
Abstract
The aim of this study was to assess the effect of weight status on body perception and satisfaction, occurrence of Anorexia Readiness Syndrome (ARS), and dietary behaviors in adolescent girls. The study was conducted among 516 girls aged 14 to 16 living in Szczecin (Poland). The ARS Diagnosis Questionnaire designed by Ziółkowska and the author’s own questionnaire about self-perception of body were used, and anthropometric assessment was performed. The weight status significantly affected weight status perception, body satisfaction, and dietary behaviors. The girls with a body mass index (BMI) > 50th percentile more often were dissatisfied with their bodies and more often showed at least a medium ARS level. The girls with a BMI ≤ 50th percentile more often overestimated their body weight, and transferred the feeling of being unattractive to their faces. Results of this study demonstrate the importance of education for adolescent girls to help realistically assess body size and promote healthy bodies and eating behaviors, regardless of the weight status.
Introduction
Currently, obesity associated with adipocyte hypertrophy and/or hyperplasia is one of the most common diseases arising from malnutrition. According to World Health Organization (WHO, 2016) data, 340 million children and adolescents aged 5 to 19 have excessive body weight, including 41 million who are obese. Adolescence is generally considered to be a time of good health; however, many chronic diseases that can determine health in adulthood may have their beginning then. Typical complications of childhood obesity include impaired glucose tolerance, hyperinsulinaemia, lipid disorders, non-alcoholic fatty liver, cholelithiasis, obstructive sleep apnea, orthopedic and psychological problems, and arterial hypertension that occurs in obese children 3 to 5 times more often than in peers with normal body weight (Feld & Corey, 2007; Labarthe et al., 2009). Obesity that occurs during childhood increases the risk of metabolic diseases and disorders in adulthood (Lloyd et al., 2012). According to the WHO (2010), excessive body weight is responsible for 35% of cases of coronary heart disease, 55% of hypertension, and 80% of type 2 diabetes. Excessive body weight during adolescence can also lead to psychological problems resulting in an inappropriate attitude toward eating and self-perception of their own body.
Body Perception and Satisfaction
Today, there is an increase in interest in the impact of the perception of body image on self-acceptance, well-being, and mental health. An important period in shaping the attitudes toward “body self” is adolescence (Voelker et al., 2015). The interest in the changing body and its proportions, characteristic of this period of life, influences perception, acceptance, and self-assessment of the body, often made in the context of social patterns (Groesz et al., 2002; Perloff, 2014). The image of an ideal woman changed over the years and was a reflection of the canons of female beauty and fashion trends prevailing in a given place and time. Fashion for a slimmer female body began in the 1940s. In the 1950s, a female model was slimmer than the average woman by 5% to 8%, currently it is slimmer about 20% (Bovet, 2018).
Despite the existence of tools enabling measurements of body size and their reliable interpretation, self-assessment of appearance is not always consistent with reality (Schuck et al., 2018). By frequently comparing themselves with the ideal body shape promoted in the media, young women do not feel attractive and are dissatisfied with their appearance. For them, the body is a source of unpleasant sensations, and is the object of comparisons, not integrating with their identity. As a consequence, they over-control their physical appearance, often incorrectly estimating their body dimensions, which promotes negative feelings and emotions toward their body (Stice & Bearman, 2001).
Anorexia Readiness Syndrome (ARS)—Approach to Eating and Body
Dissatisfaction with one’s own body can contribute to unhealthy eating behaviors and approaches. It also poses a threat of eating disorders, among others anorexia, which is a chronic disease, difficult to treat, and often fatal. Some people have a certain predisposition to anorexia, which is called Anorexia Readiness Syndrome (ARS). It means a psychologically, socially, and culturally conditioned set of symptoms that may indicate irregularities in meeting the nutritional needs and in the attitude toward own body. This term was defined and introduced to literature by Ziółkowska (2001, 2005) who, when describing the characteristic features of ARS, presented its indicators in many areas of a person’s functioning. The ARS Diagnosis Questionnaire contains questions about forms of body weight reduction, attitude toward eating, style of parenting, and perception of own attractiveness.
