
Abstract
The objective of this study was to assess men’s acceptability of a men’s mental health promotion program in community pharmacies through pilot testing the theoretical framework of acceptability (TFA) as part of the process evaluation. Five men were interviewed about their experiences with the Headstrong program to learn about the acceptability of the program. The TFA was used as the deductive coding scheme and consists of seven constructs including affective attitude, burden, intervention coherence, ethicality, opportunity costs, perceived effectiveness, and self-efficacy. Three constructs, affective attitude, perceived effectiveness, and intervention coherence, from the TFA were coded in all five transcripts. The most frequently coded constructs were affective attitude and perceived effectiveness, coded 19 and 17 times, respectively. Interviewees all reported good relationships with their pharmacists, which influenced their willingness, attitude, and low burden for participation in Headstrong. Each of the men expressed comments reflecting anticipated effectiveness of the program outside of their own experience and how it could impact other men. Use of the TFA as part of a process evaluation of men’s experiences in a men’s mental health program was useful in identifying men’s perceptions of the program’s acceptability. Further research regarding how the quality of existing relationships with clinicians and patients impacts the TFA constructs of affective attitudes, perceived effectiveness, and burden would be useful.
Introduction
Community pharmacies are typically retail spaces in North America with high accessibility by the public (Law et al., 2013). Pharmacists are also trusted by the public for health information and services (Bishop et al., 2015; Hindi, Schafheutle, & Jacobs, 2018; Schindel et al., 2017). More recently, there has been a call for optimizing the scope of pharmacists in mental health (International Pharmaceutical Federation, 2015). Given the accessible, trust, and convenience factors (e.g., no appointments needed) of community pharmacy practice, a pharmacy-based intervention for men’s mental health was developed. Research findings of other groups have demonstrated that men’s health-seeking behaviors differ from women’s and that men avoid or delay help seeking, particularly for emotional concerns (Emslie, Ridge, Ziebland, & Hunt, 2006; Lynch, Long, & Moorhead, 2018; Magaard, Seeralan, Schulz, & Brutt, 2017). A study by DeBate, Gatto, and Rafal (2018) revealed that college-aged males have low intentions to seek care for mental health concerns. They also have low mental health literacy, unfavorable attitudes about help seeking, and experience self-stigma (DeBate et al., 2018). These factors have been associated with avoidance of help seeking from physicians (Tedstone Doherty & Kartalova-O’Doherty, 2010).
“Headstrong—Taking Things Head-On,” hereafter referred to as Headstrong, is a program developed for community pharmacists that focuses on men’s mental health promotion and was launched in 23 community pharmacies in October 2017. The program was implemented in a Canadian province with a population of approximately one million people and just over 300 community pharmacies. The Headstrong program was developed and underpinned by the Behavior Change Wheel (Michie, van Stralen, & West, 2011). The program has six areas of focus including depression, anxiety, insomnia, alcohol use, tobacco use, and suicide. Through education and training, the Headstrong program is intended to build pharmacists’ capacity in men’s mental health care. Pharmacists were brought together for a Headstrong training day and were also enrolled in a learning management system for accessing online learning modules. In addition to modules on the six areas of focus, modules on motivational interviewing were included. The Headstrong program was also developed with a dedicated website, https://headstrong.life, with curated resources for use by men and pharmacists. Accessing health information via the Internet is convenient for men (Diaz et al., 2002). It may also mitigate potential embarrassment and stigma that men may experience.
Men were made aware of the program through signage in the pharmacies. Signage could also be viewed by members of the public who may have concerns about a man in their lives and could request to speak to the pharmacist about the program. Pharmacists could also discuss the program and the resources with existing patients.
As part of the process evaluation for the Headstrong program, we aimed to determine the acceptability of the intervention. However, the acceptability of interventions in health care is poorly defined. In a recent systematic review regarding acceptability, Sekhon, Cartwright, and Francis (2017) indicate that there is “no clear conceptual definition of acceptability and no shared theoretical understanding of the nature of acceptability.” Furthermore, they propose that “acceptability research needs a theoretical framework and associated methods for assessing the cognitive and affective components of acceptability independently of the behaviours it proposes to predict or explain” (Sekhon et al., 2017). They define acceptability as “a multi-faceted construct that reflects the extent to which people delivering or receiving a health care intervention consider it to be appropriate, based on anticipated or experienced cognitive and emotional responses to the intervention” (Sekhon et al., 2017). The theoretical framework of acceptability (TFA) component constructs include ethicality, affective attitude, burden, opportunity costs, perceived effectiveness, self-efficacy, and intervention coherence (Sekhon et al., 2017). We pilot-tested the use of the TFA to explore men’s acceptability of the Headstrong program.
