
Abstract
The performance of a health system hinges upon effective and efficient allocation of resources. The nature of governance within the health system, including critical components such as purchasing mechanism of health care services, also determines the health status of program beneficiaries. This article investigates an existing purchasing mechanism of a state-funded health care scheme through the lens of governance. We applied framework method on an adapted version of a tool developed by the World Health Organization (WHO), Organizational Assessment for Improving and Strengthening Health Financing (OASIS), to draw four themes to study the status of purchasing mechanism in Madhya Pradesh (MP), India. We used purposive sampling to select subjects from the state, district, and block levels and conducted 32 in-depth interviews. Subjects from the district and block levels were drawn from a sample of three out of 51 districts in MP. We found that although the scheme is functional, it has immense scope for improvement, thereby bettering the health outcomes of its beneficiaries.
Introduction
Nations across the globe are constantly looking for ways to improve the performance of their health systems. Efficient and effective use of allocated resources is an important indicator to measure performance. More recently, governance within health care system is being increasingly regarded as another important yardstick to measure the health of health systems (Savedoff, 2011). According to the World Health Organization (WHO), governance in health sector constitutes a wide range of strategic and regulatory functions that are deemed important to achieve the goal of Universal Health Coverage (UHC; WHO, 2016a). The growing interest of governance in health sector is primarily driven by the need for increased accountability, owing to increased funding and demand for demonstrating results. Governance becomes equally important when a health system operates under limited resources. As such, a strategic purchasing mechanism under able government stewardship is more likely to produce efficient, effective, and equitable distribution of resources, translating to better health outcomes (Busse et al., 2007).
While purchasing is a mere allocation of resources, a strategic form of purchasing is closely “aligned to societal health needs and wishes, and results in the most cost-effective provision of services” (Figueras et al., 2005). Public procurement, a form of purchasing, comprises a large share of government spending. Globally, public procurement on an average accounts for 15% or more of the gross domestic product (GDP) and is higher (~29%) in the Organisation for Economic Co-operation and Development (OECD) countries (Hazarika & Jena, 2017). In India, it accounts anywhere between 20% and 30% of the GDP (Djankov et al., 2017; Hazarika & Jena, 2017; Khan, 2017), and almost 26% of the total health budget comprises purchase of goods and services made by the public sector (Sharma, 2012). By some estimates, the total procurement figure in India stands at around INR 11 trillion (Khan, 2017; Sharma, 2012). A sizable proportion of this expenditure is directed toward tertiary-level care, which comprises around 15% to 20% of India’s total health expenditure (THE) (National Health Systems Resource Center, 2016). Several states in India, including Madhya Pradesh (MP), have health financing mechanisms targeted toward tertiary-level care. Budget estimates to one such scheme are known to increase from INR 100 million in 1997–1998 to INR 800 million in 2013–2014 (Finance Department, Government of Madhya Pradesh, 2016a, 2016b). Given such high volume of purchase, it is important to have an effective and efficient public procurement system.
Based on evidence from various national-level studies, a study concluded that the quality of governance is a strong indicator of better health outcomes (Holmberg & Rothstein, 2011). Studies from India also reiterate the importance of governance, through need for containing corruption (Chattopadhyay, 2013) and “inter-sectorial and inter-ministerial coordination” (Ramani, 2014). Although governance seems to be a popular buzzword in policy circle, many believe it has been reduced to mere rhetoric instead of producing empirical evidence on its usefulness (Ranjan & Roy, 2015). Pyone et al. (2017) argue that “governance of health systems is a relatively new concept”; not much is known about governance in health purchasing mechanisms across India. This article aims to empirically understand the institutional architecture, management, and regulatory mechanisms in a state-financed health care grant-making scheme, called the State Illness Assistance Fund (SIAF), in MP through the lens of governance.
SIAF, launched in 1997–1998, is a state-funded scheme designed to provide grants for health care to people living below poverty line (BPL) in MP. Under SIAF, an eligible beneficiary receives cashless tertiary-level health care services with a provision of financial aid between INR 25,000 to INR 200,000. SIAF covers treatment and medicine cost (postsurgery medicines for 6 months) of 20 listed disease types (mostly noncommunicable diseases [NCDs]) through empanelled health institutions within and outside MP. MP being recognized as a high-focus state by the Government of India, we believe that the findings from this study could serve as a basis for the remaining eight states in this category, which is primarily distinguished by “persistently high child mortality and relatively poor socio-economic and health indicators” (Bora et al., 2019).
