
Abstract
Primary care physicians face increasing amounts of administrative work (e.g., entering notes into electronic health records, managing insurance issues, delivering test results, etc.) outside of face-to-face patient visits. The objective of this study is to qualitatively describe the experience that primary care physicians have with administrative work, with an emphasis on their beliefs about their job role. I conducted semi-structured interviews with 28 family physicians and internists in Chicago, Los Angeles, and Miami and qualitatively analyzed themes from interview transcripts using the grounded theory approach. Two major themes concerning the relationship between primary care physicians and administrative work were discovered: (a) Administrative work was not central to primary care physicians’ job role beliefs, and (b) “below license” work should be delegated to nonphysicians. Job roles should be considered in future efforts to reduce physician administrative work in primary care.
Introduction
Health care in the United States is characterized by a much higher administrative workload than comparable Western European countries. The United States has more administrative personnel per capita than the United Kingdom, the Netherlands, and Germany, while employing a similar amount of clinical staff (Cutler & Ly, 2011). Worse, this administrative work, such as charting, scheduling, and handling insurance issues, takes up a significant amount of work time that primary care physicians (PCPs) spend outside of face-to-face patient encounters (Chen et al., 2011; Dyrbye et al., 2012; Sinsky et al., 2016). It is estimated that physicians lose US$68,000 to US$85,000 a year in revenue on time spent on billing and insurance issues alone (Casalino et al., 2009). Physicians also spend significant amounts of time on administrative work unrelated to billing and insurance. Internists in two health care systems in New York reported spending an average of 20% of their work day on activities outside of office visits (Chen et al., 2011). Internists at another major medical center, on average, entered just more than seven orders, wrote almost three prescriptions, and reviewed, edited, and signed nearly two electronic health records (EHR) notes per patient visit (Dyrbye et al., 2012). A study of 57 family physicians, internists, cardiologists, and orthopedists reported that these physicians spent an average of twice the amount of time during their workday on EHR and desk work compared with direct clinical face time with patients (Sinsky et al., 2016). The administrative burden on physicians is so severe that the American College of Physicians recently issued a position paper outlining the problem and the need for solutions (Erickson et al., 2017).
Physicians who spend more time doing administrative work (Ly & Glied, 2014) and who have larger administrative workloads (Landon et al., 2002) have reported lower professional satisfaction. There is also evidence that the use of EHR is related to lower professional satisfaction (Friedberg et al., 2013; Love et al., 2012) and higher burnout (Babbott et al., 2014; Shanafelt, Dyrbye, et al., 2016). However, administrative work can still be valuable, as there is evidence that telephone and electronic communication with patients can reduce office visits (Chen et al., 2011) and improve patient outcomes (Green et al., 2008; Ralston et al., 2009; Simon et al., 2011).
Previous work has proposed (Succi & Zhiping, 1999) and confirmed (Holden, 2012) that physicians adopt EHR in relation to its perceived effect on their job role, and several working groups have urged physicians to adopt and use EHR as a part of their professional role (Brach et al., 2014; Phillips et al., 2014). Authors have examined the physician perspectives on administrative work (Colligan et al., 2016), but the relationship between administrative work and PCP role remains understudied. “The work no one sees” (as described by Dyrbye and colleagues, 2012), exclusive of EHR, is often work that physicians do not necessarily have a legal or regulatory requirement to do themselves.
