
Abstract
This study examined inequalities in the utilization of maternal reproductive health care services in urban Bangladesh. Data of 6,617 urban women were extracted from most recent two rounds of Bangladesh Demographic and Health Survey, conducted in the years 2011 and 2014. Inequalities in the utilization of antenatal checkup, receiving care from a skilled birth attendant, delivery in health care facilities, and postnatal care were investigated through concentration index. Contributions of selected predictors to inequalities were estimated by using the regression-based decomposition method. Noticeable inequalities were observed. Concentration index for utilization of at least one antenatal care visit was 0.09, four or more antenatal visits was 0.17, care from skilled birth attendant was 0.16, delivery care in health care facilities was 0.17, and postnatal care within 2 days of delivery was 0.19. Exposure to mass media, educational status of women and their spouses, wealth status, employment, birth order, and age of pregnancy were significant determinants of inequalities. There was a gradient in the utilization of services when examined across wealth status. Those with unfavorable social determinants of health reported low levels of utilization. Alongside providing tailored health care services to urban poor women, efforts should be made to reduce inequalities in social determinants of health.
Keywords
Introduction
There has been a considerable increase in the urban population in recent times. Currently, around 3.9 billion people (accounting 54% of the world population) are living in urban areas which were 0.75 billion (accounting 30% of the world population) in 1950 (United Nations [UN], 2014). The UN estimates 66% of the world population will live in urban areas by 2050 (Population Reference Bureau, 2017; UN, 2014). This increment is not uniform across the countries. Currently, developed countries have a higher proportion of the urban population. However, the rates of rural to urban migration are considerably higher in developing countries. It is estimated that in the next few decades around 90% of the projected growth of the world’s urban population will occur in underdeveloped countries (UN, 2014; World Health Organization [WHO], 2017). Employment is the main motivator of this migration (World Bank, 2007).
Worldwide, urban dwellers are thought to be healthier, as they enjoy benefits of improved health care services, than their rural counterparts (Matthews et al., 2010). However, this has not been found true everywhere, especially in resource-poor settings where large-scale rural to urban migration takes place, despite having a limited urban capacity to accommodate a growing population. A growing migration to urban areas in underdeveloped countries has led to the proliferation of slums and informal settlements which are often unfavorable for maternal and child health (Matthews et al., 2010; More et al., 2009; Ziraba et al., 2009). People living in such an unhealthy environment or those who are poor may not be able to afford even basic health care services (Agarwal et al., 2007; Goli et al., 2011). This growing problem is now promoting anti-urbanization policy, which is evident from a UN study of 193 member states that found most countries now have a policy to reduce rural to urban migration (UN, 2013).
Around 28% of the population in Bangladesh lived in urban areas in 2011 (Bangladesh Bureau of Statistics, 2012). This proportion was projected to increase around 50% by 2029 (Bangladesh Bureau of Statistics, 2012; Streatfield & Karar, 2008) mainly due to rural to urban migration, which increased to around 90 for every 1,000 urban persons in 2015 from 33 for every 1,000 urban persons in 1990 (Marshall & Rahman, 2015). This disproportionate increase in the urban population is a major cause of inequalities in overall health and utilization of maternal health care services. For instance, around 75% of poor women in Dhaka city (the capital of Bangladesh) reported at least one morbidity associated with pregnancy, and 36% reported delivery-related serious complications (Fronczak et al., 2005). Urban poor–rich gaps in the utilization of antenatal care and health facility–based delivery are around 48% and 58%, respectively (Kamal et al., 2016; National Institute of Population Research and Training [NIPORT] et al., 2012). Rates of under-five mortality, neonatal mortality, and nutritional disorder were also found higher among the urban poor people than their rich counterparts (NIPORT et al., 2016). Almost all of these adverse consequences are preventable by ensuring maternal health care services that the WHO (2018) recommends during pregnancy (at least four antenatal care), delivery (birth assisted by a skilled health care personnel, also known as skilled birth attendants), and following pregnancy (postnatal care visit within 2 days of delivery).
