
Abstract
The health care system is usually a reflection of the human development and prosperity index of a country. In particular, a sound health care system is generally deemed essential for providing quality service delivery to service users. Pakistan, in this respect, is lagging even after implementing the district health management model of World Health Organization (WHO). In particular, the province of Sindh reports a higher level of dissatisfaction among the service recipients and, therefore, remains a core concern for the concerned authorities. This study, therefore, aims to investigate the levels of employees’ commitment to service quality in Pakistan’s health care sector. A quantitative survey method was adopted to collect data from 315 medical officers working in 43 public-sector hospitals in Sindh, Pakistan. The data were analyzed using the partial least squares structural equation modeling (PLS-SEM) technique and Smart PLS 3 software. Based on cognitive dissonance theory and path-goal theory, the present study investigated the role of leadership styles in influencing commitment to service quality with the moderation of role clarity. The findings lend support to the direct hypothesized relationships of transformational and transactional leadership with commitment to service quality. The study found significant support for all the hypothetical relationships except laissez-faire leadership’s direct link with commitment to service quality. While role clarity was found to moderate the relationships of two leadership styles, namely, transformational leadership and laissez-faire leadership with commitment to service quality, there was no such moderating effect for the relationship between transactional leadership and commitment to service quality. These findings offer useful theoretical and managerial implications on the importance of leadership styles in influencing commitment to service quality and provide the basis for future research.
Keywords
Introduction
Historically, the health care system in Pakistan had remained entirely centralized. In August 2001, Pakistan implemented the World Health Organization’s (WHO) district health management model (Tarimo, 1991). From then onward, the country adopted a decentralized approach to its health care system whereby the responsibility has cascaded to the individual districts, which are managed by the administrative authority of respective district governments. As per the Economic Survey of 2013, Pakistan has 1,207 public hospitals, 5,382 dispensaries, 5,404 basic health units, and 696 maternity and child care units. Previous studies affirm the notion that public hospitals provide poor health services to clients in Pakistan (Mushtaq et al., 2012), and private-sector health care facilities usually offer better service delivery (Mumtaz et al., 2013).
Furthermore, research indicates that the province of Sindh, in particular, reports a higher level of dissatisfaction among the service users of public-sector hospitals (Irfan & Ijaz, 2011) and the very issue has remained a matter of concern for the provincial and federal authorities (Mumtaz et al., 2013; Mushtaq et al., 2012). Similarly, studies such as Khan and Aleem (2014) have also highlighted that the health care sector, in general, and doctors, in particular, face various issues that trigger staff turnover. This, hence, underscores the need for urgent attention to the matter and underlines the public policy significance of the problem.
Employees’ behavior, in the service sector context, plays a crucial role in providing quality customer service and addressing customer needs (Sergeant & Frenlel, 2000; Umrani et al., 2019). The critical issue in the service sector relates to the attitude and behavior of customer contact employees responsible for service delivery (Bowen et al., 1989; Payne & Webber, 2006). In the academic literature, it is commonly referred to as a commitment to service quality (CSQ; Peccei & Rosenthal, 1997). Studies suggest that the quality of interaction between customers and employees and the behavior of service providers considerably influence the perception of service receivers regarding the value of service delivery (Ellinger et al., 2013; Karatepe et al., 2006).
Besides, academics have argued that CSQ remains a challenge for service-based organizations. Alongside other sectors of the economy, the health care sector is also experiencing rapid development in the service orientation and higher benchmarks vis-à-vis customer expectations (Wisniewski & Wisniewski, 2005). Several studies reveal that leaders play an instrumental role in nurturing positive service quality behaviors among their subordinates (i.e., Afsar et al., 2019; Afsar & Umrani, 2019; Ahmad & Umrani, 2019; Clark et al., 2009; Jabnoun et al., 2005). Therein, leaders, while using different styles of leadership, can play a notable role in uplifting the commitment and motivation levels of their subordinates (Dumdum et al., 2002), thus delivering higher customer service. Nonetheless, to what length leaders can also engender individual CSQ in the health care sector, especially in the context of developing countries, is largely unknown. The purpose of this article is, therefore, to broaden the knowledge base by examining the relationship between different leadership styles such as transformational, transactional, and laissez-faire, and employee CSQ, in the health care sector of Pakistan, with the moderation of role clarity.
