
Abstract
Students with multiple health risk behaviors (HRB) have increased amount of research attention. The study aimed to examine the multiple health behaviors and whether these behaviors differ by demographic characteristics and social factors in a 1-year follow-up study among 1,989 students. All the measures were from the Youth Risk Behavior Surveillance System. Associations between demographic characteristics/social factors and multiple HRB were examined by logistic regression models. Binary logistic models indicated that females had generally higher odds of physical inactivity but lower odds of cigarette smoking, alcohol drinking, suicide attempt, and breakfast skipping. Students more than 18 years had higher odds of cigarette smoking. Physical inactivity was negatively correlated with playing school sports teams and taking extracurricular activities. Students with screen time >2 hr/d were more likely to be with physical inactivity or alcohol drinking. Logistic regression models showed that males showed higher odds of two, three, and four to six HRB at 3T. Not taking part in school sports teams/extracurricular activities and screen time >2 hr/d at baseline were risk factors of multiple HRB. Our results reveal a close association between youth risk behaviors and demographic characteristics/social factors. Health promotion interventions of co-occurred behavior should be conducted at schools.
Introduction
College is a critical transition period for establishing health behaviors, and it has long been considered a period of increased risk behaviors. A Chinese study showed that the prevalence of physical inactivity, poor dietary behavior, frequent alcohol use, and current smoking was 62.0%, 29.8%, 11.6%, and 9.3%, respectively, in 2,422 college students (1,433 males) aged 19.7 ± 1.2 years (Ye et al., 2016). Data of a nationwide school-based sample of adolescents in rural China indicated that the prevalence of suicide ideation, plans, and attempts during the past 1 year was 15.1%, 7.2%, and 3.5%, respectively (Zhang et al., 2018). Inner Mongolia medical students in China reported that the overall prevalence of skipping breakfast was 28.9% (Sun et al., 2013). Davila et al. (2014) reported that 29% of the participants reported engaging in at least one unhealthy weight loss behavior (e.g., fasting, purging) over the last 30 days.
Moreover, individuals with multiple health risk behaviors (HRB) have deserved an increasing amount of research attention. It has been estimated that a substantial proportion participate in multiple HRB, with physical inactivity, smoking, and excessive alcohol drinking. Researchers suggested that those engaging in one type of risk behavior often additionally engage in other risks, these risk behaviors sometimes clustering together (Busch et al., 2013; Park et al., 2010; Zhang & Ji, 2015).
In fact, HRB seem to coexist, but this differs by demographic and social factors. There is some evidence that demographic and social factors play a role in risk behavior occurrence. A study showed that Chinese undergraduate students with smoking and drinking often reported clustering with other HRB, such as unhealthy eating behaviors, substance use, and intentional injuries (Guo et al., 2013). It was also found that low leisure activity, low fruits/vegetables intake, and high alcohol use were more frequently reported among smokers in the 2002 Swiss Health Survey (Chiolero et al., 2006). Brooks et al. (2012) reported that factors related to school and community were thought to play a more important role in adolescents’ HRB than family-related factors. It has been demonstrated that risk behavioral frequencies were higher in suburban than urban districts in Beijing, China (Zhang & Ji, 2015), which was similar to Canadian adolescents (Jiang et al., 2008). The prevalence of current smoking and drinking was different in genders among a total of 7,979 students from 44 universities or colleges across China (Guo et al., 2013). It was shown that multiple HRB co-occurred among college students from Wuhan, China, with 56.4% reporting ≥2 HRB. Furthermore, statistically significant positive associations were found between HRB cluster and demographic characteristics, for example, age, gender, and body mass index (BMI; Ye et al., 2016), which were also found in Dutch adolescents (Busch et al., 2013) and U.S. adolescents (Bartlett et al., 2005). Korean adolescents from high socioeconomic status (SES) families were more likely to eat breakfast and have regular exercise and were less likely to smoke compared with those from lower SES families, this indicating a relationship between SES of the family and health behaviors among adolescents (Park et al., 2010).
Reviewing the literature, based on an ecological framework for adolescent health, the health of adolescents aged 10 to 24 years is strongly affected by social factors at personal, family, community, and national levels, such as national wealth, income inequality, and access to education. Furthermore, safe and supportive families, schools, and social environment are crucial to helping young people develop to their full potential and attain the best health in the transition to adulthood (Viner et al., 2012). Few studies have examined interconnections of demographic characteristics, school and social environment on HRB of adolescents using a longitudinal study design in China. Nevertheless, most previous studies in this area have focused on the associations between one or a few factors with one or a few risk behaviors, especially limited in the combined effect of personal, family, schools, community, social environment, and national levels on clustered health risk. The ecological framework for adolescent health could instruct our researchers to select measurement indicators surrounding the model so that achieve more comprehensive results.
