
Abstract
The accessibility of oral health care services is one of the determinants of oral health in Saudi Arabia, very little is known about the geographic distribution of dental health care services, or spatial dimensions related to dental service access (travel time, distance, etc.), especially within metropolitan areas. Therefore, this study used known community profile indicators to assess the geographic accessibility of existing dental services in the city of Al Madina, Saudi Arabia. Geographic coordinates were identified for 33 primary clinics and 48 private clinics. The Al Madina metropolitan area, containing 1,105,465 residents, was divided into 103 districts, in accordance with the 2010 population census. Clinic locations and the number of dentists at each clinic were integrated with the city’s population census data within each district, using a geographic information system. The city metropolitan area consisted of 103 neighborhoods with a total of 1,105,465 residents (715,980 Saudis and 389,485 non-Saudis). Thirty-three fixed public primary dental clinics and 48 private dental clinics were geocoded within the municipality. The city exhibited an overall practice-to-population ratio of one dental clinic per 13,647 residents. More clinics (55% public and 58% private) were located within 3 km of the city center. Notably, 8% of the population was located more than 10 km from the city center. A total of 37% of the city’s districts were identified as areas of relative need; these were primarily located in peripheral metropolitan areas. This study depicts a clear example of the inverse care law, where people living in outer metropolitan areas have less spatial access to dental care than those living in inner metropolitan areas.
Key messages
This study provided models to visualize the maldistribution of dental practices, which can facilitate understanding, planning, monitoring, and allocation of resources to disadvantaged areas.
This study is the first of its kind conducted in Al Madina, Saudi Arabia.
Introduction
Globally, a fundamental objective of health care systems is to ensure that individuals have access to essential high-quality health services based on need, rather than the ability to pay (World Health Organization [WHO], 2011). The few studies that have examined dental utilization patterns in Saudi Arabia showed that they varied among different sub-population. A recent study by Orfali and Aldossary (2020) revealed that the prevalence of routine attendance ranged from 8.6% to 11.5%, while dental emergency and routine treatment attendance ranged from 48% to 63%. Adherence to a need-based strategy in Saudi Arabia (SA) requires exploration. Currently, most dental services in Saudi Arabia are delivered through publicly funded primary dental services, which include only emergency and basic treatment; additionally, they provide limited coverage of complex treatments, particularly for low-income families (Almalki et al., 2011). These services originated in environments with high dental disease burdens and have required adaptation to the changing burden in recent years. Nationality is an important factor because Saudis enjoy free government-paid full dental health care coverage, while all expatriates are treated in private dental clinics, which are restricted to those who are insured or can afford treatment. With the absence of insurance in a private market, utilization rates are expected to be low.
Notably, a universal “one-size-fits-all” model is no longer regarded as appropriate, because it is clear that disease and suffering are not evenly distributed. Individuals with a low socioeconomic status—at the margins of society—suffer far higher burdens of disease than others (Kassim et al., 2019). Saudi Arabia’s complex geographic and demographic spread requires novel systems to address the health needs of socioeconomically disadvantaged individuals, as well as those who are distant from city centers; these individuals often endure the greatest overall suffering related to disease.
Researchers have identified two separate components of access: economic (the ability to afford health care services) and physical (the ability to overcome costs associated with distance) (Cheng et al., 2012). Previous studies have used various methods to examine health care service access and utilization, including geographical information systems (GIS) (Mushonga et al., 2017). Put simply, “GIS” is a computer-based system that analyses and displays geographically referenced information. Currently, GIS plays a major role in evaluating and quantifying the relationships between spatial and temporal trends of health-related variables, population, and environmental risk factors on different geographical scales.