Theoretical Underpinnings and Hypotheses Development
CSQ
CSQ manifests the willingness and devotion of employees for achieving service quality excellence and optimum customer satisfaction by providing quality service delivery (Clark et al., 2009). The concept of CSQ has primarily emanated from the body of literature, which deals with organizational commitment (Ahmed et al., 2020). For example, Tosi and Mero (2003) have described it as individuals’ attitudes toward work and other surrounding factors. Notably, commitment is crucial at the workplace (Hartline & Ferrell, 1996), and CSQ is imperative for organizations to realize and achieve performance prospects and offer phenomenal customer service (Babakus et al., 2003). Accordingly, service quality is indispensable for service-based enterprises whereby employees play a key role in this regard (Brady & Cronin, 2001) because these organizations consequently rely on their employees’ commitment levels (Paulin et al., 2006). In other words, an individual’s commitment can further nourish his or her devotion to enhancing service quality. Extant literature indicates numerous organizational factors and behaviors influencing employees’ attitude and CSQ across different occupational settings (e.g., Liao & Chuang, 2007). Accordingly, studies report leaders having the potential to foster varying commitment prospects (Chan & Mak, 2014), which may correspond to differentiated employee outcomes. Nevertheless, there is a paucity of research on what bearing different leadership styles may have on enhancing employees’ commitment toward service quality, especially in the health care sector (Clark et al., 2009; Elmadağ et al., 2008).
Leadership
Leadership is an art of inspiration, aimed at the attainment of a common goal (Limbare, 2012). Its focal point is to establish a direction whereby a leader attempts to influence his or her followers to achieve some common objectives (Ahmad & Umrani, 2019; Bass & Riggio, 2006; Long & Thean, 2011). Paradoxically, though, a leader’s role toward individual outcomes is highly regarded. Yet, still, it is arguably less understood across different occupational settings (Perko et al., 2014). Potentially, it may be due to different leadership styles that showcase diverse influence and effects across various occupational contexts (e.g., Howell & Hall-Merenda, 1999; MacKenzie et al., 2001; Parry & Proctor-Thomson, 2002). According to Clark et al. (2009), leadership is “the manner and approach for providing direction, implementing plans, and motivating people” (p. 1). Importantly, transformational, transactional, and laissez-faire are reported as some of the most widely practiced leadership styles for galvanizing employee behaviors and fostering positive outcomes (Afifah & Daud, 2018; Anderson & Sun, 2017; Chang et al., 2019; Chiniara & Bentein, 2018; Cummings et al., 2010; Han et al., 2016; Huertas-Valdivia et al., 2019; Miao et al., 2018; Skakon et al., 2010; Solomon & Steyn, 2017).
Transformational Leadership
Burns (1978) has defined transformational leaders as the one capable of nurturing followers up from their petty preoccupations and rally them around a common purpose to achieve things never thought possible. The transformational style of leadership energizes subordinates and inspires them to work for the responsive achievement of organizational goals. Such leaders focus on developing their followers by focusing on their capabilities, recognition, positive reinforcement, and inspiration while instilling pride and respect among them (Bass, 2000). While working with a transformational leader, subordinates feel trusted and respected, which pushes them to put more effort than usual (Yukl, 1989).
Scholars have empirically reported transformational leadership style to be effective in enhancing employee expectations (Bass, 1985; Cheung & Wong, 2011; Luo et al., 2019; Su et al., 2019) and fostering their values and self-concepts for desirable behaviors and outcomes (Jung & Avolio, 1999). Furthermore, researchers have empirically established strong statistical links between transformational leadership and employee outcomes and behaviors, such as organizational commitment (Acar, 2012), employee performance (Syafii et al., 2015), employee motivation (Deichmann & Stam, 2015), and quality of working life (Kara et al., 2013). Other studies have also drawn attention to the significance of the transformational leadership style in the service sector (Kara et al., 2013; Lee et al., 2011; Luo et al., 2019; Su et al., 2019). Moreover, evidence suggests that leaders with transformational style are more effective in the health care sector (Madathil et al., 2014).
CSQ refers to an individual’s contention regarding an organization’s service quality (Clark et al., 2009). Employees’ CSQ is all the more critical for service-based organizations (Hashim & Mahmood, 2011), where commitment to service delivery can significantly, and often instantly, translate into perceptions about the service quality, in the minds of the service users. Leaders with transformational style have the potential to make employees realize their value and subsequently positively influence their commitment outcomes. Transformational leaders can influence their followers’ self-efficacy (Nielsen & Munir, 2009), which may contribute positively toward organizational goals (Bass & Avolio, 2000; Garcí-Morales et al., 2008), such as improved service quality levels (Clark et al., 2009). This is because transformational leaders often use coaching and mentoring, which enables them to motivate and develop the self-confidence of their followers (Bass, 1998). While studying the health care sector, Hashim and Mahmood (2011) have suggested that leadership styles can be of great significance in fostering employees’ CSQ, including the transformational leadership style. Typically, changing employee attitudes in the public health care sector of Pakistan, which has emanated from the economic upheavals and increasingly rigid bureaucratic norms, is a major concern.