Therefore, the study aims to examine associations between demographic characteristics/social factors and risk behaviors in a longitudinal study among Chinese college students and identify the associations between baseline risk factors and multiple risk behavior in follow-up. We hypothesis a close association between common factors and youth risk behaviors. Health promotion interventions of co-occurred behavior could be conducted at schools.
Method
Study Design and Participants
This study was conducted in Anhui province, east of China. The college is selected by convenience sampling. All new freshmen of the selected college (n = 2,913) were recruited by cluster sampling in 2013. Absenteeism and invalid questionnaires are excluded. Baseline data were collected in October 2013, with two follow-up surveys in June and December 2014. Questionnaires were given to the students during classroom time by investigators. The purpose of the study and some tips were explained and we reassured that all participations were fully voluntary and confidential. Approximately 20 to 30 min was given to complete the questionnaire. At baseline, a total of 2,835 freshmen aged 14 to 23 years (mean ± SD: 18.45 ± 0.94) were included. There was just one student with 14 years, other students were aged more than 17 years, and sensitive analysis has shown that there were no significant differences. No missing declarations on any of the analyzed questions were used. A total of 2,616 students in the second survey completed questionnaires as some students were lost to follow-up, and in the third collection a total of 2,586 respondents were included (Figure 1). Ultimately, a total of 1,989 students with three survey data were included in the analysis.
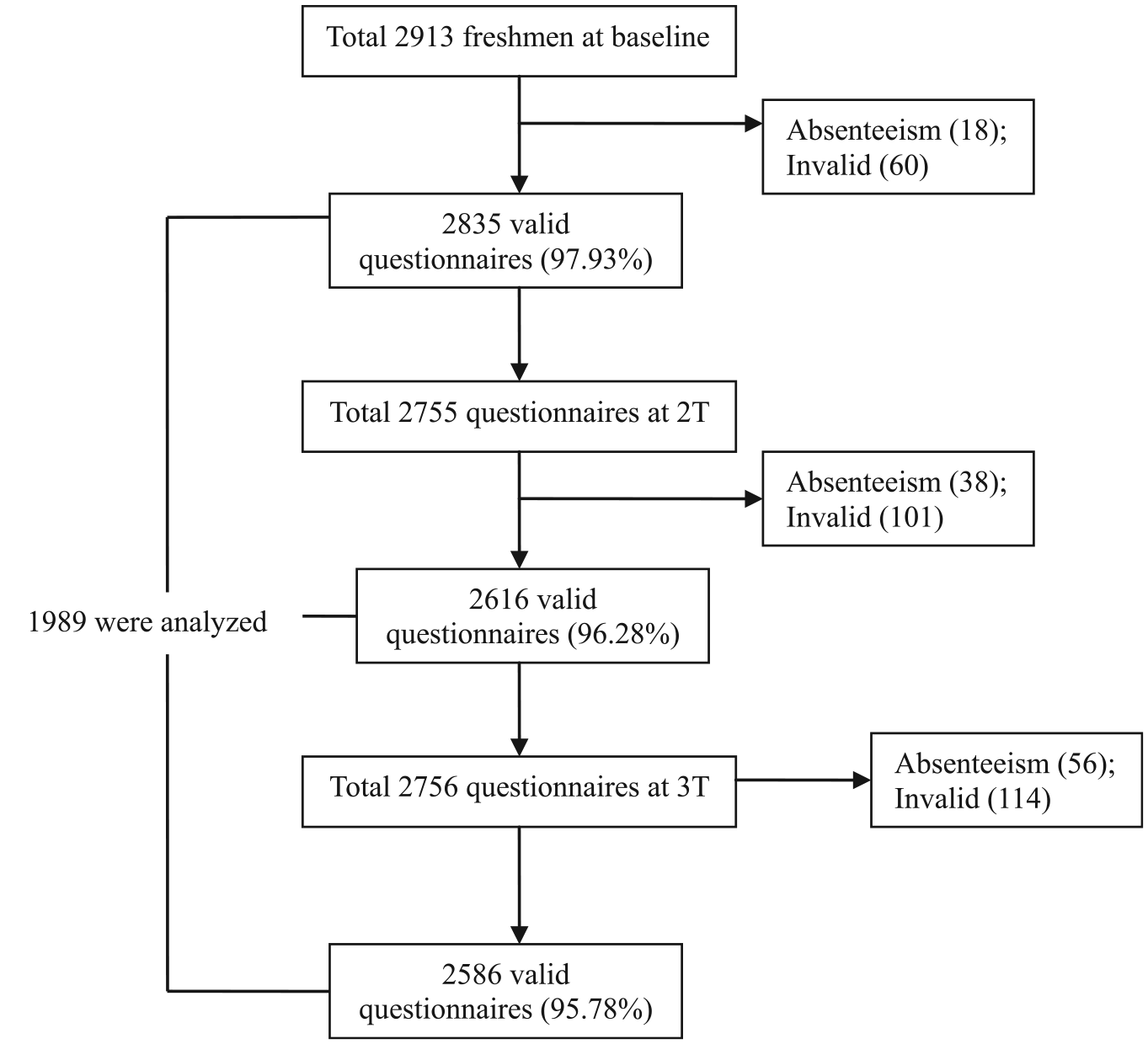
Flow of participants in 2013 to 2014.