Very little is known about dental health care service distribution or geographic access factors (travel time, distance, etc.) within Saudi Arabia metropolitan areas. Murad (2006, 2008, 2014, 2018) used GIS to measure primary and private health care services’ spatial accessibility in Jeddah and found that certain areas, including the central and northern districts, had poor accessibility to health centers. No studies have been conducted elsewhere in the Kingdom. A clear understanding of service distribution is critical to address health inequality, which, notably, can be directly related to barriers preventing access to health care (Alonge & Peters, 2015). Therefore, this study used known community profile indicators to assess the geographic accessibility of existing dental services in the city of Al Madina, Saudi Arabia, to test the hypothesis that primary and private dental clinic distributions are patterned by population densities (Saudi vs. non-Saudi).
Materials and Methods
Study Design and Setting
This was a cross sectional descriptive study conducted at Al Madina, SA. Al Madina is one of the largest administrative regions in the KSA and is highly significant because of its large population and the breadth of socioeconomic diversity in its residents. The strength of the economy and ongoing population growth thus place increasing strain on the city’s health care system (Al-Madina Al-Monawarah Authority, 2000). The Al Madina urban catchment area covers 293 km (General Authority of Statistics [GAS], 2017), and has a population of 1,105,465, with a 2.3% growth rate over the previous 3 years (GAS, 2017). This increase in population might be partially attributed to internal and external migration. Al Madina comprises 3.5% of the total Saudi population and is the third-largest city in the western region (GAS, 2017). Notably, the city has undergone dramatic spatial expansion since 1999 (Al-Madina Al-Monawarah Authority, 2000).
Framework Development Database
Census collection district
The Al Madina municipality was divided into 103 census collection districts (CDs). Each CD was assigned a unique identifier and its geographical boundaries were obtained from census data (GAS, 2017).
Population data
The population of each CD within the metropolitan area was obtained from the most recent (2010) census data available at the General Authority website (GAS, 2017).
Dental practice locations
The location of all fixed dental service clinics (both private and public) was obtained from the Department of Health. Each service location was geocoded based on the exact coordinates.
Mapping
To build this application, the present study collected the data described above, entered it into the GIS to form the database, and captured two major baseline maps, then overlayed them with relevant non-spatial data. These maps encompassed the geographical boundaries of each CD in Al Madina (Shapefile format) and all fixed dental service clinic locations. The non-spatial data included the number of people living in each CD, the number of dental chairs, and the number of dentists. As a computational approach to health planning, GIS is not new (Aronoff, 1989); however, its application to dental planning is novel. Notably, the GIS approach was tested using the data from this particular city, but was designed to be universally applicable.
To assess geographic accessibility, buffers were created to quantify the population within catchment areas. Buffers with radii that increased in 3 to 5 km increments were produced around the city center (the main business and commercial areas) and used as proxies for driving distances (Almado et al., 2013; Kruger et al., 2011, 2012; Tennant et al., 2013). Catchment areas with radii of 0.5 to 3 km were previously agreed upon for all transportation modes (Currie, 2010; Horner & Mascarenhas, 2007; Rocha et al., 2015). The use of buffers enabled quantifying population numbers (by nationality) and the number of primary dental clinics within each catchment area. High-precision analyses were conducted on the dentist-to-population ratio and practice-to-population ratio for each catchment area; these served as clinic distribution density measurements. Nationality was included as a factor because it determines the accessibility to different type of dental health care facility (public vs. private). In this context, “area of need” typically relates to any area in which there is a lack of dental clinics.
Statistical Software
All data mapping was performed using Quantum GIS (Redlands, CA, USA), version 2.4 (open-source geographic information system, licensed under the GNU General Public License). The mapping was performed at a resolution that allowed high-precision analysis of the service distribution to the population, based on the CD. Excel 2016 software (Microsoft Corp., Redmond, WA, USA) was used to tabulate the data. These methods were consistent with past studies that relied solely on descriptive statistics (Kruger et al., 2011; Tennant et al., 2013; Tennant & Kruger, 2014; Yuen et al., 2018).
Ethical Considerations
Approval was obtained from the Taibah University College of Dentistry and Hospital Research Ethics Committee (TUCDHREC 20170404AAlsharif) before study initiation, and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies (Von Elm et al., 2007).
