
Abstract
The student Burnout Syndrome is a response to chronic and severe stress linked to the role of the students and their academic context. This study aims at determining the prevalence and severity of the student Burnout Syndrome on a sample of midwifery students and its associated factors. The study is observational, cross-sectional, and analytical, with a sample of 140 students of a Chilean university. The study variables were as follows: sociodemographic background, academic profile, student Burnout Syndrome scale, and behaviors in everyday psychosocial activities. The instrument for measuring the Burnout Syndrome was the Unidimensional Scale of Student Burnout. For the analysis, descriptive statistics were used, and the association of the independent over the dependent variables was assessed through linear regression. Of the third-year students, 77.2% had a moderate or deep burnout level, which increases to 91.8% in the fourth-year students. A significant and direct association was found between the syndrome and the career year. A significant association was also found between the Burnout Scale and the scale of psychosocial risk behavior. All the students present some degree of Burnout Syndrome, which is related to both their studies and psychosocial risks.
Introduction
In most universities, students taking health care career have an 8-hr academic day, equivalent to full-time (Asencio-López et al., 2016; Rosales, 2012; Villwock et al., 2016). This schedule is one of the undergraduate studies of midwifery, whose primary purpose is mainly to contribute to the care of the sexual and reproductive health of women in all the stages of their vital cycle. This 5-year career involves lectures, tasks performed autonomously, and clinical practice in hospitals (Universidad de Santiago de Chile [USACH], 2014). Clinical training represents a methodology important for professional training that intensifies in the third year (clinical cycle). In this clinical practice, the students must apply the theoretical knowledge acquired along with the career, and starting with it, develop abilities or skills in performing clinical procedures.
Furthermore, they must interact with patients and relatives under high levels of stress, caused by a variety of health situations involved. These clinical practices, in contrast with the practice carried out in other career, have human beings as their study units with bio-psychosocial alterations, often associated with a high emotional load in the clinical setting, which can have repercussions in the students’ psychosocial life. In addition to the above, in all these scenarios, the students are evaluated continuously (Hernández et al., 2013; Schytt & Waldenström, 2013; USACH, 2014).
The student Burnout Syndrome is defined as a response to chronic and severe stress, linked to the students’ role and to their academic context (Asencio-López et al., 2016; Caballero et al., 2010, 2015; Rosales & Rosales, 2013; Villwock et al., 2016). This syndrome has been approached by Barraza (2011), who concluded that the central content of the burnout is related to the loss of the subject’s sources of energy, which is a combination of physical, emotional, and cognitive tiredness caused by the academic demands. Barraza (2011), to measure this concept, created and validated the Unidimensional Student Burnout Scale, which consists of 15 items, and shows acceptable psychometric properties (Barraza, 2008, 2009, 2011; Barraza et al., 2012).
This study seeks to determine the frequency and identify the factors associated with the existence of student Burnout Syndrome in midwifery students. In this case, we are focusing on students of Years 3 and 4 of a Chilean university during the academic year 2017. Knowing the students’ response to all their academic activity is a crucial element for the management of their academic load, understanding of their professional identity, as well as for the design and implementation of interventions focused on reducing burnout and increasing educational retention.
Method
The study is observational, quantitative, and cross-sectional, and it had an analytical character. The study’s population corresponded to the total number of students who were taking third and fourth years of the midwifery career at a university in Santiago, Chile, registered during the year 2017, with a total of 140 students. The inclusion criterion was enrollment in third- or fourth-year courses, and the exclusion criterion was absence on the day of data collection. The studied variables were as follows: sociodemographic background, academic profile, student Burnout Syndrome, and behavior in everyday psychosocial activities. The dependent variable was the Burnout Syndrome.
