
Abstract
This time and motion study aimed to explore the nursing workflow of intensive care unit (ICU) registered nurses in mainland China. We identified 107 kinds of nursing activity (six categories and 20 subcategories), observed 30 nurses for a total period of 580.8 hr, and analyzed 5,588 nursing activities. The nurses spent most of their time in direct nursing care (51.27% of the total working time), nursing documentation (17.91%), and communication (17.61%). Direct nursing care was the most time-consuming activity between 5:00 and 7:00 a.m. and the least time-consuming between 12:00 and 1:00 p.m. and 1:00 and 2:00 a.m. Although nursing records were kept by an information system, documentation still required a large percentage of the nurses’ working time. It was found that the time-consumption for each nursing activity varied during the day among the studied Chinese ICUs. Hence, nursing managers should arrange shift dynamics based on nurses’ actual workflow and load.
Introduction
Knowledge in nursing workflow is important for nursing management and human allocation (Qian et al., 2012). It is defined by a wide range of steps or activities that health nursing staff perform to care for their patients (Zheng et al., 2010), namely, the time and frequency of daily activities in a nursing ward. The working hours nurses spend with patients are associated with nursing care quality and patients’ safety (Cho et al., 2016). In particular, patients in intensive care units (ICUs) are more prone to experience worsening health conditions owing to disease changes; the majority of patients in ICU are at high risk for death (Gooch & Kahn, 2014). Kvande et al. (2017) showed that the time nurses spend at patients’ bedside is critical to identify important signs regarding patients’ condition, hence showing the importance of nurses’ working hours spent with clients, especially in the ICU context. Therefore, the distribution and duration of nursing activities in the ICU context are important to be researched. In this regard, the researchers’ observation of the workflow of nursing staff could be an effective way to identify possible redundant and inefficient processes.
Currently, general expectations and requirements regarding the quality of health care have been rising, leading patients to require increasingly improved nursing care quality and efficiency. These have transformed nursing service quality requirements and advanced the nurse engineering field (Chen et al., 2014). The application of information system can make a clearer division of nursing work, reduce human errors in nursing work, and help nurses improve work efficiency and decision support (D’Agostino et al., 2013). Waneka and Spetz (2010) made a systematic review of 74 literatures, and the results showed that information technology can reduce medication errors, with nurses being more satisfied with it.
Professional, timely, and effective life support and nursing care quality are essential for patient well-being and quality of life (Wang et al., 2016). Therefore, hospitals have experienced a substantial push toward adopting information technology into their health care procedures (Chen, 2017). Such an extensive application of information technology to the medical and health fields has allowed for further scientific management from researchers and nursing care quality control from the management. In December 2017, this research setting successfully instituted a mobile nursing system, a nursing management system, and an intensive care information system. The latter was shown to be able to perform most nurses’ tasks and responsibilities in an ICU context and also improve the intensive care efficiency and nursing care quality (Wang et al., 2016).
With the application of information technology, informatization has been embedded in many nursing activities, hence modifying the workflow of nurses in ICUs. Hains et al. (2012) conducted interviews with 66 doctors and nurses in three ICUs. The results showed that the information which is accessible to the patient could potentially improve the communication processes and change the efficiency of work processes. Conroy et al. (2015) introduced a valid ICU e-checklist into the morning rounds, and the delivery of essential daily care processes was improved. Kai-Hsuan et al. (2020) found that the handover times were shortened and the workflow was changed after conducting an informatics system combined with an automatic reminder.
However, there is little evidence regarding the workflow and time structure of ICU nurses from Asian countries, including China, when they utilize the intensive care information system to care for patients. Therefore, this study aimed to determine ICU nurses’ time structure and work low in China. Specifically, we analyzed ICU nurses’ daily activities regarding their types and duration, as well as nurses’ daily work time structure. Our final goal is to provide an objective, unified, and reasonable framework to be referenced by Chinese nursing and hospital managers when trying to improve the quality and management of their nursing care services.
Method
Design
This was a prospective, observational, and time and motion study. In such a design, the observer (researcher) continuously watches one individual, records each of the individual’s behavior, and notes the time taken for the individual to complete each behavior from beginning to end (Qian & Yu, 2014). This method enables one’s different behaviors to be assessed according to their flow, duration (i.e., the time required to complete the behavior), and frequency (Qian & Yu, 2014).