MP, India’s second largest state with an approximate area of 118,919 sq mi, is home to 72.5 million people. Approximately two-thirds of its population live in rural areas, and around 16% and 21% comprise schedule caste (SC) and schedule tribe (ST), respectively. Agriculture is the mainstay, which employs more than 70% of the working population (Government of India, 2020; Government of Madhya Pradesh, 2020; Office of the Registrar General & Census Commissioner, India [ORGI], n.d.a.). Compared with national-level estimates, MP has been one of the poor performing states (Table 1) (Office of the Registrar General & Census Commissioner, India [ORGI], 2016, n.d.b.). The THE in MP comprises around 4.2% of the state GDP. A large gap between urban and rural estimates in MP indicates that the state’s poor may be disproportionately disadvantaged compared with their urban counterparts.
Selected Health Indicators in Madhya Pradesh and India, 2014.
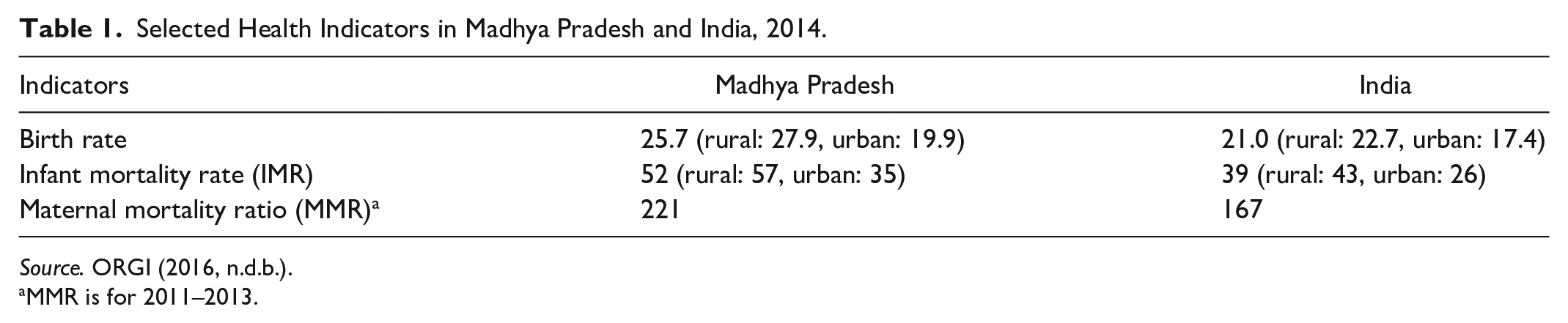
Source. ORGI (2016, n.d.b.).
MMR is for 2011–2013.
Method
Reviewing health system financing involves several aspects such as assessing how resources are mobilized, how risks are pooled, how health care goods and services are purchased, and how they are efficiently and equitably distributed (WHO, 2016b). To better understand the complexity of real-life health systems, existence of multiple perspectives on the issue of governance in purchasing, and the influence of local contexts that shape the functioning of a scheme, we used the framework method (Gale et al., 2013). This qualitative method allowed us to generate themes, based on our interviews, that were drawn by “making comparisons within and between cases” (Gale et al., 2013). In addition to this, the framework method made it suitable for an interdisciplinary collaboration and involvement in the study, bringing in the perspectives of a public health researcher, a policy analyst, and management professional, who were involved in the data analysis process (Gale et al., 2013).
We applied the framework method on an adapted version of a conceptual framework developed by WHO called Organizational Assessment for Improving and Strengthening Health Financing (OASIS) that systematically reviews health financing in a system (Mathauer & Carrin, 2011). With an objective to understand the institutional architecture of an effective purchasing process, we suitably modified the OASIS framework to determine the performance of purchasing mechanism within SIAF in MP. Using OASIS and its exhaustive set of questions, we constructed four themes—decision-making authority, purchasing structure, management of purchasing, and transparency and regulation.