Model of Work Content in Primary Care
Administrative work is defined by task (Chen et al., 2011), task group (Sinsky et al., 2016), or relative value to patient care (Erickson et al., 2017) in the literature, but no cohesive model of administrative work exists. A model building off of prior conceptualizations of administrative work (Chen et al., 2011; Sinsky et al., 2016) is presented in Figure 1. This model groups administrative tasks and other outpatient primary care work content into meaningful task group categories. Work is subdivided into patient care, administrative work, and office work. Patient care (white circle in Figure 1) includes activities most directly related to the practice of medicine such as nonadministrative work like diagnosis and treatment; patient administration (light gray circle) includes activities that have mixed clinical and administrative aspects like scheduling appointments and handling insurance issues; office work (dark gray circle) includes purely administrative work like reordering supplies or troubleshooting EHR issues. Activities that can be completed by nonphysicians in part (e.g., some level of diagnosis and treatment, depending on licensure) or in total (e.g., patient education and insurance issues) are also highlighted. This model is presented to elucidate the concept of administrative work, as opposed to patient care or management of an office, and to highlight tasks that can be performed by nonphysician providers and staff.

Diagram of primary care outpatient work content.
New Contributions
Primary care is at the forefront of the changing health care landscape, and many changes intended to lower cost or increase quality lead to the unintended consequence of increased administrative work (Erickson et al., 2017). Previous authors have examined the volume or type of administrative work undertaken by PCPs (Chen et al., 2011; Dyrbye et al., 2012; Sinsky et al., 2016), but few studies have examined the qualitative aspect of this work. One recent effort did obtain physician perspectives on specific administrative tasks and reported that physicians cited these tasks as a source of time pressure and dissatisfaction (Colligan et al., 2016). The objective of our qualitative study was to extend previous analyses by characterizing the relationship between administrative work and PCPs’ job role beliefs.
Method
Study Design
Semi-structured phone interviews were conducted with family physicians and internists in the Los Angeles, Chicago, and Miami metropolitan areas from February to December 2016. Respondents were drawn from personal contacts of members of my dissertation committee (P.C., G.R., and M.T.), as well as through cold calling physicians listed as sole proprietors in the Centers for Medicare and Medicaid Services National Provider Identifier Registry. Purposeful sampling was conducted to ensure sample diversity in terms of specialty, gender, and location. The study protocol was approved by the RAND Human Subjects Protection Committee, and all respondents provided informed verbal consent. In total, 28 physicians participated in interviews.
Data Collection
All interviews were conducted over the phone. The interview guide, written for a concurrent exploratory study on factors affecting physician professional satisfaction, contained many broad overview questions of physician professional satisfaction, as well as directed questions on satisfaction and several workplace/health system drivers of satisfaction (Appendix; intrinsic/extrinsic drivers of satisfaction, EHR, patient/workplace relationships, and nontraditional payment/delivery models). Analyses of professional satisfaction overall and specific topics unrelated to administrative work will be presented elsewhere. Although the questions in Appendix were always asked, respondents were given the freedom to direct the interview toward drivers of satisfaction that they found most personally relevant. Interviews were conducted until thematic saturation was obtained. No consistent “negative cases” (as described by Morse, 1995) regarding the centrality of administrative work to the PCP job role were discovered. The first eight respondents participated without compensation, and when funding then became available, the last 20 respondents were compensated with a US$100 electronic Amazon.com gift card. Interviews were recorded and lasted 30 min on average. The recordings were professionally transcribed, and the transcripts were checked by the author for accuracy.
Analysis
Interview transcripts were read over in their entirety for familiarity (Goffman, 1989) and then inductively coded using an integrated approach (Bradley et al., 2007). First, the principles of grounded theory were used to develop an initial conceptual thematic code structure (Glaser, 1992). Next, a direct approach was used to code participant characteristics (gender, specialty, years in practice), participant setting (location, practice ownership model), and directional participant perspectives on each theme (Bradley et al., 2007). The constant comparison method was used to consolidate these conceptual codes, triangulate similar codes among different respondents (Goffman, 1989), and develop broader themes (Glaser & Strauss, 1967). The themes presented in this article were refined with input from another researcher (P.C.). A policy analytic framework was used to choose themes related to significant policy problems that could be solved by institutions or policymakers (Bardach, 2012). All coding was conducted using the qualitative analysis software Dedoose (Version 7.5.16; SocioCultural Research Consultants, LLC, Los Angeles, CA).