Bangladesh has achieved notable success in maternal health care service utilization during and following the implementation of the Millennium Development Goals between 2000 and 2015. Currently, around 64% of the total women receive at least one antenatal care consultation during pregnancy, of which 32% visit antenatal care services four or more times (Islam & Masud, 2018; NIPORT et al., 2012; Pulok et al., 2016). More than one third (37%) of women received health care services by the skilled health personnel during delivery and received postnatal care services within 2 days of delivery (NIPORT et al., 2016). This success is attributable mainly to the public facilities offering services free of cost, and some contributions of the nongovernment and charity organizations, as well as the broad media coverage regarding the importance of these services (NIPORT et al., 2016). However, utilization of maternal reproductive health care services are still low, particularly among the rural women, women with lower education and socioeconomic status, and those who have limited autonomy to visit health care facilities (M. N. Khan & Islam, 2018; NIPORT et al., 2016; Pulok et al., 2016). Importantly, these are common among urban disadvantaged women. Moreover, government-owned health care facilities in urban areas in Bangladesh are usually overcrowded (Marshall & Rahman, 2015).
Ensuring appropriate health care services for women amid a rapidly growing urban population is challenging. Limited studied have focused on the maternal health care inequalities (Haider et al., 2017; Mahabub-Ul-Anwar et al., 2006), particularly for urban women (Ahmed et al., 2005; M. M. H. Khan et al., 2011; Pulok et al., 2016). Moreover, most of the existing studies examining the inequalities adopted conventional regressions, which are not well-suited for estimating inequalities. Using the decomposition method, we examined the degree of inequalities in utilization of a set of maternal reproductive health care services in urban Bangladesh and estimated the relative contribution of some important selected socioeconomic factors to that inequalities.
Method
This study used pooled data of 6,617 urban women from two waves (2011 and 2014) of Bangladesh Demographic and Health Survey (BDHS), which is a cross-sectional survey, conducted periodically. This survey interviewed a representative sample of 37,705 (17,842 from BDHS 2011 and 17,863 from BDHS 2014) ever-married women; of them, 12,363 were from urban areas. Among these urban women, a subset of data of 6,167 women (3,342 from BDHS 2011 and 3,275 from BDHS 2014) was analyzed in this study (NIPORT et al., 2013, 2016). The criteria of inclusion were (a) had given at least one live-birth within 3 years preceding the date of survey and (b) responded to the questions of reproductive health care service use. With financial support from the United States Agency for International Development, the NIPORT conducted these surveys in collaboration with ORC Macro (NIPORT et al., 2016). A detailed description of this survey including the questionnaire and data collection procedure is available on the Demographic Health Survey website (https://www.dhsprogram.com) and in NIPORT et al. (2016). Briefly, this survey collected nationally representative data by using a two-stage cluster sampling method. In the first stage of sampling, 600 enumeration areas (primary sampling unit) were selected through the probability proportional to size from National Population and Housing Census conducted in 2011. From each enumeration area, 30 households were selected in the second stage through the systematic random sampling technique. Data were collected from all ever-married women aged 15 to 49 years in the selected households through a face-to-face interview using a predesigned questionnaire. The response rates in both waves were more than 90%. Informed verbal consent was taken from all participants prior to the interview. This consent procedure was approved by the Ethics Committee. The survey was approved by the National Research and Ethics Committee in Bangladesh.
Outcome Variables
Utilization of antenatal care, institutional delivery care, and postnatal care within 2 days of delivery are the primary outcome variables. The WHO recommends these services for every woman to assess during pregnancy, delivery, and the postpartum period to reduce pregnancy-related complications and to ensure a healthy mother and newborn(s) (WHO, 2018). Qualified doctor, nurse, midwife, paramedic, family welfare visitor, community skilled birth attendant, trained traditional birth attendant, medical assistant, and subassistant community medical officer were considered the professional personnel (also termed as skilled birth attendants) for providing antenatal checkup, institutional birth delivery, and postnatal care services (NIPORT et al., 2016). Utilization of antenatal care was categorized into two groups: (a) women received at least one antenatal care and (b) women received four or more antenatal care—following the WHO guidelines of receiving antenatal care (WHO, 2015). Professional delivery care was categorized as (a) delivery by skilled birth attendants and (b) delivery in formal health care facilities.