We reviewed the existing literature pertaining to UHC with reference to purchasing health care and its allied aspects. In addition, we also reviewed SIAF scheme–related documents. Subsequently, we conducted a stakeholder analysis to identify key resource persons and obtained their perspectives regarding successes and challenges of health care purchasing within SIAF.
We applied purposive sampling to select individuals from state, district, and block levels and conducted 32 in-depth key informant interviews (KIIs; between December 2014 and March 2015) to elicit information on various aspects of the purchasing mechanism. The coordination of interviews was initially carried out over the phone, and interviews were conducted in their places of work for the sake of comfort. The samples were selected from different levels of administrators, decision-makers, and policy makers who were involved in the strategic purchasing process of SIAF. We obtained signed consents before proceeding with an interview, and wherever the participant agreed, we recorded the interview. We sought prior appointments with respondents and shared a participation information sheet comprising project-related information. We obtained ethical approval from the Public Health Foundation of India vide reference number TRC-IEC-233/14. Through a formal communication signed between the MP state government and the Public Health Foundation of India, we solicited state officials’ support and cooperation to conduct this study.
All feedback from KIIs was organized and cross-checked to describe emerging themes. Thematic and content analysis was conducted as part of the qualitative data management process. Cross-case thematic analysis revealed patterns of discordance and/or convergence that helped both inductive and deductive analyses before recommendations were developed.
We sampled three out of 51 districts in MP using a two-pronged approach. First, we identified those districts where all or most of the schemes (e.g., Mobile Medical Units at the district level, 108 ambulance service at the state level) including SIAF were implemented. In the second and final stage, we used a district-level composite index developed by an external agency to obtain sample districts (Ram & Shekhar, 2006). For MP, this index ranged from 0.68 to 0.26—high and low index values representing a better and poor performing district, respectively. One district each from high- (Gwalior: 0.57), medium- (Sehore: 0.47), and low-performing (Chhatarpur: 0.35) districts formed part of the sample. We restricted our sampling to three districts, primarily due to limited access to resources that were available to conduct this study.
We used discussion guides during interviews to collect demographic information, and that related to current purchasing mechanism of health care services, definition of purchasing function, management of relationship between producers and purchasers, empanelment criteria for health institutions, eligibility criteria for provider selection, and rate setting of health care services. In-person interviews of state-, district-, and block-level officials were the main source of information. We transcribed recorded interviews, manually coded them, and used a summary sheet to capture any nonverbal information that respondents provided during interviews. Apart from synthesizing information from interviews, we obtained estimates on health care expenditure from published documents.
The initial examination strategy used in the analysis of the research data involved two different tactics: a priori and grounded theory (also known as qualitative content analysis). These two methods helped analyze a priori theory, using codes identified by the principal investigator prior to reviewing the research data collected. Second, grounded theory was used to understand similar qualities. Both are based on a naturalistic inquiry, which involves identifying themes and patterns, as well as rigorous coding. In addition, voice recordings of interviews and meetings, sessions, and interviews were professionally transcribed. The transcripts were read several times by at least two investigators to ensure they are clear and reflective of the KIIs. This process helped the study team to come up with the major themes presented in the “Results” section (Table 2).
Prominent Subthemes and Codes by Four Themes Under SIAF.

Source. Authors’ compilation.
Note. SIAF = State Illness Assistance Fund.
We adopted several strategies to control for and minimize any research bias. First and foremost, the study team conducted the stakeholder interviews without any preconceived notion (Galdas, 2017) so as to avoid “own” bias (Sutton & Austin, 2015). To enhance the quality and credibility of our findings, triangulation was used to cross-check for internal consistency or reliability. Another research staff, who was not involved in the stakeholder interview and coding process, applied the “document analysis” (Mackieson et al., 2018) technique to identify themes. This approach was adopted to control for any bias in the selection of one or more themes.
Results
Decision-making authority looks at the roles and responsibilities of officials under the scheme at various levels of its functioning; purchasing structure looks at ways the products are selected and later procured; management of purchasing determines ways the rates are decided and payments made; and transparency and regulation looks at ways the services are monitored, grievances redressed, and quality maintained among various aspects of the scheme. Table 2 illustrates prominent subthemes and codes by major themes that were studied under SIAF.