Method
Men’s Interviews
Five men were interviewed during March and April, 2018. Consent was required for participation as per ethical requirements. Men were notified of the opportunity to participate in interviews through the 23 participating pharmacies and through the Headstrong website. The research coordinator conducted interviews via telephone. Interviews were audio-recorded, transcribed verbatim, and cleaned and anonymized. The interview guide included questions such as, “when thinking about the Headstrong program, tell me about the experiences you have had with your community pharmacist when seeking help for mental health and/or addictions-related concerns or medications.” The interview guide is available upon request from the authors.
Ethics Approval
Ethical approval for the “Headstrong—Taking Things Head-On” program was received from the Dalhousie University Research Ethics Board, file number 2015-3728. Verbal consent from men was received and the verbal responses to the consent procedures were recorded on the audio files.
Analysis
We used a directed content analysis technique with deductive coding (Hsieh & Shannon, 2005) and applied the TFA constructs to the interview data. The seven constructs include affective attitude, burden, intervention coherence, ethicality, opportunity costs, perceived effectiveness, and self-efficacy. Coding frequencies were presented as counts along with supporting quotes for each TFA construct. The data were managed in NVivo 10 (QSR International Pty Ltd., 2012).
Coding was conducted simultaneously by both authors. The transcripts were read aloud once and then repeatedly to code excerpts of texts. Each passage of text was discussed in terms of what was being said, what it meant, and which codes were most fitting from the TFA. We attempted to use one code from the TFA to isolate the meaning of the text versus double-coding passages of text.
Results
Five men ranging from ages 27 to 62 years participated. All reported a diagnosis of mental illness. The frequency of visits to their respective pharmacies was at a minimum of monthly and at one individual disclosed daily visits for witnessed opioid replacement therapy.
Coding Results
Three constructs, affective attitude, perceived effectiveness, and intervention coherence, from the TFA were coded in all five transcripts (Table 1). The most frequently coded constructs were affective attitude and perceived effectiveness.
Coding Frequency in the Component Constructs of the Theoretical Framework of Acceptability (Sekhon, Cartwright, & Francis, 2017) From Men’s Interviews in the Headstrong Program.
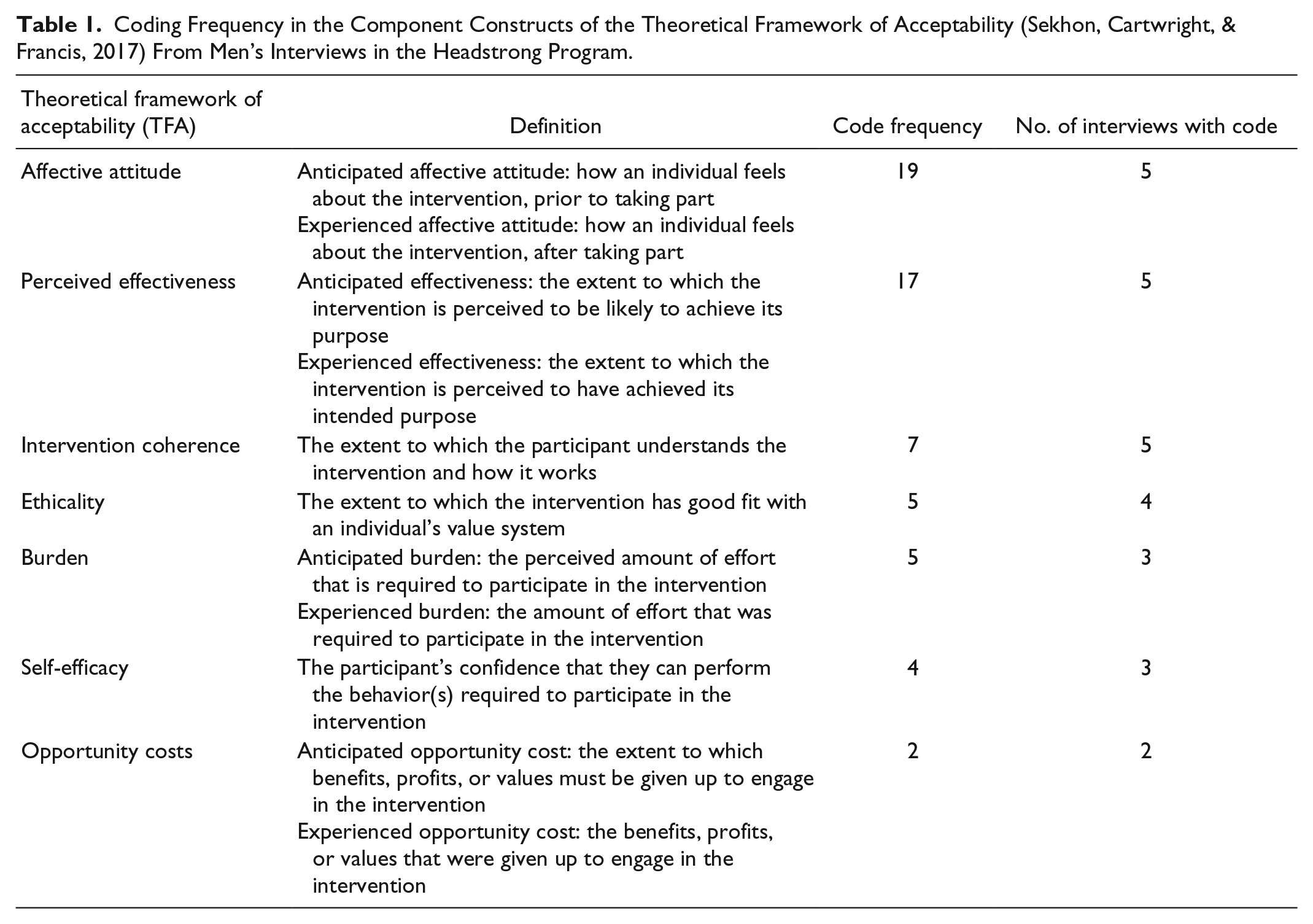
The remaining TFA constructs were coded between 2 and 7 times. Sample quotes are provided in Table 2 as well as through the description of findings for each TFA construct.