Exposure Variables
Household’s wealth index was considered the key variable for estimating the effect of economic inequalities in reproductive health care service utilization. The BDHS developed wealth quintiles (poorest, poorer, middle, richer, and richest) based on the information of selected household assets by using the principal component analysis (NIPORT et al., 2016). Sociodemographic factors that are known to contribute to reproductive health care service utilization (Ahmed et al., 2005; Collin et al., 2007; Pulok et al., 2016) were included in the analysis. These factors are, namely, adolescent pregnancy (pregnancy occurs at or before 19 years of age), women’s educational and employment status, spouse’s occupation type, birth order, and mass media exposure. Women were classified as exposed to mass media if they read newspapers or magazines, listened to the radio, or watched television at least once a week.
Statistical Analysis
Descriptive statistics were used to describe the selected socioeconomic factors of the respondents by their wealth quintiles. The gaps of maternal reproductive health care service utilization between the richest and the poorest were presented in percentages. Concentration index was calculated to identify socioeconomic inequalities in reproductive health care service utilization. Household wealth quintile was used as a proxy of household income and its cumulative percentage was plotted against the cumulative percentage of reproductive health care service utilization to generate the concentration curve. The curve value was then compared with the line of perfect equality to get the concentration index value (O’Donnell et al., 2008). Briefly, the concentration index presents the degree of inequality by measuring the area between the concentration curve and the line of perfect equality (O’Donnell et al., 2008). In a more detailed term, the concentration index is defined as twice the weighted covariance between the outcome and fractional rank in the wealth distribution divided by the variable mean (O’Donnell et al., 2008). The formula used for calculation is
Regression model–based decomposition method was then used to decompose the concentration index to estimate the contribution of a set of eight socioeconomic factors to the inequalities in reproductive health care service utilization. A detailed description of the concentration index and regression-based decomposition method could be found elsewhere (O’Donnell et al., 2008). Briefly, an advantage of the regression-based decomposition method is its ability to both identify and quantify the determinants of inequality. In this method, the number of determinants can be arbitrary, and their proxies can be used. For each of the decomposition models, we dichotomized the selected socioeconomic factors into an advantaged and a disadvantaged group (e.g., received vs. did not receive formal education; poor [consists of poorest and poorer subgroups] vs. nonpoor [middle, richer, and richest]; exposed vs. not exposed to mass media, etc.). Key socioeconomic predictor variables were selected by reviewing the previously published in public health literature (Collin et al., 2007; M. N. Khan et al., 2017; Pulok et al., 2016). These factor variables were used across the models irrespective of their individual level of significance. The analyses were adjusted for the complex sampling design of BDHS by using Stata svy command. All analyses were carried out by Stata Version 15.1 (Stata Crop LP, College Station, Texas).
Results
A total of 6,617 urban women were included in this study. In the combined data set, the contribution of two waves was 50.5% (2011) and 49.5% (2014), respectively. Around 20% of women from low economic status (consists of poorest and poorer subgroups) and 66% women from richer socioeconomic status (richer and richest subgroups) were working in the formal sectors (Table 1). Mass media exposure among the poorest and the poorer was low—around 8%, compared with 80% among the richer and the richest subgroups.
Background Characteristics of the Respondents (N = 6,617).