Decision-Making Authority
SIAF’s stewardship roles are at state and district levels, with the majority of the decision-making occurring at state level. Key decision-makers at state level include the Minister of Public Health & Family Welfare (PH&FW), Principal Secretary Health (PSH), and Director of Public Health (DPH). A deputy director who acts as a liaison between government, empanelled hospitals, stakeholders, and beneficiaries, along with consultants, provides support to PSH. The Chief Medical & Health Officer (CM&HO) with help from supporting staff leads and manages all activities at the district level, including monitoring and grievance redressal. In addition, two high-powered supervisory committees at state and district levels exist to ensure smooth functioning. The state-level committee in consultation with specialists/experts, including those from the private sector, determines disease types and benefit packages for each disease. Empanelment decisions are made by state-level officials, whereas district-level officials could only recommend for de-empanelment. In addition, involvement of several stakeholders in SIAF’s oversight and execution leads to multilevel clearances, and any absence of officials significantly delays fund release. As per scheme guidelines, grant money should be released to a health institution typically within 10 days from application: Unless the signature is made by tehsildar, magistrate, civil surgeon, or the collector, the cheque is not released. If collector is not present, then it gets delayed. Normally it takes 15 or more days to get signed by everyone. (Official in-charge)
Purchasing Structure
The state-level committee considered three factors to finalize benefit package rates for 20 listed disease types. Using the standard rates of central government as reference point, it analyzed prevailing market rates, as well as consulted with specialists from the Department of Medical Education (DME) and private practitioners before determining package rates. Cancer and cardiac surgery with 47 and 26 packages, respectively, comprised the most number; remaining categories comprised single package each. The benefit package rates were last revised in 2012 and include rates for both government and private hospitals. Secondary data on empanelment reveal a high concentration of empanelled health institutions located in two major cities in MP—Indore and Bhopal. From a beneficiary perspective, this poses a serious concern in terms of coverage and accessibility.
Management of Purchasing
Under this scheme, an empanelled hospital first provides an approximate estimate of medical procedure to the patient in advance, per a prefixed maximum limit. The patient then provides the estimate to district authority, who after due verification of patient’s domicile and BPL status and the hospital estimate directly releases the grant to the hospital: Payment is already made in advance; else the hospital will not start the treatment. They will initiate treatment after receiving cheque. (Chief Medical and Health Officer)
Under this scheme, a patient (a) could only avail a general ward facility, (b) would not receive any assistance fund prior to grant approval, and (c) should not pay any additional money to the hospital for the procedure. Hospitals are required to submit a discharge ticket to district authority within 15 days of treatment completion along with a utilization certificate (UC). However, officials from two districts (Chhatarpur and Gwalior) mentioned that only 35% to 40% of UCs are received on time; the remaining come much after completion of financial year.
Transparency and Regulation
State government–released documents indicated provisions of random check with patients to verify whether their medical procedure was conducted according to approved grant. Upon establishment of any wrongdoing, deviant hospitals were blacklisted for 3 years based on the complaint received. Furthermore, a staff member handling the scheme in a study district opined that “we only threaten the hospitals who err in furnishing the utilization certificate. District has no authority in terminating the contract of the erring hospital. These powers rest with the State Head Quarter.”
Based on scrutiny of documents and consultations with concerned officials, we found that any form of random checks was inadequate. Moreover, regulatory mechanisms are poor and nonexistent for private-sector empanelled hospitals, and there is no system to conduct medical audits.
A senior official from the Directorate of Health Services (DHS) highlighted that several CM&HOs had no enthusiasm for monitoring the scheme and were involved in indiscriminate sanctions. As many as 12 districts in the last 2 to 3 years were identified regarding irregularities in fund sanctions. Information from interviews also indicated the presence of vested interests, leading to referral of patients to specific private hospitals in far-off places, even though the equivalent or sometimes better services and providers are available nearby. Another respondent mentioned of cases where private hospitals charged extra money from patients. However, in the absence of any written complaints, there were officially no registered cases of corruption in SIAF: Though there are no cases of corruption noticed in this scheme but there are cases in which hospitals charged extra money from the patient. But we don’t have any written complaint, so we are unable to take action against them. (Senior official)
SIAF does not have a specific grievance redressal mechanism. However, complainants could use Jan Sunwai, a public hearing forum headed by a district minister in-charge or the district collector, as a mode of grievance redressal. In terms of quality management, there is virtually no information, even though the scheme mandates for the same.