The self-applied data collection instrument consists of a questionnaire whose first part corresponds to sociodemographic information, with variables such as age, gender, children, and employment activity. The second part corresponds to the student’s academic profile, which includes the year he or she is coursing, subjects passed, and full academic load (attending theoretical lectures and clinical practice jointly). The third part consists of the Unidimensional Student Burnout Scale, which measured the level of physical, emotional, and cognitive exhaustion of the students (Barraza, 2008, 2011). This scale has 15 items that are answered by means of a Likert-type scale with four value categories (1 = never, 2 = sometimes, 3 = almost always, and 4 = always), which allow identifying the frequency of the evaluated item; it also has two subdimensions that include behavioral (Items 1, 2, 3, 4, 5, 7, 9, 11, 14, and 15) and attitudinal (Items 6, 8, 10, 12, and 13) indicators. This scale was created and validated by Barraza (2009), reporting a Cronbach’s alpha reliability level of .91 and .89 in split-half reliability, according to the Spearman–Brown formula (Barraza, 2009). The addition of its items creates the Burnout Scale, so it has a variation of 15 to 60 points. It is then divided into four sections, depending on the percentage obtained, and interpreted from a four-value calculation: from 0% to 25% there is no Burnout; from 26% to 50% there is a mild level; from 51% to 75% there is a moderate level, and from 76% to 100% there is a deep burnout level. Finally, the fourth part describes the scale of behaviors of everyday psychosocial activities, the tension perceived when facing clinical practice, and the methods used to cope with the Burnout Syndrome.
The psychosocial activities behavioral scale is composed of four items (1 = never, 2 = sometimes, 3 = almost always, and 4 = always). The reliability analysis gives a Cronbach’s alpha of .71, which represents an acceptable level. In the data analysis, descriptive statistics were carried out for the dependent variable and the sociodemographic profile variables. In turn, statistically significant differences per class were calculated using the Bonferroni coefficient. For the association between categorical variables, we use the chi-square statistic. Regression is used to assess the specific effect of the sociodemographic, academic, and psychosocial everyday activity variables on the Burnout Scale, with the dependent variable “total score on the Unidimensional Student Burnout Scale.” Compound summative indices of “behavioral indicators” and “attitudinal indicators” were constructed.
For data analysis, we used SPSS Statistics 23.0. Concerning the application of the instrument, it was done in the classroom in a single instance during the academic week 14 (of a total of 17), which corresponded to a week without integral evaluations. Participation of the students was voluntary and anonymous, after giving their verbal approval and signing an informed consent form. The research project was authorized by the school authorities and was approved by the Ethics Committee. Ethical considerations followed the proposal for research in human beings by Ezekiel Emanuel and the orientations for medical research involving human subjects of the Declaration of Helsinki (Emanuel, 2003; World Medical Association, 2013).
Results
The studied population consisted of 140 students: 79 in the third year and 61 in the fourth year. Concerning the sociodemographic profile of the students, the average age of those in the third year was 22.2 (SD = 1.4) years, with a minimum of 20 years and a maximum of 27 years. In the case of those in the fourth year, the average age was 22.6 (SD = 1.5) years, with a minimum of 21 years and a maximum of 31 years. Concerning gender, in both groups, there was a predominance of women: 92.4% (73/79) in the third year and 93.4% (57/61) in the fourth year. As to employment, 31.6% (25/79) in the third year and 16.3% (10/61) in the fourth year reported that they had a paid job at the time the instrument was applied. Finally, four students in the third year and two in the fourth year reported that they had children.
Concerning the academic environment, the weekly time load of the students was 52.9 hr for both classes. For students in the third year, time allocation during the first semester translates into 19.5 hr of direct lectures, 27.6 hr of autonomous work (a learning mode in which the students are responsible for organizing their academic work), and 5.8 hr of clinical practice. In the second semester, the time load consists of 16.5 hr of direct lectures, 23.7 hr of autonomous work, and 12.7 hr of clinical practice. On the contrary, fourth-year students have 16.5 hr per week of direct lectures, increasing their clinical practice to 28.8 hr and decreasing the autonomous work to 10.6 hr during the whole year. The percentage of students who attended all these academic activities, or in other words completed the curriculum, corresponded to most of them, 96.2% (76/79) in the third year and 95.0% (58/61) in the fourth year.