The study was approved by the Ethics Committee of Anhui Medical University (No. 20131196). We reassured that all data are used for research purposes only, and no disclosure of personal information. Written informed consent was provided by all participants.
Measures
All participants were asked to complete a self-report questionnaire. For the purpose of this specific study, we focused on sociodemographic characteristics and HRB.
Basic information
Basic information included gender, date of birth, height and weight (subjectively measured), residential area, whether students had any siblings, and perceived family economic status. This information was reported by students. Age was calculated by date of survey minus the date of birth. BMI is defined as the weight (measured to the nearest 0.1 kg) in kilograms divided by the square of the height (measured to the nearest 0.1 cm) in meters (kg/m2) based on World Health Organization (WHO) standards (WHO, 2016). Some questions describing family environment were asked. Residence was categorized into urban and rural. Any siblings was measured by “Are you the only child in your family?” Perceived family economic status was measured by the question: “How is your family economic status compared to other students in your class?” The answers were categorized into three classes: higher, similar, and lower.
School variables
Some questions describing school environment were asked. Learning burden was measured by “In general, how stress do you feel at school nowadays?” In Chinese universities, learning burden is generally considered as the level of curriculum understanding and the feeling of examination stress. The answers were “Heavy,” “Medium,” and “Light.” School sports teams were measured by “How many sports teams (school or community groups) did you play during the past 12 months?” including team-based sports (football, basketball, etc.) and groups for someone have a passion for the same kind of sport. The original four-point ordinal scale was divided into two categories: “Play sports teams” (“1 team,” “2 teams,” and “3 or more teams”) and “Didn’t play sports teams” (“0 teams”). Extracurricular activities were measured by “Did you do some personal sports activities after school?”
Media factors
The question for screen time measurement was “How many hours do you play video or computer games or use mobile phone or use a computer/tablet for something that is not related to learning on an average school day?” (Eaton et al., 2012). The original seven answers were recoded into two categories (Tremblay et al., 2011): less than or equal to 2 hr/d (“I do not play,” “Less than 1 hr/d,” “1 hr/d,” and “2 hr/d”) and more than 2 hr/d (“3 hr/d,” “4 hr/d,” and “5 or more hr/d”). The university guarantees the accommodation when the students are studying in the school and there are no televisions in dormitories, so watching TV is not included.
HRB
Several questions based on the questionnaire developed by the Young Risk Behavior Surveillance System (YRBSS) were adopted (Eaton et al., 2012). Physical inactivity was measured by “How many days of the past 7 days were you involved in at least 60 minutes of physical activity in total per day?” The original answers were recoded into two categories: <3 d/w and ≥3 d/w (cutoff point: P75). Cigarette smoking was measured by “How many cigarettes did you smoke per day on the days you smoked during the past month?” Smoking was defined as smoked at least one cigarette per day. Alcohol drinking was measured by “How many days did you have at least one drink of alcohol during the past month?” Alcohol drinking was defined as drinking at least 1 day during the past 30 days. Suicide attempt (SA) was measured by “How many times did you actually attempt to suicide during the past year?” SA was defined as actually attempt to suicide at least one time during the past year. Breakfast skipping was measured by “How many days of the past 7 days did you eat breakfast?” The original answers were recoded into two categories: <3 d/w and ≥3 d/w (cutoff point: P75). Unhealthy weight control behaviors were measured by asking if students took one of the following three actions to lose weight or to keep from gaining weight during the past 30 days: Did you go without eating for 24 hr or more; did you take any diet drugs without a doctor’s advice; and did you induce vomiting or take cathartics? Unhealthy weight control behaviors were defined as engaging in at least one behavior during the past 30 days.