Discussion
The four themes, the prominent subthemes under them, and codes presented in the “Results” section, and particularly in Table 2, resonate with findings from other studies conducted in less developed countries such as Cambodia (Annear et al., 2013) and Lao People’s Democratic Republic (Ahmed et al., 2013), confirming additional validity to our findings. Applying strategic purchasing would ensure efficient use of resources that are necessary for a resource-constrained health system in MP, as is opined by Tien et al. (2011) in the context of Vietnam.
Financial constraints are one of the major barriers of access to health care for marginalized sections of the society (Garg & Karan, 2009). A new report released by WHO and The World Bank estimated that at least 400 million people currently lack access to essential health services and that 6% of the populations from low- and middle-income countries (LMICs) are pushed into—or further into—poverty due to health care expenditure (WHO, 2016c). Recent empirical evidence indicated that annually around 8% of Indians fell into poverty due to out-of-pocket (OOP) expenditure on health care, resulting in higher impoverishment (Kumar et al., 2015).
Governments typically strive to provide affordable health care to all. They also face a daunting challenge of generating, apportioning, and efficiently and effectively managing resources required to purchase health care services. To address these challenges, the Indian government too has adopted strategic purchasing mechanism that brings together a range of separate functions with a potential to improve efficiency, effectiveness, and responsiveness. Such purchasing mechanism can also make significant contribution toward achieving major public health goals and wider social objectives of equity within the health care system (Figueras et al., 2005).
Using governance as a tool, we looked at the strategic purchasing mechanism of SIAF. Such schemes that provide full subsidization of premium exist in many LMICs with varying degree of success (Bauhoff et al., 2011; Hidayat et al., 2004). Recent estimates from MP indicate that although there has been an improvement in per capita expenditure on health care (INR 238 in 2006–2007 vs. INR 312 in 2009–2010; Choudhury & Amar Nath, 2015), there has also been an increase in OOP expenditure on health care as the percentage of household consumption expenditure between two National Sample Survey (NSS) rounds (50th—1993–1994 and 61st—2004–2005), as has the percentage of people impoverished due to OOP health expenditure (Ghosh, 2011) (see Figure 1).
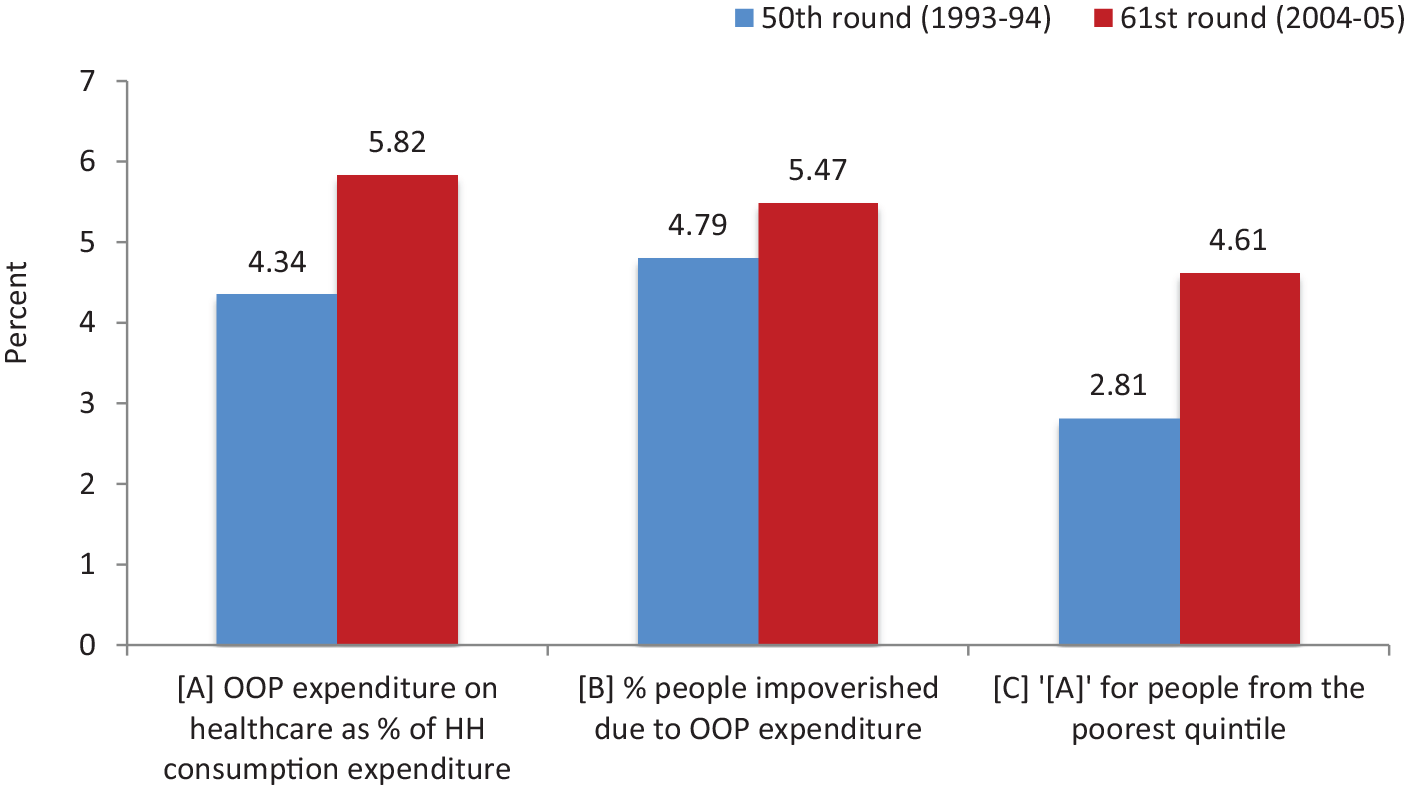
OOP expenditure on health care in Madhya Pradesh by NSS rounds.