Regarding academic background, 40.5% (32/79) and 24.5% (15/61) of third- and fourth-year students, respectively, had failed at least one subject during their studies. The results obtained by applying the Unidimensional Student Burnout Scale show that Item 1 “Having to attend lectures every day gets me tired,” Item 3 “During the lectures I feel sleepy,” and Item 5 “I find it increasingly harder to concentrate on the lectures” are the highest average indices (3.2) in fourth-year students, whereas for third-year students, only Item 1 had a broadest average index (2.9). All these indicators are of the behavioral type. On the contrary, the lowest average index in both classes was that of Item 13 “I do not think I will finish my studies successfully” (1.6) and (1.9), and this index is an attitudinal indicator. This last item is the only one in the Burnout Scale that has no statistical significance. In general, the average score of each indicator and each subdimension is higher in fourth-year students (Table 1).
Average and Standard Deviation of Behavioral Indicators in the Unidimensional Student Burnout Scale.

Note. Letters with different subscripts indicate statistically significant differences at p < .05.
The overall average of the Burnout Scale (which includes both subdimensions) has a significantly higher mean in fourth-year students (M = 42.3) than in third-year students (M = 35.5) (F = 26.6, Sig. = .000). So, as a result of the application of the scale, we can see in Table 2 that all the participants suffer the Burnout Syndrome to some extent (Table 2).
Prevalence of the Burnout Syndrome in Third and Fourth Years According to Degree of Seriousness.

Students also responded about risk behaviors using a psychosocial risk behavior scale. It was composed of four different behaviors, and each item scored from 1 (minimum) to 4 (maximum). The four evaluated behaviors have higher averages in the fourth-year than in the third-year students, with the one related to mood changes as the highest (3.2). All these differences are statistically significant (Table 3).
Psychosocial Risk Behavior of the Students by Class.

The association between this psychosocial risk behavior scale and the student Burnout Scale is significant and direct (r = .582, p < .001). A linear regression model using the psychosocial risk behavior scale as a dependent variable (Table 4) reports that only two variables are significant predictors: the behavioral component of the Burnout Scale (β = .358, Sig < .001) and the year of studies (β = .209, Sig < .008). This model accounts for 40% of the variance (R2 = .400, Sig < .000).
Predictors of the Psychosocial Risk Scale (n = 140).

Note. (R2 = .400; Sig. < .000).
If we relate each of these four psychosocial behaviors with the degree of seriousness of the Burnout Syndrome by class, it is found that the highest perception percentages stated as nearly always or always in these risk behaviors have in the third year a range of 25%–75% at the deep burnout, increasing to 77%–100% in the fourth year (Table 5).
Psychosocial Risk Behavior and Level of Burnout Syndrome According to the Students’ Year.2

Note. Values in the same row not sharing the same subscript are significantly different at p < .05 in the two-sided test of equality for column proportions. Cells with no subscript are not included in the test. Tests assume equal variances.
This category is not used in comparisons because its column proportion is equal to 0 or 1.
Tests are adjusted for all pairwise comparisons within a row using the Bonferroni correction.
To deal with stress, most of the students, 85.7% (120/140), undertook some coping activity, with each student carrying out an average of two activities. On the contrary, 14.2% (20/140) of the students mention that they are neither consuming nor carrying out any activities to cope with the academic Burnout Syndrome.
There are no significant differences between those who do and those who do not carry out a coping activity regarding burnout. Only those students who take medicines to treat these situations declare a higher burnout level. Now, concerning the Psychosocial Risk Scale, there are significant differences between those who take medicines (higher risk) and those who carry out recreational activities (lower risk), and also who use other coping methods (carry out another activity = higher risk) (Table 6).