Results
Demographic Characteristics
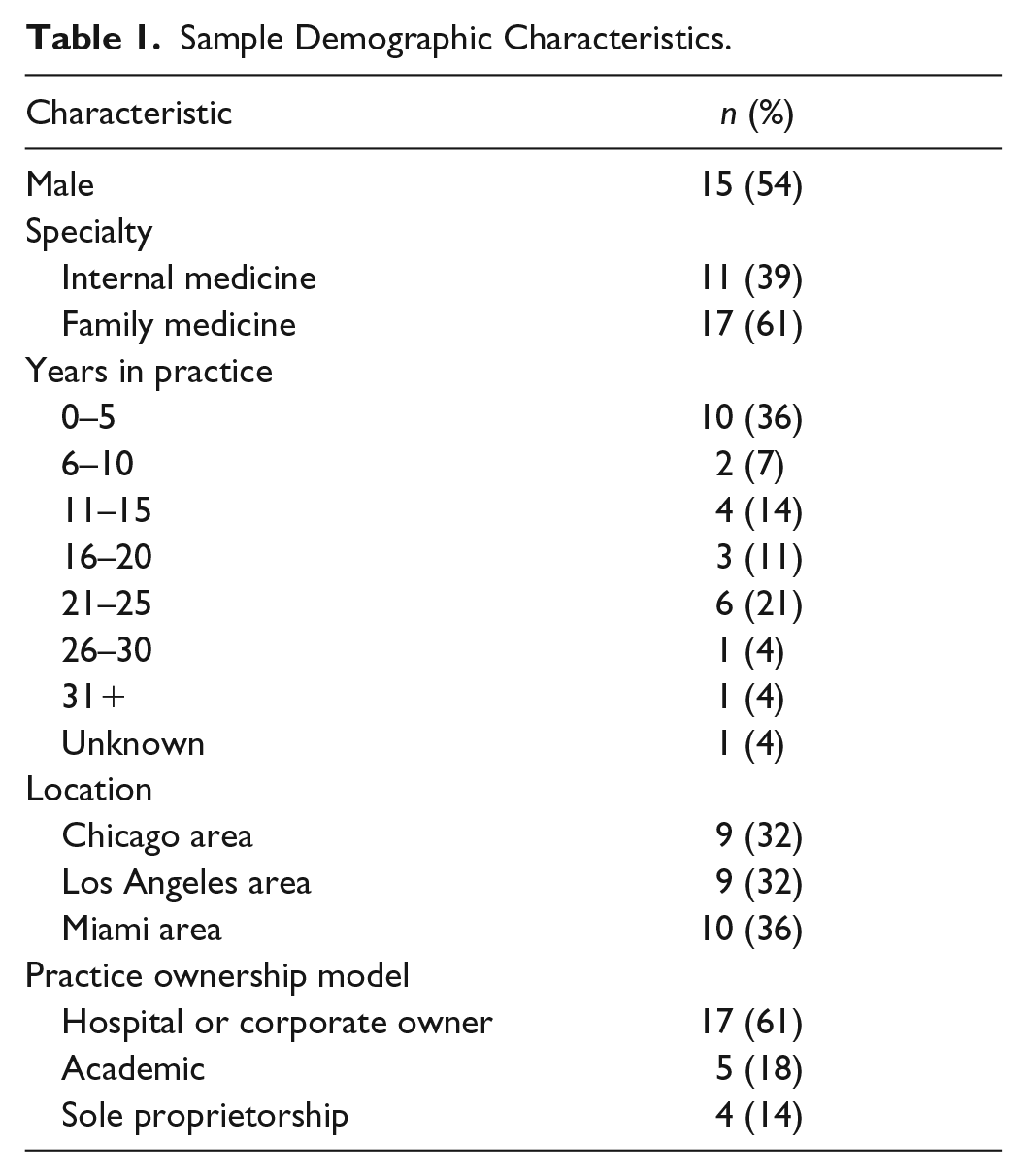
The sample consisted of 28 PCPs (Table 1). Just more than half of the respondents were male and were nearly equally divided between the Chicago, Los Angeles, and Miami areas. About two thirds specialized in family medicine (vs. internal medicine), and most worked in a setting owned by a hospital or other corporation. Years in practice ranged from less than 1 to more than 31 years, but most respondents had less than 16 years in practice, and more than a third of respondents had less than 6 years in practice.