Statistical Analysis
Binary variables (yes/no) were physical inactivity, cigarette smoking, alcohol drinking, SA, breakfast skipping, and unhealthy weight control behaviors. Multiple HRB was categorized into five levels: 0 (without any HRB), 1 (those with one HRB), 2 (those with two types of HRB), 3 (those with three types of HRB), and 4–6 (those with four to six HRB). Chi-square test and logistic regression model were used to assess the associations between demographic characteristics and social factors with HRB. Associations between demographic characteristics and social factors and categories of multiple HRB were examined using multinomial logistic regression models (test of parallel lines showed p < .05). SPSS software, version 10.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses.
Results
All prevalence of single behaviors is displayed in Figure 2. Demographics and social factors for each behavior at baseline and follow-up are presented in Tables 1 and 2. Males reported more cigarette smoking, alcohol drinking, and breakfast skipping but less physical inactivity than females at baseline and follow-up. Moreover, males reported more SA at follow-up. The older students (>18 years) reported more smoking at baseline and follow-up. Individuals who were overweight or obese reported more alcohol drinking at baseline and 2T and less physical inactivity at 2T. Students from urban were more likely to experience alcohol drinking, SA, and unhealthy weight control behaviors at baseline, but reported less breakfast skipping at follow-up. Students without siblings reported more alcohol drinking, SA, and unhealthy weight control behaviors at baseline, more cigarette smoking at 2T, and more alcohol drinking at follow-up. The prevalence of unhealthy weight control behaviors at baseline, SA, and breakfast skipping at 2T was different among three levels of perceived family economic status. Students with heavy learning burden reported more SA at baseline and breakfast skipping at 3T. Students playing in school sports teams or taking some extracurricular activities were both less likely to be physical inactivity in three surveys and experience breakfast skipping at follow-up. Students with screen time >2 hr/d were more likely to be physical inactivity in three surveys, as well as alcohol drinking at baseline and 2T or breakfast skipping at follow-up.

The percentage of health risk behaviors in 2013 to 2014 (N = 1,989).
Prevalence of Health Risk Behavior by Factors Among College Students at Baseline in Anhui, 2013 (N = 1,989).

Note. BMI = body mass index.
p < .05. **p < .01.
Prevalence of Health Risk Behavior by Factors Among College Students at Follow-Up in Anhui, 2014 (N = 1,989).
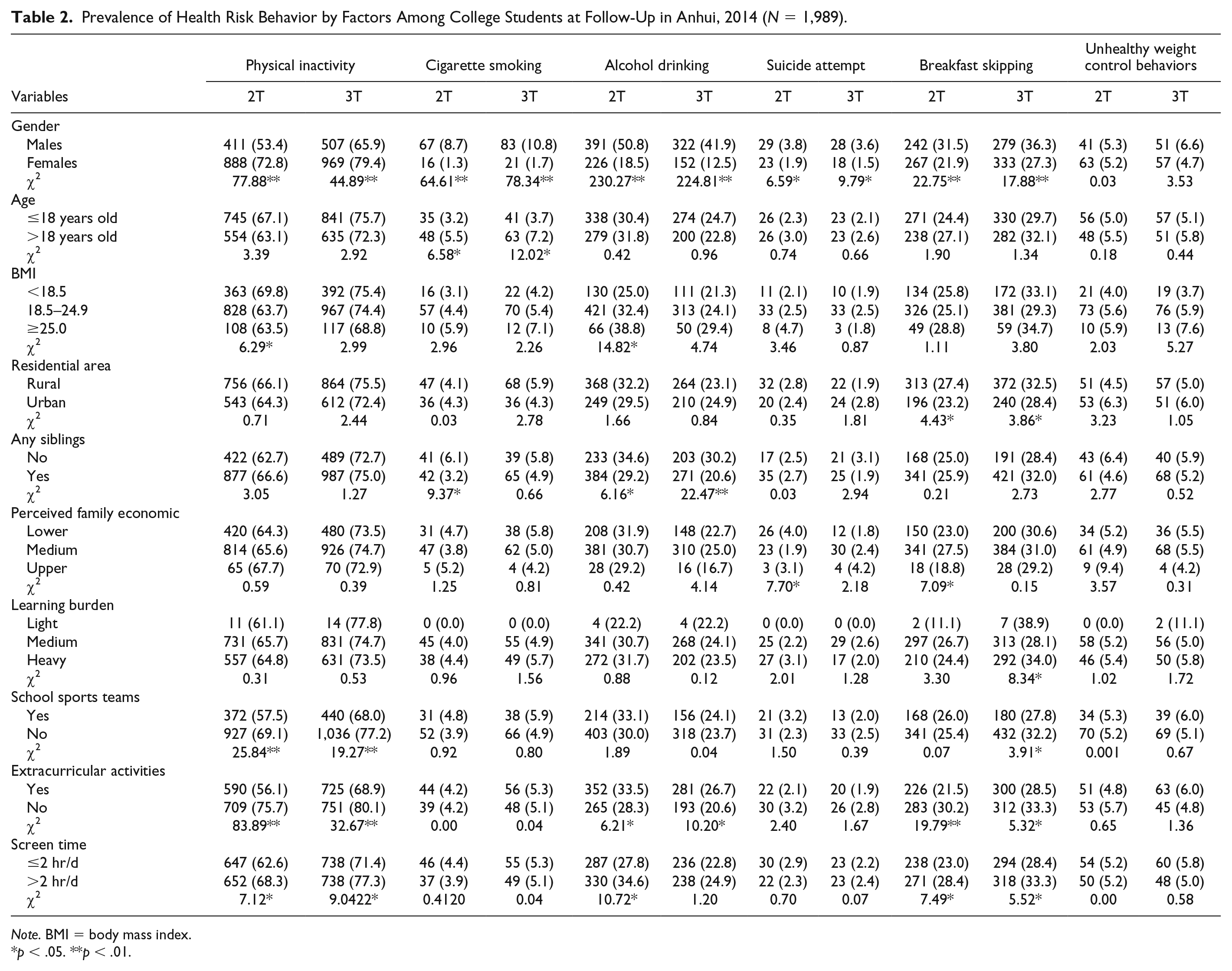
Note. BMI = body mass index.