Anorectic behaviors characteristic of the manifestation of anorexia syndrome include
above-average knowledge about the nutritional value of food, counting the energy value (calories) of food consumed;
high interest in own appearance and own person, comparing oneself with the patterns of an ideal female body presented in mass media;
obsession with controlling own weight and size and the associated emotional tension;
exaggerating own body size;
sudden interest in and manifestation of motor activity;
need for control, excessive perfectionism;
unstable emotions, conditioned by the wrong image of own body and the wrong approach to meeting the nutritional needs;
particular susceptibility to external stimuli, especially those coming from mass media, mainly regarding the current canons of female beauty presented by them (Ziółkowska, 2000, 2001, 2009; Brytek-Matera & Rybicka-Klimczyk, 2012; Chytra-Gędek & Kobierecka, 2008).
Early identification of people with increased risk of anorexia allows appropriate prophylactic measures and can prevent the occurrence of this disease (Rienecke, 2017).
Determinants of Body Perception and Its Acceptance During Adolescence
An important period during which an image of own appearance and attitude toward own body is created is adolescence. On one hand, it results from the search for one’s identity, and on the other, from simultaneous physical, psychological, and cultural changes (Ackard & Peterson, 2001). During this period, young people have a special need to feel accepted by peers, often putting the needs and beliefs of their peers over their own (Webb & Zimmer-Gembeck, 2014). There is evidence that complexes regarding appearance, attractiveness, or weight developed during this period will most likely accompany the person throughout their adult life. To shape a stable body image, it is important to realistically perceive it and accept the natural changes that occur in it (Hausenblas et al., 2008; Hausenblas & Fallon, 2002).
Research Justification
Although a volume of research on body satisfaction was published in recent years, there are still unanswered questions. Few studies focus on adolescent girls and most research targets overweight young women. In this study, we consider how perception and attitudes about one’s body depend upon weight status among normal weight, underweight, and overweight adolescents.
Aim of the Study
The aim of this study was to assess the effect of weight status on body perception and satisfaction, occurrence of ARS, and dietary behaviors in adolescent girls.
Material and Methods
Data Collection and Analysis
Participants
The study was conducted among 516 girls aged 14 to 16 (15.1 ± 1.2) living in Szczecin (Poland) and attending lower secondary schools. The study was approved by the local Bioethics Committee and school boards, and parental and students consent was obtained.
Questionnaire about self-perception of body
For survey questions about self-perception of body developed by the authors, participants reported their body weight and height, self-assessed their body weight, declared its desired value, and assessed their sense of attractiveness and attitude toward their body weight and body shape. It also included questions about their perception of weight status and body, its emotional and behavioral aspects. Sample questions in this part of the survey are as follows: Are you satisfied with your body weight? Are you satisfied with the shape of your body? Would you like to lose body weight/increase your body weight? Do you feel the pressure of having a slim body? Which parts of your body do you find unattractive?
ARS Questionnaire
The survey part also included the Questionnaire for Testing Individual Approach to Eating (ARS) designed by Ziółkowska (2001) containing 20 statements that relate to four variables diagnosing the ARS, such as forms of losing weight, attitude toward eating, style of parenting, and perception of own attractiveness. These statements should receive an affirmative or negative answer. Depending on the question, the affirmative (Questions 1–12, 15, 17–20) or negative (Questions 13, 14, 16) answer is scored with 1 point and indicates anorectic behavior. The maximum number of points is 20, the result up to 6 points indicates a low ARS level, from 7 to 13 a medium ARS level, and above 14 indicates a high ARS level (Merkiel et al., 2014; Ziółkowska, 2001).
Body mass, body height, and body mass index (BMI) estimation
In the second stage of the study, on the same day the survey was conducted, the body weight and height of the respondents were measured (after completing the questionnaires). Body weight was determined in light outerwear using a certified medical scale, with an accuracy of 0.1 kg, while body height using a stadiometer, in the Frankfurt Plane position, with an accuracy of 0.1 cm. BMI was calculated based on the results obtained using the following formula:

The weight status of the respondents was determined based on the current BMI growth charts applicable in Poland (Różdżyńska-Świątkowska et al., 2013). The cut-off points on the charts for 15-year-old girls, being characteristic of underweight (BMI ≤ 17.45), weight within range defined as normal (BMI 17.45–23.94), overweight (BMI 23.95–29.1), and obesity (BMI ≥ 29.1), are consistent with the classification of the weight status in the method of Cole et al. (2000) and Cole et al. (2007). For further analysis, the girls were divided into four groups: underweight (UW), weight within range defined as normal below the 50th percentile (NW ≤ P50), weight within range defined as normal above the 50th percentile (NW > P50), and overweight (OW). Based on the body weight given by the respondents and obtained in anthropometric measurements, the percentage of girls who overestimated and underestimated their body weight was calculated in individual body weight groups, assuming a tolerance of ±1 kg.