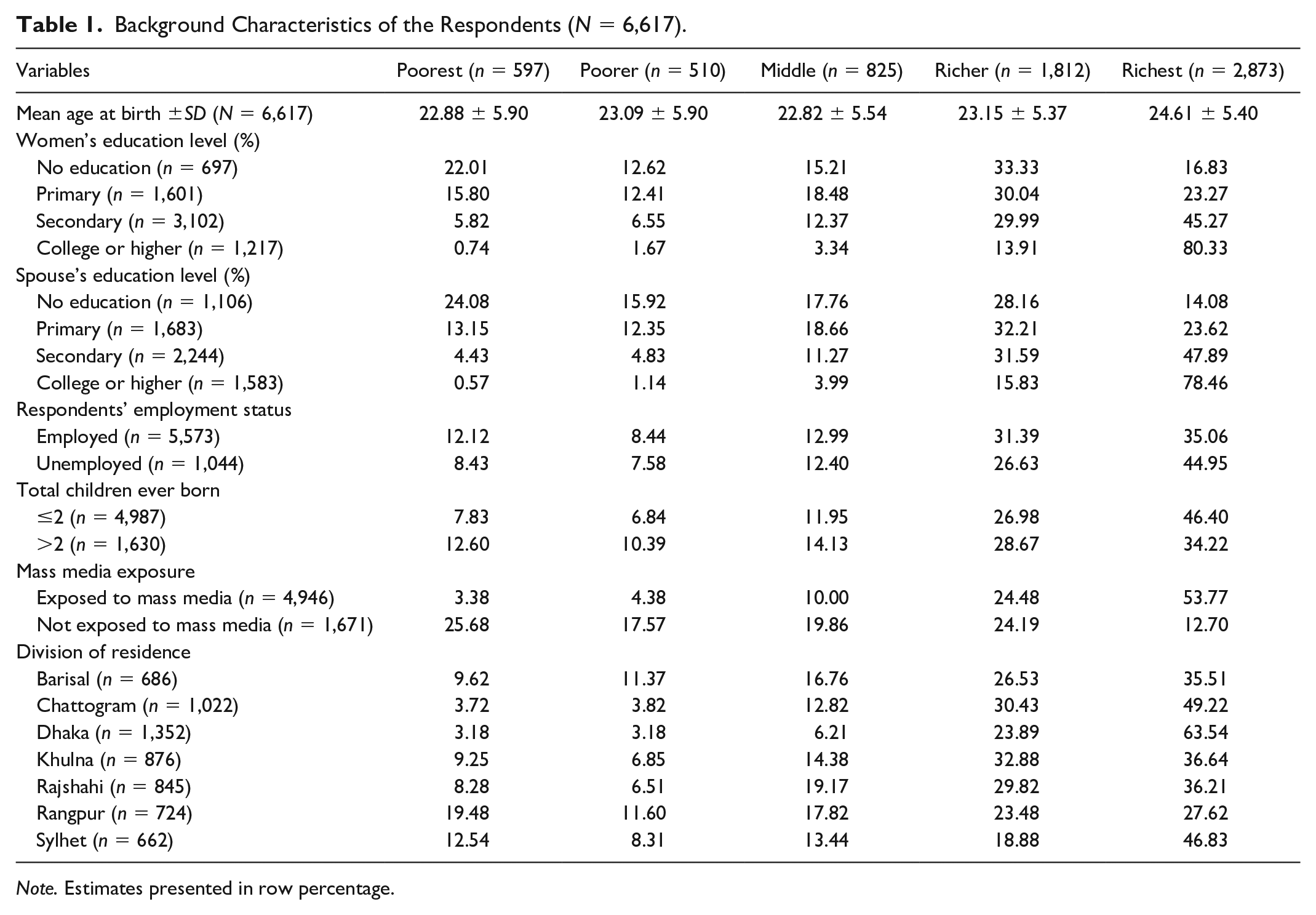
Note. Estimates presented in row percentage.
There was a clear gradient for all five health care items included in this study; utilization gradually increased from the poorest to the richest group (Table 2). Around 46% of the poorest women received at least one antenatal care compared with 89% of the richest women, showing a 43% gap between the richest and the poorest. The inequality widened further (49.55%) for “postnatal care within 2 days of delivery.”
Inequalities in the Utilization of Maternal Reproductive Health Care Services by Wealth Quintile in Urban Bangladesh.

Overall for the entire country (both urban and rural).
A comparison of the utilization of the five maternal health care services between 2011 and 2014 shows the richest to the poorest equalities decreased for antenatal visits and increased for delivery by skilled birth attendants, delivery in health care facilities, and postnatal care within 2 days of delivery (Figure 1). This gap is smaller for intra-urban women than for the overall women of the country (Table 2). In the combined data set, the inequalities between the richest and the poorest subgroups of urban women in terms of utilization of the five maternal health care services were in the range of 35% and 55% (Table 2).
