
Abstract
This study aimed to develop a questionnaire to evaluate person-centered critical care nursing from a patient perspective (PCCNPq). We created a 26-item preliminary questionnaire based on a literature review and qualitative interviews and administered it to 411 patients who had experienced critical care. We assessed the questionnaire’s reliability and validity using exploratory factor analysis and confirmatory factor analysis and tested internal consistency and test–retest reliability. The final version of the PCCNPq comprised five factors: compassion, expertise, communication, comfort, and respect. The model fit was satisfactory, and the items demonstrated good convergent and discriminant validity. In conclusion, the 20-item PCCNPq has acceptable reliability and validity and is applicable for assessing person-centered critical care nursing from a patient perspective.
Introduction
Critically ill patients receive treatment in the intensive care unit (ICU) where they are closely monitored and managed by medical staff 24 hr a day. In the ICU setting, patients not only experience physiological stress but also other negative situations such as isolation from the family, lack of autonomy, or impersonal treatment. According to qualitative studies (Aro et al., 2012; Rattray et al., 2004), ICU patients experience loneliness, likened to being alone on a desert island, and frustration because of their limited capacity for self-care and may experience hallucinations and nightmares. Some patients who find the ICU setting impersonal perceived their lives to be dependent on machines. Furthermore, the trend toward light sedation, which has enabled consciousness to be maintained during highly complex procedures such as mechanical ventilation and cardiopulmonary bypass (Kress et al., 2000), allows patients to remember more of their ICU experience. Negative experiences in the ICU can affect the quality of life as well as the cognitive, mental, and physical health of survivors after discharge (Aro et al., 2012; Granja et al., 2005).
Person-centered care (PCC) has attracted attention as it emphasizes the importance of the patient experience. PCC recognizes and respects the value of individual patients and engages patients in decision-making about their own treatment and care by establishing a trusting relationship (Morgan & Yoder, 2012). Lusk and Fater (2013) suggested “communication and listening,” “treating the patient as a unique individual,” “teaching/learning,” “respecting values,” and “responding to patient needs” as factors of PCC. Researchers have also proposed the application of PCC in various settings, including oncology nursing and elderly care (Kogan et al., 2016; Radwin et al., 2003). In particular, the critical care environment involves additional considerations as patients are separated from their families and communication is limited. Jakimowicz and Perry (2015) assessed the characteristics of critically ill patients, the unique ICU environment, and nurses’ competence with regard to the person-centered concept in the critical care setting. They identified patient identity, biomedical nursing practice, compassionate presence, and professional presence as the defining attributes of person-centered critical care nursing (PCCN). The concept of PCCN to enhance patient experience not only served as the basis for measuring PCC performance of critical care nurses (Kang, Cho, et al., 2018a) but also increased the interest in family-centered critical care (Coombs et al., 2017; Mitchell et al., 2016).
The increasing interest in PCC led to the development of several tools for its quantitative measurement, including the Individualized Care Scale (ICS; Suhonen et al., 2005), the Oncology Patients’ Perceptions of the Quality of Nursing Care Scale (Radwin et al., 2003), the Person-Centered Climate Questionnaire (Edvardsson et al., 2008), and the Person-Centered Critical Care Nursing Questionnaire (PCCNQ; Kang, Cho, et al., 2018a). Among these tools, the PCCNQ reflects the characteristics of critical care nursing, and its reliability and validity have been assessed in Korea. This tool was used to recently assess the relationship between PCCN and family’s satisfaction (Kang & Shin, 2019) and nursing work environment (Kang & Lim, 2019). However, the PCCNQ evaluates the degree of nursing care performed by critical care nurses and does not reflect patient perception. Perception of the care provided may differ between nurses and patients (Weiss et al., 2010), and the degree of PCC perceived by patients is significantly different from that of nurses (Sidani et al., 2016). The core of the PCC concept is regarding the patient as a person, and thus it is important to evaluate PCCN from a critical patient perspective. Accordingly, this study aimed to develop a questionnaire to measure PCCN from a patient perspective and to validate its psychometric properties.
Method
Study Design and Ethical Considerations
We conducted a methodological study to develop the Person-centered Critical Care Nursing perceived by Patient Questionnaire (PCCNPq). We used the seven steps described by DeVellis (2016) as a guide to the scale-development process, as follows: Step 1: Determining the concept; Step 2: Generating an item pool; Step 3: Determining the measurement format; Step 4: Expert reviews; Step 5: Considering the inclusion of items; Step 6: Administering the items to a sample of patients; and Step 7: Evaluating the items. We used Steps 1 to 5 to develop the preliminary questionnaire during Phase 1 and Steps 6 and 7 to evaluate the psychometric properties of the questionnaire during Phase 2.