Concern as to what length, leadership style, such as transformational leadership, can continue to yield desired results. Furthermore, given there is a considerable dearth of empirical evidence in the literature on the effects of transformational leadership on followers’ commitment toward service quality, especially when it comes to the health care sector, there becomes a stronger case to examine such effects empirically. Thus, we hypothesize the following proposition:
Transactional Leadership
Critical appraisal of the leadership literature suggests that transactional leadership was once considered one of the most effective leadership style in achieving organizational outcomes (Bass et al., 2003). Burns (1978) has explained transactional leadership as an exchange process whereby a leader provides rewards in exchange for the subordinate’s efforts. Contrary to the transformational style, leaders with transactional style actively shape employee behaviors and outcomes through attractive extrinsic reward provisions in exchange for the desired performance outcomes (Berson & Linton, 2005). In essence, transactional leadership works in contrast to the principles of transformational leadership as it focuses on the exchange of resources and rewards rather than vision and inspiration. Hence, they are opposite ends of a single continuum (Judge & Piccolo, 2004). Transactional leaders establish clear objectives and action plans, offer useful feedback, and responsively extend rewards upon achievements (Afshari & Gibson, 2016; Bass, 1985). Typically the main reason why transactional leadership works well in situations where leaders may lack the ability to foster motivation among subordinates. Instead, the leader uses compensation and rewards, primarily, to fill these gaps in achieving the required outputs (den Hartog & Koopman, 1997).
Studies have underlined transactional leaders’ potential in fostering employee commitment (Chen, 2004) as they focus on contingent rewards that play a crucial role in motivating employees for exhibiting higher service delivery levels (Nguni et al., 2006). Accordingly, the transactional style of leadership can also facilitate in furthering organizational citizenship behavior (Pillai et al., 1999). Empirical evidence by Walumbwa et al. (2008) has also highlighted that contingent rewards by transactional leaders can significantly shape employee behaviors and resultantly strengthen the service environment in an organization. Although transactional leadership is often believed to have influenced several desired employee behaviors and outcomes in the workplace, the effects of transactional leadership on followers’ CSQ are, ostensibly, scarcely discussed in the academic literature. Transactional leadership is usually adopted in crisis and emergencies, as well as when work needs to be carried out in a specific fashion. In this backdrop, it makes it a compelling empirically testable proposition to ascertain whether or not transactional leadership would increase employees’ CSQ in a health care setting. Emanating from the above discussion, we hypothesize the following proposition:
Laissez-Faire Leadership
Laissez-faire leadership style denotes to an approach, which chiefly lacks prominent leadership traits (Avolio et al., 1999; Hinkin & Schriesheim, 2008; Northouse, 2010). It is considered as a delegative style of leadership, where leaders adopt a hands-off approach and allow a great deal of freedom to their followers, especially concerning decision making. Leaders with such a style generally abdicate their roles and responsibilities, pay less attention to their subordinates, and avoid giving feedback or getting involved in decision making (Bass& Avolio, 1990). Individuals with a laissez-faire style of leadership often exert a unique behavior that does not focus on employees or organizational outcomes (Xirasagar, 2008). The body of literature, which deals with the laissez-faire style of leadership and its effects, is comparably limited (cf. Hinkin & Schriesheim, 2008). Although such a style of leadership can bring considerable benefits in some work contexts, especially where employees require autonomy and independence in their work, yet still, to what extent it would yield objective results pertaining to CSQ is yet to be tested. Laissez-faire leaders make employees feel acknowledged and respected and establish a sense of confidence, which can potentially yield positive outcomes for the organizations (Yang, 2015).
Although the nature of the laissez-faire style of leadership is passive and less inspiring, some occupational settings have empirically reported its significance in fostering positive employee outcomes and behaviors (Williams, 1987). Mondy and Premeaux (1995) posit that laissez-faire leaders offer enhanced leverage to their subordinates for decision making. Consequently, this style of leadership has the potential to galvanize desired employee behavior in certain situations. Accordingly, the laissez-faire style of leadership is vital for professions with challenging tasks, such as firefighters and medical emergency service jobs (Ghorbanian et al., 2012). Similar inferences were also shared by study conducted on teachers (Sorenson, 2000). Therein, because the principal did not interfere due to the laissez-faire style of leadership, it enhanced teachers’ commitment. Hence, it could be argued that the laissez-faire style of leadership could considerably help in some occupational settings based on its nature and characteristics. Therefore, we speculate that employees would prefer such a style of leadership in the health care sector to do their jobs effectively. Resultantly, it leads us to expect that such a style would also help in nurturing employee CSQ among the medical staff. Thus, we propose to investigate the following hypothesis:
Role Clarity
Role clarity denotes the extent to which employees are provided with the necessary information and guidelines on all ambiguities to effectively perform their jobs (Rogers et al., 1994). Studies have highlighted the significance of role clarity for responsive performance and employee outcomes (Lyons, 1971) whereby role ambiguities are reported to negatively affect employee outcomes (Kahn et al., 1964; Mukherjee & Malhotra, 2006). Typically, role clarity is found to be more critical in service-based organizations (Kauppila, 2014), where an explicit understanding of tasks and responsibilities is essential for providing robust customer service to clients. Likewise, studies have also delineated the equally important function of role clarity in the health care sector (Lyons, 1971).