Statistical Analyses
Statistical analyses of the obtained results were performed using Statistica® software (version 12.0). The studied population was divided according to the weight group. Qualitative variables are presented in the contingency tables, and Kruskal–Wallis rank ANOVA was used to determine statistically significant differences. To find out between which subgroups statistical differences occurred, a mean-ranks post hoc multiple comparison test was used for all groups. The tables present the frequencies of responses to questionnaire questions and p values of Kruskal–Wallis rank ANOVA test. All p values of post hoc test ≤ 0.05 were considered statistically significant.
Results
Anthropometric Measurements
Of the surveyed participants, 17.8% who completed the questionnaire refused to participate in anthropometric measurements, therefore their survey data were not included in further analyses.
When analyzing the results of anthropometric measurements, it was found that 71.6% of the surveyed girls had weight within range defined as normal for age and height (31.1% of the respondents with BMI ≤ P50% and 40.5% of the respondents with BMI > P50), more than 11% were underweight, 14.1% overweight, and 2.83% obese (Figure 1).

Evaluation of weight status based on the BMI value (n = 424).
Body Weight Perception—Self-Estimation
More than 20% of the respondents could not accurately provide their body weight (±1 kg; Table 1). Taking into account the percentages of girls who underestimated their body weight reported in the survey before the anthropometric measurements, it was found that they were significantly different in individual weight groups, with the highest percentage of girls who underestimated their body weight being recorded in the group with BMI considered as normal > P50 (20.9% vs. 8.3%, 0%, 5.6% in other weight groups). The slimmer girls—underweight and with BMI considered as normal ≤ P50—significantly more often overestimated their body weight than the girls with BMI considered as normal > P50 and overweight ones (16.7% and 18.2% vs. 6.9% and 5.6%).
Self-Estimation of Body Weight (n = 424).

Note. UW = underweight; NW =weight within range defined as normal; OW = overweight and obesity.
The percentages in a row marked with different letters differ significantly between weight groups, p ≤ .05.
Moreover, when analyzing the obtained results, it was found that 23.6% of the surveyed girls could not interpret their body weight properly (Table 1). Taking into account distribution of responses in individual weight groups, underweight participants were more likely to consider their body weight normal (50%) compared with overweight (11%), while 22.4% of normal weight participants were unable to interpret their body weight status relative to standards.
Body Weight and Body Shape Satisfaction, Dieting, and Weight Behavior
Systematic body weight control was declared by 86.7% of the respondents, most often they were the girls with body weight within range defined as normal at the upper range (BMI > P50; Table 2). Less than half of the girls (45.7%) systematically measured their waist and hip circumference, and the underweight girls weighed and measured their body least often.
Satisfaction With the Body, Desire to Change, Dieting, and Behavioral Intention and Weight Behavior of the Examined Girls (n = 424).

Note. UW = underweight; NW = weight within range defined as normal; OW = overweight and obesity.
The percentages in a row marked with different letters differ significantly between weight groups, p ≤ .05.
Despite the fact that more than 70% of the respondents had body weight within range defined as normal, only 32.1% of all girls were satisfied with it, most often they were underweight (66.7%); in the group of girls with body weight within range defined as normal, only 38% were satisfied with their body weight (Table 2). Statistically significant differences in satisfaction occurred between the groups of underweight and body weight within range defined as normal (BMI ≤ P50) girls and those of body weight within range defined as normal (BMI > P50) and overweight and obese girls (66.7% and 48.5% vs. 23.3% and 0%).