The Institutional Review Board of Dong-A University approved the study protocol (Approval number: 2-1040709-AB-N-01-201805-HR-004-02). We informed all participants of the purpose and procedure of the study and obtained informed consent to participate.
Phase 1: Development of Preliminary Questionnaire
Conceptual Framework and Item Generation
We defined the concept of PCCN and established its constructs by reviewing relevant literature, including Jakimowicz and Perry’s (2015) concept analysis and Hong and Kang’s (2018) deductive content analysis. First, we defined PCCN as “being respected as a unique individual, and being provided with advocacy, compassion, and comfort from professional nursing staff.”
The constructs of the PCCN concept were “Compassion,” “Expertise,” “Communication,” “Respect,” and “Comfort.” Compassion means that nurses understand the patient’s position and provide emotional support for relief (Hudon et al., 2011; Jakimowicz & Perry, 2015). Expertise means that nurses provide nursing care based on their biomedical knowledge and ensure safety and prompt treatment, even in emergencies (Davidson et al., 2007; Hong & Kang, 2018; Jakimowicz & Perry, 2015). Communication means that the medical staff interact with the patient and advocate for the patient (Hong & Kang, 2018; Morgan & Yoder, 2012; Slatore et al., 2012). Jakimowicz and Perry (2015) considered communication as one of the features of professional presence. “Respect,” a representative construct of person-centered nursing (Morgan & Yoder, 2012), recognizes the patient as a unique individual and allows the family to participate in patient care and treatment (Hong & Kang, 2018; Jakimowicz & Perry, 2015). Finally, “Comfort,” which was an aspect of patient identity in Jakimowicz and Perry’s (2015) concept analysis, ensures physical and mental well-being in the ICU (Hong & Kang, 2018; Kang, Cho, et al., 2018a).
Based on the above conceptual framework, we initially generated 30 initial items. Of these, we adopted nine items from existing questionnaires on PCC (Edvardsson et al., 2008; Kang, Cho, et al., 2018a; Radwin et al., 2003; Rattray et al., 2004; Suhonen et al., 2005) and created 21 items based on a review of the relevant literature (Aro et al., 2012; Hong & Kang, 2018; Jakimowicz & Perry, 2015; Slatore et al., 2012). All investigators were certified advanced practice critical care nurses with relevant knowledge and clinical experience. J.K. had previously developed a number of measurement tools, including a PCCN questionnaire, and was familiar with the item generation process.
Then, we conducted qualitative interviews with 10 ICU patients to reflect on specific and vivid experiences regarding the initial items. We interviewed six men and four women aged 18 to 79 years with varying diagnoses (e.g., myocardial infarction, lung cancer, and stroke). We conducted the interviews at the bedside after the patient consented to participate. The main topic of the interview was the patient’s experience of PCC during the hospital admission. Each interview took 20 to 30 min. One of the investigators (J.H.) conducted all of the interviews. After analyzing the contents of the interviews, we added 10 new items, bringing the total to 40, and revised the wording of some items to improve patient comprehension.
Assessment of Content Validity
A group of experts comprising a nursing professor, an ICU head nurse, and eight advanced practice nurses in critical care evaluated the content validity of the initial items. The item-level content validity index (I-CVI) ranged from .80 to 1.00, and the Scale’s Content Validity Averaging (S-CVI/Ave) value was .93. We removed 14 items with an I-CVI of less than .78 or overlapping content (Polit & Beck, 2006).
Pretest Questionnaire Refinement
Twenty ICU patients pretested the items being validated to ensure readability and understanding, appropriateness of item length, and response time. In addition, a Korean linguist modified the expression of some of the items to improve their readability. Finally, we created a preliminary questionnaire comprising 26 items.
Phase 2: Evaluation of the Psychometric Properties of the Questionnaire
Place/Participants
Patients admitted to the ICU participated in a survey using the preliminary questionnaire. The hospital was a university medical center located in Busan, South Korea, with about 1,000 beds. There were five adult ICUs, with a total of 80 beds, and there were 127 ICU nurses at the time of the survey.