Notably, scholars have claimed that role clarity can significantly enrich/buffer the relationship between different organizational components and service aspects (e.g., Mukherjee & Malhotra, 2006). Therein, Newman et al. (2015) have empirically underlined the moderating potential of role clarity for leadership styles. They asserted that employees with high role clarity are more likely to flourish their perceptions about leadership, which results positively in fostering their workplace outcomes. Another reason for the moderation of role clarity can be comprehended from the explanations of O’Driscoll and Beehr (1994). They suggested that managers in the supervising and leadership roles are responsible for providing role clarity through job tasks, mentoring, and by alleviating complexities. Furthermore, some scholars suggest that employees with high role clarity express a positive perspective about their leaders and, therefore, exhibit a higher level of meticulousness in their job tasks (e.g., Stinglhamber & Vandenberghe, 2004). Henceforth, we posit the following:
Cognitive Dissonance and Path-Goal Theories
The current study utilizes cognitive dissonance theory (CDT; Festinger, 1957) to investigate the relationship between leadership styles and employee CSQ. As per CDT, every individual tends to seek consistency among its beliefs and opinions (cognitions) and, therefore, when there is any level or amount of inconsistency in the behaviors or attitudes (dissonance), the change is warranted to eliminate the discomfort. Hence, from this study’s point of view, the leaders need to be consistent in their behaviors to bring about attitudinal changes in terms of enhancing employees’ commitment toward service quality. On the contrary, if the leader expresses dissonance through not recognizing their efforts, pressurizing and maintaining a less convenient environment, it will evoke negative attitudinal changes among employees regarding the work and leadership. Furthermore, path-goal theory (House, 1971) is considered regarding the moderating influence of role clarity. Leaders are generally responsible for providing important job-related information that helps subordinates perform more proficiently and responsively (Clark et al., 2009; Greene, 1979). Conclusively, the conceptual framework of the study is as follows (see Figure 1).
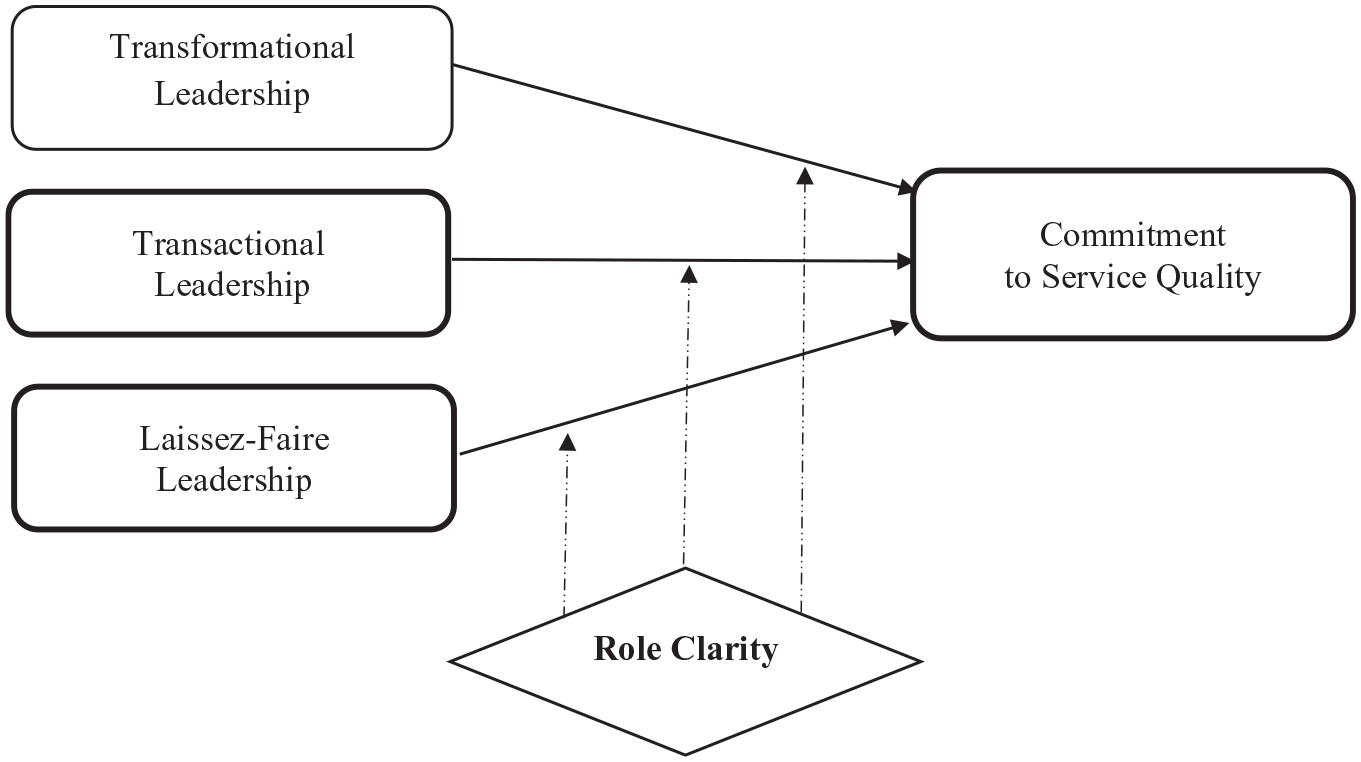
Research model.
