strategies specific to Nigerian Americans to prevent health status erosion, minimize healthcare disparity, and improve quality care especially taking into account their engagement into the U.S. healthcare system (Obichi & Dee, 2022).
Acculturation
Acculturation consists of two components: ESI or immersion into ethnic society and DSI or immersion into dominant society. The degree of immersion in either or both components could indicate the acculturating strategy of the population (Berry, 1992, 1997, 2012; Gamst et al., 2012). The four acculturating strategies articulated (Berry, 1992, 1997, 2012) are separation (being traditional), assimilation (becoming immersed in the new country of residence), marginalization (being alienated), and integration (becoming bicultural). Although there are no established cut points in the literature, study findings suggest that Nigerian Americans are adapting the acculturation strategy of integration with a high mean ESI score of 3.17 and a comparable, high mean DSI score of 3.11. Individuals and groups are more successful when immersed in both the ethnic and dominant cultures (Berry, 2017). Berry further explained that this might be associated with a greater personal sense of well-being, intercultural relations, and greater sociocultural competence and adaptation. A review of African-born migrants noted that adopting to host culture (e.g., DSI) and maintaining home culture (e.g., ESI) were correlated with social relations and economic outcomes, while discrimination was associated with home culture adoption and healthcare utilization was associated with host culture maintenance (Deslandes et al., 2024).
The comparative analysis of acculturation’s impact on health across diverse immigrant groups in the United States reveals both shared and distinct findings across studies. This study on Nigerian Americans, along with some others (Deslandes et al., 2024; Obichi & Dee, 2022; Sanchez et al., 2022; Xu et al., 2023), demonstrate a significant influence of acculturation on health-promoting behaviors and overall health outcomes. The studies collectively affirm the complexity of societal integration, highlighting that the extent and nature of acculturation can variably affect health. However, differences emerge in the population focus, health domains studied, and methodological approaches.
Health-Promoting Lifestyle
Based on study findings on the HPLP domains, physical activity among Nigerian Americans had the lowest mean. It was noted that physical activity decreased with acculturation for U.S. men of different ethnicities (Zan & Fan, 2017). This was supported by another study (Joseph et al., 2017) demonstrating that higher levels of acculturation predicted low physical activity. Among Nigerian Americans, it is important to consider cultural perceptions and understanding of physical activity while incorporating culturally sensitive approaches (Ibe-Lamberts et al., 2017; Ibe-Lamberts et al., 2018; Turk et al., 2014; Webb et al., 2024). For example, study findings (Hurston et al., 2024) reported that African immigrants preferred their body mass index to be at the normal or overweight range, likely influenced by cultural beliefs that larger body sizes are viewed as signs of prosperity and health.
Spiritual Growth and Acculturation
For the first research question, all of the health-promoting variables were significantly associated with ESI and DSI with spiritual growth having the largest predictive influence on ESI and DSI. Spiritual growth also had the highest average among all the health-promoting lifestyle domains. Many Nigerian Americans used religion as their key source of support, relied on their faith in God, especially while coping with the stresses of immigration and acculturation (Adewunmi, 2015). Nigerian Americans used religious retreats as a stress management strategy (Ekwonye et al., 2018). Even in the United Kingdom, Nigerian immigrants integrated religious and cultural aspects in their healthcare practices which could influence mainstream healthcare utilization (Onyigbuo et al., 2016). Nigerian churches in the United States make it possible for Nigerian Americans to find a place not only for worship but also to gather together and participate in rituals and other events that help them feel united as Nigerians, an enhancement to those who feel more strongly toward ESI, providing the sense of having a home away from home (Onwumelu, 2020). It is also known that churches assist Nigerian Americans with DSI by providing much-needed support for acculturation and citizenship. For example, in various communities, religious organizations and leaders advocate for Nigerians by assisting with the Immigration and Naturalization Service forms, providing a source of sponsors for immigrants, and also officiating at marriage ceremonies.
Spiritual Growth and Health Status
In response to the second research question, spiritual growth was also statistically significant for physical and mental health (PCS and MCS). Searching the literature further to investigate the relationship between spiritual growth and physical health with an emphasis on the Nigerian culture, a study of spirituality and adherence to HIV therapy regimens by Nigerians (Ayuk et al., 2017) indicated a small, yet significant, correlation between spirituality and adherence (r = 0.265; p < .01). The odds ratio from the study indicated that every unit rise in spirituality score yielded a 1.3 times increased likelihood to adhere to HIV treatment regimen. Systematic reviews on international studies indicated that spirituality and religiosity promoted outcomes of both physical and mental health among other ethnicities (Litalien et al., 2021; Moreira et al., 2020) and that religion or spirituality can be conceptualized in three ways: as a (a) coping mechanism, (b) source of social support, and/or (c) tool for behavioral control (Litalien et al., 2021). Although much of the published research is geared towards populations other than Nigerian Americans, the literature does indicate positive associations between spirituality and both physical and mental health among various immigrants. This underscores the importance of spirituality in health which may even be more likely among Nigerian Americans due to their strong affinity to religion (Ekwonye et al., 2018; Onwumelu, 2020) which helps explain why spirituality had a predictive value to PCS as well as MCS. In recent studies, although Nigerian American men felt that depression was not something that existed among Nigerians (Ezeobele et al., 2019), Nigerian American women preferred the clergy for treatment of depression instead of healthcare professionals (Ezeobele et al., 2010). It is important to be able to consider the values, beliefs, and preferences of immigrant populations when targeting health promotion and treatment approaches for best success (Kerrigan et al., 2022).