Results
The city metropolitan area consisted of 103 neighborhoods with a total of 1,105,465 residents (715,980 Saudis and 389,485 non-Saudis). Thirty-three fixed public primary dental clinics and 48 private dental clinics were geocoded within the municipality. The city exhibited an overall practice-to-population ratio of one dental clinic per 13,647 residents.
Current Distribution of Primary Dental Clinics
More than half (55%) of clinics were located within 3 km of the city center, and more than 80% were within 6 km (Figure 1, Table 1). In comparison, less than 40% of the population was located within three km of the city center, and more than two-thirds (70%) were within six km. Approximately 29% of the population lived within 6 to 15 km of the city center, and only six primary dental practices were located within the latter mentioned areas (Table 1).

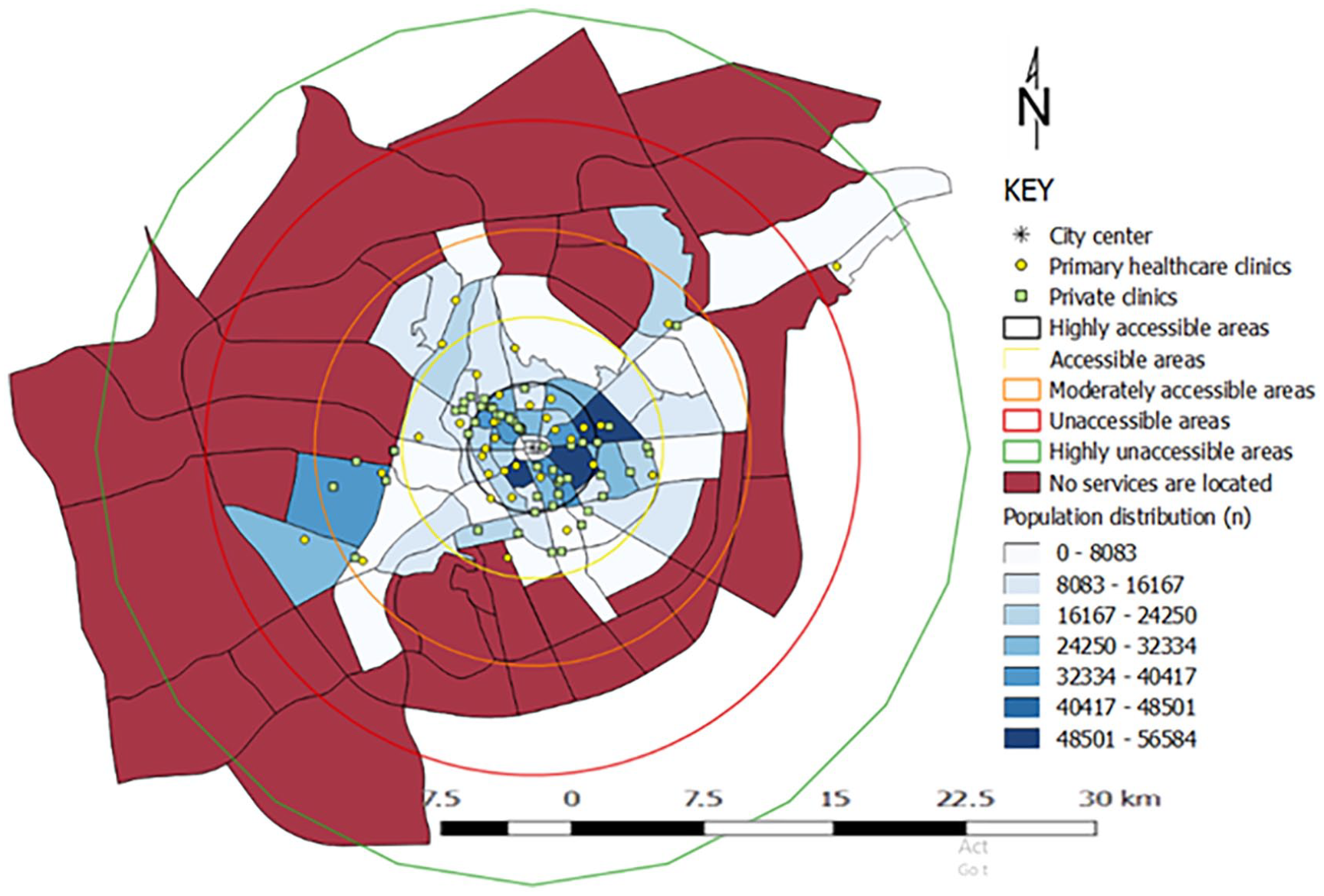
A high-resolution image shows the distribution of population per district and fixed primary dental clinics based on accessibility areas in Al Madina, KSA.