High OOP expenditure on health care and inadequate access to health care services under SIAF have only benefited a small proportion of BPL families. This is despite indications of formidable burden of disease in the state due to any chronic illness (Figure 2; ORGI, 2014). Around 5,400 people per 100,000 population in MP suffered from any form of chronic illness. Upon extrapolation, this disease burden is estimated to be around 4 million, of which about 1.5 million live BPL. Clearly, this gap between chronic burden of disease and SIAF beneficiaries indicates a high proportion of BPL population not receiving any form of required health care. This reflects poorly on ways health care services are purchased, highlighting an urgent need for restructuring the health financing mechanism.

Persons diagnosed with any form of chronic illness in Madhya Pradesh by gender and place of stay, 2011.
The MP government can learn from the experiences of similar schemes implemented across other states in India, notably the Comprehensive Health Insurance Scheme Plus (CHIS+) in Kerala. Although a clear stewardship role of state-level authorities is mandatory for the smooth functioning of a scheme, it is also important to delegate some form of authority to their district-level counterparts. Not doing so may likely demotivate the “actual implementers” of the scheme at ground level. For example, in MP, like in Kerala, there are district-level representatives for the functioning and implementation of the scheme. However, while Kerala has one key decision-maker each from the state and district level, in MP, the scope of decision-making is limited only to state-level representatives. Apart from this, the political spectrum should demonstrate higher willingness toward improving the functioning of the scheme: State has the final authority to take a decision on empanelment and de-empanelment of hospital under the SIAF scheme. District level committee can only send their recommendations or views to the state. (Chief District Health Official)
Timely access to health care services is an important determinant of health outcomes. SIAF implementers, by introducing a one-window approval system, can do away with long waiting time to release grant to hospitals. This will help beneficiaries to avail timely services, thereby improving their quality of life, which can have a positive ripple effect on family, community, society, and the nation (Rice & Fineman, 2004). One-window systems at districts should be computerized and linked to a central server at state level, which can be used to store beneficiary- and provider-level information. This will allow for stock-taking of various aspects of the scheme, leading to increased efficiency. Contractual arrangements are a part of systematic process that will ensure that services are delivered based on price and quality criterion. This should be backed up by transparent and appropriate data-reporting standards. It is important that these standards are uniform across public and private sectors and are reviewed from time to time while considering for empanelment. This will ensure a level playing field for health system providers and health care institutions, leading to promoting optimal performance.