Sample Demographic Characteristics.
Key Themes
The analysis of these interviews uncovered two key themes: (a) Administrative work was not central to PCPs’ job role beliefs, and (b) “below license” work should be delegated to nonphysicians.
Administrative work was not central to PCPs’ job role beliefs
Nearly half of the respondents spontaneously described a relationship between administrative work and their job role and work content. Much of this discussion centered around beliefs that PCPs have about their job role while performing clinical work. No respondents complained about their duty to deliver patient care, but many bemoaned the level of administrative work they were required to perform. As one family practitioner in Miami summarized the problem, “I feel like I was trained to be a doctor. And now I’m like 50% a doctor and 50% this computer clerk person.” This loss of patient care time to administrative work was expanded upon by a family practitioner in Los Angeles: Yeah, and trying to get the medicine that’s right for the patient is often a[n] administrative hassle. Trying to basically do what’s right for the patient requires dealing way too much with bureaucracy and cuts away from my ability to spend more time with the patients.
Although respondents did not always elaborate on what they considered “administrative work,” their descriptions were similar to the type of administrative work detailed in the administrative work domain in Figure 1 (light gray circle; e.g., charting, insurance, orders, etc.). These tasks are largely “paperwork” and may require some physician expertise, but there was no consensus on how much of this work can or should be delegated to nonphysicians. Many respondents complained about one of these tasks, charting, even though many physicians are legally required to perform this work. These requirements were touched on by an internist in Chicago discussing the increasing necessity of performing administrative work to get paid for clinical work: . . . In my clinical role, the reason I enjoy it is because I love seeing patients, but it comes at a cost these days. The cost is the amount of administrative bureaucracy and paperwork that goes along with seeing those patient[s], and often the volume that we have to see to maintain the salaries that we are accustomed to . . . And then over the past ten years they’ve added on so many more layers, actually 20 years of documentation requirements, electronic medical records. You know, it’s basically put more and more work onto the doctor. I can go in and see a patient and talk to them for two minutes, figure everything out and know what I need to do. I then need to spend the next 10 to 15 minutes documenting everything so, I can get paid for it.
Only one physician in my sample was satisfied with their administrative work. This physician worked in a prepaid concierge practice, whereas most of the other respondents worked in traditional, hospital- or corporate-owned practice with a noncash payment model. This Chicago concierge internist noted that the lack of administrative work was directly tied to the payment model: So [, in this concierge practice,] the volume of administrative work is much less and that’s a huge satisfier. And so, I have more time to follow-up on the actual patient care. Say, if my patient has seen a specialist, now I have time to actually call that specialist on the phone and talk to the other doc and discuss the case as opposed to wanting to do that but not ever having the time to.
This counterexample highlights the importance of the system that surrounds a physician’s job role. New payment models such as pay-for-performance have been associated with an increase in administrative work (Friedberg et al., 2013). Physicians working in cash-based concierge practices may not have as much administrative work as those working in practices that accept insurance (Friedberg et al., 2013). A few physicians in the sample working in nonconcierge practices acknowledged that some of their burden of administrative work was related to the requirements laid out by third-party payers or their employer. However, most of these physicians were employed directly or had a contracting relationship with a hospital or corporate health care system, so their knowledge of the legal or regulatory requirements for administrative work may have been limited.