Primary Dental Practice-to-Population and Dentist -to-Population Ratios at Various Distances From the City Centre in Al Madina, KSA.
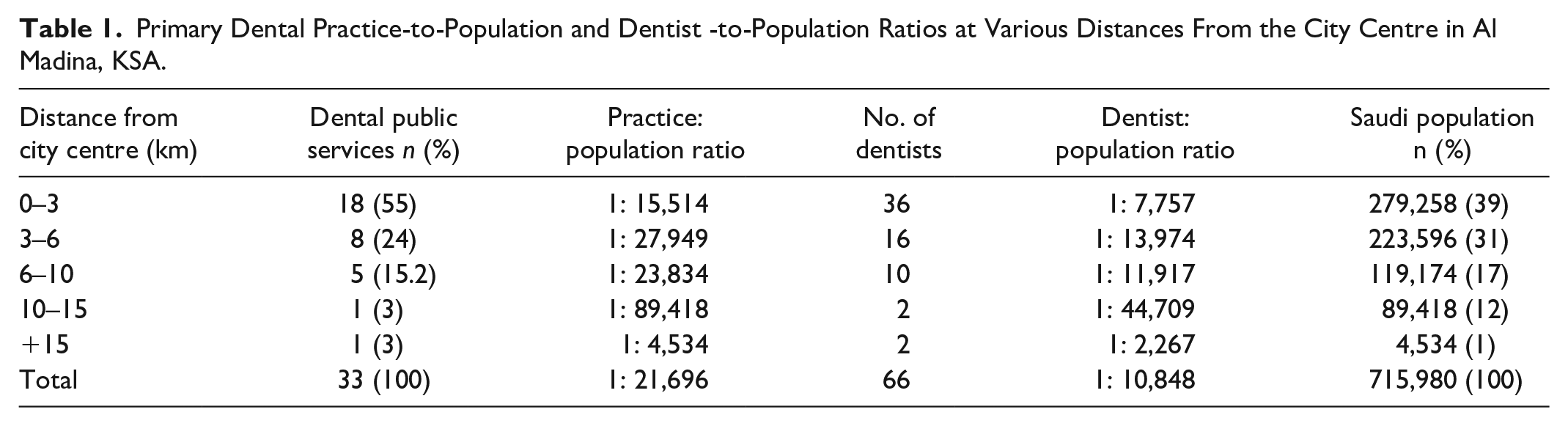
The smallest practice-to-population and dentist-to-population ratios were observed within a three km radius of the city center (1:15,514 and 1:7,757, respectively). The greatest ratios occurred at a distance of 10 to 15 km, which revealed a practice-to-population ratio of 1:89,418 and a dentist-to-population ratio of 1:44,709. This was approximately 6-fold higher than the ratio of the inner metropolitan area (Table 1).
Distribution of Private Dental Clinics
Forty-eight private dental clinics in Al Madina served 1.1 million people; the practice-to-population ratio was 1:23,030 (Table 2). There was an unequal distribution of private dental clinics in Al Madina (Figure 2), with 85% of private dental services located within 6 km of the city center. Of these, 58% were located within 3 km (Figure 2, Table 2). The central areas included 28 private clinics for 538,418 people (279,258 Saudi and 259,160 non-Saudi residents), and exhibited the lowest population-to-practice ratio (19,229:1) (Table 2). The population-to-practice ratio of each subsequent area increased exponentially.