More than 70% of the respondents wanted to reduce their body weight (Table 2). This group included not only the overweight girls (94.4%) but also girls from other groups, including more than 10% of the underweight girls. Statistically significant differences occurred between the group of underweight girls and the groups of body weight within range defined as normal and overweight and obese girls (11% vs. 57.1%, 86.8% and 94.4%), and between the girls with body weight within range defined as normal (BMI ≤ P50) and other groups (57.1% vs. 86.8% and 94.4%). Among all the surveyed girls, only 19.8% did not want to change their body weight, with the highest percentage being recorded in the group of underweight girls (66.1%).
During the preceding year, 37.1% of the respondents declared dieting, most often the overweight girls (66.7%) responded in this way (Table 2). Statistically significant differences occurred between all groups of girls, the percentage of dieting girls increased in each subsequent weight group (from 10% in the group of underweight girls to 66.7% in the group of overweight girls).
Of the participants, 40.6% felt the pressure of having a slim body promoted in the media; this was declared by half of the overweight girls, slightly less (41.7%) by the underweight girls, and more than 33% of the girls with body weight within range defined as normal (Table 2). The feeling of pressure was independent of their body weight.
Over half of the respondents (53.8%) were dissatisfied with the shape of their body, most often they were the girls with higher body weight (Table 2).
Among the body parts with which the girls were the most dissatisfied, the legs and/or buttocks were most often chosen; 70.8% of all respondents did not accept them (Table 3). These body parts were chosen by all overweight and obese girls, and more than three fourths of them also indicated the abdomen and/or waist, and over two thirds the shoulders. Legs and/or buttocks were also indicated by most girls with body weight within range defined as normal and half of the underweight girls. The underweight girls were most often dissatisfied with the appearance of their face (58.3%).
Parts of the Body Considered Unattractive (n = 424).
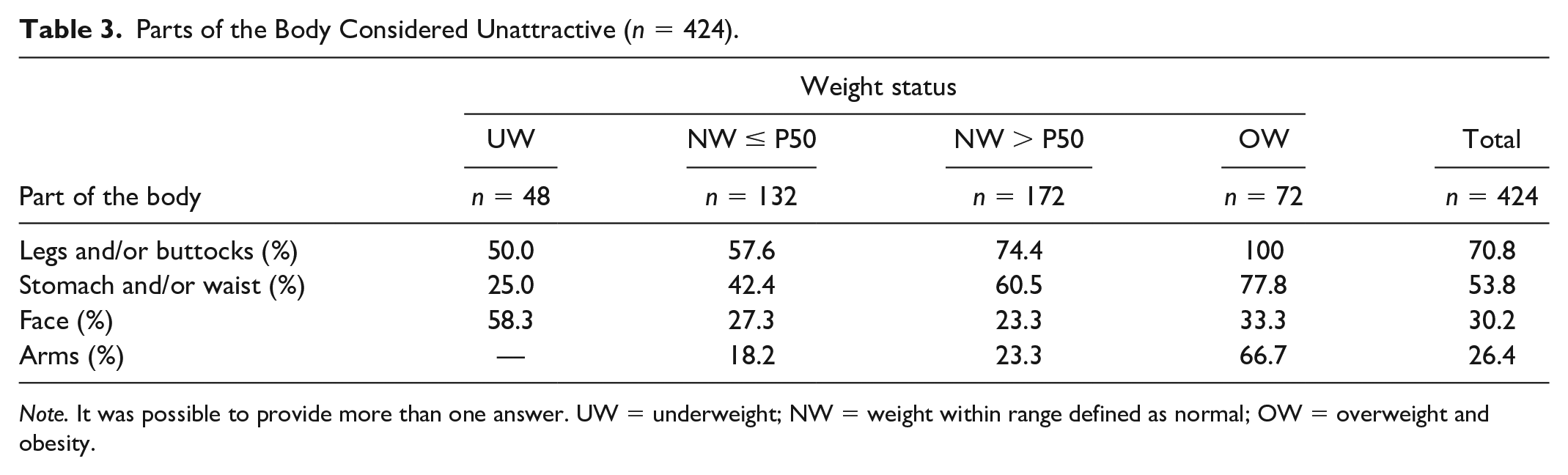
Note. It was possible to provide more than one answer. UW = underweight; NW = weight within range defined as normal; OW = overweight and obesity.