p < .05. **p < .01.
Combinations of multiple HRB are presented in Figure 3. Table 3 provides rates of HRB co-occurrence by demographic characteristics and social factors in 2013 to 2014. Males have a significantly higher proportion of the “Two risks,” “Three risks,” and “Four to six risks” but lower proportion of the “Without HRB” and “One risk” than females. Students less than 18-year-old reported lower proportion of the “Without HRB,” “Two risk,” and “Four to six risk” but higher proportion of “One risk” and “Three risks” than those more than 18-year-old at follow-up. Students with higher BMI value have a lower percent of “Without HRB,” “One risk,” and “Four to six risks,” but higher percent of “Two risks” and “Three risks” at baseline. Students coming from rural area or without siblings reported higher proportions of “Without HRB” and “One risk” but lower percent of “Two risks,” “Three risks,” and “Four to six risks” at baseline. Generally, students playing sports teams or taking extracurricular activities tended to have a higher proportion of “Without HRB” and lower percentages of “One risk,” “Two risks,” “Three risks,” and “Four to six risks” at baseline and follow-up. However, the rates of “One risk” at 2T or 3T were higher among students playing sports teams or taking extracurricular activities. Similarly, students with screen time >2 hr/d mainly reported a lower percentage of “Without HRB” and “One risk,” as well as higher percentages of “Two risks,” “Three risks,” and “Four to six risks” both at baseline and follow-up, but higher percentages of “One risk” and “Four to six risks” at 3T were listed.
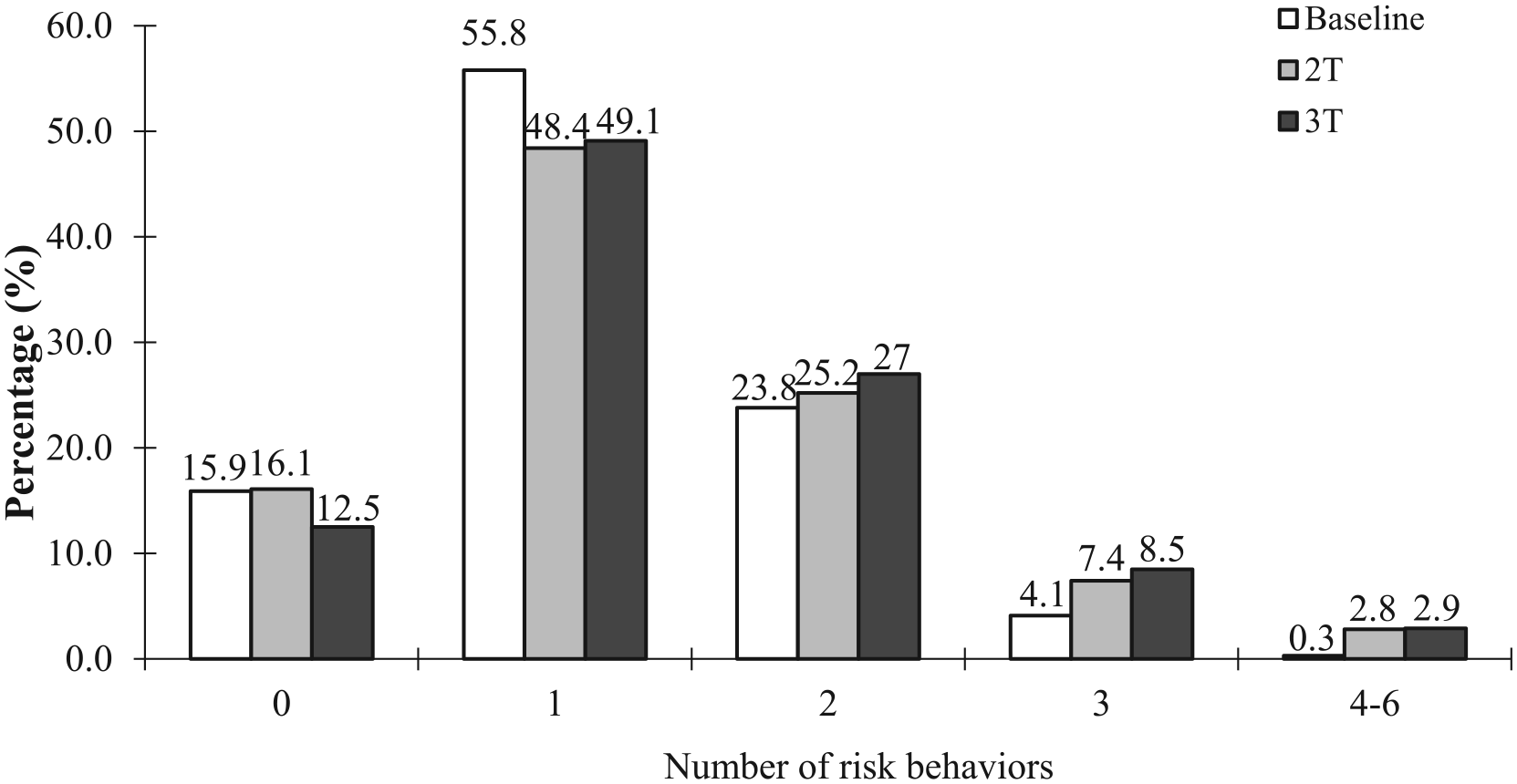
Percentage of the number of risk behaviors in 2013 to 2014 (N = 1,989).
Prevalence of Multiple Health Risk Behaviors by Factors Among College Students in Anhui, 2013–2014 (N = 1,989).