Private Dental Practice-to-Population Ratio at Various Distances Out From the City Centre in Al Madina, KSA.


A high-resolution image shows the population distribution by district, private dental clinics and accessibility areas in Al Madina, KSA.
A higher percentage of the Saudi (66%) than non-Saudi populations (39%) lived within the central areas, which exhibited a practice-to-population ratio of 1:19,229 (Table 2). In contrast, nearly 130,000 people who lived more than 10 km from the city center had no private dental clinic service (Figure 2). Those areas included a lower proportion of Saudi citizens (8.8%) and higher proportion of non-Saudi residents (13%).
Areas in Need
No clinics were located more than 15 kms from the city center (Figure 3). A total of 37% of the city’s districts were identified as areas of relative need; these were primarily located in peripheral metropolitan areas.
A high-resolution image showing areas with no dental services in Al Madina, KSA.
Populations in the outer metropolitan areas had no spatial access to public or private dental health care. Significantly, 8% (more than 87,000 people) lived in underserved areas (Table 3). Half of those individuals lived 10 to 15 km from the city center; approximately 29% of the population was located 6 to 10 km from the city center (Table 3).
Population Living in Areas Where No Services Are Located.

Discussion
This study examined primary and private dental practice spatial accessibility in Al Madina. The key findings indicated that primary oral health care services were concentrated within the central districts, where opportunities (e.g., employment) and facilities (e.g., public services) are most readily available. More than two-thirds of the population lived in highly accessible or accessible areas, which was consistent with the hypothesis that primary dental clinic distribution is patterned by population densities. Yet, high practice-to-population ratios were observed in these highly accessible (1:15,514) and accessible (1:27,949) areas.
Significant disparities were found in primary dental service coverage, with clinics more sparsely distributed in peripheral districts than in central districts. Consistent with this observation, Murad (2014) concluded that several peripheral districts north of Jeddah were not well served by health centers; they were also typically socio-demographically disadvantaged (with low access to essential services), and had a greater disease burdens (Alsharif et al., 2016; Peres et al., 2013; Petersen et al., 2005). These findings suggest that the inverse care law still exists, with practice locations determined by factors other than need (Hart, 1971). The impact of this disparity is not limited to a greater prevalence of dental and oral disease; it extends to higher morbidity and mortality rates.
The dentist-to-population ratio is a widely accepted measure of workforce outcomes (Australian Bureau of Statistics [ABS], 2006; Spencer et al., 2003; Tennant et al., 2013). The city exhibited an overall dentist-to-population ratio of 1:10,848 for primary dental clinics, which was higher than the ideal ratio of 1:7,500 suggested by the WHO. In the peripheral metropolitan areas, the dentist-to-population ratio was 1:44,709, compared to about 1:7,757 in the central city areas. Our result is very similar to the situation in other developing countries, where the WHO’s dentist-to-population ratio has not been met. In Kenya, the ratio is 1:150,000 and similarly Malaysia has a dentist to population ratio of 1:6000 (Bohari et al., 2019; WHO, 2016). This quantitative workforce shortage (in peripheral metropolitan areas) likely influences both the utilization level and productive capacity of the health care system. The outer ring districts or new suburbs have better dentist-to-population ratios, but these suburbs are witnessing extensive growth. The region’s future health, economy, and prosperity are largely dependent on the continuous provision of accessible dental health services. Thus, integrated planning is needed to develop the infrastructure, such as roads, transport networks, and primary health services needed when residents move into new communities.