ARS Diagnosis
When analyzing the results of the survey, 63.1% of the surveyed girls scored at the medium level of anorexia readiness, with girls of a BMI in the upper normal and above normal range more likely to score compared with underweight and lower normal range (67.4% and 83.3% vs. 41.7% and 48.5%; Table 4).
Diagnosis of the ARS Level (n = 424).

Note. ARS = Anorexia Readiness Syndrome; UW = underweight; NW = weight within range defined as normal; OW = overweight and obesity.
The percentages in a row marked with different letters differ significantly between weight groups, p ≤ .05.
Discussion
The study showed that more than 21% of 424 respondents were unable/unwilling to accurately report their body weight in the survey, over- or underestimating it. Underestimation of body weight by the surveyed girls could be due to dynamic weight changes over time in this developmental period. However, it can be seen that among the participants with a BMI > P50, who least often reported their body weight accurately, the highest percentage of girls systematically controlling their weight was recorded.
However, weight loss–oriented behaviors do not always give positive health effects. Health benefits primarily result from lifestyle modifications, including physical activity and improved nutritional habits. Favoring a slim body means that people with excessive body weight do not accept themselves, are on a diet, and then gain weight again. Rapid fluctuations in body size and dissatisfaction with own body can cause more health damage than excessive body weight. Therefore, the Weight-Centered Health Paradigm (WHCP) is increasingly being subjected to critical analysis, which is moving toward a focus on health and well-being (O’Hara & Taylor, 2018). To counteract the stigmatization of obese people and emphasize the importance of health (and not a slim body at all costs), the Health at Every Size (HAES) movement, among others, was created. The HAES theory emphasizes that people of all sizes can and should take action to improve their health and well-being, regardless of whether these practices cause body weight changes. Maintaining a proper lifestyle provides health benefits over a wide range of body sizes, while dissatisfaction with own body size and shape can also lead to illness. However, societal pressures influence unhealthy body perceptions, increasing pressure for a slim body (Suelter et al., 2018). But good health is not conditioned by being slim. It depends on a healthy lifestyle and satisfying attitude to the holistically expressed body. The attitude to body size, however, must be balanced, because research shows that the “fat but fit” people are still more vulnerable to many diseases and adverse health effects than the general population (Caleyachetty et al., 2017). For this reason, it is worth conducting education in the area of own body perception, proper nutrition, and health.
Pressure to have a slim body contributes to dissatisfaction with one’s own body weight and paradoxically translate into further weight gain caused by emotional eating (Sharpe et al., 2013). Social and environmental pressure to have a slim body was declared by 40% of the surveyed girls, slightly more often in the group with higher body weight (50%). Other researchers also found that girls with higher BMIs express greater dissatisfaction with their own body and feel a greater sense of pressure to have a slim body (Petrie et al., 2010). The impact of the internet and social media in this area is currently highlighted (Perloff, 2014). Girls may not know their body weight, but it should be noted that 86.7% of those surveyed said they weighed regularly. It cannot therefore be ruled out that they consciously underestimated their body weight. Studies conducted so far show that women tend to underestimate their body weight (Burke & Carman, 2017), especially if they give it in a telephone interview (Courtemanche et al., 2015; Pinkston, 2017). In contrast, psychologists often rely on self-description of body weight, which can create research problems.
Inaccuracy of the assessment of one’s own body weight compared with standards may be due to the adopted impression management strategy, self-presentation, consisting in telling others that you have a socially desirable body weight. It can also be a form of self-defense, allowing people to protect their self-esteem, convincing themselves and their social environment that they are slimmer than they really are (Burke & Carman, 2017; Holbrook & Krosnick, 2010).
Social beliefs about body size in women (and men) include a belief that a slimmer body makes a person more attractive and increases employment and economic opportunities (van Vliet et al., 2015). In the study conducted by Chytra-Gędek and Kobierecka (2008), 65% of respondents were convinced that slim women are more successful with men, therefore one could expect that the tendency to underestimate body weight will be more likely to affect girls with excessive body weight. The presented study, however, showed that the girls with weight within range defined as normal, oscillating at the upper limit range, most often underestimated their body weight. Perhaps in a direct interview, girls who are overweight or obese realize that it is impossible to hide excessive body weight, which already translated into obvious visual impressions. Some of the respondents, especially slim girls, overestimated their bodyweight. This could be due to the desire to avoid comments and pressure from adults who pay attention to their low body weight and the associated risk of growth inhibition, development, puberty, and an increased risk of eating disorder.