Setting and Participants
This study was performed in the nine ICUs of a comprehensive tertiary hospital in Beijing, China, which has 1,159 beds and 40 inpatient units. All nine ICUs had their nursing workflow analyzed. In total, 96 beds and 277 registered nurses worked in those ICUs (details in Table 1). Regarding management, each ICU comprised one nurse manager and varied number of charge nurses, with the latter being responsible for nurses’ primary tasks. One ICU (neurology) had a daily work shift that lasted from 8:00 a.m. to 8:00 p.m. and a night shift that lasted from 8:00 p.m. to 8:00 a.m. (of the next day). The other ICUs had three daily shifts: a day shift from 8:00 a.m. to 5:00 p.m., 5:00 p.m. to 1:00 a.m. of the next day for the middle shift, and 1:00 a.m. to 8:00 a.m. for the night shift.
Details of ICUs.

Note. ICU = intensive care unit.
In each of these ICUs, information technology has been embedded into nurses’ workflows. Most nursing activities are now performed through an intensive care information system and a personal digital assistant (PDA), which have helped to make such activities more convenient and efficient. For example, a nurse’s work flow for an intravenous infusion procedure in this hospital is as follows: check the physician’s orders, use the PDA to verify liquid information, dispense the liquid, scan the two-dimensional code for the drug label, and finally scan the patient’s wristband by the PDA. After infusion, the PDA is used again to scan the drug label to identify the completion of the infusion procedure. The intravenous infusion started with drug verification and ended with the verification of the infusion, and all verifications were performed by the PDA.
Classification of Nursing Activities
Nursing activities refer to specific behaviors or actions taken by nurses to implement nursing measures and promote patients’ progress toward expected outcomes (Butcher et al., 2018). The nursing activities are sorted or arranged into different groups according to the relationship between nursing activities so as to facilitate the overall analysis (Butcher et al., 2018). The correct identification of nursing activities is the basis of the accurate record of the nursing workflow, which is essential to carry out the time and motion study. Two steps were used to develop the classification system of nursing activities.
Step 1
Two researchers adopted a literature review method to retrieve data from the China National Knowledge Infrastructure and the Wanfang databases regarding nursing activities; the following search terms were used: “Intensive care unit,” “care unit,” “ICU,” “nursing time,” “nursing item,” and “operation item.” The data were collected on July 31, 2018. Two researchers read the literature to extract classifications for nursing activities, including the interpretation of hygiene policies, regulations, and plans introduced by the National Health Commission of the People’s Republic of China (2016; Munyisia et al., 2011, 2014; Yu et al., 2019). A list of 143 nursing activities was produced through the literature review and group discussion.
Step 2
To ensure the reliability and feasibility of the classification list, a panel of experts composed of ICU nursing managers and nursing department members discussed the activities proposed in Step 1. The results yielded 107 nursing activities, six categories, and 20 subcategories. The categories were direct nursing care, indirect nursing care, nursing documentation, communication, and personal and miscellaneous affairs (Table 2).
Categorization of ICU Nursing Activities.

Note. ICU = intensive care unit.
The terms direct and indirect nursing care were defined based on previous studies (Helgheim et al., 2018; Westbrook & Ampt, 2009). Direct nursing care refers to activities in which the nurses spend time with the patient and/or the patient’s family; indirect nursing care refers to activities that are not applied directly to patients or are performed in preparation to engage in direct nursing care. Based on previous literature (Meiqin et al., 2014), nursing documentation and communication refer to activities not related to patients’ care, but must be completed to ensure the provision of high-quality nursing care. Personal affairs refer to nonproductive activities, including inevitable delay and necessary rest time. Finally, to acquire enough granularity, we added the miscellaneous category to measure some of the low-frequency activities.