Theoretical Framework of Acceptability (Sekhon, Cartwright, & Francis, 2017) Illustrative Quotes From Pharmacists’ Interviews in the Headstrong Program.

Affective Attitude
The participants discussed positive feelings about the program and their existing relationships with their pharmacists prior to the Headstrong program. The positive relationships that existed with their pharmacists influenced their willingness to use the program.
Perceived Effectiveness
The anticipated and the experienced effectiveness of the Headstrong program were generally positive for the men. They not only referred to their perceptions of the program for personal use but also discussed using the program with others and more from the public’s perspective as being an intervention to decrease stigma and self-stigma.
Intervention Coherence
All interviews had codes for intervention coherence. Men mostly understood the Headstrong program’s intended purpose (Interviewee 4, Table 2). However, the discussion of the Headstrong program as an intervention caused some men to describe expectations beyond the program offerings and into the general mental health system (Interviewee 1, Table 2). One interviewee understood the intervention but also described ways to improve the intervention from his personal perspective considering his bipolar disorder diagnosis. This was not one of the content areas of Headstrong. He also described a more general public perspective to improve awareness of the program (Interviewee 5, Table 2).
One participant also commented on some of the materials from the website regarding health promotion campaigns. For example, there was a posting regarding abstaining from alcohol for a specific month of the year. The participant discussed this in relation to their own personal relapse with alcohol use and the importance of reevaluating substance use regularly versus with a temporary campaign (Interviewee 3, Table 2).
Ethicality
Ethicality was coded in all transcripts. Most coding occurred around the expressed importance of the relationships with pharmacists and qualities within that relationship such as trust and rapport that align with values. Interviewee 4 discussed this in the context of physician shortages occurring of many people in the province (Table 2). Some participants also discussed their values around “spreading” and promoting mental health awareness and resources (Interviewee 5, Table 2).
Burden
The men primarily discussed low effort with the Headstrong program. However, although one man discussed being proficient with the website, he first experienced some difficulty using resources on the website (Interviewee 2, Table 2). He also discussed burden as being high in terms of effort to participate when men do not want to disclose or “admit” problems. When relationships with men and pharmacists are good, the burden of participation in the program is low (Interviewee 5, Table 2).
One interviewee who self-disclosed the use of methadone maintenance treatment experienced low burden with the program but reflected on the larger context of burden with his personal mental health care (Interviewee 1, Table 2).
Self-Efficacy
Self-efficacy was typically coded when men spoke of their roles in the relationship with their pharmacist and their abilities in being honest about information given the nature of the Headstrong program and its interdependence of men and pharmacists working together. Another participant similarly discussed honesty with pharmacists and reflecting on his own limitations with medication knowledge (Interviewee 5, Table 2). Interviewee 2 also discussed gaining more competence with the use of the resources on the website (Table 2).
Opportunity Costs
Opportunity costs were coded least in the interviews with men. Interviewee 1 discussed issues with giving up privacy when some pharmacies lack a private space to discuss mental health concerns (Table 2).
There was no charge to men for the pharmacists’ services in the Headstrong program, outside of regular prescription medication charges if they received prescriptions. The Headstrong website had a mixture of free and fee-based programs (e.g., mobile apps). However, paying the fees for a resource recommended by Headstrong was not necessarily seen as a negative aspect of the program and the website (Interviewee 4, Table 2).