Differences Between Burnout Values and Psychosocial Risk According to the Type of Coping Activity.
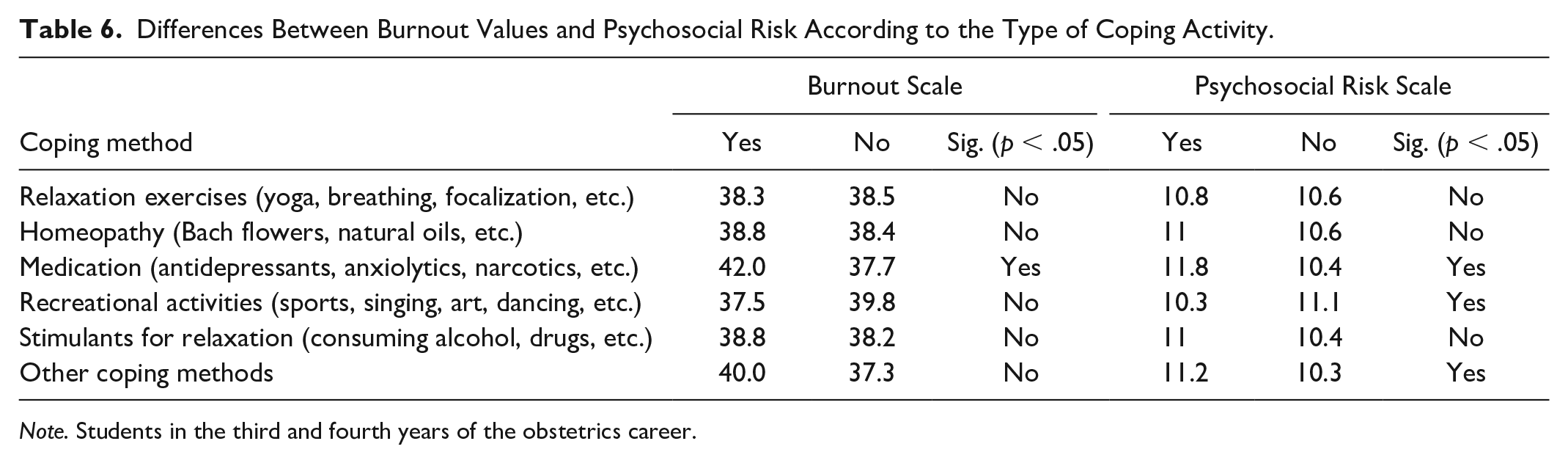
Note. Students in the third and fourth years of the obstetrics career.
Asking the students on their perception of tension when carrying out clinical practice, most of those in the third year (74.7%) and fourth year (77%) state that they are almost always or always under tension. Relating this perception with the Burnout Scale, we find that there is a percentage correspondence between the subjective rating that the students assigned to their tension and the degree of seriousness of the scale (Table 7).