Note. BMI = body mass index.
p < .05. **p < .01.
Table 4 summarizes the results of separate binary logistic models for each HRB. Females had generally higher odds of physical inactivity but lower odds of cigarette smoking, alcohol drinking, SA, and breakfast skipping than males. Students >18 years had higher odds of cigarette smoking compared with ≤18 years. Physical inactivity was negatively correlated with playing school sports teams and taking extracurricular activities. There were significant correlations between screen time and physical inactivity or breakfast skipping. Students with screen time >2 hr/d were more likely to suffer physical inactivity or breakfast skipping.
Odds Ratios (OR) and 95% CI for Health Risk Behaviors Among College Students at 3T in Anhui, 2013–2014 (N = 1,989).

Note. BMI = body mass index; CI = confidence interval.
p < .05. **p < .01.
Table 5 presents results of multiple HRB by the multinomial logistic model. Generally, males had 0.67 times lower odds of one HRB at 3T than females; however, they showed higher odds of two HRB, three HRB, and four to six HRB than females. Medium learning burden was protective factor of two HRB. Students did not take part in school sports teams and extracurricular activities were risk factors of multiple HRB. For example, students not taking part in sports teams had 1.45 times higher odds of two HRB at 3T. Students without extracurricular activities showed 1.50, 1.58, and 2.24 times higher odds of two HRB, three HRB, and four to six HRB, respectively. Screen time ≤2 hr/d was protective factor of multiple HRB. Multiple HRB were lower in the students with screen time ≤2 hr/d compared with screen time >2 hr/d.
Odds Ratios (OR) and 95% CI for Multiple Health Risk Behaviors Among College Students at 3T in Anhui, 2013–2014 (N = 1,989).