Discussion
To our knowledge, this is the first study to pilot the application of the TFA as part of a process evaluation to examine men’s acceptability of a community pharmacy–based mental health intervention. Several important findings resulted from applying the TFA to men’s interviews. This information can be used for program revisions and to inform the design of other interventions.
Overall, the men interviewed had positive feelings about the Headstrong program and perceived the effort to participate as low (i.e., minimal burden). It should be noted that the men had good preexisting relationships with their pharmacists. They also had a relatively high rate of contact with pharmacists occurring monthly or more. This may have influenced their overall impressions and willingness to participate in the Headstrong program. These findings support those of Robertson et al. (2018) in that the pharmacy environment may represent a safe space that promotes trust, reduces stigma, and normalizes the men’s involvement with the intervention. In situations in which men have good relationships with their pharmacists, the Headstrong program’s tools and resources can be used to augment and support pharmacists and men. Importantly, men not only commented on their feelings about the program from their personal perspectives but also discussed their perceptions of the program’s potential impact as an opportunity to decrease stigma and self-stigma. Stigma is recognized as a barrier to help seeking for both men and women experiencing mental illness and addictions. Their comments on stigma also demonstrate good intervention coherence with the program’s intention to increase awareness. A component of the Headstrong program included advertising and signage within pharmacies, which intended to bring attention to the program, let men know that pharmacists care about men’s mental health issues and that a pharmacy is a place to seek help. As reported by Lynch et al. (2018) from a focus group study with men, “to tackle stigma and increase service awareness, participants envisioned direct, positive, and solution-focused advertising that was relevant to their lives and represented diverse young men . . .” (p. 143). Related to this, the men expressed a willingness to not only use the resources personally but to act as a conduit to spread the information about the Headstrong program and resources to other people that they perceived were struggling with mental illness. One man discussed the website with friends, co-workers, and was intending to use it with a relative for substance use issues. This phenomenon is worth further exploration to examine roles that men can play in sharing resources and interventions such as Headstrong. These activities by the interviewee mirror activities in what Cutrona et al. (2016) refer to as a “health information broker.” The broker is someone friends and family turn to for information or advice on health-related topics (Cutrona et al., 2016). These individuals seek, acquire, and pass on information (Cutrona et al., 2016).
Intervention coherence about the program was good; however, there are potential areas of improvement that could occur. For example, the Headstrong resources (e.g., website) are intended for use all year round versus just during 1 month of the year. Monthly health campaigns were expressed as a general concern by one of the interviewees. The sentiment differs from the findings of Lynch et al. (2018) in which a potential solution for targeting men’s health was using advertising “ . . . at specific times of the year, such as winter, and on gaming websites and through social media . . .” (p. 144). More research in this area would be beneficial to determine the impact of advertising and timed health campaigns on factors such as intervention coherence and the subsequent influence on the perceived effectiveness of the interventions and attitudes toward them.
Limitations
The interviewees were a convenience sample of men recruited from the Headstrong pharmacies. Only five men accepted the broader call for participation, which is a small sample and warrants caution for the interpretation of the findings. Ideally, this study would be repeated with a larger sample to explore saturation of constructs. This would allow for a more in-depth exploration of the constructs as well as an increase in the opportunity to determine how many men participated in the program overall. The potential for volunteer bias also exists.
In addition, men did not consistently distinguish whether they were referring to the website versus their personal interactions with the pharmacist during their interviews, and at times, these may have been integrated in the discussion. Thus, further research should explore the individual components of the intervention to determine their individual acceptability.
Affective attitude and perceived effectiveness were coded more often than other TFA constructs. This could reflect bias with overly positive views given the preexisting good relationships with pharmacists.
Conclusion
Use of the TFA as part of a process evaluation to examine men’s acceptability of a mental health program was helpful in identifying aspects of the program that were positive and others that may require redesign. Men with good preexisting relationships with their pharmacists perceived the program positively and had good intervention coherence. The acceptability by men who had less established or no relationships with pharmacists remains unknown. Future research should include an exploration of ways to measure and evaluate roles such as health information brokers who actively seek, acquire, and pass on information from interventions such as Headstrong.
Footnotes
Acknowledgements
We acknowledge Drs. Stan Kutcher and Ruth Martin-Misener for their contributions to the successfully funded grant and Ms. Taylor Currie who was the research assistant that conducted the interviews. Thank you to the men who agreed to be interviewed and to the larger group of pharmacies who participated in the Headstrong program.
Compliance With Ethics Guidelines
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Data Availability
The dataset analyzed during the current study are not publicly available as participants were not asked to consent to full datasets being publicly available. Supporting quotes for the constructs are provided in ample detail.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study and the article processing charges were funded by the Movember Foundation.