Most of the girls (67.9%) were not satisfied with their body weight and wanted to reduce it (71.3%), it concerned mainly participants with normal body weight at the upper limit of normal and overweight ones. Miranda et al. (2014) showed that 78.9% of students are dissatisfied with their body shape and 60.8% would like to reduce body weight. In the study by Kołoło and Woynarowska (2004) conducted in 2002, 56.5% of the surveyed girls aged 15 thought that their body weight was too high. In the years 2009–2010, the HBSC (Health Behaviour in School-Aged Children) survey was conducted, which showed that in Poland the percentage of 15-year-old girls who think they are too fat was 51% and was one of the highest in Europe (Currie et al., 2012). The group that most often did not want to change body weight were underweight girls, but among them were girls (11%) who thought they were too fat and would like to weigh less. In the study by Cheung et al. (2011), the percentage of underweight young women who still wanted to reduce their body weight was higher and was more than 30%. A significant percentage of underweight girls (62%) who wanted to reduce their body weight was also reported by Woźniak et al. (2014). Kim and Lee (2010) and Isomaa et al. (2011) found that not only overweight teenagers, but also underweight ones, perceive themselves through the prism of excessive body weight. This perception is associated with more frequent occurrence of depression in adolescents (Armstrong et al., 2014; Isomaa et al., 2011). It seems that the reason for such dissatisfaction could be, among others, the lack of ability to interpret their own body weight in the context of the norms adopted in a given age group. Our own research shows that 23.6% of the respondents could not interpret their body weight properly; significantly more often they were girls with lower body weight. Studies indicate that adolescents often have problems with self-assessment of the correctness of their body weight (Voelker et al., 2015). That is why education is important to this age group, to introduce concepts of healthy bodies, healthy attitudes toward their own bodies, and accurate interpretation and assessment of their own body weight. Parents and health care professionals should monitor not only actual BMI, but also students’ perception of body weight, because of its greater contributions into better self-esteem than actual body weight (Kim and Lee, 2010).
More than half of the girls (53.8%) were also dissatisfied with the appearance of their bodies. Very similar results (56%) were obtained by Cuadrado et al. (2000) among Spanish teenagers, while in Brazil 64% to 82% of teenagers (Pelegrini & Petroski, 2010) were dissatisfied with their appearance. The body parts with which teenagers were most dissatisfied were the legs and/or buttocks and the abdomen and/or waist. Similarly, Sobczak and Sobczak (2011) found a correlation between the BMI value and the assessment of individual body parts. The higher the BMI value, the lower the satisfaction with the body parts listed above. A similar correlation was also observed in our own study, in which all overweight girls were dissatisfied with their legs and/or buttocks, and 77.8% of them also with the abdomen and/or waist. Girls with weight within range defined as normal and low body weight less often showed dissatisfaction with these body parts. Miranda et al. (2014) found that dissatisfaction with their body is more common in adolescents with excessive body weight. In contrast, Lopes et al. (2017), while conducting the survey among students in Brazil, showed no influence of nutritional status on the sense of attractiveness. Coqueiro et al. (2008) found that dissatisfaction with one’s own body is correlated with the degree of fatness and not BMI value.
The surveyed girls were most often dissatisfied with their legs, buttocks, and abdomen. Similar to the presented study, young women surveyed by Frederick et al. (2014) and by Jośko-Ochojska et al. (2013) rated the shapes of their abdomen, thighs, and hips the lowest. Frederick et al. (2014) found that in the case of women, dissatisfaction with the middle and lower torso affects the dissatisfaction with their body to the greatest extent.
This study also showed that even if girls do not question their body shapes, they show dissatisfaction with their faces, which was often observed in underweight girls. The face was also the lowest rated part of their body in young female dancers surveyed by Ołpińska-Lischka, (2017). Most often they had no objections to the shape and size of their body, but they considered their face unattractive. Professional makeup and careful hairstyle are important to the exposed face of female dancers and it may affect their final score. It seems that in the case of satisfactory assessment of modifiable body parts, girls transfer their sense of lack of attractiveness to non-modifiable components (here: face appearance). This is confirmed by a critical attitude to physical appearance during this period of development. Ołpińska-Lischka (2017) showed that young women, younger than 25, are more critical of their face compared with women above 25. It should be emphasized that positive perception of the body and face is very important because it is associated with self-esteem, personal satisfaction, and well-being. It is worth improving self-esteem at all ages, but especially in teenagers, because there is a relationship between a sense of attractiveness during adolescence and dissatisfaction with appearance in the long term (Rosenblum & Lewis, 1999).