Study Procedures
In total, 27 researches majoring in nursing served as observers (5 graduates, 10 undergraduates, and 12 associates) to collect the data. A paper-based form was designed based on the list of nursing activities. The data collection form included columns for recording the start and end time of every activity. Before the field observation, the researchers collectively trained the observers by detailing the purpose, significance, and study research tools. We explained the items in each workload measurement form, demonstrated how to use the stopwatch measuring tool, identified the major workload content, and the ICU shift time periods. In this manner, we ensured that the observers utilized standardized methods and scales.
From September 24 to September 28 (5 days), 2018, observers were required to arrive at the nursing station 10 min before the start of each shift and identify one on-duty nurse for observation. Thirty nurses in charge were observed 79 times during this time period.
Data Analysis
Statistical analysis was performed using SPSS 24.0 (SPSS Inc., Chicago, IL, USA). Variables were expressed as percentages (%) and 95% confidence interval was calculated.
Descriptive statistics were applied to indicate how ICU nurses distributed their time across different nursing activities. The time and frequency spent by nurses on each activity were expressed as percentages (%); 95% confidence interval of these percentages was calculated.
Ethical Approval
This study was conducted with the approval of the ethics committees of Xuanwu Hospital, Capital Medical University. The nurses who were observed participated voluntarily and were informed that they could terminate participation at any moment without prejudice. Moreover, we ensured participants that their data would remain confidential and that their data would be used solely within the context of this study.
Results
During the 5-day observations, data on 30 charge nurses’ workflow were collected; hence, 5,588 nursing activities were recorded and with a total of 580.8 hr of observation. The average age of the nurses was 30.23 ± 3.51 years, and the average work experience was 8.07 ± 4.04 years. Most nurses (20/30; 66.7%) had associate degrees. In the participating hospital, nurses were graded from 1 to 9 based on their comprehensive capacities (Han et al., 2018)—Grade 1 was used for primary nurses and Grade 9 was used for clinical nursing experts. In our sample, most nurses were graded 4–6 (20/30; 66.7%).
Time Allocation for Nursing Activities