Interpersonal Relations and Mental Health
Findings for the second research question also showed that interpersonal relations was a significant predictor for mental health. Studies on other races supported the influence of interpersonal relations on mental health (Chai & Dibb, 2013; Yoon et al., 2012). Among Nigerian Americans, although some researchers examined aspects of mental health (Chaumba, 2011; Ezeobele et al., 2010; Ezeobele et al., 2019), studies looking into the predictive influence of interpersonal relations on health status remain few. For example, African immigrants reported physical and psychological symptoms of stress and sought mentors as well as used both individual- and group-oriented coping strategies (Adewunmi, 2015; Covington-Ward et al., 2018). In another older study, increasing acculturation, social support, and self-esteem among Nigerian Americans were found to decrease their isolation and improve their mental health (LaFleur, 2010).
Overall, there are still few, current studies published among Nigerian Americans. Further investigations into their health-promoting lifestyles and health status are necessary especially in devising targeted health promotion, prevention, and disease management strategies specific to the needs of this population to facilitate culturally congruent care. Nigerian Americans are a distinct cultural group and the United States is no longer a homogenous nation (United States Census Bureau, 2021, August 12). Health-related data need to reflect the health status of each ethnic group. Aggregating all African Americans as one diminishes salient information that can facilitate improved adaptation among specific ethnic groups (Deslandes et al., 2024).
Implications
Health policies and interventions geared toward the Nigerian immigrant population in the United States could make use of study findings (Adekeye et al., 2014) especially the elements of spirituality and religion among Nigerian Americans, to enhance the practice of preventative care. Acknowledging and incorporating patients’ spiritual needs could facilitate the effectiveness of healthcare delivery. Strategies and activities associated with spirituality and religion could be adopted by policymakers and practitioners for use in health education to increase adherence to treatment regimens. Leaders in houses of worship within the Nigerian American community could be recruited to deliver salient information or targeted to assist in reaching out to the community, while localized worship facilities can be accessed and maximized to help facilitate provision of preventative health education and disease management programs. For example, hypertension was reported by almost one quarter of the participants in this study; blood pressure and other health screenings and education could be performed by health professionals or trained community health workers of Nigerian descent at community churches or incorporated in other social events since the domain of interpersonal relations was also a significant predictor among Nigerian Americans.
For research implications, study findings provide foundational information for future interventional and longitudinal designs. This could include studies investigating changes in the association between acculturation, health-promoting lifestyles, and health status over time since acculturation is not consistently positively correlated with better health behaviors. Understanding that spirituality is a source of support and resilience, conducting intervention studies to evaluate the role of spirituality and religion as well as interpersonal relations in facilitating health intervention programs among Nigerian Americans could be highly beneficial. Future studies could elucidate ways to improve health-promoting lifestyle and health status (physical and mental health) among Nigerian Americans.
Limitations
This study was limited to a convenience and snowball sample of first-generation Nigerian Americans, majority are female, and may have had experiences different from other Nigerians who did not participate, thereby limiting generalization of study findings. Most participants were recruited from larger cities where immigrants are more densely populated. Similar findings may not have been observed for Nigerian Americans who live in rural areas. Self-reporting is another limitation of this study which can introduce bias into study findings. It is, however, notable that participants were represented in all zones in the United States.
Conclusions
Although the Nigerian American population continues to grow, acculturation studies specific to this population remain sparse and many are not current. To the best of our knowledge based on published literature, this is one study among Nigerian Americans that measured DSI and ESI as key components of acculturation beyond its proxy measures such as length of stay which provides only a unidimensional understanding of acculturation.
Using path analysis in a representative sample of Nigerian Americans, a key significant finding in this study was the relationship found between spirituality with not only DSI and ESI but also physical and mental health. No other health-promoting lifestyle domain showed these significant correlations. Interpersonal relations was also found to be a significant predictor of mental health. These are novel contributions to the literature that advances the science of acculturation among Nigerian Americans and potentially, other Nigerians who immigrated to other countries. Study findings provide foundational information that pave the way for further research and important health promotion and disease prevention and management programs that are culturally relevant to this population toward better health outcomes and healthcare equity.
Footnotes
Acknowledgements
We appreciate all the community leaders and research participants who took the time to complete the surveys despite the pandemic.
Ethical Considerations
This study was deemed exempt by the Institutional Review Board protocol #1605444 at University of Nevada, Las Vegas. All participants consented to this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the University of Nevada, Las Vegas, School of Nursing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.