Dissatisfaction with the body can lead to inappropriate eating behaviors to match the image that is considered ideal. It was found that 37.1% of the respondents declared dieting during the year preceding the survey. A higher percentage (60.6%) of dieting 15-year-old girls was obtained by Tomaszewska et al. (2012) and Janiszewska et al. (2011). During the HBSC survey, 22% of girls declared various behaviors aimed at reducing body weight (Currie et al., 2012). In our own study, dieting was declared by 10% of underweight girls, 33% of girls with weight within range defined as normal, and most often the dieting girls were overweight (66.7%). For overweight participants, body weight reduction seems appropriate. However, it should be emphasized that the method of weight reduction should be consistent with the principles of proper nutrition and carried out in a manner that is safe for health and development. Studies show, however, that girls often display various types of behavior dangerous to health to reduce body weight (Maoyong & Yanhong, 2015; Trojanowska et al., 2017). A disturbing phenomenon was the fact that even among girls with a normal body weight, every one third used slimming diets. The decision about the need to reduce body weight in girls with normal body weight could be due to a subjective assessment of their weight status and not to the objective value of BMI.
Dieting is a common phenomenon, even among young girls with weight within range defined as normal (Balantekin et al., 2018; Eaton et al., 2012). Irregularities in meeting the nutritional need and attitude toward one’s own body are referred to as ARS. Its diagnosis helps in the early identification of people at a higher risk of developing full-blown anorexia. In the presented study, using the Questionnaire for Testing Individual Attitude Toward Eating designed by Ziółkowska (2001), after diagnosing the occurrence of ARS and its level among the respondents, we found that it occurred in medium or high degree in as much as 63.1% of the subjects. Girls with excessive weight (83.3%) were more likely to have a medium or high ARS score. These results are consistent with other studies (Chalcarz et al., 2007, 2014; Merkiel et al., 2014). High scores for ARS occurred in 7% to 10% of respondents, and medium scores in 50% of respondents. Based on our own study, it can be concluded that this risk group includes not only girls with low body weight. In the present study, ARS was more often found among participants who were classified as overweight and at the upper end of normal weight standards. Early identification of people at increased risk of eating disorders enables appropriate preventive measures and can prevent the occurrence of the disease (Rienecke, 2017). It can also prevent the use of slimming diets, which cause dysregulation of basic metabolism, and may later manifest itself in an increased tendency to excessive weight gain. It has been shown that teenagers who used a reduction diet had a greater risk of developing obesity compared with adolescents who did not use diets (Neumark-Sztainer et al., 2007; Spear, 2006).
Conclusion
Weight status significantly affected the way girls perceive their body, and girls with a higher body weight had a more critical attitude toward their appearance. However, the lack of body satisfaction also applies to girls with lower body weight. Also among girls with weight within range defined as normal, the approach to “body self” differed, depending on whether the BMI value was below or above the 50th percentile.
Almost every fourth respondent could not interpret her body weight properly. The overweight and obese girls interpreted their body weight most accurately, as they most often declared their desire to reduce their weight and used slimming diets. Undesirable forms of weight reduction lead to a dysregulation of metabolism, as evidenced by a significant percentage of girls with excessive body weight who have undergone ineffective dieting.
Given the perceived sense of unattractiveness of the face appearance in the slimmest girls, who less often have objections to their body shape, it seems that in the case of satisfactory assessment of the modifiable body parts, they transfer the sense of unattractiveness to the unmodifiable body parts (here: face appearance).
Regardless of weight status, education about maintaining a healthy body and healthy body perceptions is important to healthy eating behaviors and development of adolescent girls. This would help to improve their self-esteem and reduce unhealthy practices aimed at weight reduction that are unnecessary and adverse to health, growth, and development.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.