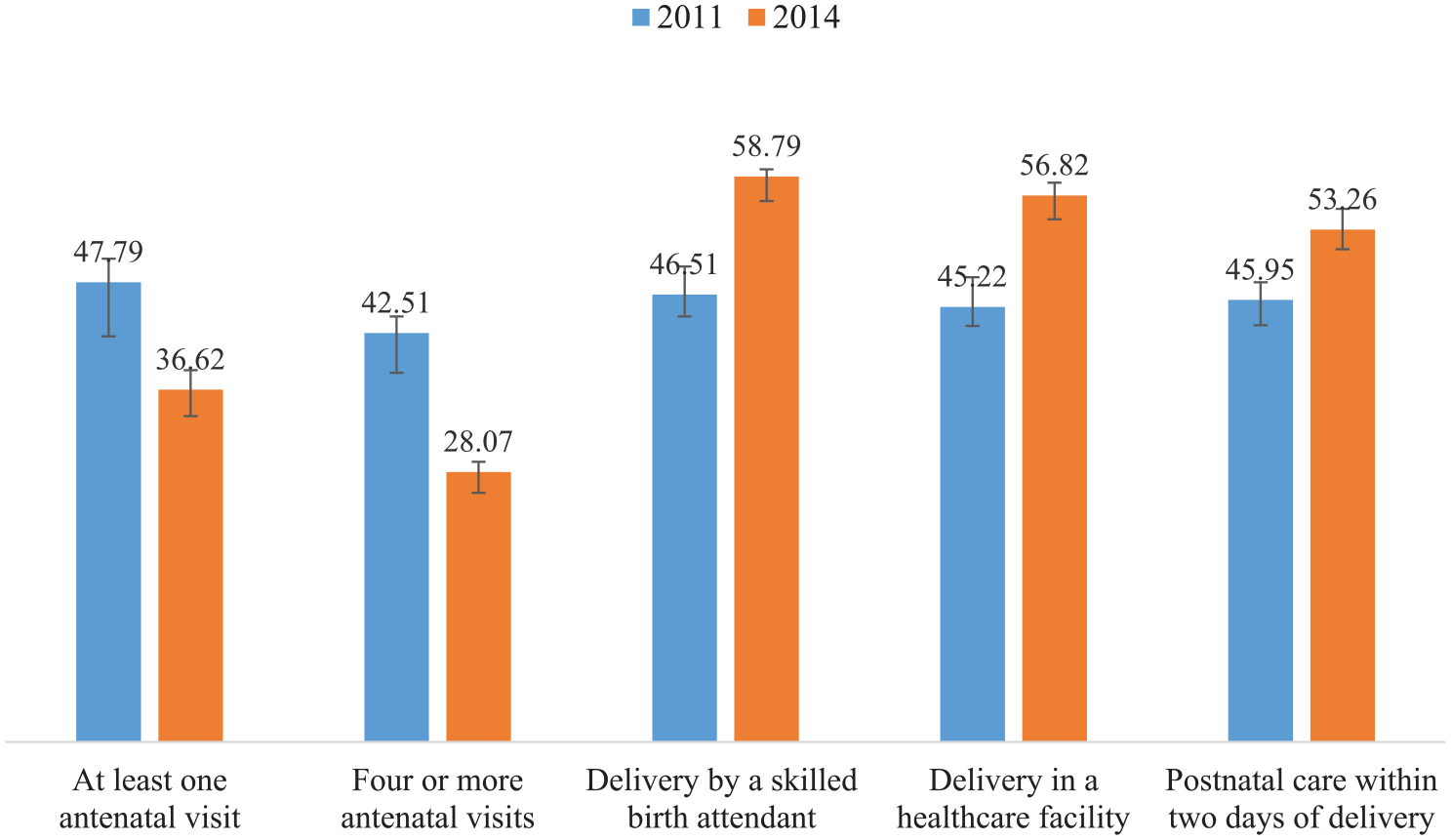
Poorest to richest gap in the utilization of maternal reproductive health care services in urban Bangladesh, 2011 and 2014.
Multivariable regression-based decomposition analysis shows the values of concentration index for each of the health care items, and the proportion of those values that were explained by the factors, namely, adolescent pregnancy, women’s educational and employment status, spouse’s occupation type, birth order, and mass media exposure (Figure 2). The positive values indicate a higher level of utilization by women of relatively higher wealth quintiles. Inequalities were highest for receiving postnatal care within 2 days of delivery (0.19; 95% confidence interval [CI] = 0.14, 0.25) followed by delivery in health care facilities (0.17; 95% CI = 0.11, 0.20), four and more antenatal visits (0.17; 95% CI = 0.13, 0.22), and delivery care by skilled birth attendants (0.16; 95% CI = 0.11, 0.21). Inequality in receiving at least one antenatal visit was the lowest (0.09; 95% CI = 0.05, 0.13).