Method
Research Design and Sampling
Numerous studies have highlighted the issue of service delivery and other health care challenges in the hospitals of the Sindh province of Pakistan (e.g., R. Ahmed & Samreen, 2011; Nisar & Amjad, 2007). The current study targeted 43 public hospitals from the Sindh province of Pakistan using questionnaire technique. As the purpose of the study was to examine commitment to service, medical doctors were purposefully selected based on the presumptions that doctors are usually believed to have the ability to exert direct influence on the behavior of other health care employees such as nurses and technical staff (Afsar et al., 2019). Second, this study deliberately chose newly appointed doctors to discover their commitment toward service quality, presumably based on the notion that these doctors are more likely to be influenced by the leadership styles of their immediate supervisors.
Most of these doctors are appointed and placed by the government. According to the Pakistan Medical and Dental Council (PMDC, 2015), there were 70,594 doctors employed in the province. After applying the Krejcie and Morgan (1970) sample size estimation technique, 382 termed to be the minimum required respondents for this study from the population of 70,594. Furthermore, following the suggestion of Bartlet and Kotrilik (2001), this sample size was doubled to ensure that sufficient responses were attained. Hence, a total of 764 questionnaires were distributed using the mail survey approach. The study received 391 responses, out of which 71 were found inappropriately filled or incomplete, hence were discarded. Finally, 315 utilizable questionnaires were included for the quantitative analysis; this sample size (315) deems also fit as per the power analysis method (Hair et al., 2016). The profiles of respondents are presented in Table 1.
Sample Profile.

Measurement Items
The CSQ was assessed by adapting the nine-item scale by Mowday et al. (1979). All the leadership styles were evaluated by the 36-item Multifactor Leadership Questionnaire (MLQ). Finally, to measure role clarity, a 17-item scale by Chonko et al. (1986) was adopted on a 5-point Likert-type scale.
Results of Analysis
The study employed partial least squares (PLS) path modeling to analyze data (Wold, 1985). More recently, this approach has received widespread recognition in quantitative data analysis (Hair et al., 2014; Ringle et al., 2012).
Reliability and Validity of Measures
Internal consistency reliability was assessed through composite reliability (see Table 2). All latent variables had composite reliability values above 0.7 (Bagozzi & Yi, 1988). The composite reliability values ranged from .907 to .969, suggesting a high level of internal consistency reliability. Outer loadings are used to report the indicator reliability of individual items in the model. All the absolute standardized outer loadings were above 0.5; according to Chin et al. (2003), when other items measure the same construct, the above threshold is acceptable. The absolute standardized loadings in the model ranged from 0.52 to 0.95, with all the average variances extracted greater than 0.5 (Fornell & Larcker, 1981). These figures assure the utilization of reliable measures in the present study.
Mean, Standard Deviation, Reliability, and Validity.

Note. CR = composite reliability; AVE = average variance extracted; CSQ = commitment to service quality.
Some scholars recently criticize that Fornell and Larcker’s (1981) criterion does not reliably detect the lack of discriminant validity in majority of the research situations (Henseler et al., 2015). Hence, we have tested the discriminant validity using heterotrait-monotrait (HTMT) (refer to Table 3). Typically, HTMT value greater than HTMT0.85 value of 0.85 (Kline, 2011) or HTMT0.90 value of 0.90 (Gold et al., 2001) underlines no issue of discriminant validity. The present study found all the values passing the HTMT0.90 (Gold et al., 2001) and HTMT0.85 (Kline, 2011) cutoff.
Discriminant Validity (HTMT Ratio).

HTMT = heterotrait-monotrait.
The Predictive Power of the Model
We analyzed the predictive power of the model using R2 (Ringle et al., 2005). The R2 value for the endogenous variable CSQ was .517. Furthermore, the achieved value of R2 is greater than .1, which, according to Falk and Miller (1992), is a minimum acceptable threshold. Next, we evaluated the effect size (f2) to determine the relative effect of exogenous variables over the endogenous variable. We used Cohen’s (1988) criteria for assessing f2 values whereby the f2 values of 0.02, 0.15, and 0.35 of the predictive variables are considered small, medium, and large in terms of effect size. The present study found small effect size for transformational leadership (f2 = 0.104) and transactional leadership (f2 = 0.035). However, we found no effect for the laissez-faire style of leadership. Finally, we examined the predictive relevance of the endogenous construct through Stone–Geisser’s Q2 test, given the fact that the endogenous latent variable of the present study was reflective (Geisser, 1974; Stone, 1974). Using cross-validated redundancy, we determined that the Q2 value was greater than zero (0.337). This suggested that the model applied exhibits predictive relevance (Hair et al., 2014; Henseler et al., 2015).