Referred Tension and Burnout Syndrome Level of Students Depending on Their Year Going Through.2
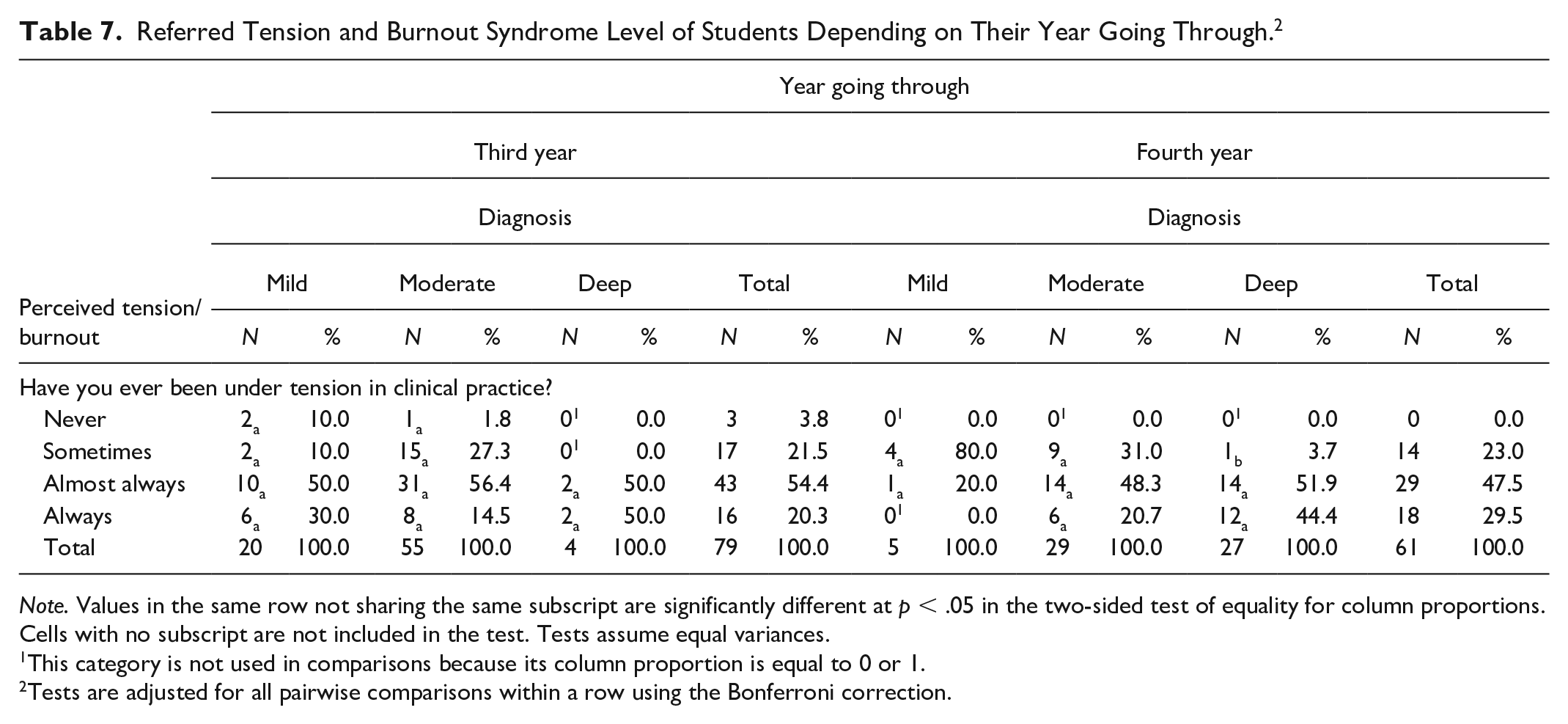
Note. Values in the same row not sharing the same subscript are significantly different at p < .05 in the two-sided test of equality for column proportions. Cells with no subscript are not included in the test. Tests assume equal variances.
This category is not used in comparisons because its column proportion is equal to 0 or 1.
Tests are adjusted for all pairwise comparisons within a row using the Bonferroni correction.
Finally, we focused on identifying the factors related to Burnout Syndrome through multiple linear regression. We tested a series of models to see which elements were able to predict burnout. The first model (Table 8) included several variables related to coping strategies as well as sociodemographic variables. The model presents a reasonable fit (R2 = .215, Sig < .003), and the results show only one significant variable: the year of studies (β = .363, Sig < .000). The second model (Table 9) added the Psychosocial Risk Scale to the previous one. The model fit increased (R2 = .392; Sig < .000), and now there are two significant predictors: year of studies and the Psychosocial Risk Scale.
Predictors of the Burnout Syndrome Scale (n = 140): Model 1: Without Psychosocial Risk.