Interestingly, the study identified more private dental practices than primary dental clinics in Al Madina, which indicates that private dental practice plays a major role in meeting dental health care needs. Private dental practice distribution is a critical measure of service supply (Kruger et al., 2011). This study’s geospatial models showed that nearly 49,000 non-Saudi residents and 94,000 Saudi residents must travel longer distances to reach the nearest private dental clinic; an accessibility trend that is noticeably similar to those observed in Saudi Arabia, Australia, Brazil, and New Zealand (Almado et al., 2013; Kruger et al., 2011; Murad, 2018; Yuen et al., 2018). For example, in Auckland, New Zealand, the most peripheral tracts demonstrated a 2-fold sparsity relative to the most central tracts (Kruger et al., 2012). The geospatial models also defined areas of relative need (no service), and showed that private practice viability is often a disincentive for initiating practice in low population density areas, resulting in poor access. Al Madina health planners can use these results to highlight the importance of developing a reform strategy for health service distribution within the structure of each city.
As shown in Tables 1 and 2, each sector (public vs. private) is available to a certain population subset. For example, Saudi and non-Saudi categories provided an indirect measure of a community’s socioeconomic composition within a geographic unit (e.g., suburb). Recently, basic health insurance became compulsory for Saudi nationals working for the private sector and for all non-Saudi nationals working in both public and private sectors. However, dental insurance in Saudi Arabia provides limited coverage within a calendar year (Council of Cooperative Health Insurance, 2016). In addition, dental insurance policies are restricted to certain groups; notably, individuals who have pre-existing medical conditions, who work in certain occupations, or who play high-risk sports are unlikely to be approved for insurance (Council of Cooperative Health Insurance, 2016). Finally, even if they are insured, people living in outlying areas must travel great distances to reach the nearest clinic.
Eight percent of the population in the outer metropolitan areas had no access to public or private dental health care, but residents do not always seek care within their respective suburbs; many work in city centers and can obtain care near their workplace (McGuire et al., 2011). However, health care accessibility is still restricted by multiple barriers that may only affect a subset of the population (e.g., distance or the absence of transportation) (Scheppers et al., 2006). Although research regarding the public transportation infrastructure in Saudi Arabia is lacking, it is believed to be a factor in many settings, including Al Madina. Socioeconomically deprived groups and certain demographic groups (such as the elderly and children) are geographically restricted, because they often must rely on other individuals’ schedules for transport (Tennant et al., 2013).
Study Limitations
Measuring accessibility in terms of distance poses some potential limitations. This study did not consider where patients seek treatment or where public transportation is available. To more accurately determine dental care access, future studies should explore the impact of primary dental care locations on utilization patterns.
The 2010 census data were used in this study. Populations can rapidly shift as a result of certain economic drivers, while dental practices may not move at the same rate. Since they are based on 2010 data, the study findings may not provide a valid assessment of the current circumstances. However, the 2010 population census was the best source of broadly accessible population data. Finally, the practice-to-population ratios, which comprised the bulk of the quantitative analyses, did not consider other factors, such as cultural, social, and economic drivers that might influence health care system productivity.
Conclusion
The study clearly demonstrates that dentist-to-population and practice-to-population ratios vary widely across the city; this is assumed to be consistent with other cities within the kingdom. The models developed by this study to visualize the irregular distribution of dental practices can facilitate understanding, planning, monitoring, and allocation of resources to disadvantaged/underserved areas. This study was the first of its kind conducted in Al Madina and in Saudi Arabia. For a clearer assessment of access inequality, subsequent studies should consider mapping primary dental clinics against specialist distribution and the burden of oral disease.
Supplemental Material
sj-pdf-1-sgo-10.1177_2158244020982970 – Supplemental material for Georeferencing of Current Dental Service Locations to Population Census Data: Identification of Underserved Areas in Al Madina, Saudi Arabia
Supplemental material, sj-pdf-1-sgo-10.1177_2158244020982970 for Georeferencing of Current Dental Service Locations to Population Census Data: Identification of Underserved Areas in Al Madina, Saudi Arabia by Alla Talal Alsharif in SAGE Open
Footnotes
Acknowledgements
The author would like to thank Dr. Estie Kruger, Prof. Marc Tennant and Dr. Saba Kassim for their valuable help. They would also like to thank Lina Alsharif, Sameer Shaheen, Ali Alsharif, and Arwa Namnakani for aiding in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.