Hypothesis Testing
By using the bootstrap technique with 5,000 resamples (Hair et al., 2014), which results in more reasonable standard error estimates, we examined the significance of path coefficients.
First, we tested the direct effects of leadership styles on the employee’s CSQ. The R2 was .470, which indicates that the three leadership styles explained 47% of the variance in employee’s CSQ. Transformational leadership (β = .421, t = 6.214, p = .000, f2 = 0.104) and transactional leadership (β = .282, t = 3.085, p = .001, f2 = 0.035) were positively related to employee’s CSQ, while laissez-faire leadership was not a significant predictor of employee’s CSQ. Thus, H1 and H2 were supported, while H3 was not supported. Next, to test the moderating effects, we used the two-stage approach because we had a large number of items. The R2 change, after we included the interaction effect, was .517. The additional variance explained by the interaction effect was 4.7%, with an effect size of 0.0973 (small effect). The Transformational × Role Clarity → CSQ (β = −.297, t = 3.158, p = .001, f2 = 0.046) and Laissez-Faire × Role Clarity → CSQ (β = .186, t = 2.523, p = .006, f2 = 0.020) were significant, while the Transactional × Role Clarity → CSQ was not significant, thus accepting H4 and H6 and rejecting H5 (see Table 4). To interpret the moderating effects, we drew two interaction plots, as shown in Figures 2 and 3.
Structural Model.

Note. LL = lower limit; UL = upper limit; CSQ = commitment to service quality.

Moderating effect of role clarity on the transformational leadership–commitment to service quality relationship.

Moderating effect of role clarity on the laissez-faire leadership–commitment to service quality relationship.
Figure 2 outlines that the relationship between transformational leadership and employee’s CSQ is stronger when role clarity is lower.
Figure 3 illustrates that when role clarity is low, then the laissez-faire leadership style → employee’s CSQ was negative, while the same relationship appears positive when role clarity is high. Clearer role clarity is important to enhance this relationship. Next, we determined the strength of the moderating effect by assessing the effect size (Cohen, 1988). The strength of the moderating effect was examined by comparing the main effects of the model with the R2 value of the complete model, including both moderating and exogenous latent variables (Henseler & Fassott, 2010). The strength of the moderating effects was tested through Cohen’s (1988) criterion. Accordingly, the f2 values of 0.02, 0.15, and 0.35 are expressing weak, moderate, and strong effects, respectively (Cohen, 1988; Henseler & Fassott, 2010). Notably, according to Chin et al. (2003), a low effect size does not mean that the moderating effects are insignificant. “Even a small interaction effect can be meaningful under extreme moderating conditions, if the resulting beta changes are meaningful, then it is important to take these conditions into account” (Chin et al., 2003, p. 221). The effect size for the moderating effect of role clarity over transformational leadership style → CSQ (f2 = 0.046) and laissez-faire style of leadership (f2 = 0.020) was found to be small.
Discussion
This study was set out to examine how prominent leadership styles, such as transformational, transactional, and laissez-faire, influence CSQ. The study further tested the moderation of role clarity on these relationship styles. The study found a positive relationship between transformational leadership and CSQ. These findings are in line with prior studies (Clark et al., 2009; Hashim & Mahmood, 2012). The results indicate that employees’ view of their leaders being visionary, optimistic, and firm in values and purpose helped them to enhance their commitment levels to service quality. Transformational leaders motivate employees to go beyond conventional expectations by focusing on high-order intrinsic needs. Such leaders act as mentors and pay attention to the individual developmental, learning, and achievement needs of each subordinate (Bass, 1985; Bass & Avolio, 1990; Clark et al., 2009). Equally, the findings also suggest that employees viewed their transformational leaders to be creative and encouraging in bringing unique perspectives for solving problems.
Furthermore, the path modeling results also reported a strong positive influence of transactional leadership and CSQ. The results lend support to existing studies (Nguni et al., 2006; Walumbwa et al., 2005). The findings suggest that individuals’ perception of their leaders being supportive in handling unexpected occurrences and proactive in addressing work-related issues harnesses their CSQ. Overall, the findings are also in conjunction with existing studies underlining the importance of contingent rewards by transactional leaders in shaping employee behaviors and outcomes (Chen, 2004; Walumbwa et al., 2008). Transactional leaders set clear and unambiguous goals, provide useful feedback, and subsequently tie extrinsic reward provisions with employees’ performance targets (Afshari & Gibson, 2016; Bass, 1985). The findings also make it logical to understand how the transactional leadership style can assist in achieving organizational outcomes even when the conventional leadership traits are absent in a particular leader such as charisma and sociability (Nguni et al., 2006).