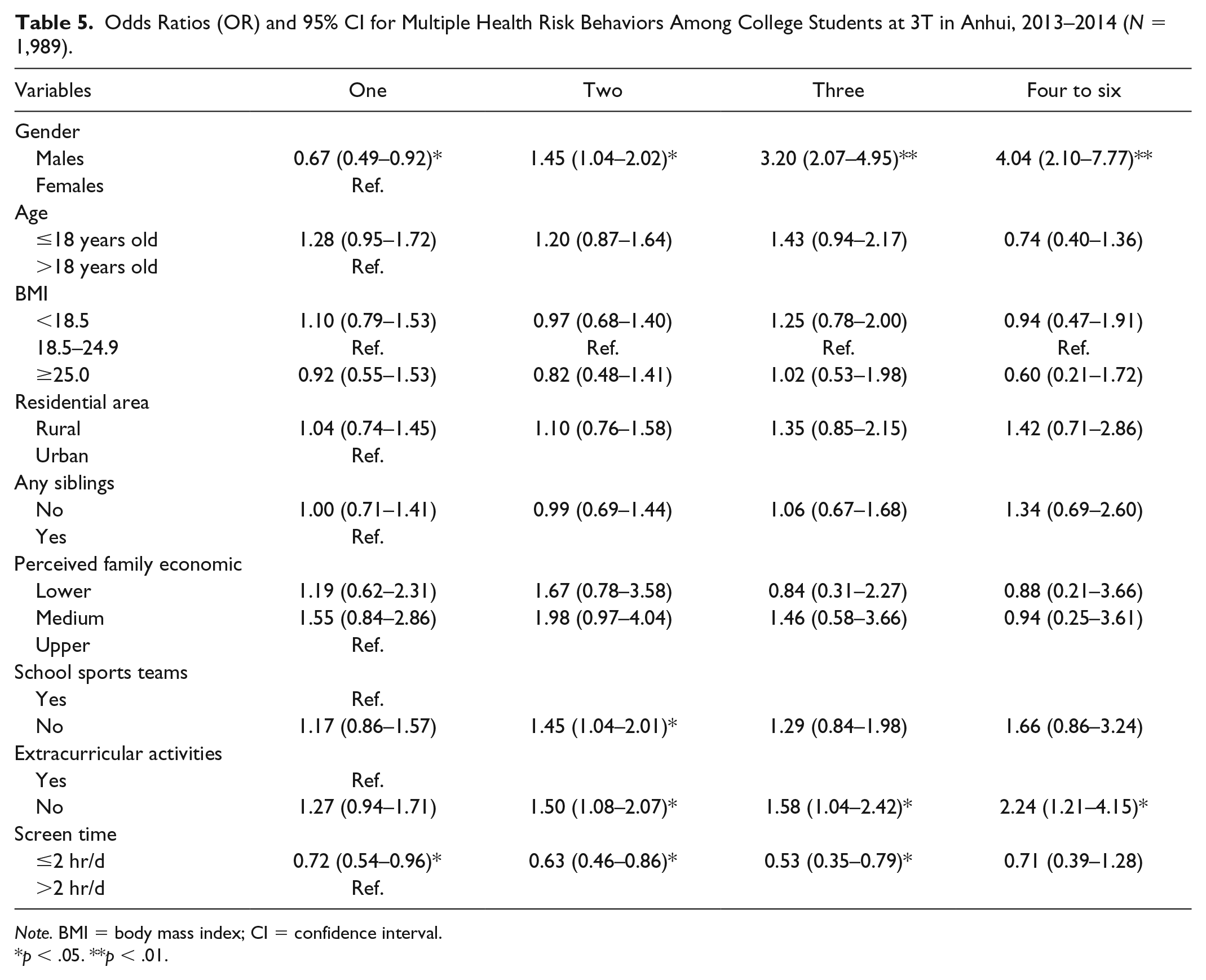
Note. BMI = body mass index; CI = confidence interval.
p < .05. **p < .01.
Discussion
This study is the first to examine the prevalence and a combination of demographic characteristics and social factors of HRB in Chinese medical college students using longitudinal study design. As expected, this study documented that physical inactivity, cigarette smoking, alcohol drinking, SA, breakfast skipping, and unhealthy weight control behaviors were highly prevalent among Chinese college students (Figure 2), which was in partial accordance with National Survey 2013 in Thai Youth (Sirirassamee & Sirirassamee, 2015).