The inclusion criteria were (a) age above 18 years, (b) more than 24 hr of ICU care, and (c) informed consent to participate in the study. The exclusion criteria were (a) difficulties in communication, (b) diagnosis of cognitive dysfunction such as dementia, and (c) discharge from the ICU more than 6 months previously.
Exploratory factor analysis (EFA) required a sample size of at least 5 to 10 times the number of items (Costello & Osborne, 2005), with a minimum sample size of 200 for confirmatory factor analysis (CFA; Myers et al., 2011). Therefore, a total of 400 participants was required, 200 per factor analysis. We administered the questionnaire to 440 participants to allow for a dropout rate of 10%. Of these, 29 participants provided no response or incomplete responses, and thus we used data from 411 participants for the final analysis. For the test–retest reliability analysis, we administered the PCCNPq again to 60 participants after 7 to 10 days (Marx et al., 2003).
Data Collection
We publicly recruited participants from June 18 to September 21, 2018, by posting fliers on the bulletin boards of ICUs, in-patient units, and outpatient clinics of the Dong-A university hospital. Once the patient had consented to participate, one of the investigators (J.H.) interviewed them at their bedside or in a designated room using a paper questionnaire. J.H. coded all the responses and entered them on a Microsoft Excel spreadsheet. The data did not include any personal identifiers of the study participants.
Statistical Analysis
We conducted all statistical analyses using IBM SPSS Statistics and IBM SPSS AMOS, version 24.0 (IBM Inc., Armonk, NY, USA). We assessed participant characteristics using descriptive statistics such as percentages, means, and standard deviations and assessed between-group differences using independent t tests and one-way analysis of variance. We used EFA and CFA to assess the construct validity of PCCNPq and evaluated the model fit (reference value) using the chi-square statistic (p > .05), chi-square minimum/degrees of freedom (CMIN/df ≤3.0), comparative fit index (CFI ≥.90), root mean square residual (RMR ≤.08), Tucker–Lewis index (TLI ≥.90), and the root mean square error of approximation (RMSEA ≤.08; Yu, 2012). We assessed the convergent validity based on standardized factor loadings, critical ratios, the average variance extracted (AVE), and construct reliability (CR) values. We evaluated the discriminant validity by comparing the square roots of the correlation coefficients between the factors and AVE values.
We assessed the criterion validity by calculating the correlation between PCCNPq and ICS using Pearson’s correlation coefficient. The ICS developed by Suhonen et al. (2005) and translated and validated in Korean by Yang (2008) is a 34-item, 5-point Likert-type scale self-report tool, with a higher score indicating more individualized care perceived by the subject. With respect to reliability, the ICS had Cronbach’s α of .89, according to a previous study (Yang, 2008) and had a Cronbach’s α of .89 to .91 in the current study.
Results
Participants’ Characteristics
A total of 411 ICU survivors with a mean age of 60.98 ± 13.00 years participated in the study. Of these, 268 (65.2%) were men. Using the random case selection function of the SPSS program, we randomly assigned 205 patients to the EFA group and 206 to the CFA group, with no significant difference in the characteristics of the two groups (Table 1).
Participant Characteristics (N = 411).

Note. EFA = exploratory factor analysis; CFA = confirmatory factor analysis; ICU = intensive care unit.
Item Analysis
None of the 26 preliminary items had extreme means or standard deviations, and the absolute values of kurtosis and skewness of all items ranged from 0.02 to 1.36. The item-total correlations were .51 to .75. All the above results satisfied the criteria for the item analysis (Field, 2013), and thus, we did not delete any item.
Validity
The data of the current study were fit for factor analysis because the Kaiser–Meyer–Olkin (KMO) value was .91, and the Bartlett’s sphere formation test result was χ2 = 3,527.59 (p < .001). We extracted the factors in EFA via principal components analysis and promax rotation. The number of factors was determined based on the eigenvalue, scree plot, and cumulative explained variance. We selected items with communality of .40 or higher and factor loadings of .40 or higher for each factor (Williams et al., 2010). In the three rounds of EFA, we deleted six items that did not meet the condition, resulting in five factors composed of 20 items, which accounted for 70.0% of the total variance. The five factors were compassion, expertise, communication, comfort, and respect, which reflected the content of the items and the conceptual framework. We initially classified the item, “I was able to listen to music or read books in the ICU” as a communication factor. However, this item’s meaning did not theoretically correspond to the communication factor, and thus, we reclassified it as a comfort factor (Tables 2 and 3).
Rotated Factor Pattern Matrix of Exploratory Factor Analysis (N = 205).