“Below license” work should be delegated to nonphysicians
“Below license” work, as defined by other authors (Friedberg et al., 2017), is administrative work that does not require clinical expertise or a medical license to complete, because the requirements to complete it are below the license of a physician. Tasks that can be completed by nonphysicians, like communicating normal test results to patients outside of office visits, dealing with insurance issues, or scheduling patient visits, are indicated by an asterisk in Figure 1. Several respondents suggested that delegating this work to nonphysicians would be a more efficient use of their time. A Los Angeles–based internist summarized this idea well: We’ve got to get everybody to the top of their license . . . A physician shouldn’t be doing what a LVN [licensed vocational nurse] can do, a LVN shouldn’t be doing what a MA [medical assistant] can do, and MA shouldn’t be doing what a secretary can do, and a secretary shouldn’t be doing what a patient can do.
Although, as above, several respondents noted that performing below license care is an inefficient use of time, others were concerned about such work encroaching on their job role as a physician. These concerns are often still expressed in terms of overall practice efficiency, even if respondents may also be concerned about their job role. A Chicago internist explains that their expertise is best allocated toward performing direct patient care, not administrative work: . . . But don’t make the doctor be the one who has to remind the patient to do the colonoscopy or get the tetanus shot when a team member can do that just as well. Let me be the one who figures out why is he dizzy[.] . . . Is his fatigue due to thyroid disease or depression or something else? That’s where I’m going to excel and be at my top level of service. Not reminding the patient to see an eye doctor and to do X, Y, and Z.
Pay was not discussed by most other respondents or it was only mentioned as fair and market rate. In most cases, physicians discussed pay separately from their hours and the content of their work. However, some below license work, such as non-face-to-face patient communication (e.g., patient email, reminders, etc.), is often unreimbursed. For clarity, it was placed in the administrative work domain of the conceptual model, rather than in the patient care domain (Figure 1). A majority of physicians in the sample were not paid by the hour, and so unreimbursed below license work could be viewed as a component of their total work duties. An internist from Chicago explores this issue and highlights the institutional pushback to paying nonphysicians to perform work that does not generate revenue: Nor do we do a good job of delegating it to ancillary staff and for everyone to work at the top of their license in a team-based approach. That’s partly because of culturally and historically that’s how we’ve been set up. It’s partly because economically, the incentives are such that the doctor literally has to do a certain number of things and/or much of it is not reimbursable work. And we haven’t gotten to the point where we feel like if we could hire an extra person to do this non-reimbursable work, the doctor would make it up somehow.
This respondent states that the cost of hiring additional staff to perform below license work would not be offset by increased reimbursement revenue from less busy physicians. This lack of efficiency in work specialization implies that the job role of a nonhourly physician encompasses some or all work duties required to support reimbursed work. However, many physicians in this sample did not perceive their job role to encompass below license work, even if it was technically a part of their total work duties.
Discussion
Qualitative, semi-structured interviews were conducted with 28 PCPs about the relationship between administrative work and their job role beliefs. Administrative work was practiced by most respondents, but it was not central to their perception of their job role. Below license administrative work was spontaneously highlighted by many respondents as being particularly unrelated to their job role and appropriate for delegation to nonphysician providers and staff. A conceptual model of clinical work was also presented to classify tasks by the domains of patient care, administrative work, and office management.
Administrative work was described as a clear source of job dissatisfaction among respondents, but this relationship is understudied in the literature. However, a related concept, EHR, is consistently linked to lower job satisfaction (Friedberg et al., 2013; Love et al., 2012; Quinn et al., 2009; Wylie et al., 2014) and burnout among physicians (Babbott et al., 2014; Shanafelt, Dyrbye, et al., 2016), especially among EHR systems with poor usability and high complexity (Babbott et al., 2014; Friedberg et al., 2013). External regulations have also been linked to increased burnout. These trends are particularly concerning in an era of increasingly regulated and digital medicine. Physician burnout due to regulation and EHR will only cause more problems to the health care system than the innovations are able to fix.