Nurses spent most of their time in direct nursing care and nursing documentation and communication activities, which occupied 51.27%, 17.91%, and 17.61% of their total work time period, respectively. Personal and miscellaneous affairs accounted for 2.42% and 3.48% of their total work time period, respectively (Figure 1).

Time allocation for the six categories of nursing activities.
Among direct nursing care activities, basic nursing, basic operations, and administrative operations accounted for 11.27%, 19.73%, and 9.71% of their total work time period, respectively. Moreover, both the frequency of and the time spent in these three activities were higher than those of other nursing activities (Table 3).
Time Allocation of Different Nursing Activities.
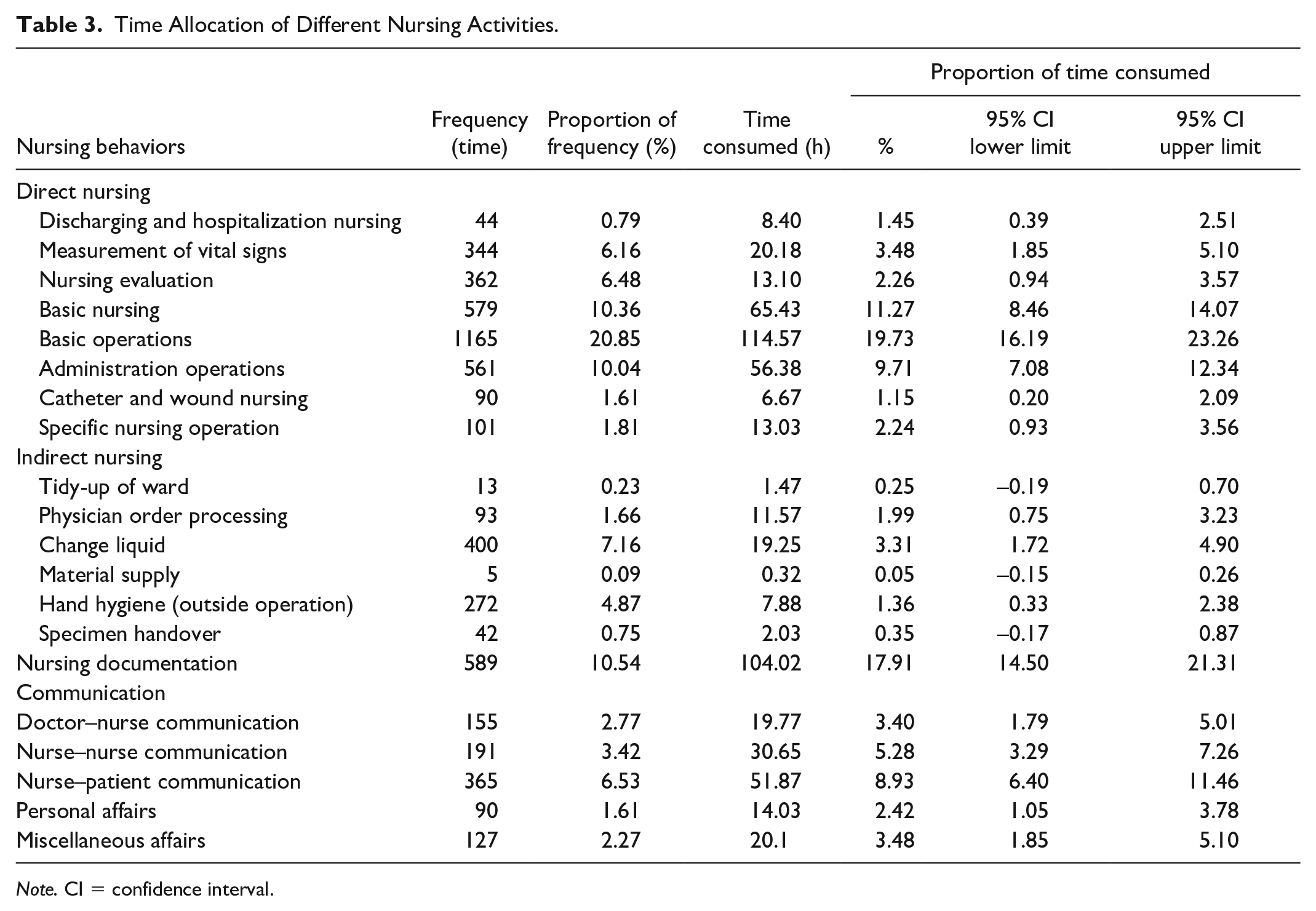
Note. CI = confidence interval.
Among indirect nursing care activities, changing liquid and physician order processing accounted for 3.31% and 1.99% of their total work time period, respectively. Nurse–patient communication accounted for 8.93% of their total work time period, hence the most time-consuming communication activity. In addition, doctor–nurse and nurse–nurse communication accounted for the remainder of the time consumed by communication activities, 3.40% and 5.28%, respectively (Table 3).
Nursing Activities in Different Departments
Direct nursing care exceeded 50% of nurses’ total work time period in the neurology (55.56%), neurosurgery (70.84%), functional neurosurgery (55.88%), general surgery (63.27%), and emergency (51.43%) ICUs. Indirect nursing care had its highest percentages for the aforementioned variable: 9.16% in neurosurgery and 11.11% in vascular surgery ICUs. Nursing documentation had its highest percentages for the said variable: 22.10% in neurology, 27.46%, in vascular surgery, and 20.44%, in gastroenterology ICUs. Communication showed its highest percentages for direct nursing care: 30.55%, 22.32%, and 20.53% in the cardiac, emergency, and gastroenterology ICUs, respectively. Personal affairs showed its highest percentages for the aforementioned variable in the neurology (4.95%) and functional neurosurgery (4.46%) ICUs. Moreover, the order from highest to lowest for time-consumption for all six categories of nursing activities is as follows: direct nursing care > nursing documentation > communication > indirect nursing care > personal affairs > miscellaneous affairs. Direct nursing care was the most time-consuming activity, whereas miscellaneous affairs was the least (Table 4).
Time Allocation of Different Nursing Activities for Different Departments.

Note. ICU = intensive care unit.