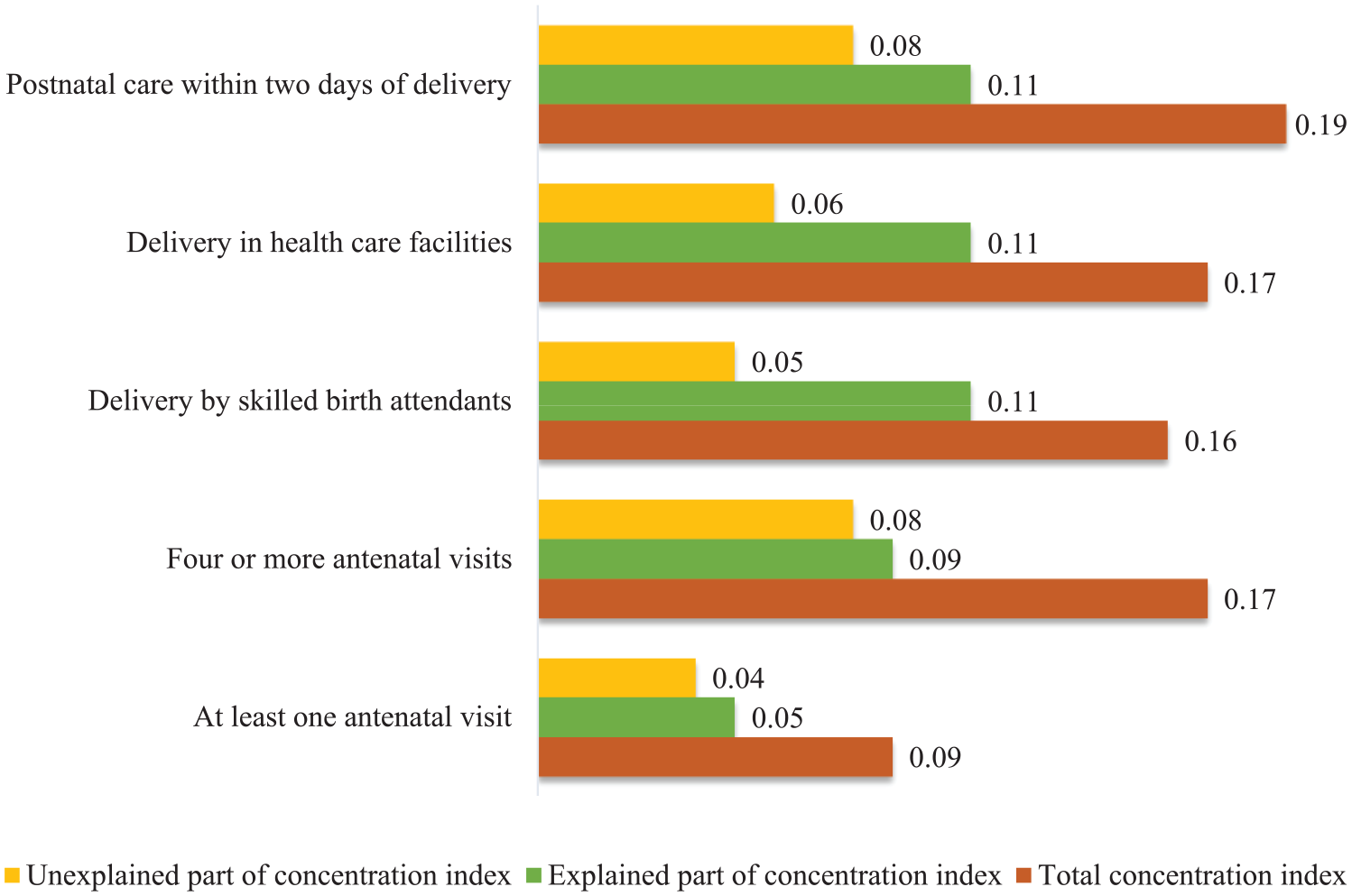
Concentration index showing inequalities in the utilization of maternal reproductive health care services in urban Bangladesh.