Note. ICU = intensive care unit.
Bold values indicate that the highest factor loadings of individual items.
Items Deleted from the Exploratory Factor Analysis.

Note. ICU = intensive care unit.
As a result of the CFA, the 20 items in five factors selected based on the EFA, the standardized factor loadings of all items were >.50, and the critical ratio was >1.97 (p < .05). In addition, each factor satisfied the model identification criterion because it contained more than three items. The measures of the model fit were as follows: χ2 = 352.99 (p < .05), CMIN/df = 2.21, CFI = .92, RMR = .06, TLI = .91, and RMSEA = .08. All fit indices met the recommended level, except for the sample size-sensitive chi-square statistics (Table 4).
Results of the Confirmatory Factor Analysis (N = 206).
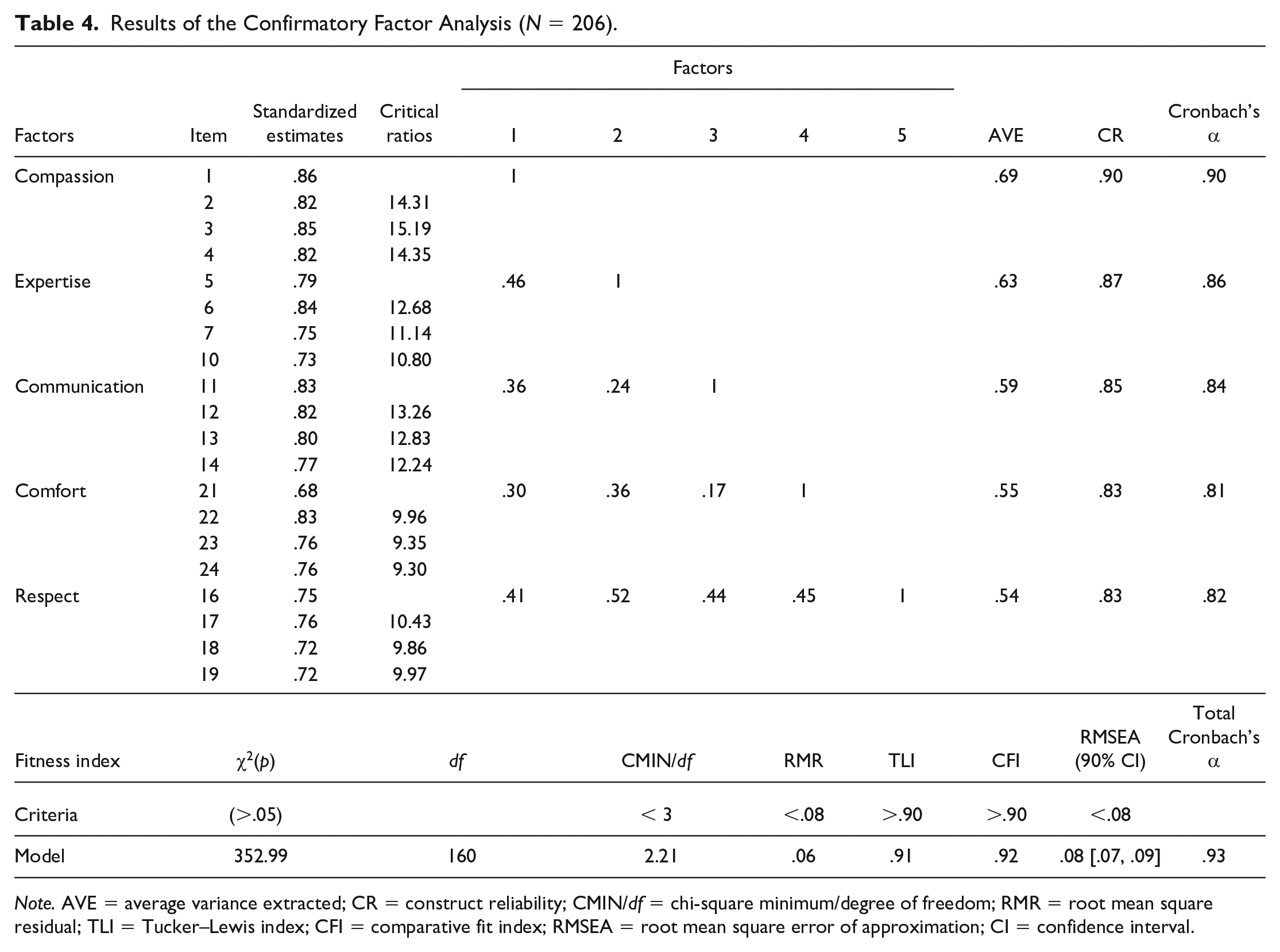
Note. AVE = average variance extracted; CR = construct reliability; CMIN/df = chi-square minimum/degree of freedom; RMR = root mean square residual; TLI = Tucker–Lewis index; CFI = comparative fit index; RMSEA = root mean square error of approximation; CI = confidence interval.