Distribution of Nursing Activities by Time of Day
Figure 2 shows that direct nursing care, indirect nursing care, nursing documentation, as well as communication occurred many times a day. From 5:00 a.m. to 7:00 a.m., direct nursing care occupied most of nurses’ time; from 1:00 a.m. to 2:00 a.m. and from 12:00 a.m. to 1:00 p.m., it occupied the least. From 6:00 p.m. to 9:00 p.m., indirect nursing care occupied most of their time. From 11:00 a.m. to 1:00 p.m., nursing documentation occupied the least of their time. From 7:00 a.m. to 9:00 a.m., communication occupied most of their time; from 5:00 a.m. to 7:00 a.m., it occupied the least. Figure 3 shows the time-consumption percentages of different nursing behaviors at different times of the day.

Percentage of time consumed by different nursing activities at different times of the day: (A) direct nursing, (B) indirect nursing, (C) nursing documentation, and (D) communication.

Percentage of time consumed by different nursing activities at different times of the day.
Discussion
To the best of our knowledge, this is the first study to analyze the nursing workflow and time structure in ICUs after the intensive care information system was applied in mainland China. This study analyzed most nursing activities that ICU charge nurses perform in a comprehensive tertiary hospital in the country. The analyses included classifying the nursing activities found through literature review and assessment of the time-consuming percentages of each of the nursing activities and their frequencies.
Currently, we know that a structured and scientific classification of nursing activities is essential for accurate measurement of nurses’ time structure and workflow. Literature review and group discussion can ensure that the formed nursing activities are comprehensive, and expert meetings can help make the formed nursing activities more credible. Hence, this study employed the principles of standardization (Li et al., 2015,). A list of nursing activities and classifications was identified. We used these classifications to ensure observers in our study could accurately measure the start and stop points for each nursing activity. It would be useful for hospital unit organization and nursing work redesign to introduce these classifications.
In this study, the results showed that direct nursing care was the most time-consuming activity in the ICU nursing context (51.27%, 95% confidence interval [CI]: [46.83%, 55.71%]). Hence, our results corroborate those of a previous research performed in Finland (Antinaho et al., 2015). In that study, nurses spend 38% of total nursing time on direct care, which is lower than the results of our study. This may be due to the fact that the former’s data are from the general ward. However, direct nursing care is still the most time-consuming (Antinaho et al., 2015). Li et al. (2015) analyzed the ICU medical staff work time structure to show that the most time-consuming activity was professional communication, followed by direct care. The discrepancy between our results and those of the cited study may be owed to the differences in the focus of each study; the cited study focused on physicians’ role and function in the ICU context. When compared, it is clear that physicians and nurses have different roles and functions. Regarding the highlighted discrepancy, we believe that the most relevant differences relate to the fact that physicians often need to communicate with patients, patients’ families, and nurses, whereas nurses need to complete a wider array of operations (i.e., patient medication, evaluation, and observation). In addition, Chinese nurses are usually assigned to look after several patients in ICUs, which is a context that requires many face-to-face nursing care activities. Nurses’ personal and miscellaneous affairs do not have a direct effect on patients—these activities are unavoidable in daily nursing practice (Meiqin et al., 2014). Our results showed that only 6% of nurses’ working time was dedicated to personal and miscellaneous affairs. We believe that these time costs will not influence nursing quality. Previous studies proved that nurses’ time spent on direct care is related to nursing quality and satisfaction of patients’ outcomes (Cho et al., 2016; Hockenberry & Becker, 2016). Moreover, Vahakangas et al. (2008) demonstrated that direct nursing care was the most influential activity of patient outcomes. To further improve patient care by strengthening basic nursing and improving nursing care services, the Chinese government has developed a project for quality care demonstration (Ma, 2010). The Chinese government staff indicated that nursing work should be dominated by direct nursing care (Wu et al., 2011). Our results were consistent with the requirement of most hospitals in mainland China. Therefore, it is reasonable and necessary for nurses to spend enough time on direct care activities.