As our study could not find empirical support for the relationship between laissez-faire style of leadership and CSQ, our findings, ostensibly, stand in contradiction to existing studies such as Ghorbanian et al. (2012) and Sorenson (2000), which suggest a positive link between laissez-faire style of leadership and employee commitment levels. One of the possible reason we did not find any support for this relationship could be due to the bespoke nature of the health care sector, where employees are likely to perceive their work role as a more integrated activity which often necessitates mutual collaborations and consequently warrant support and role ownership from their superiors. Another plausible reason laissez-faire leadership style was not effective in our study may have to do with the fact that many doctors in the public-sector hospitals in Pakistan were not necessarily the most competent ones. Traditionally, there are non-meritorious factors, such as political affiliations, which play out more profoundly when doctors are hired for the public sector in Pakistan. Furthermore, they probably do not have the required levels of self-efficacy and are less likely to be motivated intrinsically.
Hence, at the conjecture of this, we can infer that the newly appointed doctors are likely to receive positive influence when leaders exercise transformational and transactional leadership styles, but they may not exhibit higher levels of CSQ when a particular leader is exercising laissez-faire style of leadership.
For the moderating effect of role clarity, our findings, grounded on the path-goal theory, suggest that role clarity buffered the relationships of transformational and laissez-faire leadership with employees’ CSQ. These findings are, for the most part, in conjunction with the previous studies (e.g., O’Driscoll & Beehr, 1994; Stinglhamber & Vandenberghe, 2004). Our findings have seemingly affirmed that employees receiving and understanding essential and unambiguous job-specific information are likely to exhibit higher levels of commitment toward the service quality and service delivery, especially in the health care setting. These findings, therefore, imply that respondents with role clarity managed to capitalize on the visionary (transformational) leadership style, exercised by their leaders, to strengthen their commitment toward service quality further. These findings underscore the crucial influence role clarity can exert on employees’ commitment toward service quality when their leaders extend unblemished instructions and share clear expectations with their subordinates.
Correspondingly, drawing on the path-goal theory, our findings have also highlighted the moderating effect of role clarity on the relationship between laissez-faire leadership style and CSQ. The results suggest that individuals who experienced a lack of robust leadership perceived themselves to be in a better position to strengthen their CSQ through role clarity. Although role clarity failed to moderate the transactional leadership and CSQ relationship, the findings have supported the recommendations of Fisher and Gitelson (1983) and Mukherjee and Malhotra (2006) regarding the buffering potential of role clarity toward enhanced service behaviors. The findings, therefore, revealed that when employees perceive sufficiency of clarity and understanding toward their assigned roles and responsibilities, they tend to become more effective in maximizing their service quality commitment levels. These findings essentially suggest that role clarity possibly moderated these relationships because leaders have the responsibility to not only define clear roles for their subordinates but also involve them in establishing goals and mentor them on how to achieve these goals successfully.
Plausibly, no significant moderating effect of role clarity on the transactional leadership and CSQ association could be due to limited or no experience of the respondents of the current study under a leader providing ample role clarity alongside exhibiting the transactional style of leadership.
These findings also appear to be in conjunction with some of the existing studies with similar lines of inquiries (Clark et al., 2009).
Theoretical Implications
The findings of our study provide useful theoretical implications for the scarce literature on the role of various leadership styles, such as transformational, transactional, and laissez-faire, in influencing CSQ, among their followers, with the moderation of role clarity. The study was conducted based on a conceptual framework outlining a number of gaps in the literature underpinned both by the cognitive dissonance and path-goal theories. To our knowledge, this is the first study of its kind that integrated role clarity as a moderating variable in understanding the relationships between transformational, transactional, and laissez-faire leadership styles and CSQ in a health care setting. These findings broadened our understanding of how role clarity can play an important role in fostering CSQ when leaders exhibit varying approaches such as transformational, transactional, and laissez-faire leadership styles. The findings have, therefore, extended the service quality management literature by delineating the role played by different leadership styles in improving followers’ CSQ in the health care context.
Findings revealed positive relationships between transformational and transactional leadership styles and CSQ. Stimulatingly, however, our study could not find empirical support for the relationship between laissez-faire style of leadership and CSQ. This, typically, is in contradiction with the existing studies (Ghorbanian et al., 2012; Sorenson, 2000), which suggest a positive link between laissez-faire style of leadership and employee commitment levels. This could partly be due to the fact that employees in the health care context are likely to be extra vigilant about their tasks, owing to the sensitive nature of the health care profession and higher likelihood of litigation involved. This would make them view their jobs as a more integrated activity, which may compel mutual collaborations and role ownership by their leaders. To encapsulate, the current study offers an inclusive framework that defines the relationship between leadership styles and CSQ with role clarity as a robust moderator.