In the convergent validity analysis, the standardized factor loads (λ) of the item were .68 to .86, which exceeded the reference value of .50. The critical ratios were all >1.97, and the construct reliability was .83 to .90, which was higher than the reference value of .70. For the discriminant validity analysis, the largest square root of the correlation coefficients between the factors was .52, which was smaller than the lowest AVE value of .54 (Yu, 2012). Regarding the criterion validity, PCCNPq was highly correlated with ICS (r = .85; p < .001).
For internal consistency reliability of PCCNPq, we found a Cronbach’s α of .93. The Cronbach’s α values for each factor were .90 for compassion, .86 for expertise, .84 for communication, .81 for comfort, and .82 for respect (Table 4). We performed a retest to assess the stability of the PCCNPq. The correlation between the two measurements (r) was as high as .69 (p < .001).
Final Questionnaire
The final PCCNPq developed through the above process comprised five factors and 20 items (Table 5). Responses to each item are measured on a 4-point Likert-type scale (1 = strongly disagree, 2 = disagree, 3 = agree, 4 = strongly disagree), and the survey takes approximately 5 min. The mean score of PCCNPq in the current study was 2.94 ± 0.67. “Respect” had the highest score (3.04 ± 0.78), followed by “Expertise” (3.02 ± 0.75), “Compassion” (2.94 ± 0.90), “Communication” (2.80 ± 0.83), and finally, “Comfort” (2.78 ± 0.80).
Final Person-centered Critical Care Nursing Patient Version Questionnaire.

Note. ICU = intensive care unit.
Discussion
At the core of the PCC concept is regarding the patient as a person, and thus PCCN needs to be evaluated from a critical patient perspective. We developed a PCCNPq based on the conceptual framework of PCCN and evaluated its psychometric properties. The final PCCNPq was a five-factor, 20-item tool with adequate reliability and validity for measuring PCCN from a patient perspective. We performed EFA and CFA to assess the construct validity of the PCCNPq. When conducting EFA and CFA, it is desirable to assign different participants to the two sets of analyses (Swanson & Holton, 2005). In the current study, we tried to improve the robustness of the analysis by recruiting twice the number of participants required and randomly assigning them to the EFA or CFA group. The total variance explained of the five factors derived through EFA was 70.0%, exceeding the reference value of 60% (DeVellis, 2016).
During the EFA process, a total of six items were eliminated, including one item on “communication,” one on “respect,” two on “expertise,” and two on “comfort.” Each of these items had a factor loading value of <.40 and was thus nonrepresentative of the associated factor (Hair et al., 2018). We moved one item under “communication” to “comfort” in consideration of its theoretical relevance (Çiftçi & Öztunç, 2015). The fitness of the factor structure reflecting this shift was satisfactory for all indices other than chi-square, which is sensitive to the sample size. The results of the convergent validity and discriminant validity analyses revealed a high correlation between the items constituting the same factor of the PCCNPq and a low correlation between items that belonged to different factors. We also found that the PCCNPq measured a concept similar to that assessed by the ICS, a commonly used tool for measuring general PCC. These results indicate that the construct validity of PCCNPq is acceptable.
The five factors of the PCCNPq developed in the current study are similar to those of other PCC measurement tools, including the PCCNQ. This is because the basic definition and structure of PCC do not depend on the individual or the environment. Although some factors were common to both the nurse version of PCCNQ and the PCCNPq, some specific items were different. For example, both versions included “compassion,” and it was the factor that explained the largest portion of the variance. In the nurse version, the items of compassion comprised words and behaviors such as “talk to the patient and family about everyday topics” and “try to make therapeutic contact with the patient and family” (Kang, Cho, et al., 2018a). This is consistent with the finding of a previous study (Weiss et al., 2010) that there was a significant difference in the perception of PCC between nurse providers and patients. The core of PCC is patients, and thus, nurses need to pay more attention to the person-centeredness of the patient perspective.