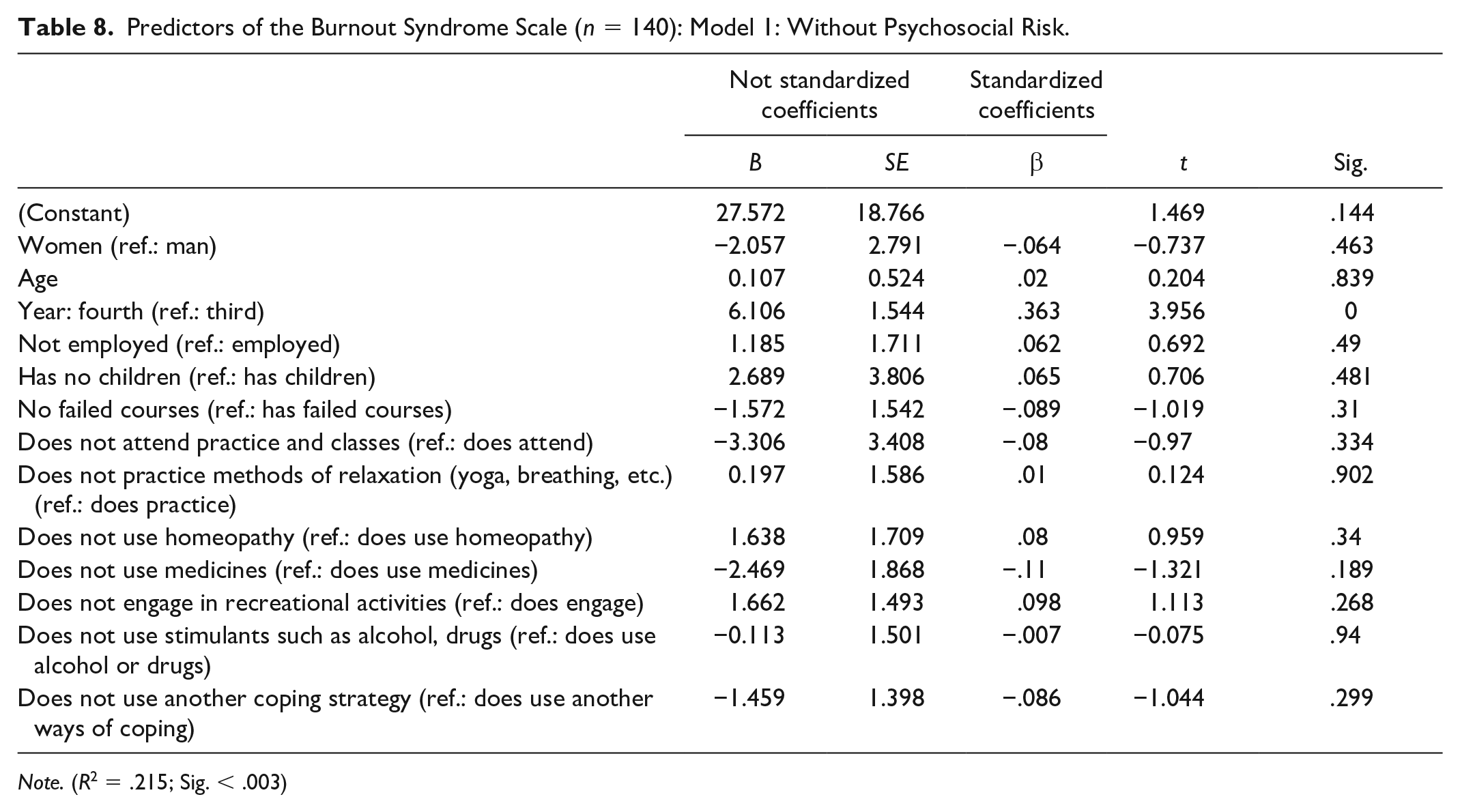
Note. (R2 = .215; Sig. < .003)
Predictors of the Burnout Syndrome Scale (n = 140): Model 2: With Psychosocial Risk.