Around 55% (0.05 out of 0.09) of inequalities in utilization of at least one antenatal visit, 53% (0.09 out of 0.17) of inequalities in utilization of four more antenatal visits, 69% (0.11 out of 0.17) of inequalities in delivery care from skilled birth attendants, 63% (0.11 out of 0.17) of inequalities in birth delivery in a health care facility, and 58% (0.11 out of 0.19) of inequalities in utilization of postnatal care within 2 days of delivery were explained by a set of eight socioeconomic factors included in this study. The remaining percentages of inequalities could not be explained by the included socioeconomic factors. The results of decomposition analysis are presented in Table 3 and Supplemental Tables S1 to S5. Among these eight factors, no exposure to mass media (35.19%) and spouse’s educational status (18.45%), women’s educational status (14.11%), and household’s wealth status (12.73%) were identified as the major contributor to the inequalities in at least one antenatal visit. All eight factors except “women’s employment status” remained significant for inequalities in receiving four or more antenatal visits, delivery care from skilled birth attendants, delivery in health care facilities, and postnatal care within 2 days of delivery.
Contribution of Some Social Determinants of Health on Inequalities in the Utilization of Maternal Reproductive Health Care Services in Urban Bangladesh (N = 6,617).

Note. % contributions in bold indicate significant contributors at p < .05 in bootstrap analysis; N = total urban women included in the study; n = number of women included in this model.
Discussion
Rising population growth in urban Bangladesh has created a wide range of socioeconomic profiles. However, such diversity was rarely considered in the available health literature, rather data were often presented in aggregate form for all urban residents. We examined the degree of inequalities and socioeconomic factors affecting the utilization of maternal reproductive health care services in urban Bangladesh. Findings from this study suggest significant inequalities exist in the utilization of reproductive health care services. Women from relatively low socioeconomic status use basic services of reproductive health care less than those of high socioeconomic status. Exposure to mass media, educational status of women and their spouses, wealth quintiles of the household, employment and its type, birth order, and age of pregnancy were significant contributors to the inequalities. We noticed a gradient in the utilization of these services when examined across wealth quintiles.
Poverty in developing countries such as Bangladesh has long been associated with the rural areas that are often known to have a higher agricultural dependency, irregularity of work, and inequitable distribution of agricultural land (Bangladesh Bureau of Statistics, 2010; Bhatta, 2010). But rapid urbanization in recent decades due to factors such as inadequate opportunities of education, employment and health care in rural areas, and disruptions of rural livelihoods by natural disasters (Marshall & Rahman, 2015; Uddin & Firoj, 2013) shifted the poverty to urban areas (UNICEF, 2010). Their expectation of having a higher income and an improved living standard in urban areas are the main motivators to migration, although rarely that expectation comes true. A recent survey on household income and expenditure in Bangladesh found that around 21% of the urban population were living below the poverty line and the majority of them were migrated from rural areas (Bangladesh Bureau of Statistics, 2010). Most importantly, the majority of these urban poor people live in slums and squatter settlements, footpaths, train stations, and other scattered places that offer substandard living conditions and often worse than their rural living (Bangladesh Bureau of Statistics, 2010).
We found a considerably lower utilization of reproductive health care services by urban poor women than their rich counterparts. As Bangladesh is increasingly being urbanized, such findings have substantial policy implications. There could be many factors that explain such inequalities. First, there is a common belief that urban areas have the necessary health care infrastructure and therefore urban people enjoy better health care services (Ompad et al., 2007; UNICEF, 2010; WHO, 2015). This perception may lead to inadequate attention to the inequalities in urban areas and motivate policy makers to focus on rural-based health care policies. In addition, addressing intra-urban health inequalities and thereafter taking appropriate policies are challenging, particularly in a resource-poor setting such as Bangladesh. Also, there is a scarcity of health data to inform the extent and pattern of urban health inequalities (Ompad et al., 2007). Moreover, existing high population density and multiple risk factors that affect health and well-being are very complex to address (UN, 2014; Vlahov et al., 2007; WHO, 2016).