There were no consistent results of demographic effects in all the six HRB. Although demographic characteristics may relate to the prevalence of HRB, they do not predict the risk of HRB. The results showed risks of HRB in this sample replicate or differentiate findings from other previous studies. There was a higher rate of all the HRB in males than females, such as smoking and alcohol use (Ohene et al., 2005), which was in accordance with the present data. This study indicated that the rates of physical inactivity in males were lower than that of females, but there were no age-based differences. Loprinzi et al. (2013) showed that males were more physically active than females engaged in at least 71 min/day of moderate-to-vigorous physical activity and younger participants engaging in more moderate-to-vigorous physical activity per week than older participants. A research has revealed no rural–urban-based differences in physical activity levels in German children and adolescents, and regular physical activity behaviors such as school sports teams and extracurricular activities were more beneficial compared with a decreased physical activity (Lammle et al., 2012) which was in line with the present data. Screen time ≤2 hr/d was associated with increased moderate–vigorous physical activity, which is in accordance with Spanish National Health Surveys (Alonso-Fernandez et al., 2015). The lowest household income group had a higher risk of smoking than the highest household income group in both urban and rural areas for Korean adult population (Yun et al., 2015), but this association has not been found in this study. Tobacco and alcohol use were higher in boys and urban students (Foulger et al., 2013). But Shin and Kang (2014) reported that adolescents living in cities were consuming alcohol and using tobacco less than adolescents in rural areas, which is inconsistent with our findings. More participation in sports has been shown to be related to a reduced incidence of suicidal ideation in the past year (Lester, 2014). Moy et al. (2009) indicated that as the participations’ age increased, their risk of BS was lower and people who ate breakfast had a significantly higher BMI compared with those who reported skipping breakfast (El Hamid Hussein, 2014). In this study, the rate of breakfast skipping was higher in older students or higher BMI students but was not statistically significant. Females consistently were more likely to report unhealthy weight control behaviors than males. Unhealthy weight control behaviors were significantly associated with higher BMI (Stephen et al., 2014), which is inconsistent with our findings, and we sighted that the rates of unhealthy weight control behaviors were higher in students living in urban, self-reported no siblings and better family economic.
Although the effects are not large, we provided important support of factors related to multiple HRB. About 12.5%–16.1% of the total sample without HRB and 0.3%–2.9% with four to six multiple HRB in this sample. In German freshmen, only 2% were without risk, 10.5% had one risk, 34.5% had two risks, 34.8% had three risks, and 18.2% of had all four HRB (Keller et al., 2008). About 64% of Czech adults reported no risk, 26% one risk, 9% two risks, and 1% reported all three HRB (Kážmér et al., 2014). Another study showed that 20.2% of the sample were no risk, 39.1% one risk, 29.0% two risk, and 11.7% three and/or four risks, which was more likely to be observed in males (Silva & Petroski, 2012). Rates of multiple HRB increased from 0.3% to 2.9% for four to six HRB. The single HRB at T1 and T2 were strongly correlated with the same HRB at T3, indicating that these behaviors reach a certain stability. Males showed higher odds of two, three, and four to six HRB than females and it was consistent with Colombia students (Cogollo & Gomez-Bustamante, 2013). It has been claimed that SES acted as a significant predictor. Wang et al. (2009) found family affluence as a significant predictor of substance use in adolescents. Teenagers with high SES were more likely to use substances than those with low SES (Hanson & Chen, 2007). Families with a low SES creates more financial burdens in purchasing food or participating in all kinds of sports. Nevertheless, based on the results of our data, we can hypothesize that relative better financial condition cannot lead to adolescent misuse compared with other schoolmates, which was consistent with results from a multicultural study in 28 countries (Richter et al., 2009). Moreover, there is a lack of clear and unambiguous explanations for the associations between SES and multiple HRB (Pampel et al., 2010), which deserves more research.
Our results suggest that integrated interventions target risk factors not only for individual risk behaviors but also for other risk behaviors and multiple risk behaviors. Demographic and social factors can directly influence the number of risk behaviors, public health interventions should target more risk behaviors and promote healthy lifestyles.
Limitations of this study deserve to be mentioned. Self-report creates recall bias. The findings may not be extended to all Chinese youths as only medical college students were included. Some variables such as parental factors, such as parental education level, parental marital status, and parental health behaviors, seem to play a very important role affecting risk behaviors among adolescents, which limited the explanations of results. However, several strengths should not be ignored. This is a longitudinal study and thus it is able to clarify the causality of the behaviors. It is exact that youths whose involvement in one behavior are strongly related to involvement in other behaviors. The results support the view that interventions may be more efficient if they focus on multiple unhealthy behaviors rather than a single behavior. The findings also provide some available implications for further research.
Conclusion
The associations between HRB in Chinese first year university students remained the same during the follow-up. There are few associations between physical inactivity and so-ciodemographic variables. The results indicated that it is necessary to address health behaviors in the university students. If these findings can be replicated in other youths, programs that promote changes in social environmental factors should be put into early implementation.
Footnotes
Acknowledgements
The authors thank all who are involved in the study for their inputs.
Author contributions
S.T. collected the data, drafted the manuscript and had a major role in data collection, and provided the funding. X.W. got the funding and contributed to subjects’ recruitment and data collection. Y.Z. contributed to subjects’ recruitment and data collection. F.T. had a great role in study design.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by grant from the National Natural Science Foundation of China (grant numbers: 81803257 and 81773455) and was supported by grants for Scientific Research of BSKY (grant number: XJ201824) from Anhui Medical University.