Note. (R2 = .392; Sig < .000).
Different models were tested to predict both the attitudinal (Table 10) and the behavioral (Table 11) aspects of burnout. The model proposed explains a higher percentage of the variance of the behavioral (R2 =.375, Sig < .000) than of the attitudinal (R2 = .300, Sig < .000) component. In both cases, the explained variance is lower than the 1 accounting for the entire scale. The significant predictors in both cases are the same as the full scale: year of studies and the Psychosocial Risk Scale.
Predictors of the Burnout Syndrome Scale: Attitudinal Component (n = 140).

Note. (R2 = .300, Sig. < .000).
Predictors of the Burnout Syndrome Scale: Behavioral Component.

Note. (R2 = .375; Sig. < .000).
Discussion
Research in the area of burnout in university students defines academic burnout as the loss of the subject’s sources of energy, which is a combination of physical, emotional, and cognitive tiredness caused by the academic demands (Barraza, 2011). The analysis of our data shows that academic demands (in this case assessed by the year of study) and psychosocial risks are the main predictors of it.
In the curriculum of the School of Midwifery, the clinical cycle begins in third year, with clinical practices lasting 6 weeks each, carried out from Monday through Thursday from 08:00 to 12:30 hr, plus six semesterly theoretical subjects in the first semester and three in the second semester (USACH, 2014). In fourth year, the students take five clinical practices with the fourth shift modality, which means a shift from 8:00 to 20:00 hr the first, then a shift from 20:00 to 08:00 the second day, with the third and fourth days free, and so on, with a duration of 6 weeks each, plus four annual theoretical subjects. During these two academic years (third and fourth), the theoretical classes are parallel to the clinical practice (USACH, 2014). As we can appreciate, the increase in clinical activities during the fourth year can play a role in the increase in burnout for these students.
As already stated, the academic Burnout Syndrome is present in the whole population considered in the study, and its degree of seriousness is moderate to severe in most of the students (77.2% in the third year and 91.8% in the fourth year). These results are similar to those of the study made by the author of the Unidimensional Student Burnout Scale with 51 students in the midwifery area at the Facultad de Enfermería y Obstetricia of the Universidad Juárez of the State of Durango, Mexico, where all the students presented the syndrome, with a prevalence of the mild character (84%). However, that paper does not go deeply into the year of the students’ career (Barraza, 2008). On the contrary, Rosales (2012) applied the scale to first-year students (without specifying the career) of the Universidad de Ciencias Médicas de Holguín, Cuba, showing that the majority of the 70 students present mild Burnout Syndrome. These studies confirm that, regardless of the class, the academic Burnout Syndrome appears, to some degree, for most of the students in the health area. This fact is confirmed by Dyrbye and Shanafelt (2016), who state that those students have higher levels of the Burnout Syndrome compared with the generic level that most of the general population have.
The second important finding in the present research is the seriousness of the Burnout Syndrome between the third and fourth years, which ranges from a moderate to high level. This phenomenon agrees with the recent research of Elkins et al. (2017) with students of medicine, where it is concluded that as they advance in years of the degree, they seem to have a higher risk of suffering burnout. Similarly, Dyrbye et al. (2006) conclude that burnout is common among students of medicine in the United States and that it probably increases with the school years. This idea was later confirmed in the bibliographic revision of papers published on academic burnout between 1990 and 2015 that the authors made 10 years later (Dyrbye et al., 2017).