Our results also showed that the amount of time spent by nurses in each of the nursing activities differed among different ICU departments; nevertheless, a general assessment showed that from the highest to lowest, the order for time-consumption of the six types of nursing activities is as follows: direct nursing care > nursing documentation > communication > indirect nursing care > personal affairs > miscellaneous affairs. Regarding nursing documentation time-consumption, when compared to manual documentation, the application of an intensive care information system was shown to significantly shorten the time spent by nurses on documentation procedures from 3.8 to 2.05 hr in a 12-hr period (Qin et al., 2017). However, in our study, registered nurses still had to spend a great deal of time on documentation, especially during the night shift, which is consistent with those of a Brazilian study on ICUs (Kakushi & Evora, 2014). This may be due to the fact that ICUs tend to receive special and critical patients that have difficult treatments for their diseases. Moreover, the heart rate and blood pressure of patients in ICU may be slowed down due to the autonomic nervous regulation during the night, which can easily aggravate the disease Nurses, therefore, have to dedicate more time to record patients’ vital signs and to analyze and record symptomatic/disease changes. Furthermore, information documentation modules in the intensive care information system need to be optimized to reduce the time of nursing documentation.
Regarding the time of the day in which nurses dedicated to specific activities, direct nursing care was shown to be mostly performed between 5:00 a.m. and 7:00 a.m. This refers to the period in which nurses need to comprehensively re-evaluate patients and organize bed units and wards before the next shift starts. Direct nursing care was least performed between 11:00 a.m. and 1:00 p.m., which is their lunch break. Regarding indirect nursing care, it was least performed between 8:00 a.m. to 9:00 a.m. and 5:00 p.m. to 6:00 p.m.; these two periods refer to the connections between day and night shifts. As for nursing documentation, it was mostly performed between 11:00 p.m. and 12:00 p.m.; this is because night shift work requires nurses to record patients’ condition changes more frequently. Regarding communication, it was mostly performed between 7:00 a.m. and 8:00 a.m. and least performed between 6:00 a.m. and 7:00 a.m. because of the shift handover. Based on these results, we were able to identify labor-intensive periods; hence, we suggest nursing managers should increase the proportion of staff during the labor-intensive periods to maximize efficiency and ensure appropriate work completion, as well as appropriately reduce the redundant staff during the more idle periods. A study conducted by Liang and Liang (2016) showed that dynamic allocation of manpower according to nursing hours could improve the enthusiasm of nurses. We do believe that the workflow and time structure provided by our results could guide nursing managers in decision-making regarding shift dynamics so as to create workflows that are confluent with nurses’ actual daily activities and work-load.
Limitations
Although we have outlined significant contributions to current theoretical research, this study also has some limitations. First, the lack of data before the implementation of the intensive care mobile information system made it impossible for us to quantitatively determine whether its implementation improved nursing care services quality or efficiency. Hence, future studies are warranted to compare our data with future data from more advanced information systems and subsequently allow for more accurate reflections over the influence of mobile information systems on nursing workflow. Second, this study assessed the ICU departments of only one comprehensive tertiary hospital; thus, the results may not reflect the time allocation of nursing activities and nurses’ workflows in hospitals with different grades or in different regions. Third, although we described nursing workflow and time structure in the ICU context, we did not describe nor analyze interruptions in nursing activities. Fourth, even though there was a positive relationship between the observers and the observed, the Hawthorne effect cannot be avoided in its entirety (Sedgwick & Greenwood, 2015). This means the observed nurses may have changed their routine activities (compared to their daily normal routines) during the observations. However, this is a limitation to all time and motion studies that use artificial observation.
Conclusion
This study observed and analyzed nursing care services time structure and workflow for ICU registered nurses in mainland China and found that nurses spent most of their time in direct nursing care, nursing documentation, and communication activities. Although nursing records/documentation were entered via an intensive care information system, this activity still occupied a large percentage of their working time. In addition, throughout a daily nursing shift in the studied Chinese ICUs, each nursing activity was the most or the least time-consuming in different and specific times during the day or night. Thus, nursing managers need to arrange shift dynamics to accommodate labor needs.
Footnotes
Acknowledgements
We thank the ICU nurses of Xuanwu Hospital, Capital Medical University for their voluntary participation in the study, as well as the nursing managers of the hospital for supporting the smooth completion of the study.
Author Contributions
B.H. and G.Z. contributed to the study concept and design. Q.L. and X.C. contributed to the acquisition of data and analysis and interpretation of data. B.H. and Q.L. contributed to the drafting of the manuscript. B.H. and G.Z. contributed to the critical revision of the manuscript for important intellectual content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.