One possible solution to these negative reactions toward regulation and digitization is an increase in team-based care. As shown in these interviews, many physicians, at least in primary care, welcome a division of labor that removes administrative work from their responsibilities. Hiring more staff to specifically perform administrative work could increase clinic productivity, as well as provider and staff satisfaction (O’Malley et al., 2015; Sinsky et al., 2015). One barrier to this solution is the un- or underreimbursed nature of most administrative work (Dyrbye et al., 2012; Erickson et al., 2017). Hiring additional staff to complete these tasks increases costs to a clinic without raising further revenue. However, burning out physicians with administrative work can also be costly; physicians experiencing more burnout over time are more likely to reduce their working hours at an organization (Shanafelt, Mungo, et al., 2016). This reduction in hours or dropping out of the workforce can be especially costly to society (Dewa et al., 2014), given that physician shortages in the United States between 40,000 and 120,000 are projected over the next decade (Health Resources and Services Administration, 2008; IHS Markit, 2018; Shanafelt, Mungo, et al., 2016). Preventing burnout before it occurs, in this case by redistributing administrative work to specialized staff, is likely to be more cost effective than addressing burnout and its downstream effects after it has already occurred (Sinsky et al., 2017).
It is important to note that hiring additional staff to complete administrative tasks is a solution from the perspective of individual hospitals and clinics, but not the health care system overall. The hiring of additional staff adds costs to the health care system to complete the same amount of work, much of which is arguably unnecessary. Cutler and Ly (2011) have suggested that high administrative costs in the United States relative to the rest of the developed world are caused by two phenomena: (a) an incentive for private insurers to create complex administrative procedures that deter reimbursement and increase profit and (b) a lack of incentive for multiple insurers to cooperate in a multipayer system. The Patient Protection & Affordable Care Act mandated some common operating rules for eligibility verification, claims status transactions, and electronic fund transfers/electronic remittance advice, but procedures for credentialing, prior authorization, and so on still vary by insurer (Cutler & Ly, 2011; “Patient Protection and Affordable Care Act, Section 1104,” 2010). More recent research shows that, even with EHR, administrative billing work is still costly likely because of the complexity of multiple payer contracts (Tseng et al., 2018). Himmelstein and coauthors (2014) have shown that the United States has much higher administrative costs than several other developed nations. They suggest that hospital financing is the cause of high administrative costs, as costs are much higher in the United States than in other countries that pay for hospital capital costs with direct allocation, lump sum payment, or add-ons to fee-for-service rates. In the United States, for- and nonprofit hospitals must pay for capital costs out of profits or operating surpluses, which creates an incentive to increase revenues in a system where reimbursement is intended to only pay for labor and materials. This may incentivize hospitals in the United States to exaggerate patient illnesses or to prioritize the treatment of better insured patients with more expensive providers and procedures. These incentives could result in health care providers and staff performing more administrative work than necessary to increase revenues. All of this evidence for high administrative costs (and work) leads to one solution: the reduction or elimination of the private, multipayer insurance system in the United States. However, this solution is a highly political one and is outside the immediate control of most stakeholders within the U.S. health care system.
One respondent discovered another solution to administrative work: the transition to concierge care. By only accepting cash payment, physicians would be able to avoid the majority of reimbursement-related paperwork. Of course, a widespread adoption of this arrangement would likely impede care transformation and increase health inequity. In a completely cash-based system, health system stakeholders would no longer be able to shape the health care system to achieve more widely accessed, higher quality care at a lower cost. Furthermore, the supply of PCPs would be constrained, funneling physicians to high-income, cash-paying patients and away from more vulnerable, lower income patients with insurance. However, concierge payment models are present only in an estimated 1% to 6% of internal medicine practices (Doherty, 2015), whereas 91% of Americans currently have some sort of employer-based, government-based, or nongroup insurance (Kaiser Family Foundation, 2019). This near-total market penetration of health insurance makes the future expansion of concierge practices seem unlikely. Given that health insurance, and its attendant paperwork, is likely here to stay, addressing the burden of administrative work on physicians remains an important issue.