Transparency, regulation, and grievance redressal mechanisms are other important components of governance that can be used to gauge the status of a program and the quality of service provided. Lack of adequate accountability at all levels prevails in the Indian health care system. Public and private health care institutions and providers are subject to certain standards of reporting. However, such reporting is mostly limited to basic accounting with minimal monitoring of quality, outputs, or outcomes. Lack of basic and essential digitized data, due to underdeveloped IT systems, has been a key hurdle for improvements in quality. Although SIAF mandates conducting random medical audits and contacting beneficiaries to verify approved service provision, not much exists on the ground. Such audits and checks can lead to reducing medical waste.
The line-item budgeting in the public health system has provided limited or no incentives for flexibility, innovation, and high-quality service levels. Until the recent formation of the National Health Authority (NHA), there were no governance mechanisms, structure, and standards. Such a lack of standard measures does not allow for transparency and protection of the members of the risk pools and insurers: First they did what they liked. Now, they are so much afraid that they don’t want to do it (after series of audit objects emerged). (Senior official)
Apart from collecting information from a beneficiary regarding the quality and correctness of services, they should also be allowed to voice their concerns at a central forum. Patients should be empowered to become better purchasers of health insurance. This will allow for addressing several bottlenecks in the scheme. The state should also take measures that allow for empanelment of more health institutions. Bringing tertiary-level health care services closer to where a beneficiary resides would reduce their burden on ancillary costs (e.g., transportation cost) associated with receiving health care services.
The state government may also focus on strengthening primary care base and promoting use of both primary and secondary care services prior to approaching providers at tertiary-care level. Similar recommendations have been made to the state government earlier (Rao et al., 2011). Furthermore, given that most of the 20 listed diseases covered under SIAF are NCDs, the benefits of early screening activities are well known (The CDC Diabetes Cost-Effectiveness Study Group, 1998; Goldie et al., 2001). The state government should improve awareness regarding various preventive measures. They may do so under the aegis of National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) by covering more districts; currently, early diagnosis and management of common NCDs are conducted in five high-focus districts in MP (Ministry of Health and Family Welfare, 2016).
Conclusion
This study reiterates the importance of governance as a tool to take stock of a health system that operates under limited resources. Using governance in purchasing mechanism within SIAF, we presented a case of how effective and efficient purchasing mechanism can lead to equitable distribution of resources. By introducing the recommendations and learning from the experiences of other countries, we believe there is a tremendous scope for improvement within SIAF that the state government can initiate to increase efficiency in service delivery.
We propose four program-oriented recommendations, which we believe is imperative to improving health outcomes in geographies that typically have a resource-starved health system. First, we propose establishing a state-level social security cell that will play the role of a steward in designing/redesigning, operating, and evaluating the functioning of the scheme, as well as constitute audit teams. Second, SIAF should establish a one-window approval system that will allow beneficiaries to quickly avail critical health services. Third, SIAF should establish a grievance redressal committee solely for the scheme, which is separate from the current Jan Sunwai mechanism, at both district and state levels, which will ensure timely accomplishment of beneficiaries’ concerns. Finally, there is a need to relax and well regulate the current empanelment criteria under the scheme, allowing for adequate representation of health care providers across MP and its neighboring states.
This study has few limitations. First, the results from this study cannot be generalized across the nation as the scheme is implemented only in one state in India. However, lessons learned from this experience can be used for similar tertiary care packages formulated with public-sector funds in India. Future studies adopting a mixed methodology, specifically focusing on governance issues in health care, may be used to address some of the issues relating to generalizability. In this study, we did not engage with beneficiaries of the scheme, not allowing to discuss what users think of this scheme, in terms of quality, its reach, and/or any other components. Further research studies may address these gaps to improve the overall understanding of how governance in strategic purchasing affects the status of similar public-funded health schemes.
Footnotes
Acknowledgements
We thank the Department of Public Health & Family Welfare of Madhya Pradesh and all respondents who willingly accepted to participate in the key informant interviews (KIIs) and allowed us access to records. We also thank two anonymous referees whose comments have helped improve this manuscript.
Authors’ Note
All authors were earlier with the Public Health Foundation of India, Gurgaon, Haryana, India.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Ethics Committee of the Public Health Foundation of India (PHFI) approved the protocol for research project vide number TRC-IEC-233/14 dated October 8, 2014.