Now, when analyzing the subdimension of the student burnout (behavioral and attitudinal) in the students of this research, we find that both subdimensions increase their averages from the third to the fourth year. The three highest averages are related to behavioral items: (1) “Having to attend lectures every day gets me tired”; (3) “During the lectures, I feel sleepy”; and (7) “Before finishing my lecture schedule I feel tired.” Both Items 3 and 7 also had the highest scores in an exploratory study in students of nursery and midwifery, and in another one with students of licentiate (the authors do not specify which), where the highest score was that of Item 3 (Barraza, 2008, 2011). These results were also similar in students in third and fourth years of medicine in a comparative study of Colombian and Mexican students; the items with the highest prevalence were 1 and 7 (Barraza et al., 2012). All these results mentioned by the authors show a predominance of behavioral indicators of student burnout which are manifestations developed in the short term, and in most cases associated with a mild burnout level, which in the present research associates with a prevalence of moderate burnout.
The student population of the present study has the characteristics of the academic context that Caballero et al. (2010) refer to as the one most frequently associated with the syndrome: carrying out training practice at the same time as theoretical subjects, subject matter overload, and activities that require much concentration are taken together. This statement supports the results obtained in the present research since there is an association between the academic activities and not with other student characteristics (e.g., sociodemographic ones).
One salient feature is the difference found on the use of medicines and burnout, showing that students who use antidepressants, anxiolytics, and sedatives present higher levels of burnout. Koutsimani et al. (2019), using a metanalytical approach, suggest that there is an association between burnout and depression, as well as between burnout and anxiety. We believe that the use of medicines (defined in the questionnaire as antidepressants, anxiolytics, and sedatives) could be an indicator of the existence of these base pathologies, making more likely the appearance of burnout symptoms.
It is important to note that this student lifestyle has a profound impact on the students’ daily activities. Our results show a significant and direct association between the Burnout Syndrome and the psychosocial risk behaviors. These conclusions are similar to those of a multicenter study that took place in five schools of medicine in the United States (Dyrbye et al., 2006). Furthermore, recently, Houpy et al. (2017) concluded that a vast majority of the students who had experienced this syndrome had, for instance, family arguments which affected their welfare.
Finally, concerning the strategies for dealing with the academic burnout, the student population studied uses recreational activities as a protective factor, including physical activity among them. Institutions like the Centers for Disease Control and Prevention (CDC) of the United States are concerned with this situation, recommending aerobic and strength exercises to deal with this syndrome. Along with this line, Dyrbye et al. (2017) made a study with 4,402 students of medicine who carried out physical activity following the exercise guidelines of the CDC, concluding that the students who followed them seem to have a lower probability of experiencing burnout.
Limitations of the study
This study presents several limitations that must be understood to interpret its results. First, it is a cross-sectional study and, as such, cannot produce causal relationships. Also, due to the characteristics of the population, midwifery students in just one university and one region, the sample is necessarily small, limiting its generalizability. To overcome this problem, further studies with more universities and locations can also allow testing other hypothesis related to the association of burnout with teaching styles and perceived or actual student support. Other meaningful associations can be applied to further studies, for instance, between burnout and subjective well-being (Oyanedel et al., 2015) or between burnout and sleep quality (Bugueño et al., 2017).
It is also necessary to note that, due to the cross-sectional design, seasonality can affect the results: it is possible that fourth-year students were more burnt out due to extra coursework during the fieldwork period, which may not be accurate for the entire year.
Conclusion
The following conclusions can be drawn from this study:
All students of midwifery suffer some form of academic Burnout Syndrome;
There is an association between the Burnout Syndrome and the year of studies in which student is in, being it significantly higher in the fourth than in the third year, mainly due to the increase in practical activities;
There is an association between the use of medicaments to treat mental health diseases and higher report of burnout;
There is a significant and direct association between the Psychosocial Risk Scale and the Burnout Scale, being psychosocial risks the main predictor of burnout when included in regression models.
In coping with burnout, recreational activities were found to be protective factors.
Footnotes
Ethical Approval
The study was approved by the Ethics Committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported under project CIE 160009 of the Comisión Nacional de Investigación Científica y Tecnológica (CONICYT). It also benefited funding from FONDECYT 1181533 awarded to JC Oyanedel.