PCCNPq was developed for patients and differs from the PCCNQ for nurses in some important respects. The nurse version of the PCCNQ includes an “expertise” factor in the conceptual framework, but this factor was removed from the PCCNPq based on the EFA results. This may be because ICU nurses tend to view expertise as an essential qualification (Kang, Cho, et al., 2018a). However, patients considered outstanding competence, that is, expertise, as a major factor in PCCN (Hong & Kang, 2018). In the qualitative interviews conducted during the preparatory phase of the current study, the patients referred to the expertise of the critical care nurses, and we eventually included this as one of the factors of the PCCNPq. Expertise, which reflects the unique characteristics of critical care nursing (Jakimowicz & Perry, 2015), is a factor that is not included in previous PCC instruments.
The comfort factor of the PCCNPq contains items on the ICU environment. ICU patients are exposed to mechanical noise, unpleasant odors, and bright lighting, and such environmental stimuli lead to sleep disturbances and psychological stress (Tembo et al., 2015). Recent meta-analytical studies (Kang, Lee, et al., 2018b; Younis et al., 2019) have reported that multifaceted interventions, including ICU environmental management, were more effective for improving sleep and preventing delirium in critical care patients than single interventions such as medication or earplugs. Therefore, interventions for improving the physical environment of the ICU are essential to ensure person-centered critical care.
Critically ill patients often have difficulty communicating due to the severity of their condition, sedation, endotracheal intubation, or invasive interventions (Happ et al., 2004). Thus, critical care nurses need to use nonverbal communication and plain terminology to improve the understanding by the patient and their family (Hong & Kang, 2018). The items of the Communication factor in the PCCNPq provide a good reflection of these communication characteristics in the ICU setting. The Respect factor in the PCCNPq includes items such as “calling patients by name” and “consideration for the family.” Patients in ICUs are sometimes treated impersonally, such as being called by a diagnosis or a bed number instead of by name (O’Connell & Landers, 2008). Because traditional ICUs are open spaces, several patients lie in a connected space, limiting patient privacy.
Also, many ICUs in Korea impose visiting hours. Because patients and families have their own unique culture, allowing family involvement, which is a crucial aspect of respect for patients (Mitchell et al., 2016), can improve the quality of nursing care (White et al., 2012). The Respect factor can be interpreted differently for each country or culture. Therefore, the PCCNPq developed in the current study should be revised according to corresponding cultural differences before it is applied in other countries.
This study is significant in that it developed a reliable and valid tool to measure PCCN from the patient perspective. Critical care has aspects that are distinct from general nursing, and this should be reflected in the development of assessment tools. The PCCNPq items reflect the unique characteristics of critical care nursing such as nonverbal communication and family involvement. The good reliability and validity of the PCCNPq makes it applicable to assess PCC in the ICU setting. Critical care nurses can use the PCCNPq to enhance their understanding of nursing to improve patient experience and also to develop and evaluate standardized PCCN interventions.
Despite these advantages, this study also has some limitations. First, we recruited the participants from a university hospital, and thus the generalizability of the results should be interpreted with caution. Second, due to the lack of empirical studies on PCC in critical patients, we could not evaluate known-groups validity. Future studies need to be conducted on the influencing factors and outcomes of PCCN and differences between patients and nurses in their perception of PCCN. Third, the items of the PCCNPq may contain some culturally sensitive content. We recommend that the PCCNPq be culturally adapted for use in other countries. Finally, although the PCCNPq, which has been validated for patients in various ICUs including surgical and medical ICUs, is applicable to most adult critical care patients, some adjustments will be needed to apply it to critically ill pediatric patients to reflect additional attributes.
Conclusion
The five-factor, 20-item PCCNPq developed in this study can measure PCCN from the patient perspective with good reliability and validity. The PCCNPq can be used to assess PCC and its effects in critical care nursing practice and related research. Moreover, the PCCNPq can be used to identify the factors influencing PCC to evaluate the effects of person-centered nursing interventions. We need further studies to estimate the reliability and validity of PCCNPq using larger samples and test it in other cultures and countries.
Footnotes
Authors’ Contributions
J.H. was responsible for data collection and drafted the article. J.H. and J.K. contributed to the study conception and design, analyzed the data, and carried out critical revisions of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board of Dong-A university in South Korea (2-1040709-AB-N-01-201805-HR-004-02).
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No.NRF-2019R1A2C1011300). The funding source had no role in the study design, analysis, data interpretation, or decision to submit for publication.