Team-based primary care is often implemented via the Patient-Centered Medical Home (PCMH) model, a concept that emphasizes team-based, patient-oriented care that can increase both quality and patient experience as well as lower costs (American Academy of Family Physicians et al., 2007). The model has widespread adoption and is practiced by an estimated 45% of family physicians (Nielsen et al., 2016). A recent systematic review reported that PCMHs reduce cost and utilization of PCPs, but that the evidence is still mixed on the effect of PCMHs toward quality and specialist utilization (Jabbapour et al., 2017). Research on the link between PCMHs and patient experience is more limited, but these models have been linked to higher patient satisfaction (Bowdoin et al., 2016; Kottke et al., 2016; Zulman et al., 2017). The relationship between PCMH and physician experience is not well studied, but one analysis of an organizational intervention emphasizing teamwork and team communication demonstrated a link between the intervention and a greater decrease in burnout and a greater increase in job satisfaction (Linzer et al., 2015). Further research on the effect of PCMHs on physician burnout and satisfaction is needed.
This study implies that much of administrative work often does not fit into the job role beliefs of many PCPs. The delegation of below license work to nonphysicians is a potential solution to reduce the burden of administrative work and clarify job roles. Future work should examine the extent that physician job role is affected by administrative workload and changes to practice workflow. Research questions similar to the following should be addressed: (a) What features of administrative work are central to physician job roles? (b) How much and what type of administrative work leads to physician dissatisfaction and burnout? (c) How do physician job roles vary by age, specialty, and location? (d) How are physician job roles affected in the medium and long term by the delegation of below license work to nonphysicians?
The major strengths of this study were providing PCP perspectives on (a) the relationship between administrative work and physician job role beliefs and (b) how that relationship is affected by delegating below license work. However, this study also had several limitations: (a) The sample is of limited size and not representative of primary physicians nationwide; (b) the sample is skewed toward younger physicians, with most having less than 16 years in practice; (c) the sample is split between eight respondents who did not receive incentives and 20 who did, with the nonreceivers expressing more sentiments about administrative and below license work; (d) administrative work is not a well-defined topic and varies by institution and position, so respondents may have discussed noncomparable experiences; (e) most respondents have not worked in enough environments to accurately compare and contrast different levels of administrative work and solutions reduce to it; and (f) the interview guide did not specifically address administrative work and all respondents discussed it either in response to direct question following up on a related topic or spontaneously as a response to an open-ended question.
Conclusion
As the health care system continues to evolve in the 21st century, so too does the role of the PCP. Physicians can now spend as much or more time conducting administrative work as they do delivering direct patient care. This burden of administrative work increases job dissatisfaction and burnout and creates a disconnect between expectations about practicing primary care and the reality of the day-to-day working environment. Many PCPs are dissatisfied with effect that this work has on their job role, but, luckily, they are largely amenable to solutions that delegate below license work to nonphysicians. As the practice and delivery of medicine become more complicated, the delegation of some administrative work is one potential solution for the increasingly overburdened physician.
Footnotes
Appendix
Acknowledgements
The author would like to acknowledge Peggy Chen, MD, MSc, MHS (chair), Gery Ryan, PhD, and Michael Tutty, PhD, for serving on my dissertation committee and supervising this research. They aided in providing contacts to recruit respondents, as well as giving substantive and editorial feedback on multiple drafts of this manuscript. P.C. also aided in the selection of exemplary quotes and the development of themes.
Author’s Note
The contents of this article do not represent the views of the U.S. Department of Veterans Affairs or the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Pardee RAND Graduate School Anne and James Rothenberg Dissertation award. Dr. E.A. was additionally supported by the VA Office of Academic Affiliations through the Advanced Fellowship in Health Services Research & Development.