Managerial Implications
A number of important managerial implications can be drawn from this study. Findings suggest that leaders play a very important role in influencing their subordinates’ CSQ in public-sector hospitals. Leaders can exhibit crucially vital behaviors such as providing clear directions, communicating realistic expectations, using motivational techniques, offering useful feedback, providing rightful rewards, and defining roles with clarity. These workplace practices and interventions ultimately offer dividends and translate into enhanced commitment levels toward service quality, on the part of their subordinates. Our findings have essentially demonstrated that the transformational leadership style is a particularly better predictor and thus imparts more influence on employees’ CSQ compared with transactional and laissez-faire styles of leadership. This is apparently because transactional leaders in public hospitals are probably less obliged to support their subordinates for enhancing their CSQ.
These findings can be applied to the public health sector organizations in a number of different ways. The results imply that when leaders are able to define clear roles and communicate their work-related expectations with the concerned employees, then it resultantly becomes convenient for the staff to live up to those expectations. Furthermore, the findings suggest that leaders and human resource management professionals should work to ensure adequate measures are taken in this regard. For instance, numerous orientation and training programs may be introduced to promote effective leadership approaches and foster their influence on enhancing CSQ. Likewise, leaders may be trained to take responsibility for facilitating employees by providing role clarity in the public-sector hospitals of Sindh, Pakistan, so that they understand the job requirements and effectively achieve the organizational goals, especially in relation to service quality. Thus, organizations should ensure that supervisors engage in healthy managerial behaviors by taking account of factors that are likely to foster improved service quality to the service users. These findings have strong underpinnings for managerial practice as concerns surrounding CSQ are gaining considerable credence in academic and practitioner literature.
Limitations and Scope for Further Study
Despite several strengths, this study has some limitations, which paves a way forward for future research to advance the relationships examined in this study. First, the study was based on a homogeneous sample of respondents, which was drawn from the public-sector hospitals in the Sindh province of Pakistan. Findings should, therefore, be treated with caution, and the generalizability of these findings to public-sector hospitals outside Pakistan can be questioned. Although these findings are in agreement with the conceptual model, the causality of the findings can be subjective to a certain extent. Future researchers may wish to test the interplay of different leadership styles with role clarity in other geographic locations and occupational settings, having different demographic compositions.
Second, the study relied upon self-reported questionnaire data. Here, the probability of common method variance may have prevailed because all the variables were measured employing a single survey instrument. We understand that the common method variance is more bothersome in analyzing the relationships between the attitudinal or psychological data obtained from a single respondent at one point in time (Avolio et al., 1991). With respect to this study, both independent and dependent variables are based on perception data. Future researchers should, therefore, take measures to reduce this common method variance. For instance, instead of using perception-based data, objective measures could be employed. Accordingly, because the research model has explained 52% of the total variance in CSQ, future researchers may wish to examine how other factors might explain the remaining 48% of the variance for CSQ, across various sectors and/or industries.
Third, these findings are not very surprising because Pakistan scores high on power distance and collectivism. Thus, we suggest future studies may be conducted in the countries that score low on power distance and collectivism. We also recommend that other critical factors such as cultural orientation, leader’s cultural sensitivity, and individual values may be incorporated in this model to confirm our results further. Finally, because the study found no significant moderating effect of role clarity on the relationship between transactional leadership and CSQ, this may potentially be explained through the mediation effects of other intervening variables (Walsh et al., 1981). Therefore, future researchers may consider evaluating the mediation of role clarity between transactional leadership and CSQ to accentuate the strength of other intervening relationships.
Conclusion
The study drawing upon CDT and path-goal theory investigated the role played by different leadership styles in influencing CSQ with the moderation of role clarity. The findings lend support to the direct hypothesized relationships of transformational and transactional leadership with CSQ, with role clarity playing the moderating role between these relationships. However, there was no such moderating effect for the relationship between transactional leadership and CSQ. Moreover, compared with the laissez-faire style of leadership, the transformational and transactional leadership styles are considered more useful when leaders desire to exert greater influence on employees’ CSQ.
This study has broadened our theoretical and empirical understanding of the interplay of varying leadership styles and service quality with the intriguing contribution of role clarity in a health care setting. The study has highlighted the prominent role of leadership styles for fostering subordinates’ CSQ and how different leadership styles can be intermingled with role clarity to further their relationship toward the CSQ.
The findings underscore the importance of providing unambiguous and value-driven role clarity on the part of leaders. It becomes all the more crucial when it comes to the health care sector because commitment toward service quality becomes more paramount and could potentially make a big difference as far as patients’ well-being is concerned. Findings also downplayed the vitality of laissez-faire style of leadership in the public-sector hospitals of the Sindh province of Pakistan. This possibly suggests that the senior management in such health care setting should avoid relying on such type of hands-off approach of leadership to offset any likelihood of mitigation in CSQ by the medical staff.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.