Mass media exposure was found to be a key predictor for the utilization of reproductive health care services. Mass media is a popular and cost-effective public health promotional tool that influences women’s health care-seeking behavior by increasing health knowledge and attitudes toward healthy living (Rahman et al., 2017; Robinson et al., 2014). Dugassa’s (2016) research demonstrates the pathways and the extant that media can affect health and well-being in a developing country context. Inequalities in the distribution of access to information and knowledge are directly related to inequalities in health matters. Not having exposure to mass media, therefore, adversely affects health care utilization. This observation is supported by a previous study conducted in Bangladesh (Rahman et al., 2017). However, improving the health knowledge by using mass media among the urban poor is challenging for either the situational difficulties or its one-way flow of information (Naugle & Hornik, 2014). Usually, urban poor people living in slums and squatter settlements rarely can afford mass media accessories such as television and newspaper (Kamal et al., 2016). Even if they can afford such accessories, having enough time to properly use them may not be possible due to other pressing needs and priorities.
The education status of women and their husbands were the second and third major contributors to urban inequalities in the utilization of reproductive health care services. This finding is consistent with the findings of a study by Goli et al. (2013) from the National Family Health Survey in India. However, education does not act on health in isolation rather intertwined with many other social determinants of health. Socioeconomic status and employment are other important factors that interact with education in many ways. For instance, those with fewer years of schooling are often less socioeconomically empowered and engaged mainly in the informal job sector (physical worker, labor, etc.) that create an economic barrier to access health care services (Hajizadeh et al., 2014; NIPORT et al., 2016). Also, women with little or no formal education may not have enough knowledge to realize the benefit of health care services and may not prioritize accessing them (Ononokpono et al., 2014). In some cases, they prefer to receive services from nonmedical professionals.
Reducing inequalities and therefore achieving equity in health is one of the core agenda in the newly adopted Sustainable Development Goals (UN, 2016). However, assessing inequalities and taking appropriate policies to reduce them are always challenging (UN, 2016; Victora et al., 2010; WHO, 2015). Even the developed countries struggle to reduce inequalities (Agency for Healthcare Research and Quality, 2009; Bleich et al., 2012). In developing countries, things become further challenging as there are substantial inequalities in social determinants of health which are a significant contributor to health inequalities (Collin et al., 2007; Say & Raine, 2007). While the targeted services for the urban poor is a quick option for reducing inequalities, improving social determinants of health is required for bringing a sustainable solution.
This study has several strengths. The greatest strength is two waves of nationally representative survey data. Large sample size and an appropriate method are some other strengths. This study also has some limitations. First, the classification of wealth index based on participants’ current assets was sometimes misleading, as the BDHS did not include information on their assets they may have in the villages they came from. This is a cross-sectional data set which does not permit assessment of the temporal and thus potentially causal relation of variables. In addition, there may have some recall and social acceptability biases in data regarding health care service utilization during the last pregnancy occurring within 3 years preceding the survey. However, despite these limitations, this is the first study that addressed the socioeconomic inequalities in the utilization of reproductive health care services in urban Bangladesh.
In conclusion, there were substantial inequalities in utilization of reproductive health care services by women of different socioeconomic status in urban Bangladesh. Exposure to the mass media, level of education of women and their husbands, wealth quintiles, occupation of the spouse, birth order, and adolescent pregnancy are the major contributors to urban inequalities in the utilization of reproductive health care services. In addition to offering targeted health care services to the poor section of the community, efforts should be made to reduce inequalities in social determinants of health.
Supplemental Material
Supplimentary_Tables – Supplemental material for Inequalities in Utilization of Maternal Reproductive Health Care Services in Urban Bangladesh: A Population-Based Study
Supplemental material, Supplimentary_Tables for Inequalities in Utilization of Maternal Reproductive Health Care Services in Urban Bangladesh: A Population-Based Study by Md. Nuruzzaman Khan, Pushpendra Kumar, Md. Mijanur Rahman, Md. Nazrul Islam Mondal and M. Mofizul Islam in SAGE Open
Footnotes
Acknowledgements
We would like to thank MEASURE DHS for granting permission to use the data set.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The data of this study could be collected from the DHS Program.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.